Stability of Estimated Premorbid Cognitive Ability over Time after Minor Stroke and Its Relationship with Post-Stroke Cognitive Ability

 , , and
, , and
Abstract
:1. Introduction
- Whether the NART is a valid test of premorbid IQ after stroke by examining the relationship between time after stroke with changes in NART IQ, and current cognitive ability (i.e., how do estimated premorbid IQ and current cognitive ability scores change between follow-up time-points). We will also examine whether the relationships with time remain after controlling for baseline demographic and stroke characteristics. Due to the obvious relationship between age and time, we examine the relationship between age, estimated premorbid IQ and cognitive ability at one to three months post-stroke.
- Whether certain baseline demographic or stroke characteristics predict changes in NART IQ and current cognition scores between two time-points post-stroke.
2. Materials and Methods
2.1. Recruitment
2.2. Follow-Up Assessments
2.3. Statistical Analysis
2.3.1. Aim 1
2.3.2. Aim 2
3. Results
3.1. Patient Characteristics
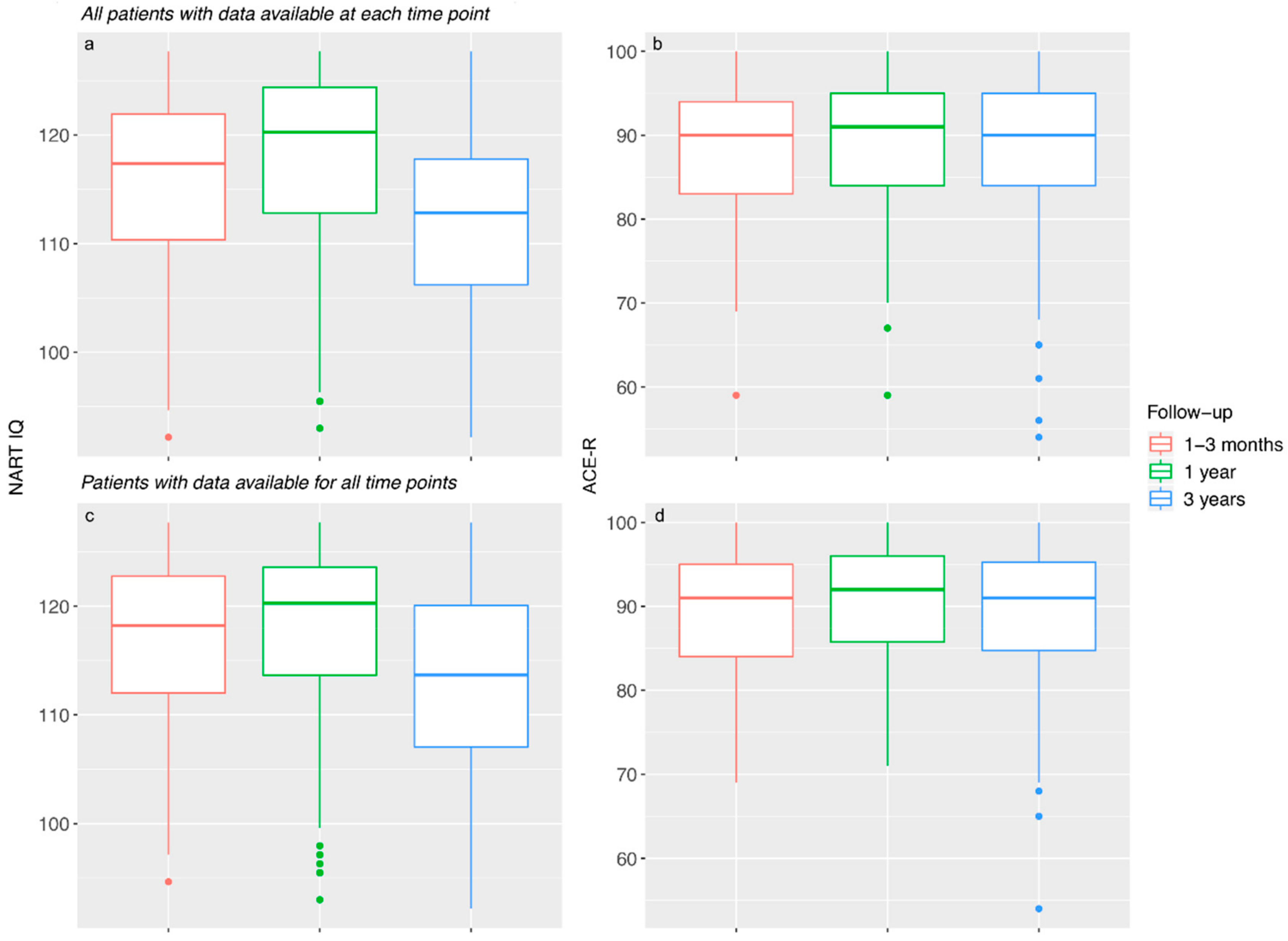
3.2. Aim 1: Changes in Estimated Premorbid IQ and Current Cognitive Ability over Time
3.2.1. NART IQ
3.2.2. ACE-R
3.2.3. Sensitivity Analysis
3.2.4. The Relationship between Age and Estimated Premorbid IQ (NART IQ) and Current Cognitive Ability (ACE-R)
3.3. Aim 2: Predictors of Changes between Time-Points
3.3.1. NART IQ
3.3.2. ACE-R
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Deary, I.J.; Whiteman, M.C.; Starr, J.M.; Whalley, L.J.; Fox, H.C. The Impact of Childhood Intelligence on Later Life: Following Up the Scottish Mental Surveys of 1932 and 1947. J. Pers. Soc. Psychol. 2004, 86, 130–147. [Google Scholar] [CrossRef] [PubMed]
- McGurn, B.; Starr, J.; Topfer, J.; Pattie, A.; Whiteman, M.; Lemmon, H.; Whalley, L.; Deary, I. Pronunciation of irregular words is preserved in dementia, validating premorbid IQ estimation. Neurology 2004, 62, 1184–1186. [Google Scholar] [CrossRef] [PubMed]
- Lezak, M.D. Neuropsychological Assessment, 3rd ed.; Oxford University Press: New York, NY, USA, 1995; 1026p. [Google Scholar]
- Schoenberg, M.R.; Lange, R.T.; Marsh, P.; Saklofske, D.H. Premorbid Intelligence. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 2004–2010. [Google Scholar]
- Jorm, A.F. A short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): Development and cross-validation. Psychol. Med. 1994, 24, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Mchutchison, C.A.; Cvoro, V.; Makin, S.; Chappell, F.M.; Shuler, K.; Wardlaw, J.M. Functional, cognitive and physical outcomes 3 years after minor lacunar or cortical ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2018, 90, 436–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makin, S.D.; Doubal, F.N.; Shuler, K.; Chappell, F.M.; Staals, J.; Dennis, M.S.; Wardlaw, J.M. The impact of early-life intelligence quotient on post stroke cognitive impairment. Eur. Stroke J. 2018, 3, 145–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, H. The National Adult Reading Test (NART): Test Manual; NFER Nelson: Windsor, Australia; Berks, UK, 1982. [Google Scholar]
- Bright, P.; Hale, E.; Gooch, V.J.; Myhill, T.; van der Linde, I. The National Adult Reading Test: Restandardisation against the Wechsler Adult Intelligence Scale—Fourth edition. Neuropsych. Rehabil. 2018, 28, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Bright, P.; Jaldow, E.; Kopelman, M.D. The National Adult Reading Test as a measure of premorbid intelligence: A comparison with estimates derived from demographic variables. J. Int. Neuropsychol. Soc. 2002, 8, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Morrison, G.; Sharkey, V.; Allardyce, J.; Kelly, R.C.; McCreadie, R.G. Nithsdale Schizophrenia Surveys 21: A longitudinal study of National Adult Reading Test stability. Psychol. Med. 2000, 30, 717–720. [Google Scholar] [CrossRef]
- Smith, D.; Roberts, S.; Brewer, W.; Pantelis, C. Test-retest Reliability of the National Adult Reading Test (NART) as an Estimate of Premorbid IQ in Patients with Schizophrenia. Cogn. Neuropsych. 1998, 3, 71–80. [Google Scholar] [CrossRef]
- Bright, P.; van der Linde, I. Comparison of methods for estimating premorbid intelligence. Neuropsych. Rehabil. 2018, 12, 1–14. [Google Scholar] [CrossRef]
- Makin, S.D.; Doubal, F.N.; Dennis, M.S.; Wardlaw, J.M. Clinically confirmed stroke with negative diffusion-weighted imaging magnetic resonance imaging: Longitudinal study of clinical outcomes, stroke recurrence, and systematic review. Stroke 2015, 46, 3142–3148. [Google Scholar] [CrossRef] [PubMed]
- Bamford, J.; Sandercock, P.; Dennis, M.; Warlow, C.; Burn, J. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 1991, 337, 1521–1526. [Google Scholar] [CrossRef]
- Fazekas, F.; Chawluk, J.; Alavi, A.; Hurtig, H.; Zimmerman, R. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Mioshi, E.; Dawson, K.; Mitchell, J.; Arnold, R.; Hodges, J.R. The Addenbrooke’s Cognitive Examination Revised (ACE-R): A brief cognitive test battery for dementia screening. Int. J. Geriatr. Psychiatry 2006, 21, 1078–1085. [Google Scholar] [CrossRef]
- Rothman, K.J. No Adjustments Are Needed for Multiple Comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Deary, I. An ‘instantaneous’ estimate of a lifetime’s cognitive change. Intelligence 2004, 32, 113–119. [Google Scholar] [CrossRef]
- Dykiert, D.; Deary, I.J. Retrospective validation of WTAR and NART scores as estimators of prior cognitive ability using the Lothian Birth Cohort 1936. Psychol. Assess. 2013, 25, 1361–1366. [Google Scholar] [CrossRef]
- Cockburn, J.; Keene, J.; Hope, T.; Smith, P. Progressive Decline in Nart Score with Increasing Dementia Severity. J. Clin. Exp. Neuropsychol. 2000, 22, 508–517. [Google Scholar] [CrossRef]
- Riley, G.A.; Simmonds, L.V. How robust is performance on the National Adult Reading Test following traumatic brain injury? Br. J. Clin. Psychol. 2003, 42, 319–328. [Google Scholar] [CrossRef]
- Skilbeck, C.; Dean, T.; Thomas, M.; Slatyer, M. Impaired National Adult Reading Test (NART) performance in traumatic brain injury. Neuropsychol. Rehabil. 2013, 23, 234–255. [Google Scholar] [CrossRef]
- Flowers, H.L.; Skoretz, S.A.; Silver, F.L.; Rochon, E.; Fang, J.; Flamand-Roze, C.; Martino, R. Poststroke Aphasia Frequency, Recovery, and Outcomes: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2016, 97, 2188–2201.e8. [Google Scholar] [CrossRef]
- Ingles, J.L.; Eskes, G.A.; Phillips, S.J. Fatigue after stroke. Arch. Phys. Med. Rehabil. 1999, 80, 173–178. [Google Scholar] [CrossRef]
- Hedden, T.; Gabrieli, J.D.E. Insights into the ageing mind: A view from cognitive neuroscience. Nat. Rev. Neurosci. 2004, 5, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Zaninotto, P.; Batty, G.D.; Allerhand, M.; Deary, I.J. Cognitive function trajectories and their determinants in older people: 8 years of follow-up in the English Longitudinal Study of Ageing. J. Epidemiol. Community Health 2018, 72, 685–694. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Tang, E.Y.; Amiesimaka, O.; Harrison, S.L.; Green, E.; Price, C.; Robinson, L.; Siervo, M.; Stephan, B.C.M. Longitudinal Effect of Stroke on Cognition: A Systematic Review. J. Am. Heart Assoc. 2018, 7, e006443. [Google Scholar] [CrossRef] [Green Version]
- Hobson, J.P.; Leeds, L.; Meara, R.J.; Woods, R. A comparison of the new executive functioning domains of the CAMCOG-R with existing tests of executive function in elderly stroke survivors. Age Ageing 2001, 30, 251–254. [Google Scholar]
- Rajan, K.B.; Aggarwal, N.T.; Wilson, R.S.; Everson-Rose, S.A.; Evans, D.A. Association of Cognitive Functioning, Incident Stroke, and Mortality in Older Adults. Stroke 2014, 45, 2563–2567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horn, J.L.; Cattell, R.B. Age differences in fluid and crystallized intelligence. Acta Psychol. (Amst.) 1967, 26, 107–129. [Google Scholar] [CrossRef]
- Crawford, J.R.; Parker, D.; Stewart, L.; Besson, J.; de Lacey, G. Prediction of WAIS IQ with the National Adult Reading Test: Cross-validation and extension. Br. J. Clin. Psychol. 1989, 28, 267–273. [Google Scholar] [CrossRef]
- Sharpe, K.; O’Carroll, R. Estimating premorbid intellectual level in dementia using the National Adult Reading Test: A Canadian study. Br. J. Clin. Psychol. 1991, 30, 381–384. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| One to Three Months (n = 158) | 1 Year (n = 151) | 3 Years (n = 153) | ||||
|---|---|---|---|---|---|---|
| With vs. Without Cognitive Data | With vs. Without Cognitive Data | With vs. Without Cognitive Data | ||||
| Demographics | ||||||
| Age at index stroke | 65.09 ± 11.82 | W = 9544.5 | 65.01 ± 11.02 | W = 9845 * | 65.50 ± 11.18 | W = 9476.5 |
| Sex: Male | 93 (58.86%) | χ2 = 0.007 | 93 (61.59%) | χ2 = 1.242 | 83 (54.25%) | χ2 = 2.115 |
| Years of Education a | 11.71 ± 2.94 | W = 876.5 | 11.88 ± 3.02 | W = 1098.5 * | 12.04 ± 3.11 | W = 2633 |
| Smoker: | χ2 = 2.954 | χ2 = 7.551 | χ2 = 12.256 * | |||
| Yes | 48 (30.38%) | 42 (27.81%) | 43 (28.29%) | |||
| No | 56 (35.44%) | 58 (38.41%) | 61 (40.13%) | |||
| Ex-smoker (for more than 1 year) | 47 (29.75%) | 44 (29.14%) | 44 (28.95) | |||
| Ex-smoker (for less than 1 year) | 7 (4.43%) | 7 (4.64%) | 4 (2.63) | |||
| Stroke Characteristics | ||||||
| Stroke subtype: | χ2 = 0.287 | χ2 = 0.998 | χ2 = 0.224 | |||
| Cortical | 90 (56.96%) | 88 (58.28%) | 87 (56.86%) | |||
| Lacunar | 68 (43.04%) | 63 (41.72%) | 66 (43.14%) | |||
| Stroke severity (NIHSS) | 1.00 (1.00) | W = 9853.5 * | 1.00 (1.00) | W = 9319.5 | 1.00 (2.00) | W = 7709 |
| Cognitive Variables | ||||||
| ACE-R | 88.09 ± 8.17 | - | 88.93 ± 7.98 | W = 815 **,b | 88.32 ± 8.92 | W = 2512/W = 1864 *,c |
| NART IQ | 115.40 ± 8.60 | - | 117.56 ± 8.61 | W = 1031 *,b | 112.28 ± 8.40 | W = 2549.5/W = 1998.5 c |
| Scores | Change in Scores | ||||||
|---|---|---|---|---|---|---|---|
| 1–3 Months | 1 Year | 3 Years | 1–3 Months to 1 Year | 1 to 3 Years | 1–3 Months to 3 Years | ||
| NART IQ | |||||||
| n | 154 | 140 | 153 | n | 124 | 101 | 100 |
| Mean ± SD (range) | 115.40 ± 8.60 (92.18–127.70) | 117.56 ± 8.61 (93.08–127.70) | 112.28 ± 8.40 (92.18–127.70) | Mean change (95% CI) | 1.322 (0.54 to 2.13) ** | −4.269 (−5.12 to −3.41) ** | −3.155 (−3.99 to 2.32) ** |
| Decreased n (%) | 35 (28.23%) | 82 (81.19%) | 78 (78.00%) | ||||
| Increased n (%) | 77 (62.10%) | 12 (11.88%) | 15 (15.00%) | ||||
| No change n (%) | 12 (9.68%) | 7 (6.93%) | 7 (7.00%) | ||||
| ACE-R | |||||||
| n | 157 | 151 | 151 | n | 135 | 106 | 101 |
| Mean ± SD (range) | 88.09 ± 8.17 (59.00–100.0) | 88.93 ± 7.98 (59.00–100.0) | 88.32 ± 8.92 (54.00–100.0) | Mean change (95% CI) | 0.289 (−0.49 to 1.07) | −1.047 (−2.08 to −0.01) * | −0.178 (−1.35 to 1.00) |
| No impairment n (%) a | 91 (57.96%) | 91 (60.26%) | 85 (56.29%) | Decreased n (%) | 54 (40.00%) | 57 (53.77%) | 42 (41.58%) |
| Mild impairment n (%) b | 28 (17.83% | 28 (18.54%) | 35 (23.18%) | Increased n (%) | 61 (45.19%) | 42 (39.62%) | 48 (47.52%) |
| Severe impairment n (%) c | 38 (24.20%) | 32 (21.19%) | 31 (20.53%) | No change n (%) | 20 (14.81%) | 7 (6.60%) | 11 (10.89%) |
| 1–3 Months and 1 Year | 1–3 Years | |||||
|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | |
| NART IQ | ||||||
| Time (years) | 1.453 | (0.657, 2.270) | <0.001 | −4.474 | (−5.345, −3.631) | <0.001 |
| Age | 0.100 | (−0.026, 0.225) | 0.118 | 0.099 | (−0.039, 0.237) | 0.170 |
| Sex (male) | 1.232 | (−1.222, 3.587) | 0.316 | 1.497 | (−1.005, 3.999) | 0.253 |
| Baseline Fazekas | 0.166 | (−0.639, 0.973) | 0.692 | −0.002 | (−0.870, 0.865) | 0.996 |
| Stroke subtype (lacunar) | 1.047 | (−1.401, 3.495) | 0.413 | 0.893 | (−1.721, 3.508) | 0.514 |
| NIHSS | −0.214 | (−1.306, 0.877) | 0.707 | 0.032 | (−1.120, 1.182) | 0.958 |
| Hypertension (yes) | 2.815 | (0.222, 5.409) | 0.075 | 2.304 | (−0.466, 5.075) | 0.112 |
| Smoker (yes) | −0.536 | (−3.158, 2.086) | 0.696 | −1.574 | (−4.397, 1.251) | 0.287 |
| Years of education | 1.287 | (0.877, 1.697) | <0.001 | 1.193 | (0.775, 1.612) | <0.001 |
| ACE-R | ||||||
| Time (years) | 0.403 | (−0.375, 1.195) | 0.312 | −1.028 | (−2.039, −0.003) | 0.047 |
| Age | −0.194 | (−0.308, −0.080) | 0.001 | −0.162 | (−0.292, −0.032) | 0.017 |
| Sex (male) | 0.362 | (−1.758, 2.479) | 0.743 | 0.392 | (−1.947, 2.732) | 0.749 |
| Baseline Fazekas | −0.316 | (−1.039, 0.410) | 0.403 | −0.692 | (−1.499, 0.114) | 0.101 |
| Stroke subtype (lacunar) | 0.728 | (−1.474, 2.927) | 0.526 | 1.376 | (−1.070, 3.825) | 0.282 |
| NIHSS | −0.421 | (−1.398, 0.556) | 0.410 | −0.316 | (−1.382, 0.749) | 0.571 |
| Hypertension (yes) | 3.709 | (1.380, 6.037) | 0.002 | 3.465 | (0.864, 6.066) | 0.011 |
| Smoker (yes) | −0.355 | (−2.716, 2.009) | 0.772 | −0.182 | (−2.819, 2.461) | 0.895 |
| Years of education | 0.952 | (0.581, 1.322) | <0.001 | 1.009 | (0.615, 1.404) | <0.001 |
| Variable | Variation in NART IQ with Variable at: | Change in NART IQ between: | Change in NART IQ with Variable at: | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1–3 Months | 1–3 Months and 1 Year | 1 Year | |||||||
| B | 95% CI | p | B | 95% CI | p | B | 95% CI | p | |
| Age | 0.095 | (−0.038, 0.229) | 0.160 | 1.339 | (−3.545, 6.223) | 0.588 | 0.097 | (−0.039, 0.233) | 0.160 |
| Sex | 1.546 | (−0.998, 4.090) | 0.231 | 1.878 | (0.582, 3.173) | 0.005 | 0.847 | (−1.760, 3.453) | 0.521 |
| Baseline Fazekas | 0.402 | (−0.458, 1.262) | 0.357 | 2.954 | (1.306, 4.602) | <0.001 | −0.123 | (−1.004, 0.758) | 0.782 |
| Stroke subtype (lacunar) | 0.704 | (−1.926, 3.334) | 0.597 | 1.122 | (0.035, 2.210) | 0.043 | 1.454 | (−1.238, 4.145) | 0.287 |
| NIHSS | −0.340 | (−1.513, 0.833) | 0.567 | 1.163 | (0.066, 2.260) | 0.038 | −0.062 | (−1.253, 1.130) | 0.918 |
| Hypertension (yes) | 2.970 | (0.162, 5.778) | 0.038 | 1.695 | (0.121, 3.269) | 0.035 | 2.642 | (−0.222, 5.506) | 0.070 |
| Smoker (yes) | −0.256 | (−3.073, 2.562) | 0.858 | 1.672 | (0.692, 2.651) | 0.001 | −0.957 | (−3.836, 1.923) | 0.512 |
| Years of education | 1.400 | (0.958, 1.842) | <0.001 | 4.277 | (1.060, 7.494) | 0.010 | 1.165 | (0.721, 1.608) | <0.001 |
| 1 Year | 1 and 3 Years | 3 Years | |||||||
| Age | 0.098 | (−0.061, 0.257) | 0.223 | −2.107 | (−4.706, 0.492) | 0.111 | 0.0963 | (−0.050, 0.243) | 0.194 |
| Sex | 1.214 | (−1.866, 4.293) | 0.436 | −2.327 | (−2.997, −1.657) | <0.001 | 1.3677 | (−1.345, 4.081) | 0.319 |
| Baseline Fazekas | −0.242 | (−1.281, 0.797) | 0.644 | −2.633 | (−3.551, −1.716) | <0.001 | −0.103 | (−1.035, 0.828) | 0.826 |
| Stroke subtype (lacunar) | 2.980 | (−0.160, 6.119) | 0.063 | −1.723 | (−2.283, −1.164) | <0.001 | 1.842 | (−0.979, 4.663) | 0.198 |
| NIHSS | 0.213 | (−1.166, 1.592) | 0.760 | −2.129 | (−2.727, −1.531) | <0.001 | 0.116 | (−1.122, 1.354) | 0.852 |
| Hypertension (yes) | 2.012 | (−1.383, 5.406) | 0.242 | −2.36 | (−3.215, −1.505) | <0.001 | 2.176 | (−0.815, 5.168) | 0.152 |
| Smoker (yes) | −1.051 | (−4.446, 2.344) | 0.540 | −2.152 | (−2.658, −1.646) | <0.001 | −1.369 | (−4.393, 1.656) | 0.371 |
| Years of education | 0.873 | (0.375, 1.372) | 0.001 | −4.332 | (−6.003, −2.661) | <0.001 | 1.046 | (0.598, 1.495) | <0.001 |
| Variable | Variation in ACE-R with variable at: | Change in ACE-R between: | Change in ACE-R with variable at: | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1–3 Months | 1–3 Months and 1 Year | 1 Year | |||||||
| B | 95% CI | p | B | 95% CI | p | B | 95% CI | p | |
| Age | −0.239 | (−0.345, −0.133) | <0.001 | −2.191 | (−7.337, 2.954) | 0.401 | −0.202 | (−0.311, −0.093) | <0.001 |
| Sex (male) | −0.370 | (−2.417, 1.677) | 0.721 | −0.001 | (−1.389, 1.387) | 0.999 | −0.030 | (−2.150, 2.090) | 0.977 |
| Baseline Fazekas | −0.221 | (−0.915, 0.473) | 0.529 | 0.207 | (1.597, 2.011) | 0.820 | −0.222 | (−0.937, 0.494) | 0.541 |
| Stroke subtype (lacunar) | −0.327 | (−2.433, 1778) | 0.759 | −0.020 | (−1.177, 1.137) | 0.973 | 0.191 | (−1.995, 2.377) | 0.863 |
| NIHSS | −0.609 | (−1.541, 0.323) | 0.198 | −0.536 | (−1.683, 0.612) | 0.357 | 0.115 | (−0.840, 1.070) | 0.812 |
| Hypertension (yes) | 2.761 | (0.499, 5.033) | 0.018 | 0.073 | (−1.601, 1.746) | 0.932 | 2.943 | (0.605, 5.280) | 0.014 |
| Smoker (yes) | 0.388 | (−1.859, 2.635) | 0.733 | 0.595 | (−0.452, 1.642) | 0.263 | −0.835 | (−3.165, 1.494) | 0.479 |
| NART IQ | 0.290 | (0.171, 0.408) | 0.000 | −6.217 | (−18.303, 5.869) | 0.310 | 0.345 | (0.229, 0.461) | <0.001 |
| Years of education | 0.407 | (0.026, 0.788) | 0.037 | −2.157 | (−5.616, 1.302) | 0.219 | 0.603 | (0.229, 0.977) | 0.002 |
| 1 Year | 1 and 3 Years | 3 Years | |||||||
| Age | −0.054 | (−0.196, 0.087) | 0.447 | 5.771 | (2.560, 8.981) | 0.001 | −0.137 | (−0.255, −0.019) | 0.024 |
| Sex (male) | 1.016 | (−1,928, 3.960) | 0.495 | 0.803 | (−0.114, 1.720) | 0.085 | 0.370 | (−1.882, 2.622) | 0.745 |
| Baseline Fazekas | −0.123 | (−1.088, 0.842) | 0.801 | 1.250 | (0.018, 2.482) | 0.047 | −0.407 | (−1.167, 0.353) | 0.291 |
| Stroke subtype (lacunar) | −1.008 | (−3.990, 1.974) | 0.504 | <0.001 | (−0.783, 0.783) | 0.999 | 0.022 | (−2.291, 2.335) | 0.985 |
| NIHSS | 0.227 | (−1.063, 1.517) | 0.727 | 0.683 | (−0.138, 1.504) | 0.102 | −0.005 | (−1.011, 1.000) | 0.992 |
| Hypertension (yes) | 2.378 | (−0.875, 5.632) | 0.150 | 0.444 | (−0.709, 1.598) | 0.446 | 2.367 | (−0.108, 4.843) | 0.061 |
| Smoker (yes) | −1.491 | (−4.670, 1.689) | 0.354 | 0.089 | (−0.619, 0.796) | 0.804 | −0.226 | (−2.697, 2.245) | 0.856 |
| NART IQ | 0.380 | (0.211, 0.549) | <0.001 | −3.704 | (−11.427, 4.020) | 0.343 | 0.416 | (0.286, 0.546) | <0.001 |
| Years of education | 0.548 | (0.064, 1.032) | 0.027 | 1.019 | (−1.312, 3.350) | 0.387 | 0.501 | (0.113, 0.888) | 0.012 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McHutchison, C.A.; Chappell, F.M.; Makin, S.; Shuler, K.; Wardlaw, J.M.; Cvoro, V. Stability of Estimated Premorbid Cognitive Ability over Time after Minor Stroke and Its Relationship with Post-Stroke Cognitive Ability. Brain Sci. 2019, 9, 117. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9050117
McHutchison CA, Chappell FM, Makin S, Shuler K, Wardlaw JM, Cvoro V. Stability of Estimated Premorbid Cognitive Ability over Time after Minor Stroke and Its Relationship with Post-Stroke Cognitive Ability. Brain Sciences. 2019; 9(5):117. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9050117
Chicago/Turabian StyleMcHutchison, Caroline A., Francesca M. Chappell, Stephen Makin, Kirsten Shuler, Joanna M. Wardlaw, and Vera Cvoro. 2019. "Stability of Estimated Premorbid Cognitive Ability over Time after Minor Stroke and Its Relationship with Post-Stroke Cognitive Ability" Brain Sciences 9, no. 5: 117. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9050117