
CRIF1 Deficiency Increased Homocysteine Production by Disrupting Dihydrofolate Reductase Expression in Vascular Endothelial Cells


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culturing and Transfection
2.2. Mouse Studies
2.3. Immunoblotting
2.4. Real-Time Quantitative Polymerase Chain Reaction
2.5. MTHF Content Measurement
2.6. THF Content Measurement
2.7. Ex Vivo Experiments
2.8. Isolation of Mouse Endothelial Cells
2.9. Immunofluorescent Staining
2.10. Homocysteine Content Analysis
2.11. Statistical Analysis
3. Results
3.1. CRIF1 Knockdown Caused an Increase in Homocysteine Levels While Decreasing Folate Cycle Intermediates
3.2. CRIF1 Downregulation Impaired FA Metabolism in Endothelial Cells
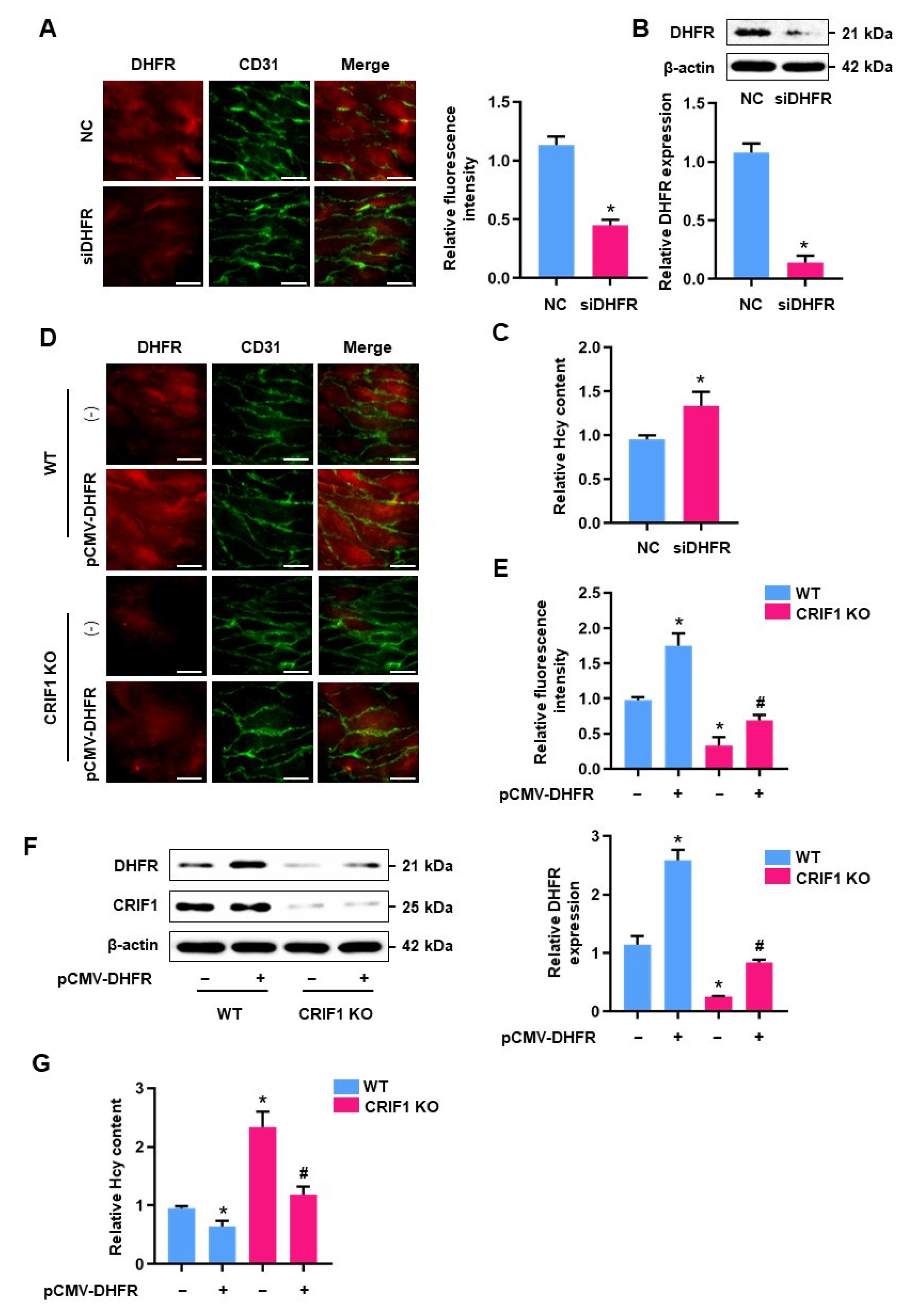
3.3. Increased Homocysteine Levels in CRIF1 siRNA-Treated HUVECs Were Mediated by DHFR
3.4. DHFR Inhibited the Levels of Homocysteine in CRIF1-Deficienct Endothelial Cells
3.5. CRIF1 Deletion Caused an Elevation in Homocysteine Levels and a Decrease in Folate Metabolites In Vivo
3.6. Elevated Homocysteine Concentrations Were Mediated by DHFR in CRIF1 KO Mice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Graham, I.M.; Daly, L.E.; Refsum, H.M.; Robinson, K.; Brattstrom, L.E.; Ueland, P.M.; Palma-Reis, R.J.; Boers, G.H.; Sheahan, R.G.; Israelsson, B.; et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action Project. JAMA 1997, 277, 1775–1781. [Google Scholar] [CrossRef]
- Petri, M.; Roubenoff, R.; Dallal, G.E.; Nadeau, M.R.; Selhub, J.; Rosenberg, I.H. Plasma homocysteine as a risk factor for atherothrombotic events in systemic lupus erythematosus. Lancet 1996, 348, 1120–1124. [Google Scholar] [CrossRef]
- Ganguly, P.; Alam, S.F. Role of homocysteine in the development of cardiovascular disease. Nutr. J. 2015, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Bautista, L.E.; Arenas, I.A.; Penuela, A.; Martinez, L.X. Total plasma homocysteine level and risk of cardiovascular disease: A meta-analysis of prospective cohort studies. J. Clin. Epidemiol. 2002, 55, 882–887. [Google Scholar] [CrossRef]
- Seshadri, S.; Beiser, A.; Selhub, J.; Jacques, P.F.; Rosenberg, I.H.; D’Agostino, R.B.; Wilson, P.W.; Wolf, P.A. Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease. N. Engl. J. Med. 2002, 346, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhang, L.; Miao, Y.; Yang, J.; Wang, X.; Wang, C.C.; Feng, J.; Wang, L. Homocysteine causes vascular endothelial dysfunction by disrupting endoplasmic reticulum redox homeostasis. Redox Biol. 2019, 20, 46–59. [Google Scholar] [CrossRef]
- Meshkin, B.; Blum, K. Folate nutrigenetics: A convergence of dietary folate metabolism, folic acid supplementation, and folate antagonist pharmacogenetics. Drug Metab. Lett. 2007, 1, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, B.; Sahyoun, N.R. Application of the Key Events Dose-response Framework to Folate Metabolism. Crit. Rev. Food Sci. Nutr. 2016, 56, 1325–1333. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Herrmann, W. The emerging role of unmetabolized folic acid in human diseases: Myth or reality? Curr. Drug Metab. 2012, 13, 1184–1195. [Google Scholar] [CrossRef] [PubMed]
- Koseki, K.; Maekawa, Y.; Bito, T.; Yabuta, Y.; Watanabe, F. High-Dose folic acid supplementation results in significant accumulation of unmetabolized homocysteine, leading to severe oxidative stress in Caenorhabditis elegans. Redox Biol. 2020, 37, 101724. [Google Scholar] [CrossRef] [PubMed]
- Moll, S.; Varga, E.A. Homocysteine and MTHFR Mutations. Circulation 2015, 132, e6–e9. [Google Scholar] [CrossRef] [Green Version]
- McDowell, I.F.; Lang, D. Homocysteine and endothelial dysfunction: A link with cardiovascular disease. J. Nutr. 2000, 130, 369S–372S. [Google Scholar] [CrossRef] [Green Version]
- Hultberg, B.; Andersson, A.; Isaksson, A. Higher export rate of homocysteine in a human endothelial cell line than in other human cell lines. Biochim. Biophys. Acta 1998, 1448, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Kwon, M.C.; Ryu, M.J.; Chung, H.K.; Tadi, S.; Kim, Y.K.; Kim, J.M.; Lee, S.H.; Park, J.H.; Kweon, G.R.; et al. CRIF1 is essential for the synthesis and insertion of oxidative phosphorylation polypeptides in the mammalian mitochondrial membrane. Cell Metab. 2012, 16, 274–283. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.; Kim, S.; Nagar, H.; Choi, S.J.; Jeon, B.H.; Piao, S.; Kim, C.S. CR6-Interacting factor 1 deficiency reduces endothelial nitric oxide synthase activity by inhibiting biosynthesis of tetrahydrobiopterin. Sci. Rep. 2020, 10, 842. [Google Scholar] [CrossRef] [PubMed]
- Cario, H.; Smith, D.E.; Blom, H.; Blau, N.; Bode, H.; Holzmann, K.; Pannicke, U.; Hopfner, K.P.; Rump, E.M.; Ayric, Z.; et al. Dihydrofolate reductase deficiency due to a homozygous DHFR mutation causes megaloblastic anemia and cerebral folate deficiency leading to severe neurologic disease. Am. J. Hum. Genet. 2011, 88, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Gellekink, H.; Blom, H.J.; van der Linden, I.J.; den Heijer, M. Molecular genetic analysis of the human dihydrofolate reductase gene: Relation with plasma total homocysteine, serum and red blood cell folate levels. Eur. J. Hum. Genet. 2007, 15, 103–109. [Google Scholar] [CrossRef]
- Lu, W.; Li, H.; Zhang, Y.; Ang, C.Y. Rapid method for the determination of total 5-methyltetrahydrofolate in blood by liquid chromatography with fluorescence detection. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2002, 766, 331–337. [Google Scholar] [CrossRef]
- Gao, L.; Chalupsky, K.; Stefani, E.; Cai, H. Mechanistic insights into folic acid-dependent vascular protection: Dihydrofolate reductase (DHFR)-mediated reduction in oxidant stress in endothelial cells and angiotensin II-infused mice: A novel HPLC-based fluorescent assay for DHFR activity. J. Mol. Cell. Cardiol. 2009, 47, 752–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crabtree, M.J.; Hale, A.B.; Channon, K.M. Dihydrofolate reductase protects endothelial nitric oxide synthase from uncoupling in tetrahydrobiopterin deficiency. Free Radic. Biol. Med. 2011, 50, 1639–1646. [Google Scholar] [CrossRef] [Green Version]
- Obeid, R. The metabolic burden of methyl donor deficiency with focus on the betaine homocysteine methyltransferase pathway. Nutrients 2013, 5, 3481–3495. [Google Scholar] [CrossRef] [Green Version]
- Jacques, P.F.; Selhub, J.; Bostom, A.G.; Wilson, P.W.; Rosenberg, I.H. The effect of folic acid fortification on plasma folate and total homocysteine concentrations. N. Engl. J. Med. 1999, 340, 1449–1454. [Google Scholar] [CrossRef] [Green Version]
- Dhonukshe-Rutten, R.A.; de Vries, J.H.; de Bree, A.; van der Put, N.; van Staveren, W.A.; de Groot, L.C. Dietary intake and status of folate and vitamin B12 and their association with homocysteine and cardiovascular disease in European populations. Eur. J. Clin. Nutr. 2009, 63, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Quadri, P.; Fragiacomo, C.; Pezzati, R.; Zanda, E.; Forloni, G.; Tettamanti, M.; Lucca, U. Homocysteine, folate, and vitamin B-12 in mild cognitive impairment, Alzheimer disease, and vascular dementia. Am. J. Clin. Nutr. 2004, 80, 114–122. [Google Scholar] [CrossRef]
- Ceruti, S.; Giammarioli, A.M.; Camurri, A.; Falzano, L.; Rufini, S.; Frank, C.; Fiorentini, C.; Malorni, W.; Abbracchio, M.P. Adenosine- and 2-chloro-adenosine-induced cytopathic effects on myoblastic cells and myotubes: Involvement of different intracellular mechanisms. Neuromuscul. Disord. 2000, 10, 436–446. [Google Scholar] [CrossRef]
- Lee, H.Y.; Chae, I.H.; Kim, H.S.; Park, Y.B.; Choi, Y.S.; Lee, Y.W.; Park, S.J.; Cha, Y.J. Differential effects of homocysteine on porcine endothelial and vascular smooth muscle cells. J. Cardiovasc. Pharmacol. 2002, 39, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Schroecksnadel, K.; Frick, B.; Wirleitner, B.; Winkler, C.; Schennach, H.; Fuchs, D. Moderate hyperhomocysteinemia and immune activation. Curr. Pharm. Biotechnol. 2004, 5, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Van der Molen, E.F.; van den Heuvel, L.P.; te Poele Pothoff, M.T.; Monnens, I.A.; Eskes, T.K.; Blom, H.J. The effect of folic acid on the homocysteine metabolism in human umbilical vein endothelial cells (HUVECs). Eur. J. Clin. Investig. 1996, 26, 304–309. [Google Scholar] [CrossRef]
- Christensen, B.; Refsum, H.; Vintermyr, O.; Ueland, P.M. Homocysteine export from cells cultured in the presence of physiological or superfluous levels of methionine: Methionine loading of non-transformed, transformed, proliferating, and quiescent cells in culture. J. Cell. Physiol. 1991, 146, 52–62. [Google Scholar] [CrossRef]
- Sharma, G.S.; Bhattacharya, R.; Singh, R. Protein Covalent Modification by Homocysteine: Consequences and Clinical Implications. In Protein Modificomics: From Modifications to Clinical Perspectives, 1st ed.; Dar, T., Singh, L., Eds.; Elsevier: Waltham, MA, USA, 2019; pp. 281–311. [Google Scholar]
- Jiang, X.; Yang, F.; Brailoiu, E.; Jakubowski, H.; Dun, N.J.; Schafer, A.I.; Yang, X.; Durante, W.; Wang, H. Differential regulation of homocysteine transport in vascular endothelial and smooth muscle cells. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1976–1983. [Google Scholar] [CrossRef] [Green Version]
- Selhub, J. Homocysteine metabolism. Annu. Rev. Nutr. 1999, 19, 217–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, P.; Melnyk, S.; Pogribna, M.; Pogribny, I.P.; Hine, R.J.; James, S.J. Increase in plasma homocysteine associated with parallel increases in plasma S-adenosylhomocysteine and lymphocyte DNA hypomethylation. J. Biol. Chem. 2000, 275, 29318–29323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.C.; Yang, F.; Capecci, L.M.; Gu, Z.; Schafer, A.I.; Durante, W.; Yang, X.F.; Wang, H. Regulation of homocysteine metabolism and methylation in human and mouse tissues. FASEB J. 2010, 24, 2804–2817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, J.; Loscalzo, J. Methoxistasis: Integrating the roles of homocysteine and folic acid in cardiovascular pathobiology. Nutrients 2013, 5, 3235–3256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stam, F.; Smulders, Y.M.; van Guldener, C.; Jakobs, C.; Stehouwer, C.D.; de Meer, K. Folic acid treatment increases homocysteine remethylation and methionine transmethylation in healthy subjects. Clin. Sci. 2005, 108, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaric, B.L.; Obradovic, M.; Bajic, V.; Haidara, M.A.; Jovanovic, M.; Isenovic, E.R. Homocysteine and Hyperhomocysteinaemia. Curr. Med. Chem. 2019, 26, 2948–2961. [Google Scholar] [CrossRef] [PubMed]
- Hannibal, L.; Blom, H.J. Homocysteine and disease: Causal associations or epiphenomenons? Mol. Asp. Med. 2017, 53, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Nazki, F.H.; Sameer, A.S.; Ganaie, B.A. Folate: Metabolism, genes, polymorphisms and the associated diseases. Gene 2014, 533, 11–20. [Google Scholar] [CrossRef]
- Wright, A.J.; Dainty, J.R.; Finglas, P.M. Folic acid metabolism in human subjects revisited: Potential implications for proposed mandatory folic acid fortification in the UK. Br. J. Nutr. 2007, 98, 667–675. [Google Scholar] [CrossRef]
- Danese, S.; Sgambato, A.; Papa, A.; Scaldaferri, F.; Pola, R.; Sans, M.; Lovecchio, M.; Gasbarrini, G.; Cittadini, A.; Gasbarrini, A. Homocysteine triggers mucosal microvascular activation in inflammatory bowel disease. Am. J. Gastroenterol. 2005, 100, 886–895. [Google Scholar] [CrossRef]
- Ma, F.; Wu, T.; Zhao, J.; Song, A.; Liu, H.; Xu, W.; Huang, G. Folic acid supplementation improves cognitive function by reducing the levels of peripheral inflammatory cytokines in elderly Chinese subjects with MCI. Sci. Rep. 2016, 6, 37486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asbaghi, O.; Ghanavati, M.; Ashtary-Larky, D.; Bagheri, R.; Rezaei Kelishadi, M.; Nazarian, B.; Nordvall, M.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Oxidative Stress Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2021, 10, 871. [Google Scholar] [CrossRef] [PubMed]
- Bleie, O.; Semb, A.G.; Grundt, H.; Nordrehaug, J.E.; Vollset, S.E.; Ueland, P.M.; Nilsen, D.W.; Bakken, A.M.; Refsum, H.; Nygard, O.K. Homocysteine-Lowering therapy does not affect inflammatory markers of atherosclerosis in patients with stable coronary artery disease. J. Intern. Med. 2007, 262, 244–253. [Google Scholar] [CrossRef]
- Nagar, H.; Jung, S.B.; Ryu, M.J.; Choi, S.J.; Piao, S.; Song, H.J.; Kang, S.K.; Shin, N.; Kim, D.W.; Jin, S.A.; et al. CR6-Interacting Factor 1 Deficiency Impairs Vascular Function by Inhibiting the Sirt1-Endothelial Nitric Oxide Synthase Pathway. Antioxid. Redox Signal. 2017, 27, 234–249. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.; Piao, S.; Kim, S.; Nagar, H.; Choi, S.-J.; Jeon, B.H.; Oh, S.-H.; Irani, K.; Kim, C.-S. CRIF1 Deficiency Increased Homocysteine Production by Disrupting Dihydrofolate Reductase Expression in Vascular Endothelial Cells. Antioxidants 2021, 10, 1645. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10111645
Lee I, Piao S, Kim S, Nagar H, Choi S-J, Jeon BH, Oh S-H, Irani K, Kim C-S. CRIF1 Deficiency Increased Homocysteine Production by Disrupting Dihydrofolate Reductase Expression in Vascular Endothelial Cells. Antioxidants. 2021; 10(11):1645. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10111645
Chicago/Turabian StyleLee, Ikjun, Shuyu Piao, Seonhee Kim, Harsha Nagar, Su-Jeong Choi, Byeong Hwa Jeon, Sang-Ha Oh, Kaikobad Irani, and Cuk-Seong Kim. 2021. "CRIF1 Deficiency Increased Homocysteine Production by Disrupting Dihydrofolate Reductase Expression in Vascular Endothelial Cells" Antioxidants 10, no. 11: 1645. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox10111645