
The Prognostic Value of Derivatives-Reactive Oxygen Metabolites (d-ROMs) for Cardiovascular Disease Events and Mortality: A Review

 , , ,
, , ,
Abstract
:1. Introduction
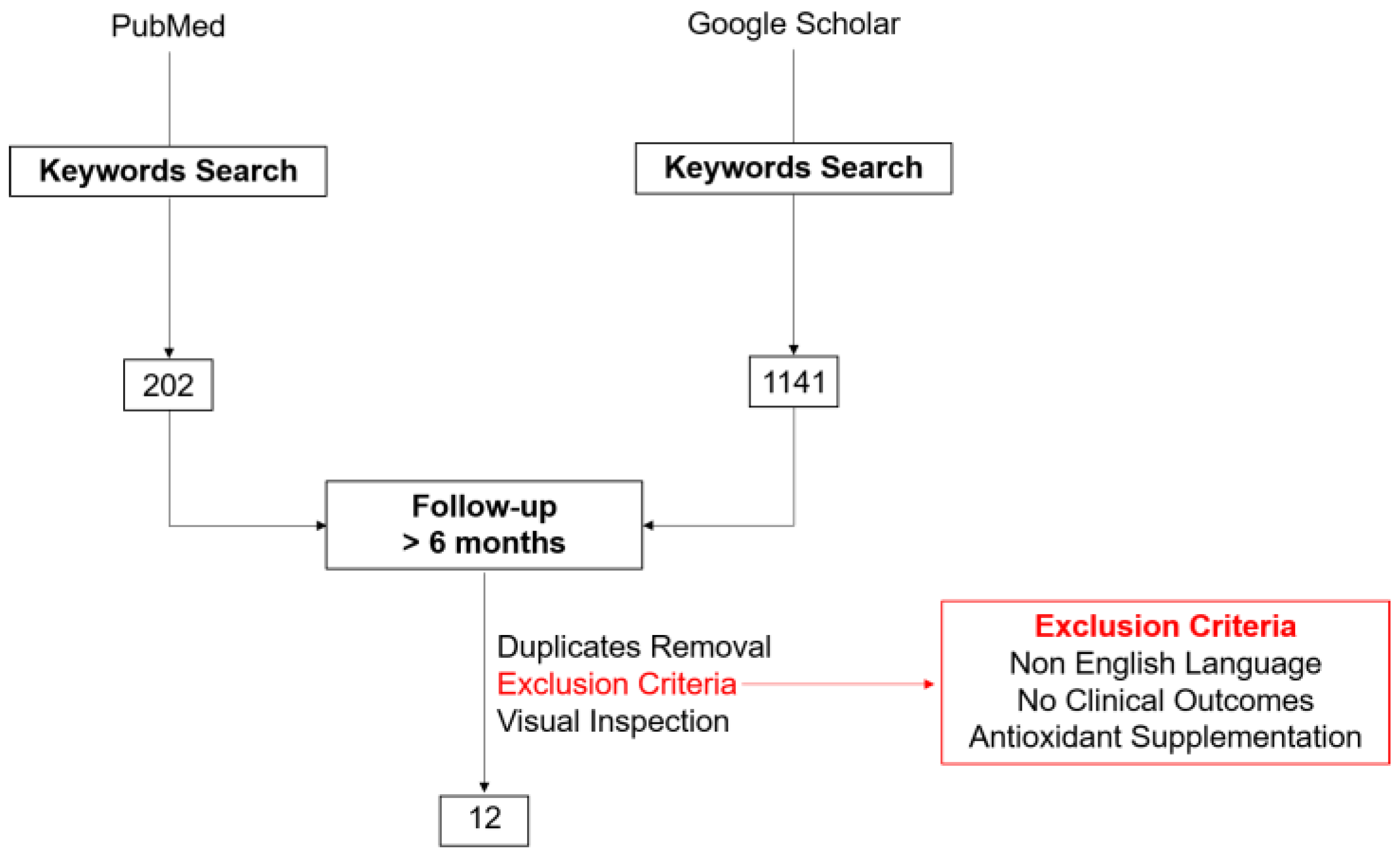
2. Literature Search Methods
3. Reactive Oxygen Species (ROS), Antioxidants, and RedOx Balance
4. Role of Oxidative Stress in the Pathogenesis of Cardiovascular Diseases
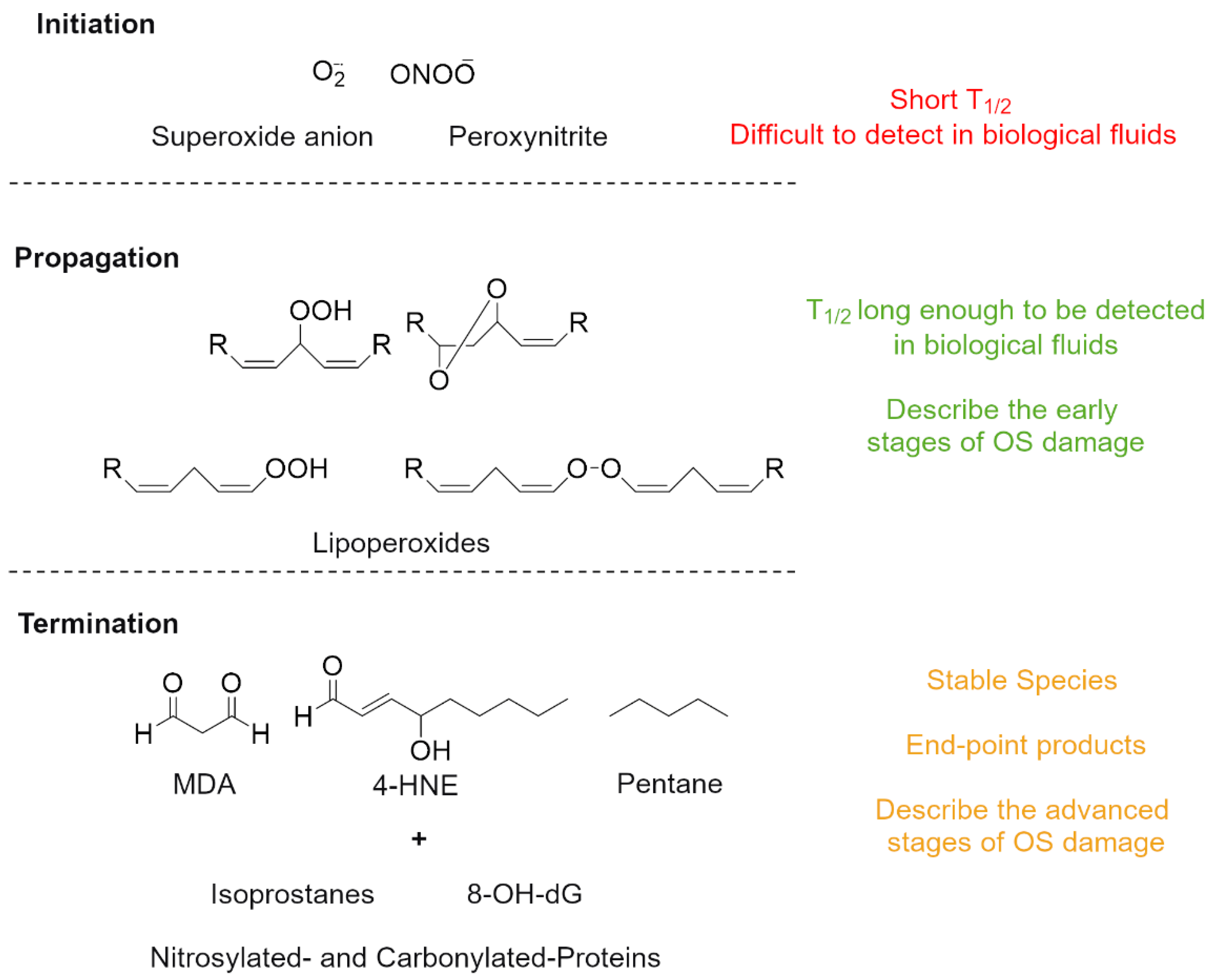
5. Oxidative-Stress Measurement and d-ROMs Test (Peroxide Assay)
6. Relation of d-ROMs to Cardiovascular Risk Factors
7. d-ROM Prognostic Value in Small Cohorts of Individuals with Known Cardiovascular Disease
7.1. d-ROMs in Coronary Artery Disease (CAD)
7.2. d-ROMs in Heart Failure
7.3. d-ROMs in Atrial Fibrillation
8. The d-ROM Prognostic Value in Large General-Population-Based Cohorts
8.1. d-ROMs in Individuals with No History of CVD
8.2. d-ROMs in the General Population
8.3. d-ROMs in Type II Diabetes Mellitus
9. Discussion
9.1. Clinical Perspective
9.2. Limitations
9.3. Future Actions
10. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Margulis, L.; Sagan, D. Microcosmos: Four Billion Years of Evolution from Our Microbial Ancestors; University of California Press: Berkeley, CA, USA, 1997; ISBN 978-0-520-21064-6. [Google Scholar]
- Sies, H.; Jones, D.P. Reactive Oxygen Species (ROS) as Pleiotropic Physiological Signalling Agents. Nat. Rev. Mol. Cell Biol. 2020, 21, 363–383. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative Stress, Aging, and Diseases. Cent. Intell. Agency 2018, 13, 757–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursini, F.; Maiorino, M.; Forman, H.J. Redox Homeostasis: The Golden Mean of Healthy Living. Redox Biol. 2016, 8, 205–215. [Google Scholar] [CrossRef]
- Harman, D. Aging: A Theory Based on Free Radical and Radiation Chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [Green Version]
- Poprac, P.; Jomova, K.; Simunkova, M.; Kollar, V.; Rhodes, C.J.; Valko, M. Targeting Free Radicals in Oxidative Stress-Related Human Diseases. Trends Pharmacol. Sci. 2017, 38, 592–607. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free Radicals and Antioxidants in Normal Physiological Functions and Human Disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef] [PubMed]
- Daiber, A.; Hahad, O.; Andreadou, I.; Steven, S.; Daub, S.; Münzel, T. Redox-Related Biomarkers in Human Cardiovascular Disease—Classical Footprints and Beyond. Redox Biol. 2021, 42, 101875. [Google Scholar] [CrossRef]
- Pignatelli, P.; Menichelli, D.; Pastori, D.; Violi, F. Oxidative Stress and Cardiovascular Disease: New Insights. Kardiol. Pol. 2018, 76, 713–722. [Google Scholar] [CrossRef] [Green Version]
- Rumley, A.G.; Woodward, M.; Rumley, A.; Rumley, J.; Lowe, G.D.O. Plasma Lipid Peroxides: Relationships to Cardiovascular Risk Factors and Prevalent Cardiovascular Disease. QJM 2004, 97, 809–816. [Google Scholar] [CrossRef]
- Antman, E.M.; Loscalzo, J. Precision Medicine in Cardiology. Nat. Rev. Cardiol. 2016, 13, 591–602. [Google Scholar] [CrossRef]
- Sies, H. On the History of Oxidative Stress: Concept and Some Aspects of Current Development. Curr. Opin. Toxicol. 2018, 7, 122–126. [Google Scholar] [CrossRef]
- Vergara, D.; Casadei-Gardini, A.; Giudetti, A.M. Oxidative Molecular Mechanisms Underlying Liver Diseases: From Systems Biology to the Personalized Medicine. Oxidative Med. Cell. Longev. 2019, 2019, 7864316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortese-Krott, M.M.; Koning, A.; Kuhnle, G.G.C.; Nagy, P.; Bianco, C.L.; Pasch, A.; Wink, D.A.; Fukuto, J.M.; Jackson, A.A.; van Goor, H.; et al. The Reactive Species Interactome: Evolutionary Emergence, Biological Significance, and Opportunities for Redox Metabolomics and Personalized Medicine. Antioxid. Redox Signal. 2017, 27, 684–712. [Google Scholar] [CrossRef] [Green Version]
- Alberti, A.; Bolognini, L.; Macciantelli, D.; Caratelli, M. The Radical Cation of N,N-Diethyl-Para-Phenylendiamine: A Possible Indicator of Oxidative Stress in Biological Samples. Res. Chem. Intermed. 2000, 26, 253–267. [Google Scholar] [CrossRef]
- Trotti, R.; Carratelli, M.; Barbieri, M. Performance and Clinical Application of a New, Fast Method for the Detection of Hydroperoxides in Serum. Panminerva Med. 2002, 44, 37–40. [Google Scholar] [PubMed]
- Iamele, L.; Fiocchi, R.; Vernocchi, A. Evaluation of an Automated Spectrophotometric Assay for Reactive Oxygen Metabolites in Serum. Clin. Chem. Lab. Med. 2002, 40, 673–676. [Google Scholar] [CrossRef]
- Lubrano, V.; Vassalle, C.; L’Abbate, A.; Zucchelli, G.C. A New Method to Evaluate Oxidative Stress in Humans. Immuno-Anal. Biol. Spéc. 2002, 17, 172–175. [Google Scholar] [CrossRef]
- Verde, V.; Fogliano, V.; Ritieni, A.; Maiani, G.; Morisco, F.; Caporaso, N. Use of N, N -Dimethyl-p-Phenylenediamine to Evaluate the Oxidative Status of Human Plasma. Free. Radic. Res. 2002, 36, 869–873. [Google Scholar] [CrossRef]
- Ridker, P.M. Established and Emerging Plasma Biomarkers in the Prediction of First Atherothrombotic Events. Circulation 2004, 109, IV-6–IV-19. [Google Scholar] [CrossRef] [Green Version]
- Frijhoff, J.; Winyard, P.G.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical Relevance of Biomarkers of Oxidative Stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef] [Green Version]
- Dröge, W. Free Radicals in the Physiological Control of Cell Function. Physiol. Rev. 2002, 82, 47–95. [Google Scholar] [CrossRef] [PubMed]
- D’Autréaux, B.; Toledano, M.B. ROS as Signalling Molecules: Mechanisms That Generate Specificity in ROS Homeostasis. Nat. Rev. Mol. Cell Biol. 2007, 8, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Baros, S.; Valko, M. Redox Active Metal-Induced Oxidative Stress in Biological Systems. Transit. Met. Chem. 2012, 37, 127–134. [Google Scholar] [CrossRef]
- Tsunoda, S.; Kimura, N.; Fujii, J. Oxidative Stress and Redox Regulation of Gametogenesis, Fertilization, and Embryonic Development. Reprod. Med. Biol. 2014, 13, 71–79. [Google Scholar] [CrossRef]
- Emma, R.; Bansal, A.T.; Kolmert, J.; Wheelock, C.E.; Dahlen, S.-E.; Loza, M.J.; De Meulder, B.; Lefaudeux, D.; Auffray, C.; Dahlen, B.; et al. Enhanced Oxidative Stress in Smoking and Ex-Smoking Severe Asthma in the U-BIOPRED Cohort. PLoS ONE 2018, 13, e0203874. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Cederbaum, A. Oxidative Stress and Alcoholic Liver Disease. Semin. Liver Dis. 2009, 29, 141–154. [Google Scholar] [CrossRef]
- Bhardwaj, J.K.; Mittal, M.; Saraf, P.; Kumari, P. Pesticides Induced Oxidative Stress and Female Infertility: A Review. Toxin Rev. 2020, 39, 1–13. [Google Scholar] [CrossRef]
- Aschbacher, K.; Kornfeld, S.; Picard, M.; Puterman, E.; Havel, P.J.; Stanhope, K.; Lustig, R.H.; Epel, E. Chronic Stress Increases Vulnerability to Diet-Related Abdominal Fat, Oxidative Stress, and Metabolic Risk. Psychoneuroendocrinology 2014, 46, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Aseervatham, G.S.B.; Sivasudha, T.; Jeyadevi, R.; Arul Ananth, D. Environmental Factors and Unhealthy Lifestyle Influence Oxidative Stress in Humans—An Overview. Environ. Sci. Pollut. Res. 2013, 20, 4356–4369. [Google Scholar] [CrossRef]
- Halliwell, B.; Gutteridge, J.M.C. The Definition and Measurement of Antioxidants in Biological Systems. Free. Radic. Biol. Med. 1995, 18, 125–126. [Google Scholar] [CrossRef]
- Chuang, C.Y.; Degendorfer, G.; Davies, M.J. Oxidation and Modification of Extracellular Matrix and Its Role in Disease. Free. Radic. Res. 2014, 48, 970–989. [Google Scholar] [CrossRef] [PubMed]
- Eble, J.A.; de Rezende, F.F. Redox-Relevant Aspects of the Extracellular Matrix and Its Cellular Contacts via Integrins. Antioxid. Redox Signal. 2014, 20, 1977–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, E.; Gori, T.; Münzel, T. Oxidative Stress and Endothelial Dysfunction in Hypertension. Hypertens. Res. 2011, 34, 665–673. [Google Scholar] [CrossRef]
- Madamanchi, N.R.; Vendrov, A.; Runge, M.S. Oxidative Stress and Vascular Disease. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Togliatto, G.; Lombardo, G.; Brizzi, M.F. The Future Challenge of Reactive Oxygen Species (ROS) in Hypertension: From Bench to Bed Side. Int. J. Mol. Sci. 2017, 18, 1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Incalza, M.A.; D’Oria, R.; Natalicchio, A.; Perrini, S.; Laviola, L.; Giorgino, F. Oxidative Stress and Reactive Oxygen Species in Endothelial Dysfunction Associated with Cardiovascular and Metabolic Diseases. Vasc. Pharmacol. 2018, 100, 1–19. [Google Scholar] [CrossRef]
- Lubrano, V.; Balzan, S. LOX-1 and ROS, Inseparable Factors in the Process of Endothelial Damage. Free. Radic. Res. 2014, 48, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.-L.; Shi, Y.-H.; Hao, G.; Li, W.; Le, G.-W. Increasing Oxidative Stress with Progressive Hyperlipidemia in Human: Relation between Malondialdehyde and Atherogenic Index. J. Clin. Biochem. Nutr. 2008, 43, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Dikalov, S.; Itani, H.; Richmond, B.; Arslanbaeva, L.; Vergeade, A.; Rahman, S.M.J.; Boutaud, O.; Blackwell, T.; Massion, P.P.; Harrison, D.G.; et al. Tobacco Smoking Induces Cardiovascular Mitochondrial Oxidative Stress, Promotes Endothelial Dysfunction, and Enhances Hypertension. Am. J. Physiol-Heart Circ. Physiol. 2019, 316, H639–H646. [Google Scholar] [CrossRef]
- Dimmeler, S.; Zeiher, A.M. Nitric Oxide–an Endothelial Cell Survival Factor. Cell Death Differ. 1999, 6, 964–968. [Google Scholar] [CrossRef] [Green Version]
- Mitra, S.; Goyal, T.; Mehta, J.L. Oxidized LDL, LOX-1 and Atherosclerosis. Cardiovasc. Drugs Ther. 2011, 25, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Lauer, T.; Preik, M.; Rassaf, T.; Strauer, B.E.; Deussen, A.; Feelisch, M.; Kelm, M. Plasma Nitrite Rather than Nitrate Reflects Regional Endothelial Nitric Oxide Synthase Activity but Lacks Intrinsic Vasodilator Action. Proc. Natl. Acad. Sci. USA 2001, 98, 12814–12819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuchi, C.; Tritto, I.; Carluccio, E.; Mattei, C.; Cattadori, G.; Ambrosio, G. Role of Endothelial Dysfunction in Heart Failure. Heart Fail. Rev. 2020, 25, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Fulton, D. Post-Translational Regulation of Endothelial Nitric Oxide Synthase in Vascular Endothelium. Front. Physiol. 2013, 4, 347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potje, S.R.; Grando, M.D.; Chignalia, A.Z.; Antoniali, C.; Bendhack, L.M. Reduced Caveolae Density in Arteries of SHR Contributes to Endothelial Dysfunction and ROS Production. Sci. Rep. 2019, 9, 6696. [Google Scholar] [CrossRef]
- Kattoor, A.J.; Kanuri, S.H.; Mehta, J.L. Role of Ox-LDL and LOX-1 in Atherogenesis. Curr. Med. Chem. 2019, 26, 1693–1700. [Google Scholar] [CrossRef]
- Kattoor, A.J.; Goel, A.; Mehta, J.L. LOX-1: Regulation, Signaling and Its Role in Atherosclerosis. Antioxidants 2019, 8, 218. [Google Scholar] [CrossRef] [Green Version]
- Ferrario, C.M.; Smith, R.; Levy, P.; Strawn, W. The Hypertension-Lipid Connection: Insights into the Relation between Angiotensin II and Cholesterol in Atherogenesis. Am. J. Med. Sci. 2002, 323, 17–24. [Google Scholar] [CrossRef]
- Lu, J.; Mitra, S.; Wang, X.; Khaidakov, M.; Mehta, J.L. Oxidative Stress and Lectin-Like Ox-LDL-Receptor LOX-1 in Atherogenesis and Tumorigenesis. Antioxid. Redox Signal. 2011, 15, 2301–2333. [Google Scholar] [CrossRef]
- Dey, S.; DeMazumder, D.; Sidor, A.; Foster, D.B.; O’Rourke, B. Mitochondrial ROS Drive Sudden Cardiac Death and Chronic Proteome Remodeling in Heart Failure. Circ. Res. 2018, 123, 356–371. [Google Scholar] [CrossRef]
- Kopáni, M.; Celec, P.; Danišovič, L.; Michalka, P.; Biró, C. Oxidative Stress and Electron Spin Resonance. Clin. Chim. Acta 2006, 364, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Grotto, D.; Maria, L.S.; Valentini, J.; Paniz, C.; Schmitt, G.; Garcia, S.C.; Pomblum, V.J.; Rocha, J.B.T.; Farina, M. Importance of the Lipid Peroxidation Biomarkers and Methodological Aspects FOR Malondialdehyde Quantification. Quím. Nova 2009, 32, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Montuschi, P.; Barnes, P.J.; Roberts, L.J. Isoprostanes: Markers and Mediators of Oxidative Stress. FASEB J. 2004, 18, 1791–1800. [Google Scholar] [CrossRef] [PubMed]
- Zarkovic, N. 4-Hydroxynonenal as a Bioactive Marker of Pathophysiological Processes. Mol. Asp. Med. 2003, 24, 281–291. [Google Scholar] [CrossRef]
- Aghdassi, E.; Allard, J.P. Breath Alkanes as a Marker of Oxidative Stress in Different Clinical Conditions. Free. Radic. Biol. Med. 2000, 28, 880–886. [Google Scholar] [CrossRef]
- Paredi, P.; Kharitonov, S.A.; Leak, D.; Ward, S.; Cramer, D.; Barnes, P.J. Exhaled Ethane, a Marker of Lipid Peroxidation, Is Elevated in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2000, 162, 369–373. [Google Scholar] [CrossRef]
- Kasai, H.; Kawai, K.; Li, Y. Analysis of 8-OH-DG and 8-OH-Gua as Biomarkers of Oxidative Stress. Genes Environ. 2008, 30, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, Y.J.; Carini, M.; Butterfield, D.A. Protein Carbonylation. Antioxid. Redox Signal. 2010, 12, 323–325. [Google Scholar] [CrossRef]
- Yin, H.; Xu, L.; Porter, N.A. Free Radical Lipid Peroxidation: Mechanisms and Analysis. Chem. Rev. 2011, 111, 5944–5972. [Google Scholar] [CrossRef]
- Niki, E.; Yoshida, Y.; Saito, Y.; Noguchi, N. Lipid Peroxidation: Mechanisms, Inhibition, and Biological Effects. Biochem. Biophys. Res. Commun. 2005, 338, 668–676. [Google Scholar] [CrossRef]
- Laguerre, M.; Bily, A.; Roller, M.; Birtić, S. Mass Transport Phenomena in Lipid Oxidation and Antioxidation. Annu. Rev. Food Sci. Technol. 2017, 8, 391–411. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Roede, J.R.; Dikalov, S.; Miller, N.G.; Dudley, S.C.; Quyyumi, A.; Jones, D.P. Determination of Ebselen-Sensitive Reactive Oxygen Metabolites (EbROM) in Human Serum Based upon N,N’-Diethyl-1,4-Phenylenediamine Oxidation. Clin. Chim. Acta 2012, 414, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalleri, A.; Colombo, C.; Venturelli, E.; Miceli, R.; Mariani, L.; Cornelli, U.; Pala, V.; Berrino, F.; Secreto, G. Evaluation of Reactive Oxygen Metabolites in Frozen Serum Samples. Effect of Storage and Repeated Thawing. Int. J. Biol. Markers 2004, 19, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, S.; Lamorgese, A.; Piersantelli, M.; Pagliarani, S.; Benvenuti, F.; Canestrari, F. Oxidative Stress and Antioxidant Status in Patients Undergoing Prolonged Exposure to Hyperbaric Oxygen. Clin. Biochem. 2004, 37, 312–317. [Google Scholar] [CrossRef]
- Fukui, T.; Yamauchi, K.; Maruyama, M.; Yasuda, T.; Kohno, M.; Abe, Y. Significance of Measuring Oxidative Stress in Lifestyle-Related Diseases from the Viewpoint of Correlation between d-ROMs and BAP in Japanese Subjects. Hypertens. Res. 2011, 34, 1041–1045. [Google Scholar] [CrossRef] [Green Version]
- Hirata, Y.; Yamamoto, E.; Tokitsu, T.; Fujisue, K.; Kurokawa, H.; Sugamura, K.; Sakamoto, K.; Tsujita, K.; Tanaka, T.; Kaikita, K.; et al. The Pivotal Role of a Novel Biomarker of Reactive Oxygen Species in Chronic Kidney Disease. Medicine 2015, 94, e1040. [Google Scholar] [CrossRef]
- Schöttker, B.; Brenner, H.; Jansen, E.H.; Gardiner, J.; Peasey, A.; Kubínová, R.; Pająk, A.; Topor-Madry, R.; Tamosiunas, A.; Saum, K.-U.; et al. Evidence for the Free Radical/Oxidative Stress Theory of Ageing from the CHANCES Consortium: A Meta-Analysis of Individual Participant Data. BMC Med. 2015, 13, 300. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, T.; Dohi, Y.; Takase, H.; Yamashita, S.; Tanaka, S.; Kimura, G. Increased Reactive Oxygen Metabolites Is Associated with Cardiovascular Risk Factors and Vascular Endothelial Damage in Middle-Aged Japanese Subjects. Vasc. Health Risk Manag. 2011, 7, 475. [Google Scholar] [CrossRef] [Green Version]
- Dalan, R.; Liew, H.; Goh, L.L.; Gao, X.; Chew, D.E.; Boehm, B.O.; Leow, M.K.S. Evaluation of Oxidative Stress Index and Its Correlation with Traditional Cardiovascular Risk Factors, Inflammation and Carotid Intima Media Thickness in Diabetes and Healthy Subjects. Atherosclerosis 2016, 252, e64. [Google Scholar] [CrossRef]
- Kotani, K.; Tsuzaki, K.; Taniguchi, N.; Sakane, N. Correlation between Reactive Oxygen Metabolites & Atherosclerotic Risk Factors in Patients with Type 2 Diabetes Mellitus. Indian J. Med. Res. 2013, 137, 742–748. [Google Scholar]
- Morandi, A.; Corradi, M.; Orsi, S.; Piona, C.; Zusi, C.; Costantini, S.; Marigliano, M.; Maffeis, C. Oxidative Stress in Youth with Type 1 Diabetes: Not Only a Matter of Gender, Age, and Glycemic Control. Diabetes Res. Clin. Pract. 2021, 179, 109007. [Google Scholar] [CrossRef] [PubMed]
- Hitsumoto, T. Clinical Significance of Cardio-Ankle Vascular Index as a Cardiovascular Risk Factor in Elderly Patients With Type 2 Diabetes Mellitus. J. Clin. Med. Res. 2018, 10, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griendling, K.K.; FitzGerald, G.A. Oxidative Stress and Cardiovascular Injury: Part I: Basic Mechanisms and In Vivo Monitoring of ROS. Circulation 2003, 108, 1912–1916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griendling, K.K.; FitzGerald, G.A. Oxidative Stress and Cardiovascular Injury: Part II: Animal and Human Studies. Circulation 2003, 108, 2034–2040. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.; Griendling, K.K.; Landmesser, U.; Hornig, B.; Drexler, H. Role of Oxidative Stress in Atherosclerosis. Am. J. Cardiol. 2003, 91, 7–11. [Google Scholar] [CrossRef]
- Masaki, N.; Sato, A.; Horii, S.; Kimura, T.; Toya, T.; Yasuda, R.; Namba, T.; Yada, H.; Kawamura, A.; Adachi, T. Usefulness of the D-ROMs Test for Prediction of Cardiovascular Events. Int. J. Cardiol. 2016, 222, 226–232. [Google Scholar] [CrossRef]
- Hirata, Y.; Yamamoto, E.; Tokitsu, T.; Kusaka, H.; Fujisue, K.; Kurokawa, H.; Sugamura, K.; Maeda, H.; Tsujita, K.; Kaikita, K.; et al. Reactive Oxygen Metabolites Are Closely Associated with the Diagnosis and Prognosis of Coronary Artery Disease. J. Am. Heart Assoc. 2015, 4, e001451. [Google Scholar] [CrossRef] [Green Version]
- Vassalle, C.; Bianchi, S.; Bianchi, F.; Landi, P.; Battaglia, D.; Carpeggiani, C. Oxidative Stress as a Predictor of Cardiovascular Events in Coronary Artery Disease Patients. Clin. Chem. Lab. Med. 2012, 50, 1463–1468. [Google Scholar] [CrossRef] [Green Version]
- Vassalle, C.; Boni, C.; Di Cecco, P.; Landi, P. Elevated Hydroperoxide Levels as a Prognostic Predictor of Mortality in a Cohort of Patients with Cardiovascular Disease. Int. J. Cardiol. 2006, 110, 415–416. [Google Scholar] [CrossRef]
- Hirata, Y.; Yamamoto, E.; Tokitsu, T.; Kusaka, H.; Fujisue, K.; Kurokawa, H.; Sugamura, K.; Maeda, H.; Tsujita, K.; Yamamuro, M.; et al. Reactive Oxidative Metabolites Are Associated with the Severity of Heart Failure and Predict Future Cardiovascular Events in Heart Failure with Preserved Left Ventricular Ejection Fraction. Int. J. Cardiol. 2015, 179, 305–308. [Google Scholar] [CrossRef]
- Hitsumoto, T. Efficacy of the Reactive Oxygen Metabolite Test as a Predictor of Initial Heart Failure Hospitalization in Elderly Patients with Chronic Heart Failure. Cardiol. Res. 2018, 9, 153–160. [Google Scholar] [CrossRef]
- Hunt, S.A. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J. Am. Coll. Cardiol. 2005, 46, e1–e82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishihara, T.; Tokitsu, T.; Sueta, D.; Oike, F.; Takae, M.; Fujisue, K.; Usuku, H.; Ito, M.; Kanazawa, H.; Araki, S.; et al. Clinical Significance of Reactive Oxidative Metabolites in Patients with Heart Failure with Reduced Left Ventricular Ejection Fraction. J. Card. Fail. 2021, 27, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Shimano, M.; Shibata, R.; Inden, Y.; Yoshida, N.; Uchikawa, T.; Tsuji, Y.; Murohara, T. Reactive Oxidative Metabolites Are Associated with Atrial Conduction Disturbance in Patients with Atrial Fibrillation. Heart Rhythm. 2009, 6, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Landi, P.; Boni, C.; Zucchelli, G. Oxidative Stress Evaluated Using an Automated Method for Hydroperoxide Estimation in Patients with Coronary Artery Disease. Clin. Chem. Lab. Med. 2007, 45, 367–371. [Google Scholar] [CrossRef]
- Taguchi, I.; Koizumi, S.; Kageyama, M.; Nasuno, T.; Toyoda, S.; Abe, S.; Node, K.; Inoue, T. Risk Markers for Coronary Plaque Progression and Destabilization beyond LDL-Cholesterol in Acute Coronary Syndrome. Int. J. Cardiol. 2014, 173, 329–331. [Google Scholar] [CrossRef]
- Lourenço, A.P.; Leite-Moreira, A.F.; Balligand, J.-L.; Bauersachs, J.; Dawson, D.; de Boer, R.A.; de Windt, L.J.; Falcão-Pires, I.; Fontes-Carvalho, R.; Franz, S.; et al. An Integrative Translational Approach to Study Heart Failure with Preserved Ejection Fraction: A Position Paper from the Working Group on Myocardial Function of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 216–227. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef]
- Neuman, R.B.; Bloom, H.L.; Shukrullah, I.; Darrow, L.A.; Kleinbaum, D.; Jones, D.P.; Dudley, S.C. Oxidative Stress Markers Are Associated with Persistent Atrial Fibrillation. Clin. Chem. 2007, 53, 1652–1657. [Google Scholar] [CrossRef] [Green Version]
- Raum, E.; Rothenbacher, D.; Löw, M.; Stegmaier, C.; Ziegler, H.; Brenner, H. Changes of Cardiovascular Risk Factors and Their Implications in Subsequent Birth Cohorts of Older Adults in Germany: A Life Course Approach. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 809–814. [Google Scholar] [CrossRef]
- Schöttker, B.; Haug, U.; Schomburg, L.; Köhrle, J.; Perna, L.; Müller, H.; Holleczek, B.; Brenner, H. Strong Associations of 25-Hydroxyvitamin D Concentrations with All-Cause, Cardiovascular, Cancer, and Respiratory Disease Mortality in a Large Cohort Study. Am. J. Clin. Nutr. 2013, 97, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Peasey, A.; Bobak, M.; Kubinova, R.; Malyutina, S.; Pajak, A.; Tamosiunas, A.; Pikhart, H.; Nicholson, A.; Marmot, M. Determinants of Cardiovascular Disease and Other Non-Communicable Diseases in Central and Eastern Europe: Rationale and Design of the HAPIEE Study. BMC Public Health 2006, 6, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krämer, H.U.; Raum, E.; Rüter, G.; Schöttker, B.; Rothenbacher, D.; Rosemann, T.; Szecsenyi, J.; Brenner, H. Gender Disparities in Diabetes and Coronary Heart Disease Medication among Patients with Type 2 Diabetes: Results from the DIANA Study. Cardiovasc. Diabetol. 2012, 11, 88. [Google Scholar] [CrossRef] [Green Version]
- Raum, E.; Krämer, H.U.; Rüter, G.; Rothenbacher, D.; Rosemann, T.; Szecsenyi, J.; Brenner, H. Medication Non-Adherence and Poor Glycaemic Control in Patients with Type 2 Diabetes Mellitus. Diabetes Res. Clin. Pract. 2012, 97, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Xuan, Y.; Bobak, M.; Anusruti, A.; Jansen, E.H.J.M.; Pająk, A.; Tamosiunas, A.; Saum, K.-U.; Holleczek, B.; Gao, X.; Brenner, H.; et al. Association of Serum Markers of Oxidative Stress with Myocardial Infarction and Stroke: Pooled Results from Four Large European Cohort Studies. Eur. J. Epidemiol. 2019, 34, 471–481. [Google Scholar] [CrossRef]
- Schöttker, B.; Saum, K.-U.; Jansen, E.H.J.M.; Boffetta, P.; Trichopoulou, A.; Holleczek, B.; Dieffenbach, A.K.; Brenner, H. Oxidative Stress Markers and All-Cause Mortality at Older Age: A Population-Based Cohort Study. J. Gerontol. Ser. A 2015, 70, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Xuan, Y.; Gào, X.; Anusruti, A.; Holleczek, B.; Jansen, E.H.J.M.; Muhlack, D.C.; Brenner, H.; Schöttker, B. Association of Serum Markers of Oxidative Stress with Incident Major Cardiovascular Events, Cancer Incidence, and All-Cause Mortality in Type 2 Diabetes Patients: Pooled Results from Two Cohort Studies. Diabetes Care 2019, 42, 1436–1445. [Google Scholar] [CrossRef]
- Hu, M.L. Measurement of Protein Thiol Groups and Glutathione in Plasma. Methods Enzymol. 1994, 233, 380–385. [Google Scholar] [CrossRef]
- Naruse, R.; Suetsugu, M.; Terasawa, T.; Ito, K.; Hara, K.; Takebayashi, K.; Morita, K.; Aso, Y.; Inukai, T. Oxidative Stress and Antioxidative Potency Are Closely Associated with Diabetic Retinopathy and Nephropathy in Patients with Type 2 Diabetes. Saudi Med. J. 2013, 34, 135–141. [Google Scholar]
- Suys, B.; de Beeck, L.O.; Rooman, R.; Kransfeld, S.; Heuten, H.; Goovaerts, I.; Vrints, C.; de Wolf, D.; Matthys, D.; Manuel-Y-Keenoy, B. Impact of Oxidative Stress on the Endothelial Dysfunction of Children and Adolescents with Type 1 Diabetes Mellitus: Protection by Superoxide Dismutase? Pediatric Res. 2007, 62, 456–461. [Google Scholar] [CrossRef] [Green Version]
- Nourooz-Zadeh, J.; Tajaddini-Sarmadi, J.; McCarthy, S.; Betteridge, D.J.; Wolff, S.P. Elevated Levels of Authentic Plasma Hydroperoxides in NIDDM. Diabetes 1995, 44, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Kohata, Y.; Ohara, M.; Nagaike, H.; Fujikawa, T.; Osaka, N.; Goto, S.; Fukase, A.; Kushima, H.; Hiromura, M.; Terasaki, M.; et al. Association of Hemoglobin A1c, 1,5-Anhydro-d-Glucitol and Glycated Albumin with Oxidative Stress in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study. Diabetes Ther. 2020, 11, 655–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitano, D.; Takayama, T.; Nagashima, K.; Akabane, M.; Okubo, K.; Hiro, T.; Hirayama, A. A Comparative Study of Time-Specific Oxidative Stress after Acute Myocardial Infarction in Patients with and without Diabetes Mellitus. BMC Cardiovasc. Disord. 2016, 16, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohara, M.; Fukui, T.; Ouchi, M.; Watanabe, K.; Suzuki, T.; Yamamoto, S.; Yamamoto, T.; Hayashi, T.; Oba, K.; Hirano, T. Relationship between Daily and Day-to-Day Glycemic Variability and Increased Oxidative Stress in Type 2 Diabetes. Diabetes Res. Clin. Pract. 2016, 122, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohara, M.; Nagaike, H.; Goto, S.; Fukase, A.; Tanabe, Y.; Tomoyasu, M.; Yamamoto, T.; Hayashi, T.; Fukui, T.; Hirano, T. Improvements of Ambient Hyperglycemia and Glycemic Variability Are Associated with Reduction in Oxidative Stress for Patients with Type 2 Diabetes. Diabetes Res. Clin. Pract. 2018, 139, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flammer, A.J.; Anderson, T.; Celermajer, D.S.; Creager, M.A.; Deanfield, J.; Ganz, P.; Hamburg, N.M.; Lüscher, T.F.; Shechter, M.; Taddei, S.; et al. The Assessment of Endothelial Function: From Research Into Clinical Practice. Circulation 2012, 126, 753–767. [Google Scholar] [CrossRef]
- Lupoli, R.; Calcaterra, I.; Annunziata, G.; Tenore, G.; Rainone, C.; Schiavo, L.; Capaldo, B.; Di Minno, M.N.D. Post-Bariatric Hypoglycemia Is Associated with Endothelial Dysfunction and Increased Oxidative Stress. Biomedicines 2022, 10, 916. [Google Scholar] [CrossRef]
- Nusca, A.; Bernardini, F.; Mangiacapra, F.; Maddaloni, E.; Melfi, R.; Ricottini, E.; Piccirillo, F.; Manfrini, S.; Ussia, G.P.; Grigioni, F. Ranolazine Improves Glycemic Variability and Endothelial Function in Patients with Diabetes and Chronic Coronary Syndromes: Results from an Experimental Study. J. Diabetes Res. 2021, 2021, 4952447. [Google Scholar] [CrossRef]
- Sagara, M.; Suzuki, K.; Aoki, C.; Tanaka, S.; Taguchi, I.; Inoue, T.; Aso, Y. Impact of Teneligliptin on Oxidative Stress and Endothelial Function in Type 2 Diabetes Patients with Chronic Kidney Disease: A Case–Control Study. Cardiovasc. Diabetol. 2016, 15, 76. [Google Scholar] [CrossRef] [Green Version]
- Farzadfar, F. Cardiovascular Disease Risk Prediction Models: Challenges and Perspectives. Lancet Glob. Health 2019, 7, e1288–e1289. [Google Scholar] [CrossRef] [Green Version]
- Moons, K.G.M.; Kengne, A.P.; Woodward, M.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Grobbee, D.E. Risk Prediction Models: I. Development, Internal Validation, and Assessing the Incremental Value of a New (Bio)Marker. Heart 2012, 98, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, M.A.; Verweij, N.; van der Harst, P. Associations of Combined Genetic and Lifestyle Risks with Incident Cardiovascular Disease and Diabetes in the UK Biobank Study. JAMA Cardiol. 2018, 3, 693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, C.; Guerra, J.; Slhessarenko, N.; Scartezini, M.; Franca, C.; Colombini, M.; Berlitz, F.; Machado, A.; Campana, G.; Faulhaber, A.; et al. Point-of-Care Testing: General Aspects. J. Clin. Lab. Anal. 2018, 64, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.L.V. Practical Challenges Related to Point of Care Testing. Pract. Lab. Med. 2016, 4, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shephard, M.; Shephard, A.; Matthews, S.; Andrewartha, K. The Benefits and Challenges of Point-of-Care Testing in Rural and Remote Primary Care Settings in Australia. Arch. Pathol. Lab. Med. 2020, 144, 1372–1380. [Google Scholar] [CrossRef]
- Digiesi, V.; Fiorillo, C.; Cosmi, L.; Rossetti, M.; Lenuzza, M.; Guidi, D.; Pace, S.; Rizzuti, G.; Nassi, P. Reactive Oxygen Species and Antioxidant Status in Essential Arterial Hypertension during Therapy with Dihydropyridine Calcium Channel Antagonists. Clin. Ther. 2000, 151, 15–18. [Google Scholar]
- Incandela, L.; Belcaro, G.; Cesarone, M.R.; De Sanctis, M.T.; Griffin, M.; Cacchio, M.; Nicolaides, A.N.; Bucci, M.; Barsotti, A.; Martines, G.; et al. Oxygen-Free Radical Decrease in Hypertensive Patients Treated with Lercanidipine. Int. Angiol. 2001, 20, 136–140. [Google Scholar]
- Taguchi, I.; Toyoda, S.; Takano, K.; Arikawa, T.; Kikuchi, M.; Ogawa, M.; Abe, S.; Node, K.; Inoue, T. Irbesartan, an Angiotensin Receptor Blocker, Exhibits Metabolic, Anti-Inflammatory and Antioxidative Effects in Patients with High-Risk Hypertension. Hypertens. Res. 2013, 36, 608–613. [Google Scholar] [CrossRef]
- Chida, R.; Hisauchi, I.; Toyoda, S.; Kikuchi, M.; Komatsu, T.; Hori, Y.; Nakahara, S.; Sakai, Y.; Inoue, T.; Taguchi, I. Impact of Irbesartan, an Angiotensin Receptor Blocker, on Uric Acid Level and Oxidative Stress in High-Risk Hypertension Patients. Hypertens. Res. 2015, 38, 765–769. [Google Scholar] [CrossRef]
- Toyoda, S.; Haruyama, A.; Inami, S.; Arikawa, T.; Saito, F.; Watanabe, R.; Sakuma, M.; Abe, S.; Nakajima, T.; Tanaka, A.; et al. Effects of Carvedilol vs. Bisoprolol on Inflammation and Oxidative Stress in Patients with Chronic Heart Failure. J. Cardiol. 2020, 75, 140–147. [Google Scholar] [CrossRef]
- Bloom, H.L.; Shukrullah, I.; Veledar, E.; Gutmann, R.; London, B.; Dudley, S.C. Statins Decrease Oxidative Stress and ICD Therapies. Cardiol. Res. Pract. 2010, 2010, 253803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, K.; Kotani, K.; Yagyu, H.; Ando, A.; Osuga, J.; Ishibashi, S. Effects of Treatment with Liraglutide on Oxidative Stress and Cardiac Natriuretic Peptide Levels in Patients with Type 2 Diabetes Mellitus. Endocrine 2014, 47, 962–964. [Google Scholar] [CrossRef] [Green Version]
- Feairheller, D.L.; Park, J.-Y.; Sturgeon, K.M.; Williamson, S.T.; Diaz, K.M.; Veerabhadrappa, P.; Brown, M.D. Racial Differences in Oxidative Stress and Inflammation: In Vitro and In Vivo. Clin. Transl. Sci. 2011, 4, 32–37. [Google Scholar] [CrossRef]
- Kander, M.C.; Cui, Y.; Liu, Z. Gender Difference in Oxidative Stress: A New Look at the Mechanisms for Cardiovascular Diseases. J. Cell. Mol. Med. 2017, 21, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Maffei, S.; Boni, C.; Zucchelli, G.C. Gender-Related Differences in Oxidative Stress Levels among Elderly Patients with Coronary Artery Disease. Fertil. Steril. 2008, 89, 608–613. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Disease | References | Sample Characteristics | Follow-Up | Main Observations | d-ROM Cut-Off Value (UCARR) | ||
|---|---|---|---|---|---|---|---|
| n Age Male/Female | Group Definition Criteria | ||||||
| Coronary Artery Disease (CAD) | Masaki et al., 2016 [77] | All subjects 265 65 ± 13 204/61 | CAD group 130 N/D N/D | CAD: Patients with at least one coronary stenosis proven by coronary angiography or past history of coronary revascularisation | 2.66 ± 1.47 years | d-ROM values above 395 UCARR were associated with an increased risk of all cardiovascular events * and death for any cause. In CAD patients, d-ROM values above 395 UCARR were associated with an increase in all cardiovascular events, MACEs ** and cardiovascular death. * defined as coronary or peripheral revascularisation, cardiovascular surgery, heart failure, and hospitalisation for any cardiovascular cause, in addition to major adverse cardiovascular events (MACEs). ** MACEs defined as death from cardiovascular causes, nonfatal myocardial infarction, and nonfatal cerebral infarction. | 395 |
| Hirata et al., 2015 [78] | CAD group 163 69 ± 10 113/50 | Non-CAD group 163 69 ± 10 113/50 | CAD: Patients with a diameter of stenosis in vessels ≥1.5 mm | Follow-up until the first CVD event or up to 50 months (mean follow-up 20 months) | d-ROM values were significantly higher in risk-factor-matched CAD patients (median = 338 IRQ = 302–386 UCARR) than in risk-factor-matched non-CAD patients (median = 311 IRQ = 282–353 UCARR). Kaplan–Meier analysis showed a higher probability of CVD events in CAD patients with d-ROMs >346 UCARR. Multivariate Cox hazard analysis identified ln-DROM as an independent predictor for CVD events. | 346 | |
| Vassalle et al., 2012 [79] | CAD patients 93 68 ± 10 75/18 | CAD: Patients with angiographically documented CAD | 66 ± 28 months | Kaplan–Meier survival estimates showed a significantly worse outcome in patients presenting elevated d-ROM level (>75th percentile, corresponding to 481 UCARR) for cardiac death, all-cause death, and MACEs. In a multivariate Cox regression model, an elevated oxidative stress remained a significant predictor of cardiac and all-cause death. | 481 | ||
| CVD | Vassalle et al., 2006 [80] | 166 cardiovascular inpatients 66 ± 1 112/45 | Investigated in a clinical cardiology setting | Follow-up for 20 ± 0.3 months | d-ROM values ≥ 482 UCARR (corresponding to the 75th percentile) were a strong and independent predictor of cardiac death and total mortality. | 482 | |
| Heart Failure (HF) | Hirata et al., 2015 [81] | HFpEF group 212 70 ± 9 127/85 | Control Group 212 70 ± 9 136/76 | HFpEF: patients with symptoms of HF or mildly reduced left-ventricular systolic function (LVEF > 50% and left-ventricular end-diastolic volume index <97 mL/m2 and evidence of abnormal left-ventricular diastolic distensibility and stiffness) | Patients followed up to the first CVD events or up to 50 months (mean follow-up 20 months) | d-ROM levels were significantly higher in risk-factor-matched HFpEF patients (median = 343 IRQ = 312–394 UCARR) than in non-HF controls (median = 336 IRQ = 288–381 UCARR). Authors used median value of d-ROMs (346 UCARR) to divide HFpEF patients into low- and high-d-ROM groups. Total CVD events and hospitalisation for HF were significantly higher in high-d-ROM group than in low-d-ROM group. Kaplan–Meier analysis demonstrated a significantly higher probability of CVD events in HFpEF patients with high-d-ROMs than in those with low-d-ROMs. | 346 |
| Hitsumoto et al., 2018 [82] | Patients with chronic heart failure (CHF) | 81 months (range, 6–120 months) | The mean value for Low d-ROM group was 235 ± 45 UCARR and for High d-ROM group was 421 ± 81 UCARR Multivariate Cox regression analysis revealed that the High d-ROM group exhibited a significantly higher risk for HF hospitalisation than Low d-ROM group. 319 UCARR was considered as best value for discriminating between non-hospitalisation and hospitalisation for HF during follow up. | 319 | |||
| L group (d-ROMs < 303 UCARR) 214 74 ± 6 58/156 | H group (d-ROMs > 303 UCARR) 214 76 ± 8 50/164 | CHF was defined according to the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults [83] | |||||
| Nishihara et al., 2021 [84] | Patients with HFrEF (201) and without HF (241) | HFrEF: patients with Framingham criteria for congestive HF with left-ventricular ejection fraction <50%, in stable conditions after optimal medical therapy | mean follow-up 638 days (IQR, 301–1173 days) | d-ROM levels were significantly higher in HFrEF patients (median = 344 IRQ = 297–390 UCARR) than in risk-factor-matched non-HF controls (median = 323 IRQ = 282–366 UCARR) Authors used median value of d-ROMs (353 UCARR) to divide HFrEF patients into low- and high-d-ROM groups. Total CVD events and hospitalisation for HF were significantly higher in high-d-ROM group than in low-d-ROMs group. Kaplan–Meier analysis demonstrated a significantly higher probability of HF-related events in HFrEF patients with high-d-ROMs than in those with low-d-ROMs. | 353 | ||
| L group (d-ROMs < 353 UCARR) 100 69.2 ± 9.7 100/201 | H group (d-ROMs > 353 UCARR) 101 69.2 ± 9.7 101/201 | ||||||
| Atrial Fibrillation (AF) | Shimano et al., 2009 [85] | Paroxysmal AF group 225 59 ± 11 162/63 | Persistent AF group 81 59 ± 12 64/17 | Patients with paroxysmal AF or persistent AF admitted for elective radiofrequency (RF) catheter ablation. Patients undergoing haemodialysis and those with structural heart disease were excluded. | 1.2 ± 0.8 years | d-ROM levels in patients with persistent AF (341 ± 85 UCARR) were significantly higher than in patients with paroxysmal AF (305 ± 78 UCARR). Kaplan–Meier analysis revealed that the highest quartile of basal d-ROM levels (>355 UCARR), but not within the highest quartile of hs-CRP levels (>1.20 mg/L), exhibited a significantly higher AF recurrence rate after radiofrequency catheter ablation, in the paroxysmal AF group. | 355 |
| References | Sample | Follow Up | Main Observations |
|---|---|---|---|
| n Age Male/Female | |||
| XUAN et al., 2019 [96] | MI group 476 cases (age median = 64 IRQ = 58–69, 334 males and 142 females); 2380 controls (age median = 64 IRQ = 58–69, 1680 males and 700 females) Stroke group 454 cases (age median = 66 IRQ = 61–70, 239 males and 215 females); 2270 controls (age median = 66 IRQ = 61–69, 1195 males and 1075 females) | 8 years | d-ROM levels were statistically significantly higher among MI cases than controls, and d-ROM levels were statistically significantly associated with total MI incidence. A strong 5-fold increased risk of fatal MI was observed for d-ROM values > 500 UCARR. d-ROM levels were associated with both MI (OR = 1.21; 95% CI = 1.05–1.40; for 100 UCARR increase) and stroke incidence (OR = 1.17; 95% CI = 1.01–1.35; for 100 UCARR increase). The observed relationships were stronger with fatal than with nonfatal endpoints. |
| SCHÖTTKER et al., 2015 [97] | 2932 70 ± 6 1321/1611 | 3.3 ± 0.7 years | The top tertile of d-ROM levels (>381 UCARR), compared with the bottom tertile, was associated with all-cause mortality, in models adjusted for age, sex, education, smoking, physical activity, and alcohol consumption. |
| SCHÖTTKER et al., 2015 [68] | 1702 cases of death and 8310 controls divided in 4 cohorts age range: 45–85 years male% range cases: 59–68 male% range controls: 43–68 | from 6 to 8 years | d-ROMs were significantly associated with all-cause mortality independently from established risk factors (including inflammation). Regarding cause-specific mortality, compared to low d-ROM levels (≤340 UCARR), very high d-ROM levels (>500 UCARR) were strongly associated with both cardiovascular (relative risk (RR), 5.09; 95% CI, 2.67–9.69) and cancer mortality (RR, 4.34; 95% CI, 2.31–8.16). |
| XUAN et al., 2019 [98] | 2125 patients with T2DM from ESTHER and DIANA cohorts. In total, 205, 179, and 394 MCE #, cancer, and all-cause mortality cases were observed. ESTHER: 1029 (535males, 494 females) DIANA: 1096 (600 males, 496 females) | from 6 to 7 years | An increase in d-ROM levels corresponded to an increased risk of all-cause mortality, in particular in T2DM males with previous medical history of CAD. However, only high d-ROM-to-TTL ratios were statistically significantly associated with both an increased all-cause mortality (d-ROMs-to-TTL ratio top tertile; HR 2.50, 95% CI = 1.86–3.36; p < 0.05) and incidence of major cardiovascular events (d-ROMs-to-TTL ratio top tertile; HR 1.65, 95% CI = 1.07–2.54; p < 0.05). |
| Chapter | References | Hazard Ratio (HR), Odds Ratio (OR) or Risk Ratio (RR) (Confidence Interval 95%) | Event | Population Size | d-ROM Cut-Off (UCARR) |
|---|---|---|---|---|---|
| d-ROM prognostic value in small cohorts of individuals with known CVD | Masaki et al., 2016 [77] | (HR) 3.755 (1.108–12.730), p = 0.034 | CVD events | 265 | 395 |
| Hirata et al., 2015 [78] | (HR) 10.8 (2.76–42.4), p = 0.001 | CVD events | 395 | 346 | |
| Vassalle et al., 2006 [80] | (OR) 8.6 (1.5–50.2), p = 0.016 | Cardiac death | 166 | 482 | |
| Vassalle et al., 2012 [79] | (HR) 3.9 (1.4–11.1), p < 0.01 | Cardiac death, MACEs, all-cause death | 93 | 481 | |
| Hirata et al., 2015 [81] | (HR) 14.3 (4.19–49.1), p < 0.001 | CVD events | 287 | 346 | |
| Nishihara et al., 2021 [84] | (HR) 1.01 (1.001–1.009), p = 0.02 | CVD events and HF-related events | 201 | 353 | |
| Hitsumoto et al., 2018 [82] | (HR) 2.35 (1.37–4.43), p < 0.01 | Heart failure hospitalisation | 428 | 319 | |
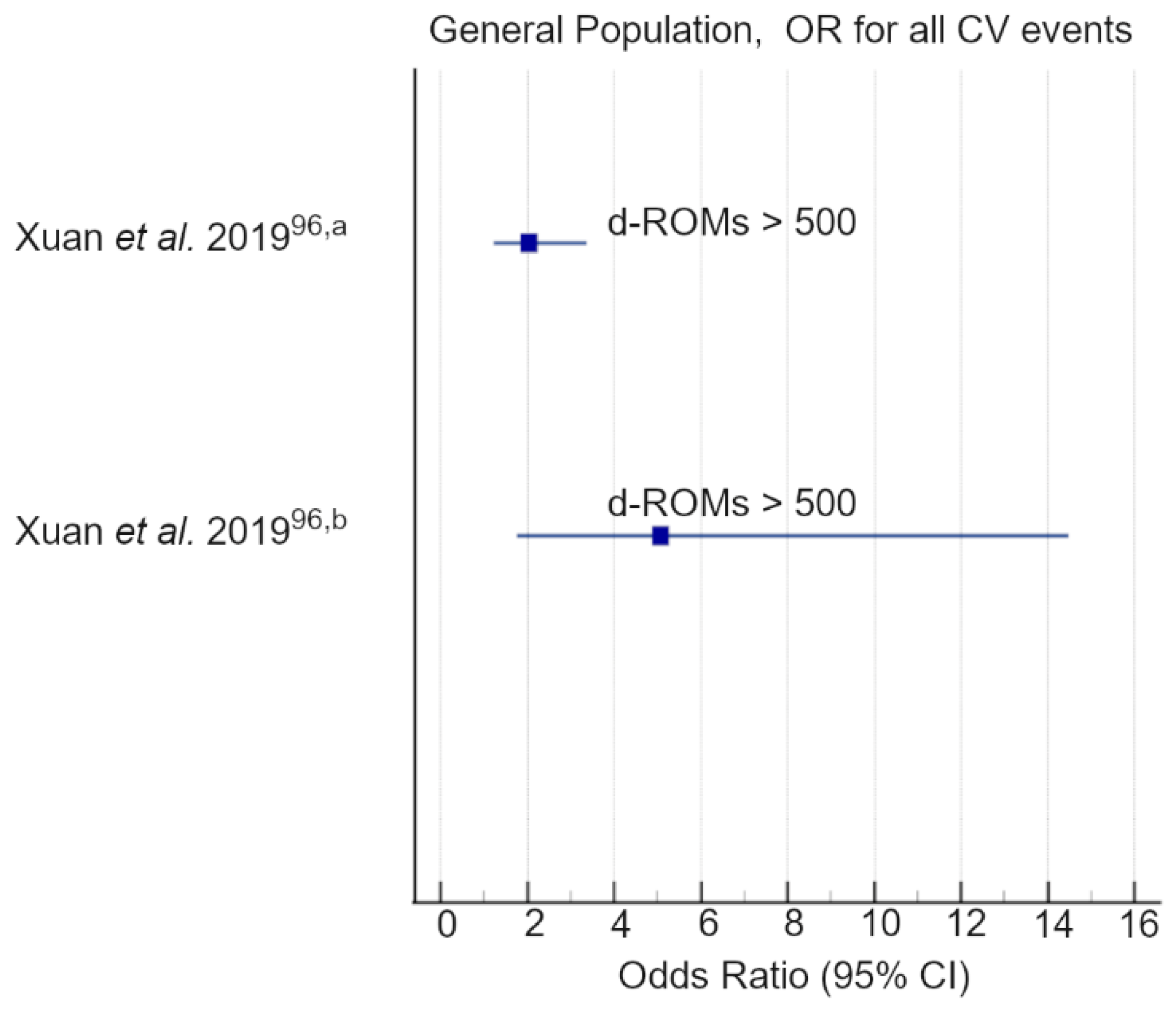
| d-ROM prognostic value in general population-based cohorts | Xuan et al., 2019 [96] | (OR) 2.04 (1.23; 3.37), p < 0.05 | Myocardial infarction (MI) | 2856 | 500 |
| (OR) 5.08 (1.78; 14.49), p < 0.05 | fatal MI | 500 | |||
| (OR) 1.21 (1.05–1.40), p < 0.05 | MI odds ratio for 100 UCARR increase | - | |||
| (OR) 1.17 (1.01–1.35), p < 0.05 | Stroke odds ratio for 100 UCARR increase | - | |||
| Schöttker et al., 2015 [97] | (HR) 1.63 (1.01; 2.63), p < 0.05 | All-cause death | 2932 | 381 | |
| (HR) 1.33 (1.04; 1.70), p < 0.05 | All-cause death per 100 UCARR increase | - | |||
| Schöttker et al., 2015 [68] | (RR) 1.32 (1.10–1.59), p < 0.05 | All-cause mortality | 10,012 | 401–500 | |
| (RR) 2.30 (1.40–3.77), p < 0.05 | >500 | ||||
| (RR) 1.49 (1.04–2.13), p < 0.05 | Cardiovascular mortality | 401–500 | |||
| (RR) 4.34 (2.06–9.15) p < 0.05 | >500 | ||||
| Xuan et al., 2019 [98] | (HR) 1.67 (1.05–2.67), p < 0.05 | All-cause mortality | 1029 * | 368 | |
| (HR) 2.49 (1.74–3.55) p < 0.05 | 1096 ** | 450 | |||
| (HR §) 2.50 (1.86–3.36), p < 0.05 | All-cause mortality | 2125 *** | - | ||
| (HR §) 1.65 (1.07–2.54), p < 0.05 | MCE # | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pigazzani, F.; Gorni, D.; Dyar, K.A.; Pedrelli, M.; Kennedy, G.; Costantino, G.; Bruno, A.; Mackenzie, I.; MacDonald, T.M.; Tietge, U.J.F.; et al. The Prognostic Value of Derivatives-Reactive Oxygen Metabolites (d-ROMs) for Cardiovascular Disease Events and Mortality: A Review. Antioxidants 2022, 11, 1541. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox11081541
Pigazzani F, Gorni D, Dyar KA, Pedrelli M, Kennedy G, Costantino G, Bruno A, Mackenzie I, MacDonald TM, Tietge UJF, et al. The Prognostic Value of Derivatives-Reactive Oxygen Metabolites (d-ROMs) for Cardiovascular Disease Events and Mortality: A Review. Antioxidants. 2022; 11(8):1541. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox11081541
Chicago/Turabian StylePigazzani, Filippo, Davide Gorni, Kenneth A. Dyar, Matteo Pedrelli, Gwen Kennedy, Gabriele Costantino, Agostino Bruno, Isla Mackenzie, Thomas M. MacDonald, Uwe J. F. Tietge, and et al. 2022. "The Prognostic Value of Derivatives-Reactive Oxygen Metabolites (d-ROMs) for Cardiovascular Disease Events and Mortality: A Review" Antioxidants 11, no. 8: 1541. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox11081541