Coenzyme Q10 Treatment Monitoring in Different Human Biological Samples

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. CoQ Treatment Protocol
2.3. Samples
- Blood samples: Ethylenediamine tetraacetic acid (EDTA) blood samples were drawn to separate BMCs, platelets, and plasma. Platelet-rich plasma (PRP) was obtained by centrifugation (60× g, 15 min, room temperature), as previously reported [16]. The PRP was then centrifuged (965× g, 20 min, room temperature) to pellet the platelets. The platelet count was analyzed in an ADVIA 2120 hematology analyzer (Siemens Healthineers, Erlangen, Germany). For BMCs isolation, the Histopaque 1077 procedure was used, as previously reported [17]. The plasma samples were separated by centrifugation (1500× g, 10 min, 4 °C). All the blood-derived samples were stored at −80 °C until CoQ analysis.
- Urine samples: The first morning urine samples were collected in standard urine containers. After centrifugation (1500× g, 10 min, 4 °C), the urinary pellet was washed with 9 mg/mL saline solution and then centrifuged as before to remove urinary proteins. The urinary pellet was stored frozen at −80 °C until CoQ analysis. The details of this procedure are reported elsewhere [18].
- Muscle samples: skeletal muscle samples were collected from the vastus lateralis muscle by vacuum-assisted biopsy. The muscle was weighed and homogenized with cold SETH buffer in an ice bath. The mixture was then vortexed, sonicated, and transferred to a polypropylene tube, followed by vortexing for 2 min, sonication for 5 min, and centrifugation (1500× g, 10 min, 4 °C). The supernatant was frozen at −80 °C until CoQ analysis.
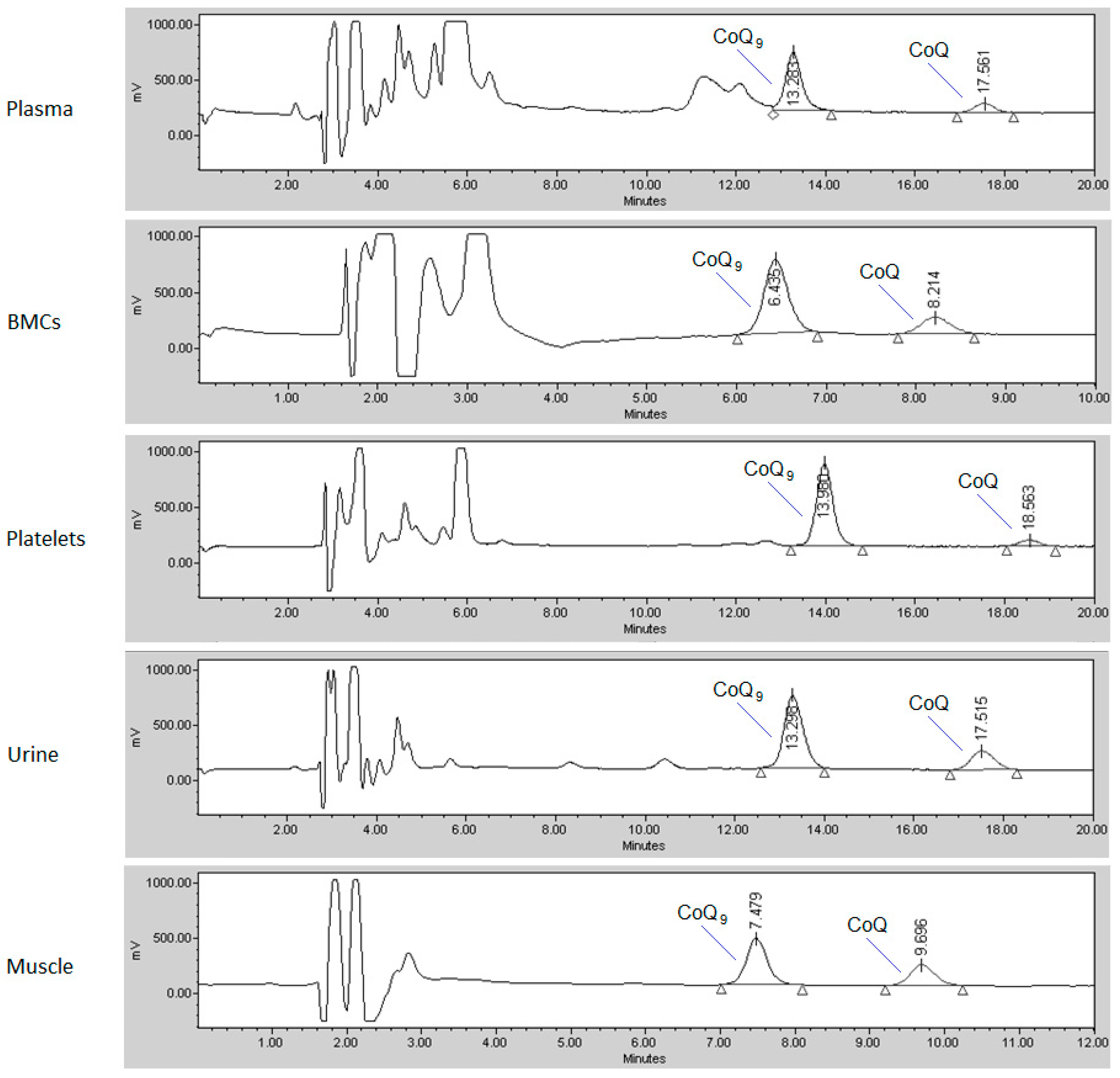
2.4. CoQ Determination
2.5. Ethical Issues
2.6. Statistical Analysis
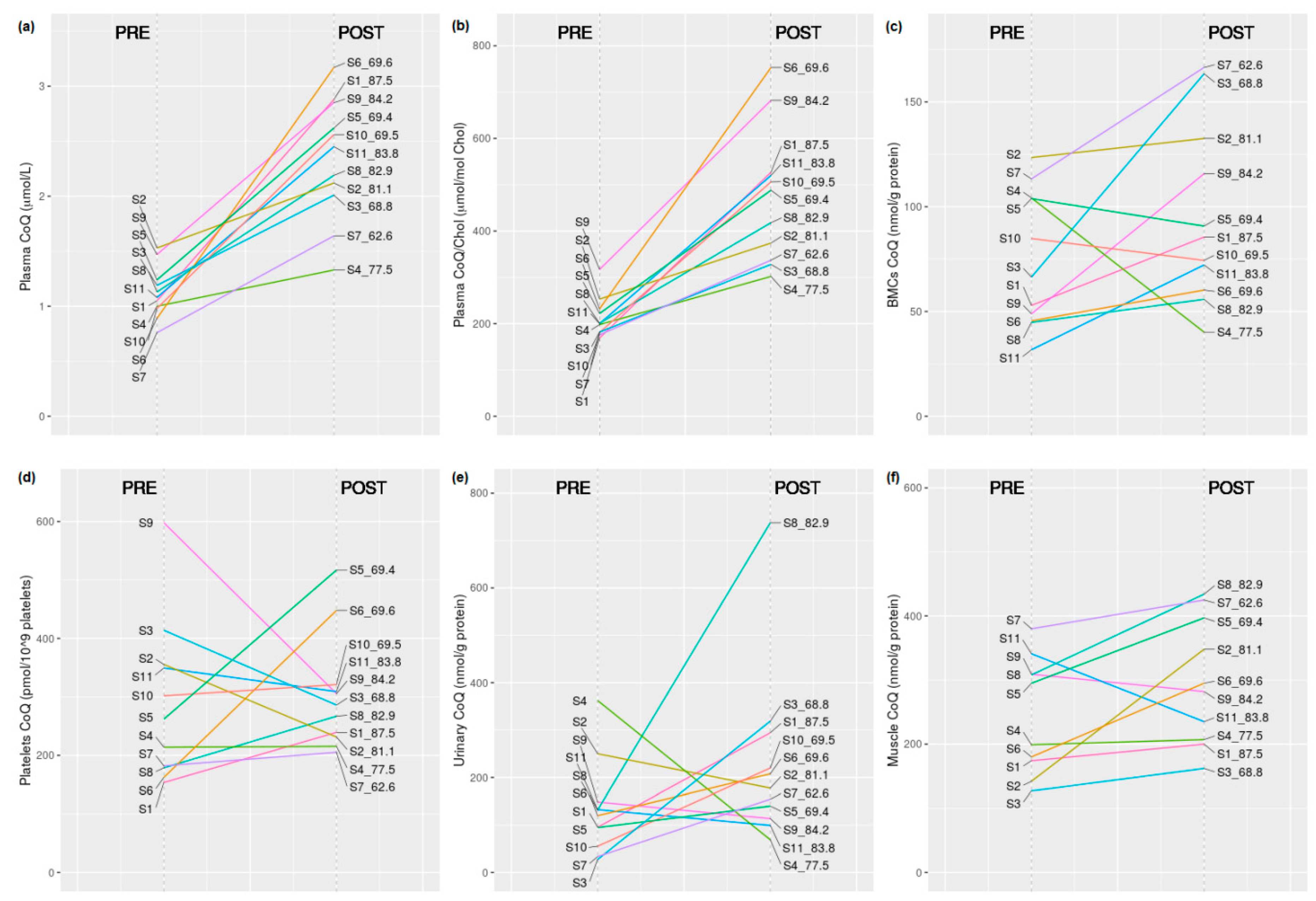
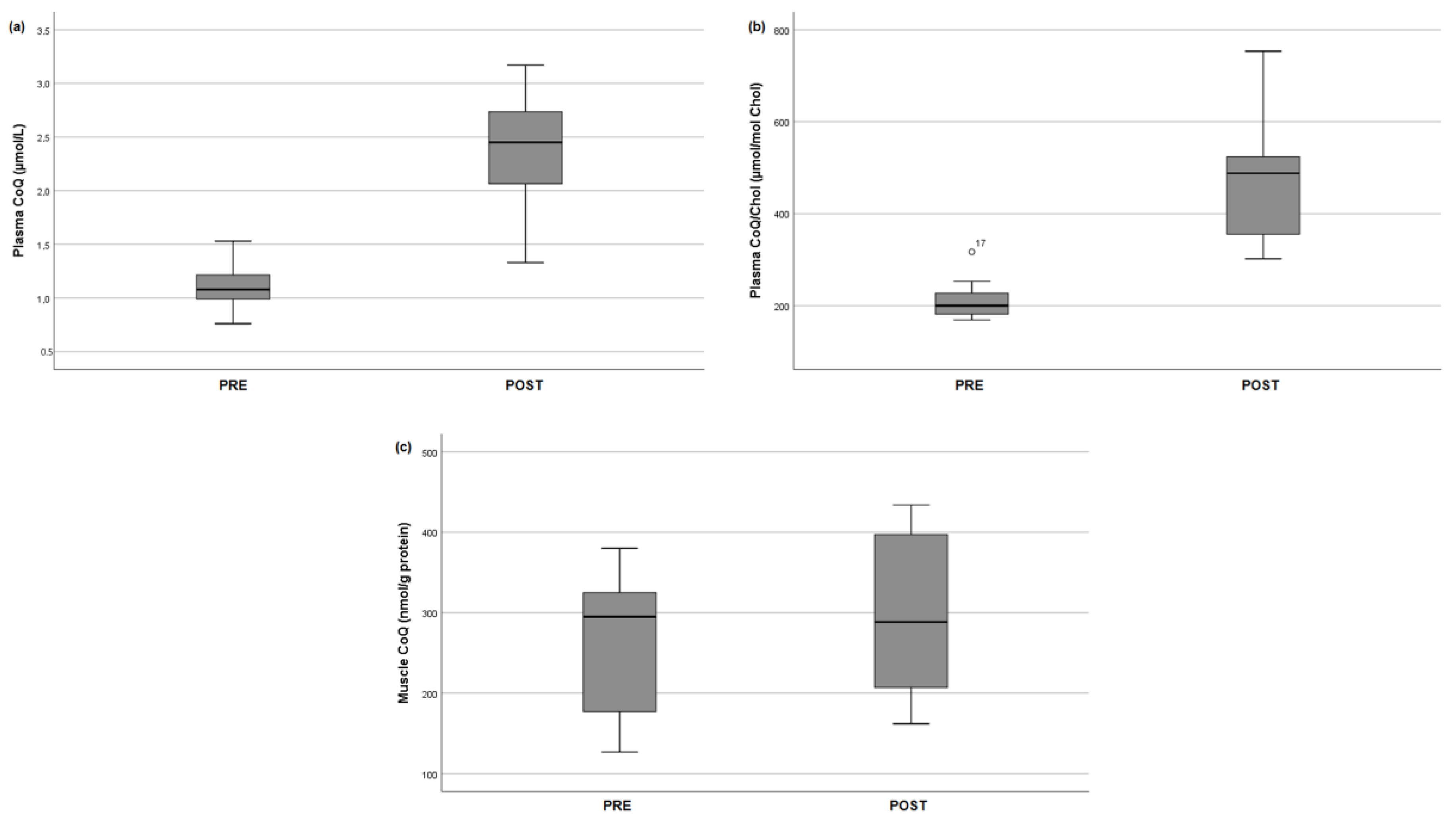
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weber, C.; Bysted, A.; Hølmer, G. Coenzyme Q10 in the diet-daily intake and relative bioavailability. Mol. Asp. Med. 1997, 18, S251–S254. [Google Scholar] [CrossRef]
- Turunen, M.; Olsson, J.; Dallner, G. Metabolism and function of coenzyme Q. Biochim. Biophys. Acta 2004, 1660, 171–199. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Aguilera, J.; Cortés, A.; Fernández-Ayala, D.; Navas, P. Biochemical assessment of coenzyme Q10 deficiency. J. Clin. Med. 2017, 6, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcázar-Fabra, M.; Trevisson, E.; Brea-Calvo, G. Clinical syndromes associated with coenzyme Q10 deficiency. Essays Biochem. 2018, 62, 377–398. [Google Scholar] [CrossRef] [PubMed]
- Desbats, M.A.; Lunardi, G.; Doimo, M.; Trevisson, E.; Salviati, L. Genetic bases and clinical manifestations of coenzyme Q10 (CoQ10) deficiency. J. Inherit. Metab. Dis. 2014, 38, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Yubero, D.; Allen, G.; Artuch, R.; Montero, R. The value of coenzyme Q10 determination in mitochondrial patients. J. Clin. Med. 2017, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- López-Lluch, G.; del Pozo-Cruz, J.; Sánchez-Cuesta, A.; Cortés-Rodríguez, A.B.; Navas, P. Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition 2019, 57, 133–140. [Google Scholar] [CrossRef]
- Cooke, M.; Iosia, M.; Buford, T.; Shelmadine, B.; Hudson, G.; Kerksick, C.; Rasmussen, C.; Greenwood, M.; Leutholtz, B.; Willoughby, D.; et al. Effects of acute and 14-day coenzyme Q10 supplementation on exercise performance in both trained and untrained individuals. J. Int. Soc. Sports Nutr. 2008, 5. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Zhang, Y.; Davie, A.; Marshall-Gradisnik, S.; Hu, H.; Wang, J.; Brushett, D. Muscle and plasma coenzyme Q10 concentration, aerobic power and exercise economy of healthy men in response to four weeks of supplementation. J. Sports Med. Phys. Fit. 2005, 45, 337–346. [Google Scholar]
- Svensson, M.; Malm, C.; Tonkonogi, M.; Ekblom, B.; Sjödin, B.; Sahlin, K. Effect of Q10 supplementation on tissue Q10 levels and adenine nucleotide catabolism during high-intensity exercise. Int. J. Sport Nutr. 1999, 9, 166–180. [Google Scholar] [CrossRef]
- Arias, A.; García-Villoria, J.; Rojo, A.; Buján, N.; Briones, P.; Ribes, A. Analysis of coenzyme Q10 in lymphocytes by HPLC-MS/MS. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2012, 908, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Turunen, M.; Wehlin, L.; Sjöberg, M.; Lundahl, J.; Dallner, G.; Brismar, K.; Sindelar, P.J. β2-integrin and lipid modifications indicate a non-antioxidant mechanism for the anti-atherogenic effect of dietary coenzyme Q10. Biochem. Biophys. Res. Commun. 2002, 296, 255–260. [Google Scholar] [CrossRef]
- Tomasetti, M.; Alleva, R.; Collins, A.R. In vivo supplementation with coenzyme Q10 enhances the recovery of human lymphocytes from oxidative DNA damage. FASEB J. 2001, 15, 1425–1427. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.V.; Tang, P.H.; Miles, L.; Steele, P.E.; Moye, M.J.; Horn, P.S. Validation and application of an HPLC-EC method for analysis of coenzyme Q10 in blood platelets. Biomed. Chromatogr. 2008, 22, 1403–1408. [Google Scholar] [CrossRef] [PubMed]
- Niklowitz, P.; Sonnenschein, A.; Janetzky, B.; Andler, W.; Menke, T. Enrichment of coenzyme Q10 in plasma and blood cells: Defense against oxidative damage. Int. J. Biol. Sci. 2007, 3, 257–262. [Google Scholar] [CrossRef]
- Ormazabal, A.; Vilaseca, M.A.; Pérez-Dueñas, B.; Lambruschini, N.; Gómez, L.; Campistol, J.; Artuch, R. Platelet serotonin concentrations in PKU patients under dietary control and tetrahydrobiopterin treatment. J. Inherit. Metab. Dis. 2005, 28, 863–870. [Google Scholar] [CrossRef]
- Silva, A.M.; Oliveira, P.J. Evaluation of respiration with Clark type electrode in isolated mitochondria and permeabilized animal cells. Methods Mol. Biol. 2012, 810, 7–24. [Google Scholar] [CrossRef]
- Yubero, D.; Montero, R.; Ramos, M.; Neergheen, V.; Navas, P.; Artuch, R.; Hargreaves, I. Determination of urinary coenzyme Q10 by HPLC with electrochemical detection: Reference values for a paediatric population. BioFactors 2015, 41, 424–430. [Google Scholar] [CrossRef]
- Montero, R.; Sánchez-Alcázar, J.A.; Briones, P.; Hernández, Á.R.; Cordero, M.D.; Trevisson, E.; Salviati, L.; Pineda, M.; García-Cazorla, A.; Navas, P.; et al. Analysis of coenzyme Q10 in muscle and fibroblasts for the diagnosis of CoQ10 deficiency syndromes. Clin. Biochem. 2008, 41, 697–700. [Google Scholar] [CrossRef]
- Montero, R.; Yubero, D.; Salgado, M.C.; González, M.J.; Campistol, J.; del O’Callaghan, M.M.; Pineda, M.; Delgadillo, V.; Maynou, J.; Fernandez, G.; et al. Plasma coenzyme Q10 status is impaired in selected genetic conditions. Sci. Rep. 2019, 9, 793. [Google Scholar] [CrossRef]
- Lowry, O.H.; Rosebrough, N.J.; Farr, A.L.; Randall, R.J. Protein measurement with the Folin phenol reagent. J. Biol. Chem. 1951, 193, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, S.L.; Florkowski, C.M.; Lever, M.; George, P.M. Biological variation of coenzyme Q10. Clin. Chem. 2005, 51, 455–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duncan, A.J.; Heales, S.J.R.; Mills, K.; Eaton, S.; Land, J.M.; Hargreaves, I.P. Determination of coenzyme Q10 status in blood mononuclear cells, skeletal muscle, and plasma by HPLC with di-propoxy-coenzyme Q10 as an internal standard. Clin. Chem. 2005, 51, 2380–2382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero, R.; Artuch, R.; Briones, P.; Nascimento, A.; García-Cazorla, A.; Vilaseca, M.A.; Sánchez-Alcázar, J.A.; Navas, P.; Montoya, J.; Pineda, M. Muscle coenzyme Q10 concentrations in patients with probable and definite diagnosis of respiratory chain disorders. BioFactors 2005, 25, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Pravst, I.; Aguilera, J.C.R.; Rodriguez, A.B.C.; Jazbar, J.; Locatelli, I.; Hristov, H.; Žmitek, K. Comparative bioavailability of different coenzyme Q10 formulations in healthy elderly individuals. Nutrients 2020, 12, 784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentinger, M.; Dallner, G.; Chojnacki, T.; Swiezewska, E. Distribution and breakdown of labeled coenzyme Q10 in rat. Free Radic. Biol. Med. 2003, 34, 563–575. [Google Scholar] [CrossRef]
- Petrangolini, G.; Ronchi, M.; Frattini, E.; De Combarieu, E.; Allegrini, P.; Riva, A. A new food-grade coenzyme Q10 formulation improves bioavailability: Single and repeated pharmacokinetic studies in healthy volunteers. Curr. Drug Deliv. 2019, 16, 759–767. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Plasma CoQ (µmol/L) | Plasma CoQ/Chol (µmol/mol Chol) and Chol (mmol/L) | BMCs CoQ (nmol/g Protein) | Platelets CoQ (pmol/109 Platelets) | Urinary CoQ (nmol/g Protein) | Muscle CoQ (nmol/g Protein) | |
|---|---|---|---|---|---|---|
| Group 1, PRE (n = 11) | 0.76–1.53 1.11 (0.23) | 169–317 212 (43.2) and 3.82–6.53 5.32 (0.82) | 32–124 75 (32.4) | 154–598 288 (135.5) | 28–362 132 (98.2) | 127–380 245 (90.7) |
| Group 2, POST (n = 11) | 1.33–3.17 2.34 (0.55) | 302–753 476 (145) and 4.18–6.13 5.02 (0.62) | 40–166 96 (42.9) | 205–517 304 (97.6) | 69–738 230 (185) | 162–434 299 (98.6) * |
| Reference values ** | 0.46–1.78 Ref. [22] | 101–265 Ref. [22] | 37–133 Ref. [23] | 133–247 Ref. [15] | 43–139 Ref. [18] | 140–580 Ref. [23] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paredes-Fuentes, A.J.; Montero, R.; Codina, A.; Jou, C.; Fernández, G.; Maynou, J.; Santos-Ocaña, C.; Riera, J.; Navas, P.; Drobnic, F.; et al. Coenzyme Q10 Treatment Monitoring in Different Human Biological Samples. Antioxidants 2020, 9, 979. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9100979
Paredes-Fuentes AJ, Montero R, Codina A, Jou C, Fernández G, Maynou J, Santos-Ocaña C, Riera J, Navas P, Drobnic F, et al. Coenzyme Q10 Treatment Monitoring in Different Human Biological Samples. Antioxidants. 2020; 9(10):979. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9100979
Chicago/Turabian StyleParedes-Fuentes, Abraham J., Raquel Montero, Anna Codina, Cristina Jou, Guerau Fernández, Joan Maynou, Carlos Santos-Ocaña, Joan Riera, Plácido Navas, Franchek Drobnic, and et al. 2020. "Coenzyme Q10 Treatment Monitoring in Different Human Biological Samples" Antioxidants 9, no. 10: 979. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9100979