
Factors Associated with COVID-19 Vaccine Hesitancy after Implementation of a Mass Vaccination Campaign

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcome
2.3. Independent Variables
2.4. Statistical Analysis
3. Results
3.1. Determinants of Vaccine Hesitancy: Contextual Influences
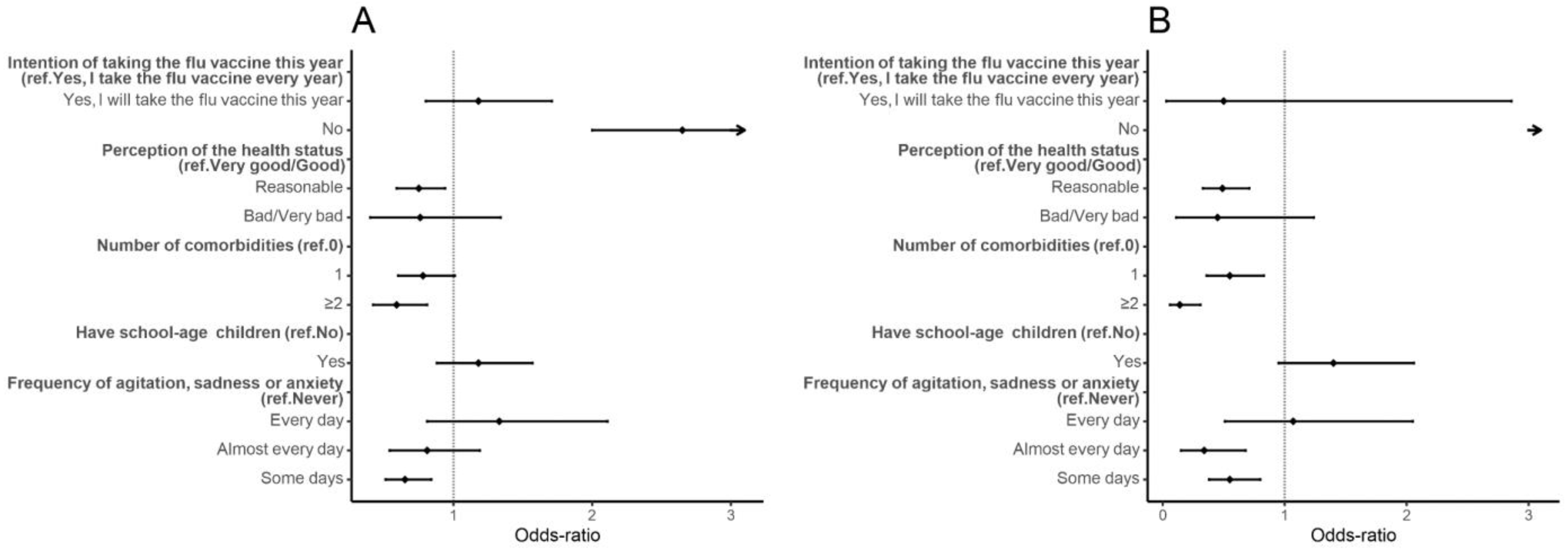
3.2. Determinants of Vaccine Hesitancy: Individual Influences
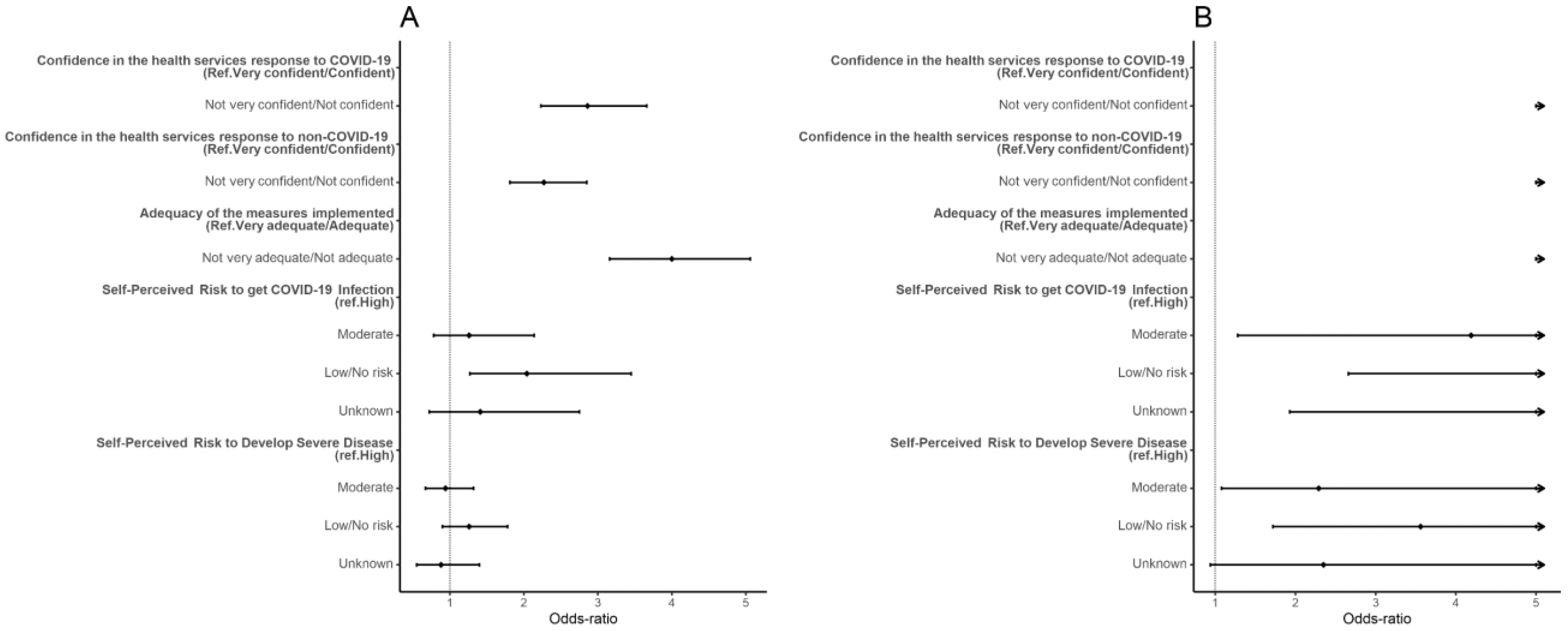
3.3. Determinants of Vaccine Hesitancy: COVID-19 Influences
3.4. Determinants of Vaccine Hesitancy: COVID-19-Vaccine-Related Influences
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Centre for Disease Prevention and Control (ECDC). COVID-19 Situation Update Worldwide, as of Week 47 2021. 2021. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 5 December 2021).
- European Centre for Disease Prevention and Control (ECDC). Overview of the Implementation of COVID-19 Vaccination Strategies and Deployment Plans in the EU/EEA. 2021. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Overview-of-the-implementation-of-COVID-19-vaccination-strategies-and-deployment-plans-23-Sep-2021.pdf (accessed on 12 October 2021).
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef]
- Rechel, B.; Priaulx, J.; Richardson, E.; McKee, M. The organization and delivery of vaccination services in the European Union. In European Observatory on Health Systems and Policies; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- AlShurman, B.A.; Khan, A.F.; Mac, C.; Majeed, M.; Butt, Z.A. What Demographic, Social, and Contextual Factors Influence the Intention to Use COVID-19 Vaccines: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9342. [Google Scholar] [CrossRef]
- Burke, P.F.; Masters, D.; Masseya, G. Enablers and barriers to COVID-19 vaccine uptake: An international study of perceptions and intentions. Vaccine 2021, 39, 5116–5128. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ten Threats to Global Health in 2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 12 October 2021).
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Thomas, K.; Shah, M.D.; Vizueta, N.; Cui, Y.; Vangala, S.; Kapteyn, A. Likelihood of COVID-19 vaccination by subgroups across the US: Post-election trends and disparities. Hum. Vaccines Immunother. 2021, 17, 3262–3267. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Nguyen, K.; Corlin, L.; Allen, J.D.; Chung, M. Changes in COVID-19 vaccination receipt and intention to vaccinate by socioeconomic characteristics and geographic area, United States, January 6–March 29, 2021. Ann. Med. 2021, 53, 1419–1428. [Google Scholar] [CrossRef]
- Lindholt, M.F.; Jorgensen, F.; Bor, A.; Petersen, M.B. Public acceptance of COVID-19 vaccines: Cross-national evidence on levels and individual-level predictors using observational data. BMJ Open 2021, 1, e048172. [Google Scholar] [CrossRef] [PubMed]
- Byrne, T.; Patel, P.; Shrotri, M.; Beale, S.; Michie, S.; Butt, J.; Hawkins, N.; Hardelid, P.; Rodger, A.; Aryee, A.; et al. Trends, patterns, and psychological influences on covid-19 vaccination intention: Findings from a large prospective community cohort study in England and Wales (Virus Watch). Vaccine 2021, 39, 7108–7116. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.H.; Yankey, D.; Coy, K.C.; Brookmeyer, K.A.; Abad, N.; Guerin, R.; Syamlal, G.; Lu, P.J.; Baack, B.N.; Razzaghi, H.; et al. Covid-19 vaccination coverage, intent, knowledge, attitudes, and beliefs among essential workers, united states. Emerg. Infect. Dis. 2021, 27, 2908–2913. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.M.; Liu, L.; Sun, J.; Yan, W.; Yuan, K.; Zheng, Y.B.; Lu, Z.A.; Ni, S.Y.; Su, S.Z.; Zhu, X.M.; et al. Public willingness and determinants of COVID-19 vaccination at the initial stage of mass vaccination in China. Vaccines 2021, 9, 1172. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.A.V.; Roberts, B.; Wong, B.L.H.; van Kessel, R.; Mossialos, E. The Relationship Between the COVID-19 Pandemic and Vaccine Hesitancy: A Scoping Review of Literature Until August 2021. Front. Public Health 2021, 9, 747787. [Google Scholar] [CrossRef]
- Martin, C.A.; Marshall, C.; Patel, P.; Goss, C.; Jenkins, D.R.; Ellwood, C.; Barton, L.; Price, A.; Brunskill, N.J.; Khunti, K.; et al. SARS-CoV-2 vaccine uptake in a multi-ethnic UK healthcare workforce: A cross-sectional study. PLoS Med. 2021, 18, e1003823. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Danaee, M.; Ahmed, J.; Lachyan, A.; Cai, C.Z.; Lin, Y.; Hu, Z.; Tan, S.Y.; Lu, Y.; et al. COVID-19 vaccination intention and vaccine characteristics influencing vaccination acceptance: A global survey of 17 countries. Infect. Dis. Poverty 2021, 10, 122. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Strohle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Sønderskov, K.M.; Dinesen, P.T.; Østergaard, S.D. Sustained COVID-19 vaccine willingness after safety concerns over the Oxford-AstraZeneca vaccine. Dan. Med. J. 2021, 68, A03210292. [Google Scholar]
- Raciborski, F.; Samel-Kowalik, P.; Gujski, M.; Pinkas, J.; Arcimowicz, M.; Jankowski, M. Factors associated with a lack of willingness to vaccinate against covid-19 in Poland: A 2021 nationwide cross-sectional survey. Vaccines 2021, 9, 1000. [Google Scholar] [CrossRef]
- Vollmann, M.; Salewski, C. To Get Vaccinated, or Not to Get Vaccinated, That Is the Question: Illness Representations about COVID-19 and Perceptions about COVID-19 Vaccination as Predictors of COVID-19 Vaccination Willingness among Young Adults in The Netherlands. Vaccines 2021, 9, 941. [Google Scholar] [CrossRef] [PubMed]
- Iguacel, I.; Maldonado, A.L.; Ruiz-Cabello, A.L.; Samatán, E.; Alarcón, J.; Orte, M.Á.; Mateos, S.S.; Martínez-Jarreta, B. Attitudes of Healthcare Professionals and General Population Toward Vaccines and the Intention to Be Vaccinated Against COVID-19 in Spain. Front. Public Health 2021, 9, 739003. [Google Scholar] [CrossRef] [PubMed]
- Fotiadis, K.; Dadouli, K.; Avakian, I.; Bogogiannidou, Z.; Mouchtouri, V.A.; Gogosis, K.; Speletas, M.; Koureas, M.; Lagoudaki, E.; Kokkini, S.; et al. Factors Associated with Healthcare Workers’ (HCWs) Acceptance of COVID-19 Vaccinations and Indications of a Role Model towards Population Vaccinations from a Cross-Sectional Survey in Greece, May 2021. Int. J. Environ. Res. Public Health 2021, 18, 10558. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, S.M.; Dehom, S.; Almutairi, D.; Alnasser, B.S.; Alsaif, B.; Alabdrabalnabi, A.A.; Bin Rahmah, A.; Alshahrani, M.S.; El-Metwally, A.; Al-Khateeb, B.F.; et al. Acceptability of COVID-19 vaccination in Saudi Arabia: A cross-sectional study using a web-based survey. Hum. Vaccines Immunother. 2021, 17, 3338–3347. [Google Scholar] [CrossRef] [PubMed]
- Jasuja, G.K.; Meterko, M.; Bradshaw, L.D.; Carbonaro, R.; Clayman, M.L.; LoBrutto, L.; Miano, D.; Maguire, E.M.; Midboe, A.M.; Asch, S.M.; et al. Attitudes and Intentions of US Veterans Regarding COVID-19 Vaccination. JAMA Netw. Open 2021, 4, e2132548. [Google Scholar] [CrossRef]
- Cooper, S.; van Rooyen, H.; Wiysonge, C.S. COVID-19 vaccine hesitancy in South Africa: How can we maximize uptake of COVID-19 vaccines? Expert Rev. Vaccines 2021, 20, 921–933. [Google Scholar] [CrossRef]
- Aloweidi, A.; Bsisu, I.; Suleiman, A.; Abu-Halaweh, S.; Almustafa, M.; Aqel, M.; Amro, A.; Radwan, N.; Assaf, D.; Abdullah, M.Z.; et al. Hesitancy towards COVID-19 Vaccines: An Analytical Cross–Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5111. [Google Scholar] [CrossRef]
- Shacham, M.; Greenblatt-Kimron, L.; Hamama-Raz, Y.; Martin, L.R.; Peleg, O. Increased COVID-19 Vaccination Hesitancy and Health Awareness amid COVID-19 Vaccinations Programs in Israel. Int. J. Environ. Res. Public Health 2021, 18, 3804. [Google Scholar] [CrossRef]
- Toro-Ascuy, D.; Cifuentes-Munoz, N.; Avaria, A.; Pereira-Montecinos, C.; Cruzat, G.; Zorondo-Rodriguez, F.; Fuenzalida, L.F. Underlying factors that influence the acceptance of COVID19 vaccine in a country with a high vaccination rate. medRxiv 2021. [Google Scholar] [CrossRef]
- Dong, C.; Liang, Q.; Ji, T.; Gu, J.; Feng, J.; Shuai, M.; Zhang, X.; Zhao, R.; Gu, Z. Determinants of Vaccine Acceptance against COVID-19 in China: Perspectives on Knowledge and DrVac-COVID19S Scale. Int. J. Env. Res. Public Health 2021, 18, 11192. [Google Scholar] [CrossRef]
- Singh, A.; Lai, A.H.Y.; Wang, J.; Asim, S.; Chan, P.S.F.; Wang, Z.; Yeoh, E.K. Multilevel Determinants of COVID-19 Vaccine Uptake Among South Asian Ethnic Minorities in Hong Kong: Cross-sectional Web-Based Survey. JMIR Public Health Surveill. 2021, 7, e31707. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.R.; Watanapongvanich, S.; Kadoya, Y. COVID-19 Vaccine Hesitancy among the Younger Generation in Japan. Int. J. Env. Res. Public Health 2021, 18, 11702. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.; Waitzberg, R.; Israeli, A.; Hartal, M.; Davidovitch, N. Addressing vaccine hesitancy and access barriers to achieve persistent progress in Israel’s COVID-19 vaccination program. Isr. J. Health Policy Res. 2021, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, M.J.P.; Caramujo, C.; Julio, N.; Magalhães, J.C.; Basto, R.; Fraga, T.; Gomes, I.F.; Pazos, I.; Sousa, G. Acceptance of SARS-CoV-2 vaccination among patients with cancer undergoing immunosuppressive therapy: Portuguese study. Ann. Oncol. 2021, 32 (Suppl. S5), S1145–S1146. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 14 December 2021).
- Otto, S.P.; Day, T.; Arino, J.; Colijn, C.; Dushoff, J.; Li, M.; Mechai, S.; Van Domselaar, G.; Wu, J.; Earn, D.J.; et al. The origins and potential future of SARS-CoV-2 variants of concern in the evolving COVID-19 pandemic. Curr. Biol. 2021, 31, R918–R929. [Google Scholar] [CrossRef]
- Dryer, O. Covid-19: Delta infections threaten herd immunity vaccine strategy. BMJ 2021, 374, n1933. [Google Scholar] [CrossRef]
- World Health Organization (WHO) Europe. Statement—Update on COVID-19: Europe and Central Asia again at the Epicentre of the Pandemic. 4 November 2021. Available online: https://www.euro.who.int/en/media-centre/sections/statements/2021/statement-update-on-covid-19-europe-and-central-asia-again-at-the-epicentre-of-the-pandemic (accessed on 14 December 2021).
- Pedro, A.R.; Gama, A.; Soares, P.; Moniz, M.; Laires, P.A.; Dias, S. COVID-19 Barometer: Social Opinion—What Do the Portuguese Think in This Time of COVID-19? Port. J. Public Health 2021, 38 (Suppl. S1), 42–50. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: http://r.meteo.uni.wroc.pl/web/packages/dplR/vignettes/intro-dplR.pdf (accessed on 25 November 2021).
- Direção-Geral da Saúde. Plano de Vacinação: Relatório de Vacinação em Portugal nº 40. Semana 45. 2021. Available online: https://covid19.min-saude.pt/wp-content/uploads/2021/11/Relato%CC%81rio-Vacinac%CC%A7a%CC%83o-n.o-40.pdf (accessed on 5 December 2021).
- Direção-Geral da Saúde. Monitorização das Linhas Vermelhas para a COVID-19 nº39. 24 December 2021. Available online: https://www.insa.min-saude.pt/wp-content/uploads/2021/12/20211224_Monitorizacao_Epidemia_COVID-19.pdf (accessed on 29 December 2021).
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde. Plano de Vacinação: Relatório de Vacinação Diário Covid-19 + Gripe nº16. 2021. Available online: https://covid19.min-saude.pt/wp-content/uploads/2021/12/Relatorio-Vacinacao-Diario-20211214.pdf (accessed on 14 December 2021).
- United Nations Children’s Fund. Vaccine Misinformation Management Field Guide. New York. 2020. Available online: https://www.unicef.org/mena/reports/vaccine-misinformation-management-field-guide (accessed on 14 December 2021).
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Determinants of Vaccine Hesitancy | Variables |
|---|---|
| Contextual influences | Gender |
| Age group | |
| Education | |
| Monthly household income | |
| Partial or total income loss during the pandemic | |
| Occupation Month of the questionnaire | |
| Individual influences | Intention to take the flu vaccine |
| Perception of the health status | |
| Number of comorbidities | |
| Having school-age children Frequency of agitation, sadness, or anxiety | |
| COVID-19 disease-specific | Confidence in the health services response to COVID-19 |
| Confidence in the health services response to non-COVID-19 | |
| Perception of the adequacy of measures implemented by the Government | |
| Self-perceived risk of getting COVID-19 infection | |
| Self-perceived risk of developing severe disease following COVID-19 infection | |
| COVID-19 vaccine-specific | Confidence in the safety of the COVID-19 vaccines |
| Confidence in the efficacy of the COVID-19 vaccines |
| Contextual Influences | Vaccinated (N = 2857) | Hesitant (N = 375) | Total (N = 3232) |
|---|---|---|---|
| Gender (N = 3224) | |||
| Male | 686 (24.1%) | 117 (31.3%) | 803 (24.9%) |
| Female | 2164 (75.9%) | 257 (68.7%) | 2421 (75.1%) |
| Age group (N = 3232) | |||
| 16–24 | 44 (1.5%) | 7 (1.9%) | 51 (1.6%) |
| 25–49 | 933 (32.7%) | 106 (28.3%) | 1039 (32.1%) |
| 50–64 | 1080 (37.8%) | 117 (31.2%) | 1197 (37.0%) |
| 65–79 | 767 (26.8%) | 138 (36.8%) | 905 (28.0%) |
| 80+ | 33 (1.2%) | 7 (1.9%) | 40 (1.2%) |
| Education (N = 3221) | |||
| No education/Basic education | 149 (5.2%) | 32 (8.6%) | 181 (5.6%) |
| Secondary | 609 (21.4%) | 103 (27.7%) | 712 (22.1%) |
| University | 2091 (73.4%) | 237 (63.7%) | 2328 (72.3%) |
| Monthly household income (N = 2958) | |||
| <EUR 650 | 118 (4.5%) | 26 (8.1%) | 144 (4.9%) |
| EUR 651–1000 | 275 (10.4%) | 60 (18.8%) | 335 (11.3%) |
| EUR 1001–1500 | 523 (19.8%) | 57 (17.8%) | 580 (19.6%) |
| EUR 1501–2000 | 509 (19.3%) | 72 (22.5%) | 581 (19.6%) |
| EUR 2001–2500 | 474 (18.0%) | 39 (12.2%) | 513 (17.3%) |
| >EUR 2501 | 739 (28.0%) | 66 (20.6%) | 805 (27.2%) |
| Lost of income due to the pandemic (N = 3165) | |||
| No | 2082 (74.4%) | 264 (72.3%) | 2346 (74.1%) |
| Partial/Total | 718 (25.6%) | 101 (27.7%) | 819 (25.9%) |
| Occupation (N = 3232) | |||
| Worker | 1736 (60.8%) | 194 (51.7%) | 1930 (59.7%) |
| Student | 52 (1.8%) | 10 (2.7%) | 62 (1.9%) |
| Retired | 764 (26.7%) | 127 (33.9%) | 891 (27.6%) |
| Unemployed | 143 (5.01%) | 17 (4.53%) | 160 (4.95%) |
| Other | 162 (5.67%) | 27 (7.20%) | 189 (5.9%) |
| Month (N = 3232) | |||
| September | 454 (15.9%) | 45 (12.0%) | 499 (15.4%) |
| October | 848 (29.7%) | 110 (29.3%) | 958 (29.6%) |
| November | 1555 (54.4%) | 220 (58.7%) | 1775 (54.9%) |
| Individual Influences | Vaccinated (N = 2857) | Hesitant (N = 375) | Total (N = 3232) |
|---|---|---|---|
| Intention of taking the flu vaccine this year (N = 3178) | |||
| Yes, I take the flu vaccine every year | 1224 (43.6%) | 126 (34.2%) | 1350 (42.5%) |
| Yes, I will take the flu vaccine this year | 428 (15.2%) | 42 (11.4%) | 470 (14.8%) |
| No | 1158 (41.2%) | 200 (54.3%) | 1358 (42.7%) |
| Perception of the health status (N = 3226) | |||
| Very good/Good | 1421 (49.8%) | 205 (55.1%) | 1626 (50.4%) |
| Reasonable | 1326 (46.5%) | 154 (41.4%) | 1480 (45.9%) |
| Bad/Very bad | 107 (3.75%) | 13 (3.49%) | 120 (3.72%) |
| Number of diseases (N = 3160) | |||
| 0 | 1339 (47.8%) | 188 (52.2%) | 1527 (48.3%) |
| 1 | 866 (30.9%) | 111 (30.8%) | 977 (30.9%) |
| ≥2 | 595 (21.2%) | 61 (16.9%) | 656 (20.8%) |
| Have school-age children (N = 3222) | |||
| No | 2042 (71.7%) | 274 (73.5%) | 2316 (71.9%) |
| Yes | 807 (28.3%) | 99 (26.5%) | 906 (28.1%) |
| Frequency of agitation, sadness or anxiety (N = 3218) | |||
| Never | 772 (27.1%) | 135 (36.1%) | 907 (28.2%) |
| Some days | 1655 (58.2%) | 176 (47.1%) | 1831 (56.9%) |
| Almost every day | 291 (10.2%) | 38 (10.2%) | 329 (10.2%) |
| Every day | 126 (4.4%) | 25 (6.7%) | 151 (4.7%) |
| COVID-19 Influences | Vaccinated (N = 2857) | Hesitant (N = 375) | Total (N = 3232) |
|---|---|---|---|
| Confidence in the health services response to COVID-19 (N = 3213) | |||
| Very confident/Confident | 2416 (84.8%) | 245 (67.1%) | 2661 (82.8%) |
| Not very confident/Not confident | 432 (15.2%) | 120 (32.9%) | 552 (17.2%) |
| Confidence in the health services response to non-COVID-19 (N = 3210) | |||
| Very confident/Confident | 1623 (57.2%) | 140 (37.7%) | 1763 (54.9%) |
| Not very confident/Not confident | 1216 (42.8%) | 231 (62.3%) | 1447 (45.1%) |
| Perception of the adequacy of the measures implemented by the Government (N = 3172) | |||
| Very adequate/Adequate | 2220 (79.2%) | 193 (52.3%) | 2413 (76.1%) |
| Not very adequate/Not adequate | 583 (20.8%) | 176 (47.7%) | 759 (23.9%) |
| Self-Perceived Risk of getting COVID-19 Infection (N = 3226) | |||
| High | 221 (7.8%) | 19 (5.1%) | 240 (7.4%) |
| Moderate | 1321 (46.3%) | 139 (37.1%) | 1460 (45.3%) |
| Low/No risk | 1143 (40.1%) | 197 (52.5%) | 1340 (41.5%) |
| Not sure | 166 (5.8%) | 20 (5.3%) | 186 (5.8%) |
| Self-Perceived Risk of Developing Severe Disease Following COVID-19 Infection (N = 3221) | |||
| High | 415 (14.6%) | 58 (15.5%) | 473 (14.7%) |
| Moderate | 1047 (36.8%) | 124 (33.2%) | 1171 (36.4%) |
| Low/No risk | 1090 (38.3%) | 159 (42.6%) | 1249 (38.8%) |
| Not sure | 296 (10.4%) | 32 (8.6%) | 328 (10.2%) |
| COVID-19 Vaccine-Related Influences | Vaccinated (N = 2857) | Hesitant (N = 375) | Total (N = 3232) |
|---|---|---|---|
| Safety perception in the COVID-19 vaccines (N = 3134) | |||
| Completely safe/Safe | 2670 (96.1%) | 232 (65.0%) | 2902 (92.6%) |
| Not very safe/Not safe | 107 (3.9%) | 125 (35.0%) | 232 (7.4%) |
| Efficacy perception in the COVID-19 vaccines (N = 3143) | |||
| Completely effective/Effective | 2613 (93.9%) | 228 (63.3%) | 2841 (90.4%) |
| Not very effective/Not effective | 170 (6.1%) | 132 (36.7%) | 302 (9.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, I.A.; Soares, P.; Rocha, J.V.; Gama, A.; Laires, P.A.; Moniz, M.; Pedro, A.R.; Dias, S.; Goes, A.R.; Leite, A.; et al. Factors Associated with COVID-19 Vaccine Hesitancy after Implementation of a Mass Vaccination Campaign. Vaccines 2022, 10, 281. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10020281
Gomes IA, Soares P, Rocha JV, Gama A, Laires PA, Moniz M, Pedro AR, Dias S, Goes AR, Leite A, et al. Factors Associated with COVID-19 Vaccine Hesitancy after Implementation of a Mass Vaccination Campaign. Vaccines. 2022; 10(2):281. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10020281
Chicago/Turabian StyleGomes, Inês Afonso, Patricia Soares, João Victor Rocha, Ana Gama, Pedro Almeida Laires, Marta Moniz, Ana Rita Pedro, Sónia Dias, Ana Rita Goes, Andreia Leite, and et al. 2022. "Factors Associated with COVID-19 Vaccine Hesitancy after Implementation of a Mass Vaccination Campaign" Vaccines 10, no. 2: 281. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10020281