
A Systematic Review and a Meta-Analysis of the Yellow Fever Vaccine in the Elderly Population

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
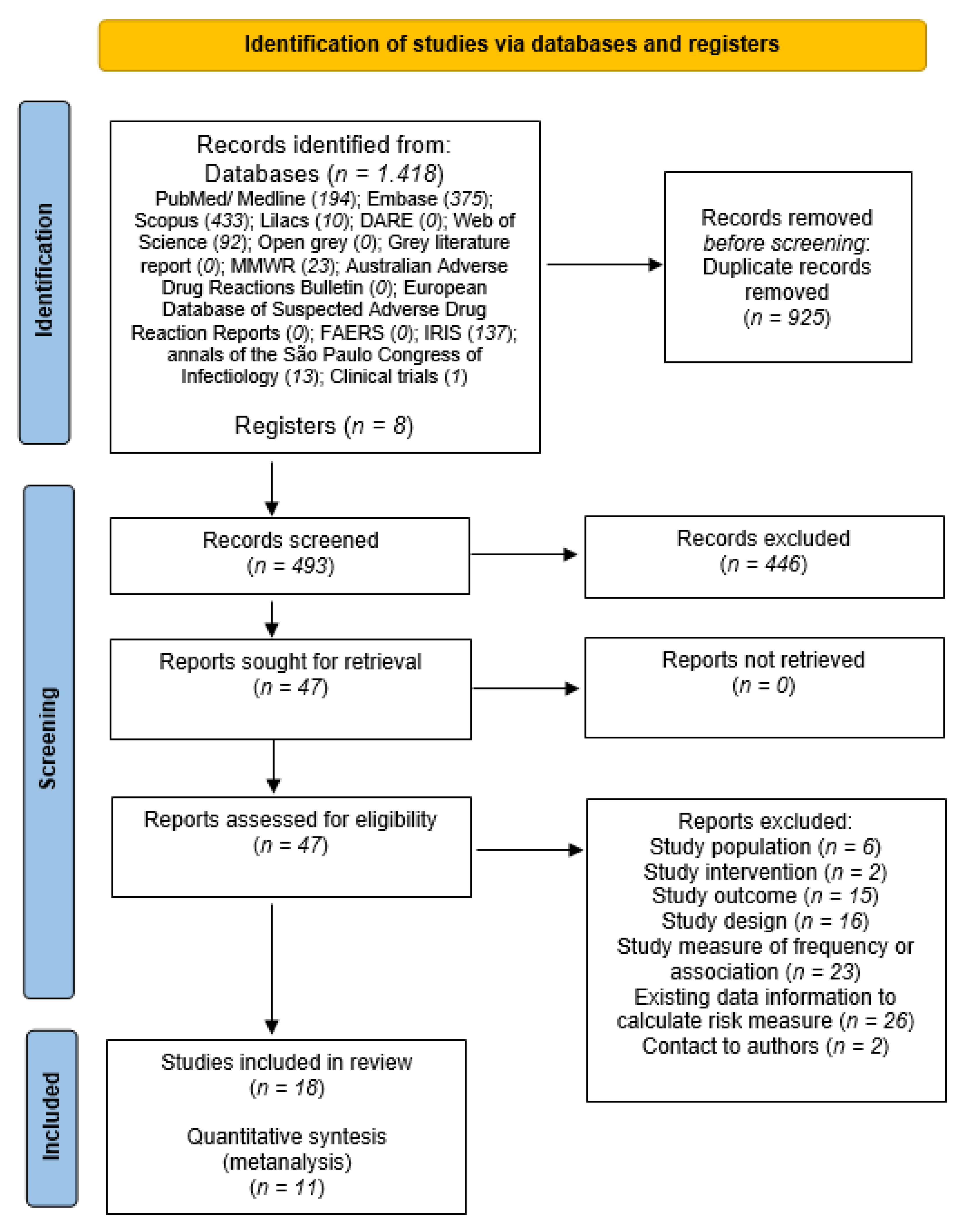
2.1. Information Sources and Search Strategy
2.2. Information Sources and Search Strategy
2.3. Information Sources and Search Strategy
2.4. Information Sources and Search Strategy
3. Results
3.1. Study Characteristics
3.2. Risk of Bias within Studies and across Studies
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Yellow Fever. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/yellow-fever (accessed on 7 November 2021).
- Ministério da Saúde do Brasil. Manual de Vigilância Epidemiológica de Eventos Adversos Pós-Vacinação. Brasília. 2021. Available online: www.saude.gov.br/bvs (accessed on 7 November 2021).
- World Health Orgnization. Global Manual on Surveillance of Adverse Events Following Immunization. 2014. Available online: www.who.int (accessed on 7 November 2021).
- Lindsey, N.P.; Schroeder, B.A.; Miller, E.R.; Braun, M.M.; Hinckley, A.F.; Marano, N.; Slade, B.A.; Barnett, E.; Brunette, G.W.; Horan, K.; et al. Adverse event reports following yellow fever vaccination. Vaccine 2008, 26, 6077–6082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordin, J.; Parker, E.D.; Kharbanda, E.O.; Naleway, A.; Marcy, S.M.; Molitor, B.; Kuckler, L.; Baggs, J.; Vazquez-Benitez, G. Safety of the Yellow Fever Vaccine: A Retrospective Study. J. Travel Med. 2013, 20, 368–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.H.; Kozlovsky, B.F.; Effros, R.B.; Grubeck-Loebenstein, B.; Edelman, R.; Sztein, M.B. Vaccination in the elderly: An immunological perspective. Trends Immunol. 2009, 30, 351–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da Saúde do Brasil. Febre Amarela. 2021. Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/f/febre-amarela (accessed on 7 November 2021).
- Chen, L.H.; Wilson, M.E. Yellow fever control: Current epidemiology and vaccination strategies. Trop. Dis. Travel Med. Vaccines 2020, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Klitting, R.; Gould, E.A.; Paupy, C.; de Lamballerie, X. What Does the Future Hold for Yellow Fever Virus? (I). Genes 2018, 9, 291. [Google Scholar] [CrossRef] [Green Version]
- Barrett, A.D.T. The reemergence of yellow fever. Science 2018, 361, 847–848. [Google Scholar] [CrossRef]
- World Health Organization. Yellow Fever: Latest Outbreak News. 2021. Available online: https://www.who.int/emergencies/emergency-events/item/yellow-fever (accessed on 7 November 2021).
- World Health Organization. World Report on Ageing and Health. 2015. Available online: https://apps.who.int/iris/handle/10665/186463 (accessed on 7 November 2021).
- Morais Duarte Miranda, G.; da Cruz Gouveia Mendes, A.; Lucia Andrade da Silva, A.; Oswaldo Cruz, F.; Gabriella Morais Duarte Miranda, C. Population aging in Brazil: Current and future social challenges and consequences. Rev. Bras. Geriatr. Gerontol. 2016, 19, 507–519. [Google Scholar] [CrossRef]
- Miyaji, K.T.; Luiz, A.M.; Lara, A.N.; Chaves, T.D.S.S.; Piorelli, R.D.O.; Lopes, M.H.; Sartori, A.M.C. Active assessment of adverse events following yellow fever vaccination of persons aged 60 years and more. Hum. Vaccines Immunother. 2013, 9, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Rafferty, E.; Duclos, P.; Yactayo, S.; Schuster, M. Risk of yellow fever vaccine-associated viscerotropic disease among the elderly: A systematic review. Vaccine 2013, 31, 5798–5805. [Google Scholar] [CrossRef]
- Tanizaki, R.; Ujiie, M.; Hori, N.; Kanagawa, S.; Kutsuna, S.; Takeshita, N.; Hayakawa, K.; Kato, Y.; Ohmagari, N. Comparative study of adverse events after yellow fever vaccination between elderly and non-elderly travellers: Questionnaire survey in Japan over a 1-year period. J. Travel Med. 2016, 23, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Seligman, S.J. Risk groups for yellow fever vaccine-associated viscerotropic disease (YEL-AVD). Vaccine 2014, 32, 5769–5775. [Google Scholar] [CrossRef] [PubMed]
- Khromava, A.Y.; Eidex, R.B.; Weld, L.; Kohl, K.S.; Bradshaw, R.D.; Chen, R.T.; Cetron, M.S. Yellow fever vaccine: An updated assessment of advanced age as a risk factor for serious adverse events. Vaccine 2005, 23, 3256–3263. [Google Scholar] [CrossRef] [Green Version]
- Thomas, R.E.; Williamson, T.; Lorenzetti, D.L.; Spragins, W.; Jackson, D. The Safety of Yellow Fever Vaccine 17D or 17DD in Children, Pregnant Women, HIV+ Individuals, and Older Persons: Systematic Review. Am. J. Trop. Med. Hyg. 2012, 86, 359–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zorzela, L.; Loke, Y.K.; Ioannidis, J.P.; Golder, S.; Santaguida, P.; Altman, D.G.; Moher, D.; Vohra, S. PRISMA harms group PRISMA harms checklist: Improving harms reporting in systematic reviews. BMJ 2016, 352, i157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde do Brasil. Diretrizes Metodológicas Sistema GRADE-Manual de Graduação da Qualidade da Evidência e Força de Recomendação Para Tomada de Decisão em Saúde. Brasília. 2014. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_metodologicas_sistema_grade.pdf (accessed on 23 December 2021).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Lau, J.; Ioannidis, J.P.; Schmid, C. Summing up evidence: One answer is not always enough. Lancet 1998, 351, 123–127. [Google Scholar] [CrossRef]
- Center for Diseases Control and Prevention. Adverse Events Associated with 17D-Derived Yellow Fever Vaccination—United States, 2001–2002. Morb Mortal Wkly Rep. 2002, 51, 989–993. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5144a1.htm (accessed on 7 November 2021).
- Azevedo, L.; Lasmar, E.; Contieri, F.; Boin, I.; Percegona, L.; Saber, L.; Selistre, L.; Netto, M.; Moreira, M.; Carvalho, R.; et al. Yellow fever vaccination in organ transplanted patients: Is it safe? A multicenter study. Transpl. Infect. Dis. 2011, 14, 237–241. [Google Scholar] [CrossRef]
- Bae, H.; Domingo, C.; Tenorio, A.; De Ory, F.; Muñoz, J.; Weber, P.; Teuwen, D.E.; Niedrig, M. Immune Response during Adverse Events after 17D-Derived Yellow Fever Vaccination in Europe. J. Infect. Dis. 2008, 197, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Breugelmans, J.; Lewis, R.; Agbenu, E.; Veit, O.; Jackson, D.; Domingo, C.; Böthe, M.; Perea, W.; Niedrig, M.; Gessner, B.; et al. Adverse events following yellow fever preventive vaccination campaigns in eight African countries from 2007 to 2010. Vaccine 2013, 31, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Cottin, P.; Niedrig, M.; Domingo, C. Safety profile of the yellow fever vaccine Stamaril®: A 17-year review. Expert Rev. Vaccines 2013, 12, 1351–1368. [Google Scholar] [CrossRef] [PubMed]
- Da Mota, L.M.H.; Oliveira, A.C.V.; Lima, R.A.C.; Dos Santos-Neto, L.L.; Tauil, P.L. Vacinação contra febre amarela em pacientes com diagnósticos de doenças reumáticas, em uso de imunossupressores. Rev. Soc. Bras. Med. Trop. 2009, 42, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, G.L.; Burgess, M.A.; Kass, R.B. Age-Related Risk of Adverse Events Following Yellow Fever Vaccination in Australia. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cda-pubs-cdi-2004-cdi2802-htm-cdi2802o.htm (accessed on 7 November 2021).
- Lindsey, N.P.; Rabe, I.B.; Miller, E.R.; Fischer, M.; Staples, J.E. Adverse event reports following yellow fever vaccination, 2007–13. J. Travel Med. 2016, 23, taw045. [Google Scholar] [CrossRef] [Green Version]
- Martin, M.; Weld, L.H.; Tsai, T.F.; Mootrey, G.T.; Chen, R.T.; Niu, M.; Cetron, M.S.; GeoSentinel Yellow Fever Working Group. Advanced Age a Risk Factor for Illness Temporally Associated with Yellow Fever Vaccination. Emerg. Infect. Dis. 2001, 7, 945–951. [Google Scholar] [CrossRef] [Green Version]
- Martins, R.D.M.; Pavão, A.L.B.; de Oliveira, P.M.N.; dos Santos, P.R.G.; Carvalho, S.M.D.; Mohrdieck, R.; Fernandes, A.; Sato, H.K.; de Figueiredo, P.M.; Doellinger, V.D.R.V.; et al. Adverse events following yellow fever immunization: Report and analysis of 67 neurological cases in Brazil. Vaccine 2014, 32, 6676–6682. [Google Scholar] [CrossRef]
- Monath, T.P.; Marchesani, R.; Thomas, N.; E Shope, R.; Schrader, R.; Nichols, R.; Bedford, P.; Tian, J.; Moore, L.; Furby, D.; et al. Comparative safety and immunogenicity of two yellow fever 17D vaccines (ARILVAX and YF-VAX) in a phase III multicenter, double-blind clinical trial. Am. J. Trop. Med. Hyg. 2002, 66, 533–541. [Google Scholar] [CrossRef]
- Ujo, E.S.A.; Lima, W.J.; Correia, A.M. Segurança da Vacina Contra Febre Amarela em Idosos. Registro da Experiência em um Centro de Referência Para Idosos na Baixada Santista. Braz. J. Infect. Dis. 2018, 22, 66–67. [Google Scholar] [CrossRef]
- Martin, M.; Tsai, T.F.; Cropp, B.; Chang, G.-J.J.; A Holmes, D.; Tseng, J.; Shieh, W.-J.; Zaki, S.R.; Al-Sanouri, I.; Cutrona, A.F.; et al. Fever and multisystem organ failure associated with 17D-204 yellow fever vaccination: A report of four cases. Lancet 2001, 358, 98–104. [Google Scholar] [CrossRef]
- McMahon, A.W.; Eidex, R.B.; Marfin, A.A.; Russell, M.; Sejvar, J.J.; Markoff, L.; Hayes, E.B.; Chen, R.T.; Ball, R.; Braun, M.M.; et al. Neurologic disease associated with 17D-204 yellow fever vaccination: A report of 15 cases. Vaccine 2007, 25, 1727–1734. [Google Scholar] [CrossRef] [PubMed]
- Biscayart, C.; Carrega, M.E.P.; Sagradini, S.; Gentile, Á.; Stecher, D.; Orduna, T.; Bentancourt, S.; Jiménez, S.G.; Flynn, L.P.; Arce, G.P.; et al. Yellow fever vaccine-associated adverse events following extensive immunization in Argentina. Vaccine 2014, 32, 1266–1272. [Google Scholar] [CrossRef] [PubMed]
- Lucena, A.R.F.P.; Souza, L.R.D.O.; Percio, J.; Carvalho, S.M.D.; Romano, A.P.M.; Domingues, C.M.A.S. Fatores associados à gravidade dos eventos adversos pós-vacinação contra a febre amarela durante o maior surto da doença registrado no Brasil, 2016–2017. Epidemiol. Serviços Saúde 2020, 29, e2018331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porudominsky, R.; Gotuzzo, E.H. Yellow fever vaccine and risk of developing serious adverse events: A systematic review. Rev. Panam. Salud Pública 2018, 42, e75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaeger, V.K.; Tschudi, N.; Rüegg, R.; Hatz, C.; Bühler, S. The elderly, the young and the pregnant traveler—A retrospective data analysis from a large Swiss Travel Center with a special focus on malaria prophylaxis and yellow fever vaccination. Travel Med. Infect. Dis. 2015, 13, 475–484. [Google Scholar] [CrossRef]
- Cavalcante, K.R.L.J.; Tauil, P.L. Risco de reintrodução da febre amarela urbana no Brasil. Epidemiol. Serviços Saúde 2017, 26, 617–620. [Google Scholar] [CrossRef]
- Martins, R.D.M.; Leal, M.D.L.F.; Homma, A. Serious adverse events associated with yellow fever vaccine. Hum. Vaccines Immunother. 2015, 11, 2183–2187. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Journal | Data Collection Period | Study Design | Follow up Time | Total Sample Size | Elderly Age Group Assessed | Total Number of Elderlies Assessed | Comorbidities Presented in the Studies | Included in the Meta-Analysis |
|---|---|---|---|---|---|---|---|---|---|
| CDC, 2002 [26] | Morbidity and Mortality Weekly Report | >1 to 3 years | Case series | >1 to 3 years | 6 | 70 to 79 years | 2 | History of cardiovascular disease | No |
| Azevedo et al. 2011 [27] | Transplant Infectious Disease Journal | Missing information | Cross sectional | Missing information | 19 | 60 to 69 years | 2 | History of cardiovascular disease | No |
| Bae et al. 2008 [28] | The Journal of Infectious Diseases | >3 years | Case series | <6 months | 6 | 60 to 69 years | 3 | Missing information | No |
| Biscayart et al. 2014 [40] | Vaccine | 6 months to 1 year | Cross sectional | 6 months to 1 year | 165 | >60 years | 7 | History of cardiovascular disease and allergies | Yes |
| Breugelmans, 2013 [29] | Vaccine | >3 years | Cross sectional | >3 years | 3116 | >60 years | 2 | Missing information | Yes |
| Cottin et al. 2013 [30] | Expert review of vaccines | >3 years | Cross sectional | >3 years | 1460 | >60 years | Missing information * | History of cardiovascular disease and chronic kidney disease | No |
| Mota et al. 2009 [31] | Revista da Sociedade Brasileira de Medicina Tropical | Missing information | Cross sectional | Missing information | 70 | >60 years | 3 | History of immunosuppressive disease | No |
| Khromava et al. 2005 [18] | Vaccine | >3 years | Cohort | >3 years | 722 | >60 years | 58 | Missing information | Yes |
| Lawrence et al. 2004 [32] | Communicable Diseases Intelligence Quarterly Report | >3 years | Cross sectional | <6 years | 42 | >60 years | Missing information * | Missing information | Yes |
| Lindsey et al. 2016 [33] | Journal of Travel Medicine | >3 years | Cross sectional | >3 years | 938 | >60 years | Missing information * | Missing information | Yes |
| Martin et al. 2001 [38] | Emerging infectious diseases | >3 years | Cross sectional | >3 years | 5125 | >60 years | 285 | Missing information | Yes |
| Martins et al. 2014 [35] | Vaccine | >3 years | Cross sectional | >3 years | 67 | >60 years | Missing information * | History of immunosuppressive disease | Yes |
| Lindsey et al. 2008 [4] | Vaccine | >3 years | Cross sectional | >3 years | 660 | >60 years | 97 | Missing information | Yes |
| Monath et al. 2002 [36] | The American journal of tropical medicine and hygiene | <6 months | Randomized clinical trial | <6 months | 1440 | >60 years | 123 | Missing information | Yes |
| Araujo et al. 2018 [37] | The Brazilian Journal of Infectious Diseases | 6 months to 1 year | Cohort | 6 months to 1 year | 131 | >60 years | 131 | History of immunosuppressive and cardiovascular diseases and diabetes | Yes |
| Martin et al. 2001 [38] | The Lancet | 6 months to 1 year | Case series | <6 months | 4 | >60 years | 4 | History of cardiovascular disease and chronic kidney disease | No |
| McMahon et al. 2006 [39] | Vaccine | 6 months to 1 year | Cross sectional | 6 months to 1 year | 15 | >60 years | 6 | Missing information | No |
| Lucena et al. 2020 [41] | Epidemiologia e Serviços de Saúde | >1 to 3 years | Case control | >1 to 3 years | NA | >60 years | NA | Missing information | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Abreu, A.d.J.L.; Cavalcante, J.R.; de Araújo Lagos, L.W.; Caetano, R.; Braga, J.U. A Systematic Review and a Meta-Analysis of the Yellow Fever Vaccine in the Elderly Population. Vaccines 2022, 10, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050711
de Abreu AdJL, Cavalcante JR, de Araújo Lagos LW, Caetano R, Braga JU. A Systematic Review and a Meta-Analysis of the Yellow Fever Vaccine in the Elderly Population. Vaccines. 2022; 10(5):711. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050711
Chicago/Turabian Stylede Abreu, Ariane de Jesus Lopes, João Roberto Cavalcante, Letícia Wigg de Araújo Lagos, Rosângela Caetano, and José Ueleres Braga. 2022. "A Systematic Review and a Meta-Analysis of the Yellow Fever Vaccine in the Elderly Population" Vaccines 10, no. 5: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050711