Factors Influencing COVID-19 Vaccine Uptake among Nepali People in the UK: A Qualitative Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Design and Sites
2.2. Participant Selection and Data Collection Methods
- What do you think about the COVID-19 vaccine? If offered today, will you be willing to take the COVID-19 vaccine?
- If you have already been vaccinated, what motivated you to take the vaccine?
- In your opinion, why do you think that people come for the COVID-19 vaccination? Why don’t they come for the COVID-19 vaccination?
2.3. Data Analysis
2.4. Ethical Consideration
3. Results
3.1. Motivation for the COVID-19 Vaccination
- (a)
- Personal safety
I’ve seen the family being wiped out with the infection. I’ve seen the devastation. This virus works in a very strange way, we are slowly starting to understand … I don’t want them to be hospitalised and wanted to get vaccinated as soon as possible … Thankfully, I got my first vaccination. So, hopefully, in the next few weeks, I’ll get my second one as well.(P 8, Health Worker)
I would strongly advise everybody to get the vaccine. These have been rigorously tested and now millions of people have been vaccinated. So, we have crossed seven million in terms of vaccination in the UK. So, nobody’s been admitted or had any serious side effects. The vaccine is safe; that was the motivation to go for [the] jab.(P 12, Health Worker)
- (b)
- To save other people
I took vaccines as a part of infection prevention measures. I have to keep myself safe so that I can keep my family safe as my wife is with me now. The main motivation was for infection prevention.(P 3, Health Worker)
People also know that there might be side-effects, but the risk of dying is more dangerous than the side-effects, and [we should] promote the vaccine using local community leaders.(P 11, Community Leader)
- (c)
- Trusted on science and evidence to control the pandemic
The COVID-19 vaccine has been made after many studies and the government has declared it safe, so I do not see any reason to be worried. The vaccine will protect us as individuals as well as reduce infection.(P 11, Community Leader)
I believe in science and the only way we can get out of this is to vaccinate. We have waited and waited and waited, the herd immunity [herd immunity occurs when a large portion of a community becomes immune to a disease, making the spread of disease from person to person unlikely] never happened …. social distancing and lockdown did not work much. So, the only way out is now getting everybody vaccinated.(P 6, Health Worker)
I was better informed because I know about these vaccines. I take my flu vaccine every year. I’ve done that for 20 years now. I had probably had all childhood vaccinations. I know how rigorously the [vaccine] production [is, and] the safety and their approval processes are. So, I didn’t have any doubt whatsoever [and] that fostered me to take jab.(P 2, Community Leader)
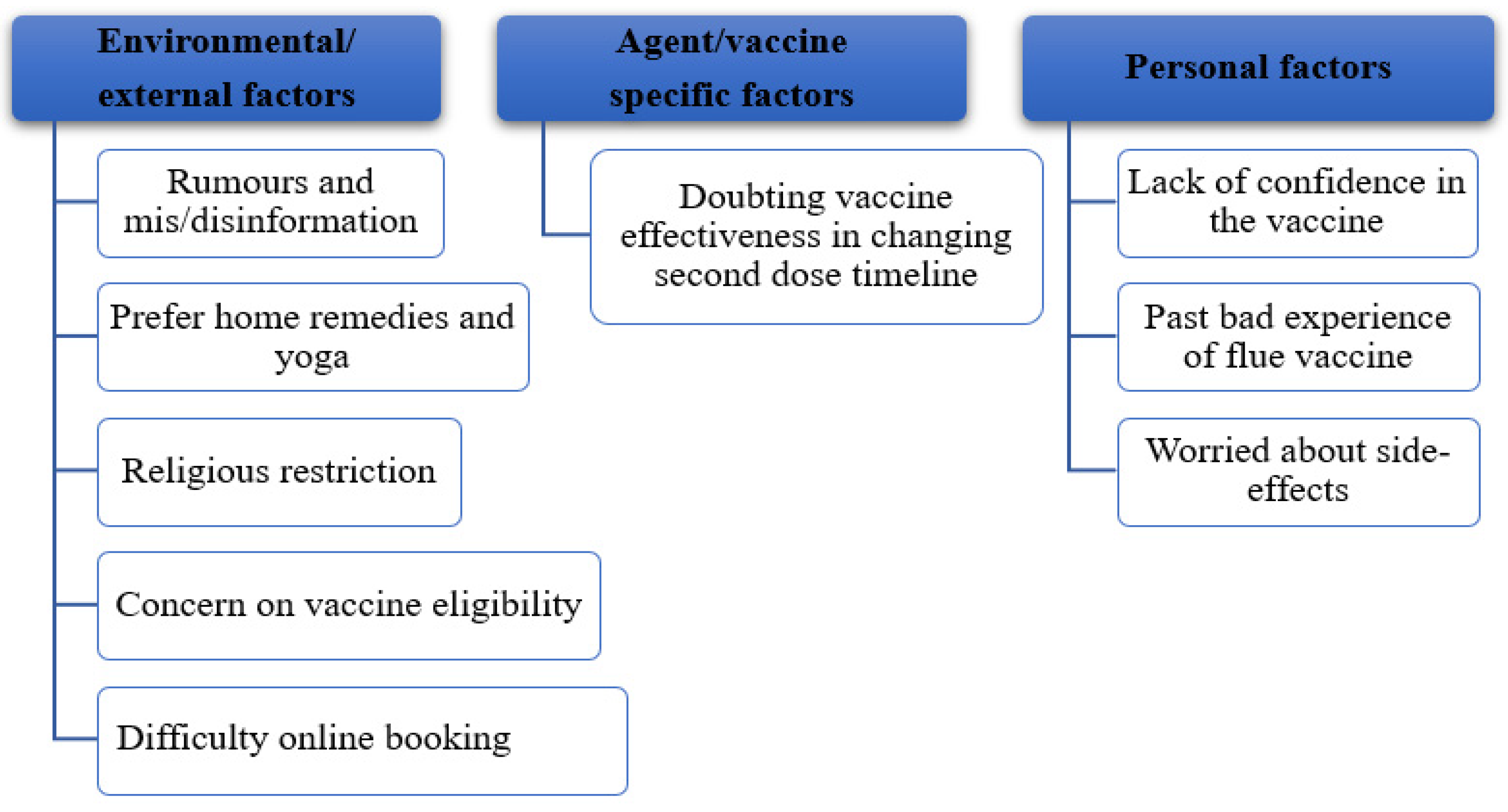
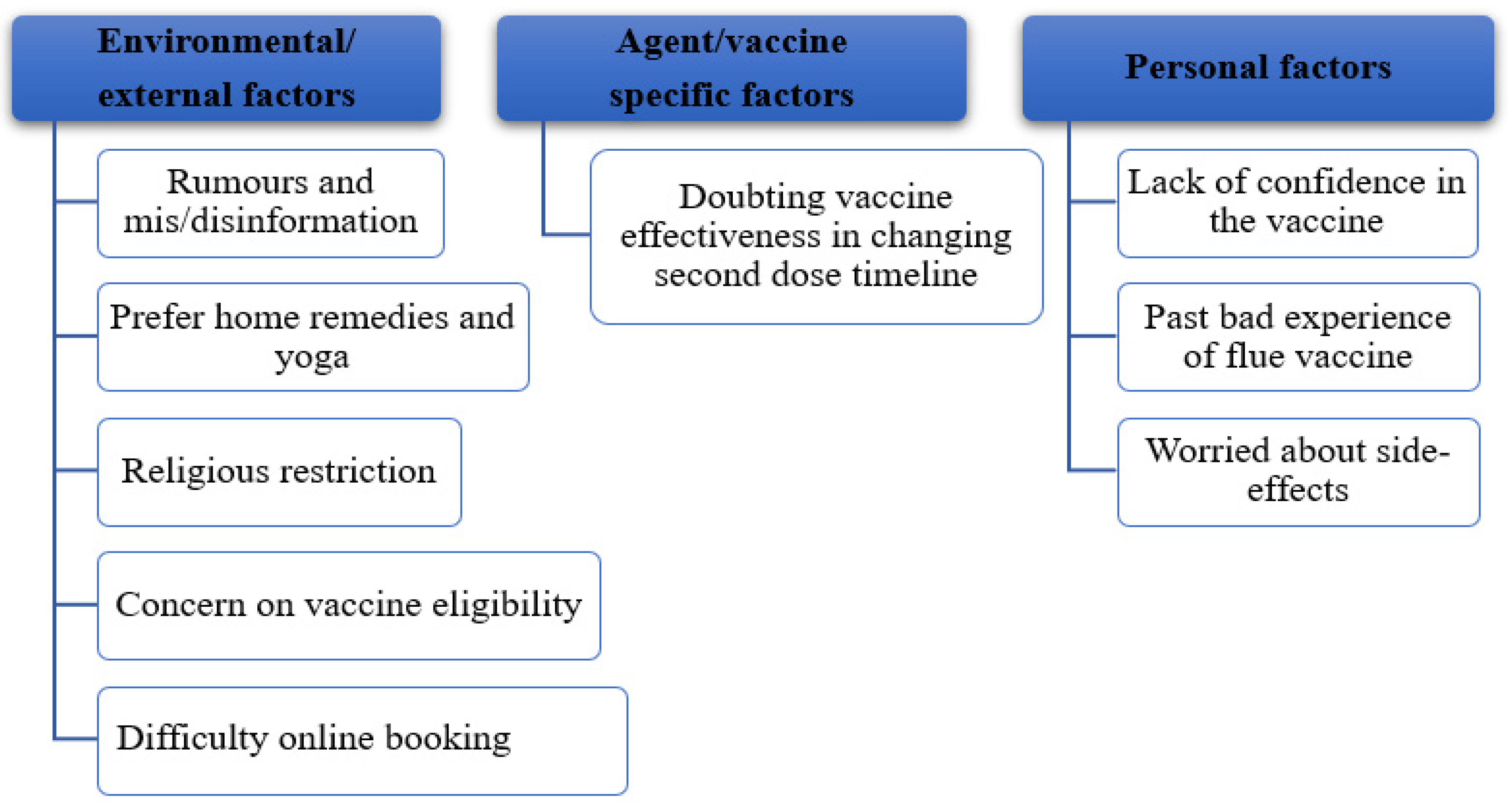
3.2. Barriers to the Uptake of the COVID-19 Vaccine
- (1)
- Environmental/External Factors
3.2.1. Rumours and Dis/Misinformation Regarding the Vaccine
I know that in our media, our social media, the South Asian media, negativity sells quicker, and they have been there pointing out the negative side of the vaccine more than the positive things of it.(P 6, Health Worker)
I think some people are just being bombarded with misinformation over social media.(P 2, Community Leader)
There [is] lots of fake news over WhatsApp, Facebook and in everything. So, I think this social media is making another trouble. Yes, my wife asked the same question when she went for the vaccine.(P 14, Ordinary Nepali Person in the Community)
I was looking at Facebook earlier today as well, a lot of my friends who are talking about side-effects, you know, what sort of side-effects did you get and they’ve started a poll as well saying, you know, like, with lots of symptoms, saying minor, major or serious symptoms but it’s very, very rare.(P 8, Health Worker)
Some people might not be getting their answer like me, some White colleagues at my workplace fear … [a] long-term side-effect that might happen, some Muslim colleagues at the beginning said they don’t want [it] because the vaccine is made out of pork.(P 9, Health Worker)
There is multiple information in social media where it says that the trial has not been completed for the vaccines and the long-term effect of the vaccine is still uncertain. So, there are a group of people who say that due to these reasons, the vaccine shouldn’t be taken.(P 3, Health Worker)
3.2.2. Home Remedies and Yoga
Most people are using home remedies such as turmeric, ginger water, pepper tea, drinking plenty of water, massage at night with mustard oil. Open windows every day to let the fresh air in, sleep on time and do exercise regularly.(P 16, Ordinary Nepali Person in the Community)
I take raw turmeric, Ajawin, cumin seeds with warm water in a big glass and then go to work. I also take steam every day. Again, after coming from work, I take [a] shower and then follow the same home remedies. Sometimes I take basil leaves, ginger and many other home remedies. I use turmeric every day twice a day with Ajawin, cumin seed, [and] ginger with warm water.(P 9, Health Worker)
My neighbour was saying that his medical doctor, who is also British, suggested to take home remedies rather than vaccination. So, I was shocked to hear that there is a medical practitioner who doesn’t believe in vaccination.(P 3, Health Worker)
I do meditation every morning, after doing that my body feels so relaxed. I do [it] every morning and maintain the balance of my body. That helps me to avoid stress when I go to work. I feel relaxed and this helps to keep anxiety and stress levels very low. When we do such yoga and meditation, then there is a development of positive hormones in our body.(P 9, Health Worker)
3.2.3. Religious Restrictions
Well, this country [UK] is full of cultures. Some of them religiously can’t take a serum and vaccinations, so, people have a diverse opinion about the vaccine. Probably that’s why they don’t want to take this.(P 13, Health Worker)
Very few people, they don’t believe [that] vaccines work for COVID-19 which may be the reason from their culture and religion.(P 2, Community Leader)
3.2.4. Concern about Vaccine Eligibility
I’m breastfeeding at the moment and should not be vaccinated when you are breastfeeding. So, I’m hoping to get one when my baby will have solid food and I would not be breastfeeding. I might get it after six-months.(P 13, Health Worker)
3.2.5. Difficulty with the Online Vaccine Booking System
To take a vaccine is not easy in the UK where we need to take an appointment which is not easy for all our [Nepali] community. You know that a large proportion of the Nepali community in the UK are Gurkha families [retired British army] which is not easy to make an appointment and vaccinate due to the system.(P 3, Health Worker)
I do not understand the guideline given by the Government as they are in the English language. I do not know much English, and my wife does not know any English at all. We have a big problem when we go to General Practitioners. They provide health information in many local languages, but we do not have it in Nepali. I can speak some English but when my wife has appointments, they ask to come one person only so it’s difficult for her as she does not understand English at all.(P 4, Ordinary Nepali Person in the Community)
While booking an appointment we cannot understand the English properly so we cannot ask for an interpreter too. Before COVID-19, we could go to the clinic and book in person, which was easy, but phone booking takes a long wait and [it is] very difficult to understand English too. It took me 1 h 45 min last week to book an appointment for a vaccine. This is not practical [for] everyone.(P 4, Ordinary Nepali Person in the Community)
- (1)
- Agent/vaccine-specific factors
3.2.6. Doubt of Vaccine Effectiveness after Changing the Second Dose Timeline
The most important thing … is the conflicting information that the British government has been providing and irritating people. For example, the leaflet that we are given during the vaccination says that both the doses of vaccine should be taken within 21 days otherwise it won’t be effective. However, the government made a policy where people will get the second dose in 12 weeks with the intention that the first dose has to cover a maximum number of people. A medical scientist has been saying that the maximum gap is six weeks. After that, there aren’t any benefits of the vaccine from first to second doses. But the government ignored the scientific evidence and brought a rule of [a] 12-week gap between the doses. So, when such conflicting information comes to the media then people get very much confused about the decision.(P 3, Health Worker)
I have a question about [the] vaccine which I have not got answered yet, how long will this vaccine work? Whether it will work for one year, 10 years or forever? I didn’t get an answer to this question. Now, there is another thing, when this vaccine was developed it was COVID-19, but now there are different new variants. So, I don’t know whether it will work for this or not.(P 9, Health Worker)
- (1)
- Host/Person-Specific Factors
3.2.7. Lack Confidence in the Vaccine
One of my staff didn’t want…the vaccination and I asked the reason and she said this is her choice and she doesn’t feel safe.(P 14, Ordinary Nepali Person in the Community)
I heard from someone or read somewhere that this vaccination does not protect us against COVID infection, rather it only prevents us from getting worse from infection.….I have not found anyone who has [been] vaccinated and is well protected from COVID-19.(P 16, Ordinary Nepali Person in the Community)
It is also unsure whether [the vaccine] will work [for] the new strain or not. This is also one of the reasons for people not believing [in] the vaccines.(P 3, Health Worker)
I have not taken a jab yet. I am not saying that I don’t want to, but I want to see the side-effects and how it will go. It has been developed so fast and is used so quickly. I am just wondering that it might affect everyone at once when it’s used. At present, I have no fear and I am managing well. I will take the vaccine a little later. I have three questions that are not clear to me about this vaccine. So, I am delaying [it].(P 9, Health Worker)
3.2.8. Past Bad Experience with the Influenza Vaccine
Ram [name changed] in his late 40′s has been working in [the] NHS for more than 10 years as a health support staff [member]. Since the start of the COVID-19 pandemic, he has worked in contact with COVID-19-positive cases admitted to the hospital for treatment. But Ram is reluctant to take the COVID-19 vaccine. Despite being the priority group for the vaccine programme as a frontline worker, he says that he doesn’t want to take the vaccine and has been “escaping from his vaccination”. His supervisor has been continuously doing follow-ups for the vaccine. However, Ram has been postponing it every time, saying that he will take it later. Ram has had the flu vaccine in the past, and he suffered from severe side-effects of the flu vaccine. He was ill for more than 2 weeks after taking the flu vaccine. He had [a] fever for about two to three weeks and some people told him that he developed [a] fever due to the flu vaccine. Since then, Ram completely left out taking the flu vaccine. Ram fears that the COVID-19 vaccine will do the same to him and he doesn’t want to go for a jab because of the fear of side effects. He heard, as well as [he] read somewhere, that the currently offered vaccination does not protect against COVID-19 infection, rather it only prevents from getting worse from infection only. It saves [you] from getting worse, [and does] not protect [you] from getting the infection. Steve [name changed] also told Ram that he took the first dose of the vaccine and felt sick, and he has been asking Ram for suggestions on how to skip the second dose, which doubled Ram’s fear of vaccine side-effect. Ram believes in following natural processes like sleeping on time, eating on time, eating healthy food, doing regular exercise, drinking plenty of water and avoiding alcohol. Ram believes that this will help him against COVID-19 attacks. Ram will only take the vaccine if there are rules which say that people who do not get vaccinated will have travel restrictions, or if everybody in the UK is vaccinated except him. When Ram sees everyone is safe after getting the vaccine, then he will feel confident that nothing happens and will gain trust towards the vaccine.(P 16, Health Worker)
3.2.9. Being Worried about Side-Effects
I did get some side-effects with the second dose of the vaccine for about two days. I was getting chills, very cold and unwell but I have fully recovered. Nothing serious happened.(P 12, Health Worker)
My wife and I … our arm was very, very sore the next day, which was fine.(P 8, Health Staff)
I have heard mixed feelings about the side-effects of the vaccine. Some people say they have mild pain and flu-like symptoms. Some people say it’s only niggling in the hand, not much really. Some people have headaches and [are] feverish.(P 13, Health Worker)
I have heard and seen immediate side-effects of the vaccine. I have seen-side effects on my other colleagues, [and] older people at the care homes. I wanted to see but I don’t know anything about the long-term side-effects. Lots of other vaccines are coming and other vaccines worked so far, [more] than the current one.(P 9, Health Worker)
The side-effects that I experienced were fever after 2–3 weeks. Some people said that I developed a fever due to the flu vaccine. So, I completely left out taking the flu vaccine. I felt it was better without a vaccine.(P 16, Community Leader)
Very few people may worry about [the] jab because they might have a severe allergic reaction to the vaccine.(P 2, Community Leader)
4. Discussion
4.1. Motivations to Take a COVID-19 Vaccine
4.2. Barriers to Uptake of the COVID-19 Vaccine
- (1)
- Environmental factors
- (2)
- Vaccine-specific factors
- (3)
- Personal factors
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. COVID-19 in Racial and Ethnic Minority Groups. February 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/racial-ethnic-minorities.html (accessed on 24 July 2021).
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Mills, M.; Rahal, C.; Brazel, D.; Yan, J.; Gieysztor, S. COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies; The Royal Society & The British Academy: London, UK, 2020. [Google Scholar]
- COVID-19. Vaccines Tracker: Vaccines Candidates in Clinical Trials. 2021. Available online: https://covid19.trackvaccines.org/vaccines/ (accessed on 24 December 2021).
- Jegede, A.S. What led to the Nigerian boycott of the polio vaccination campaign? PLoS Med. 2007, 4, e73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khattak, F.A.; Rehman, K.; Shahzad, M.; Arif, N.; Ullah, N.; Kibria, Z.; Arshad, M.; Afaq, S.; Ibrahimzai, A.K.; Haq, Z.U. Prevalence of Parental refusal rate and its associated factors in routine immunization by using WHO Vaccine Hesitancy tool: A Cross sectional study at district Bannu, KP, Pakistan. Int. J. Infect. Dis. 2021, 104, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J.; Nuzhath, T.; Colwell, B. Combating vaccine hesitancy and other 21st century social determinants in the global fight against measles. Curr. Opin. Virol. 2020, 41, 1–7. [Google Scholar] [CrossRef]
- Wilder-Smith, A.B.; Qureshi, K. Resurgence of measles in Europe: A systematic review on parental attitudes and beliefs of measles vaccine. J. Epidemiol. Glob. Health 2020, 10, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velan, B.; Kaplan, G.; Ziv, A.; Boyko, V.; Lerner-Geva, L. Major motives in non-acceptance of A/H1N1 flu vaccination: The weight of rational assessment. Vaccine 2011, 29, 1173–1179. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- WHO. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Ledford, H. Six Months of COVID Vaccines: What 1.7 Billion Doses Have Taught Scientists. Nature 2021, 594, 164–167. [Google Scholar] [CrossRef]
- OWiD. Statistics and Research Coronavirus (COVID-19) Vaccinations. 2021. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 23 December 2021).
- COVID-19. COVID-19 Vaccine Tracker: The global Race to Vaccinate. 2021. Available online: https://ig.ft.com/coronavirus-vaccine-tracker/?areas=gbr&areas=isr&areas=usa&areas=eue&areas=can&areas=chn&areas=ind&cumulative=1&doses=total&populationAdjusted=1 (accessed on 24 December 2021).
- WHO. Coronavirus Disease (COVID-19): Vaccines. February 2021. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-(covid-19)-vaccines?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQiAj9iBBhCJARIsAE9qRtDDyahb4vd2_aa6WE6A70yL5l1lN4-aO7x50MqzMzPIrKUqV-4Jg_EaAvXCEALw_wcB (accessed on 5 February 2021).
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- QRsearch. Factors Influencing COVID-19 Vaccine Uptake among Minority Ethnic Groups. 2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/952716/s0979-factors-influencing-vaccine-uptake-minority-ethnic-groups.pdf (accessed on 5 February 2021).
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF joint reporting form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. medRxiv 2020, 39, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccin. Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, M.; Sahin, M.K. Parents’ willingness and attitudes concerning the COVID-19 vaccine: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14364. [Google Scholar] [CrossRef]
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 94, 41–50. [Google Scholar] [CrossRef]
- WHO. Behavioural Considerations for Acceptance and Uptake of COVID-19 Vaccines: Who Technical Advisory Group on Behavioural Insights and Sciences for Health; Meeting Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Miller, R.E. Epidemiology for Health Promotion and Disease Prevention Professionals; Routledge: New York, NY, USA, 2002. [Google Scholar]
- Simkhada, B.; Sah, R.K.; Mercel-Sanca, A.; van Teijlingen, E.; Bhurtyal, Y.M.; Regmi, P. Perceptions and experiences of health and social care utilisation of the UK-Nepali population. J. Immigr. Minority Health 2020, 23, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Kamal, A.; Hodson, A.; Pearce, J.M. A rapid systematic review of factors influencing COVID-19 vaccination uptake in minority ethnic groups in the UK. Vaccines 2021, 9, 1121. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 4th ed.; University of Nebraska: Lincoln, SD, USA; Los Angeles, CA, USA; Sage Publication: London, UK, 2014. [Google Scholar]
- Bowling, A. Research Methods in Health: Investigating Health and Health Services, 2nd ed.; McGraw-Hill Education: London, UK, 2002. [Google Scholar]
- Wang, P.-W.; Ahorsu, D.; Lin, C.Y.; Chen, I.H.; Yen, C.F.; Kuo, Y.J.; Griffiths, M.; Pakpour, A. Motivation to have COVID-19 vaccination explained using an extended protection motivation theory among university students in china: The role of information sources. Vaccines 2021, 9, 380. [Google Scholar] [CrossRef]
- WSDH. COVID-19 Vaccine Qualitative Research Report; Washington State Department of Health: Washington, DC, USA, 2021. [Google Scholar]
- Tannenbaum, M.B.; Hepler, J.; Zimmerman, R.S.; Saul, L.; Jacobs, S.; Wilson, K.; Albarracín, D. Appealing to fear: A meta-analysis of fear appeal effectiveness and theories. Psychol. Bull. 2015, 141, 1178. [Google Scholar] [CrossRef] [Green Version]
- Li, H.O.-Y.; Bailey, A.; Huynh, D.; Chan, J. YouTube as a source of information on COVID-19: A pandemic of misinformation? BMJ Glob. Health 2020, 5, e002604. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; McKee, M.; Torbica, A.; Stuckler, D. Systematic literature review on the spread of health-related misinformation on social media. Soc. Sci. Med. 2019, 240, 112552. [Google Scholar] [CrossRef] [PubMed]
- Balami, A.D.; Meleh, H.U. Misinformation on salt water use among Nigerians during 2014 Ebola outbreak and the role of social media. Asian Pac. J. Trop. Med. 2019, 12, 175. [Google Scholar] [CrossRef]
- Bora, K.; Das, D.; Barman, B.; Borah, P. Are Internet videos useful sources of information during global public health emergencies? A case study of youtube videos during the 2015–2016 Zika virus pandemic. Pathog. Glob. Health 2018, 112, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Garett, R.; Young, S.D. Online misinformation and vaccine hesitancy. Transl. Behav. Med. 2021, 11, 2194–2199. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Eshun-Wilson, I.; Mody, A.; Tram, K.H.; Bradley, C.; Scheve, A.; Fox, B.; Thompson, V.; Geng, E.H. Strategies that make vaccination easy and promote autonomy could increase COVID-19 vaccination in those who remain hesitant. medRxiv 2021. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.-L.; Yau, P.S.Y.; Dong, D.; Wong, S.Y.S.; Yeoh, E.K. Change of willingness to accept COVID-19 vaccine and reasons of vaccine hesitancy of working people at different waves of local epidemic in Hong Kong, China: Repeated cross-sectional surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the US. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar] [CrossRef]
- Uscinski, J.E.; Enders, A.M.; Klofstad, C.; Seelig, M.; Funchion, J.; Everett, C.; Wuchty, S.; Premaratne, K.; Murthi, M. Why do people believe COVID-19 conspiracy theories? Harv. Kennedy Sch. Misinform. Rev. 2020, 1, 1–12. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.; Moniz, M.; Gama, A.; Laires, P.; Pedro, A.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. Acceptance of COVID-19 vaccination in the elderly: A cross-sectional study in Southern Italy. Vaccines 2021, 9, 1222. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 vaccine hesitancy and attitude toward booster doses among US healthcare workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef]
- Haghpanah, F.; Lin, G.; Levin, S.A.; Klein, E. Analysis of the potential impact of durability, timing, and transmission blocking of COVID-19 vaccine on morbidity and mortality. EClinicalMedicine 2021, 35, 100863. [Google Scholar] [CrossRef] [PubMed]
- Marti, M.; de Cola, M.; Macdonald, N.E.; Dumolard, L.; Duclos, P. Assessments of global drivers of vaccine hesitancy in 2014—Looking beyond safety concerns. PLoS ONE 2017, 12, e0172310. [Google Scholar] [CrossRef] [Green Version]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Willingness to receive COVID-19 vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef]
- Avorn, J.; Kesselheim, A. Regulatory decision-making on COVID-19 vaccines during a public health emergency. JAMA 2020, 324, 1284–1285. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Number | % |
|---|---|---|
| Gender | ||
| Male | 14 | 70.0 |
| Female | 6 | 30.0 |
| Age (Median age) | 46 years | |
| Age ranges in years | 34–72 | |
| Participants’ affiliations | ||
| Retired /Gurkha’s family) | 10 | 50.0 |
| Health worker (doctor, nurse, pharmacist, care workers) | 7 | 35.0 |
| Community leaders | 3 | 15.0 |
| Vaccination status | ||
| Vaccinated | 10 | 50.0 |
| Nonvaccinated | 10 | 50.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simkhada, P.; Tamang, P.; Timilsina, L.; Simkhada, B.; Bissell, P.; van Teijlingen, E.; Sah, S.K.; Wasti, S.P. Factors Influencing COVID-19 Vaccine Uptake among Nepali People in the UK: A Qualitative Study. Vaccines 2022, 10, 780. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050780
Simkhada P, Tamang P, Timilsina L, Simkhada B, Bissell P, van Teijlingen E, Sah SK, Wasti SP. Factors Influencing COVID-19 Vaccine Uptake among Nepali People in the UK: A Qualitative Study. Vaccines. 2022; 10(5):780. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050780
Chicago/Turabian StyleSimkhada, Padam, Pasang Tamang, Laxmi Timilsina, Bibha Simkhada, Paul Bissell, Edwin van Teijlingen, Sunil Kumar Sah, and Sharada Prasad Wasti. 2022. "Factors Influencing COVID-19 Vaccine Uptake among Nepali People in the UK: A Qualitative Study" Vaccines 10, no. 5: 780. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050780