
Adult Hepatitis B Virus Vaccination Coverage in China from 2011 to 2021: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Protocol Registration and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
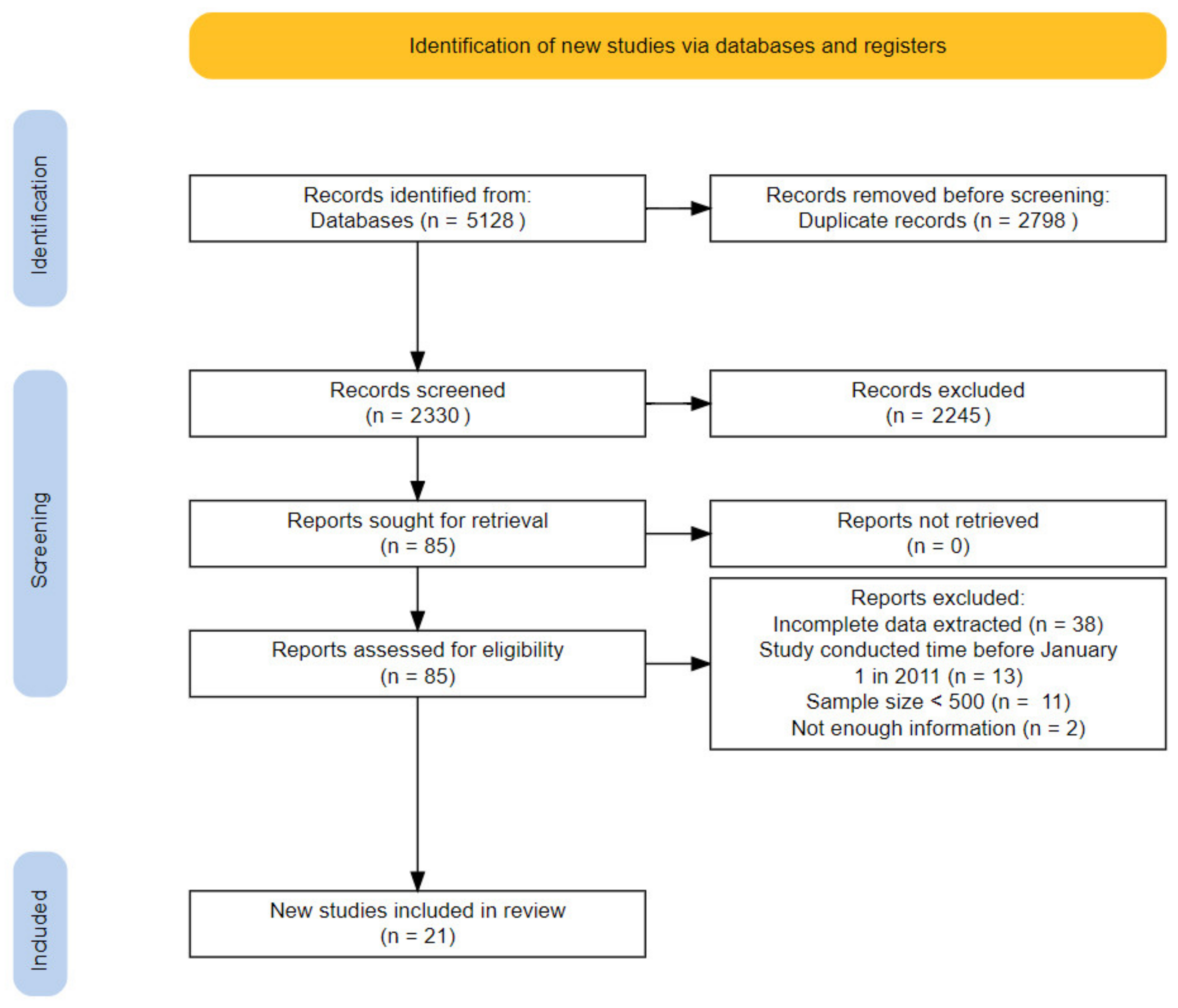
3.1. Study Selection and Characteristics of the Included Studies
3.2. Study Quality
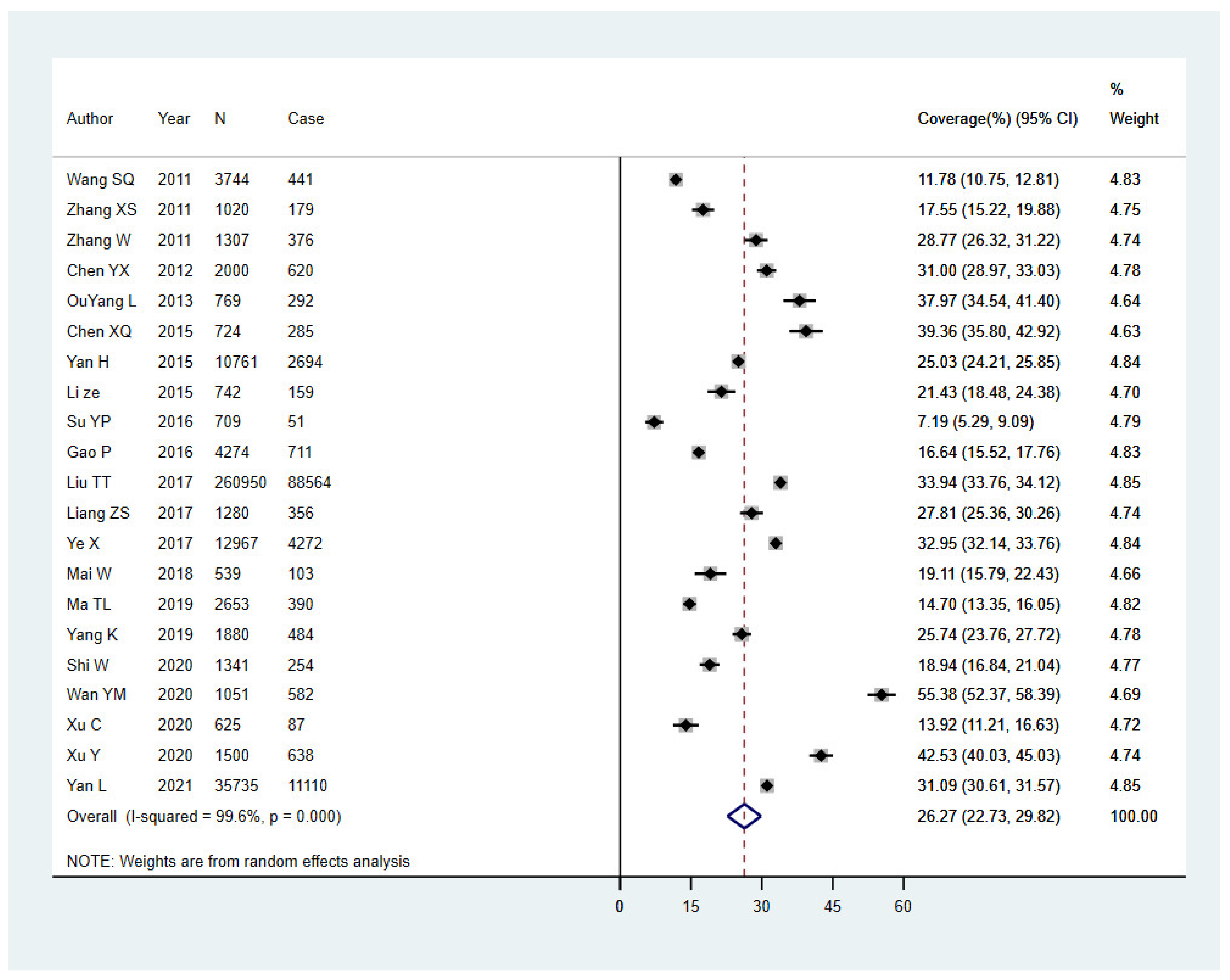
3.3. Pooled Proportion of Hepatitis B Vaccine Uptake
3.4. Subgroup Analysis
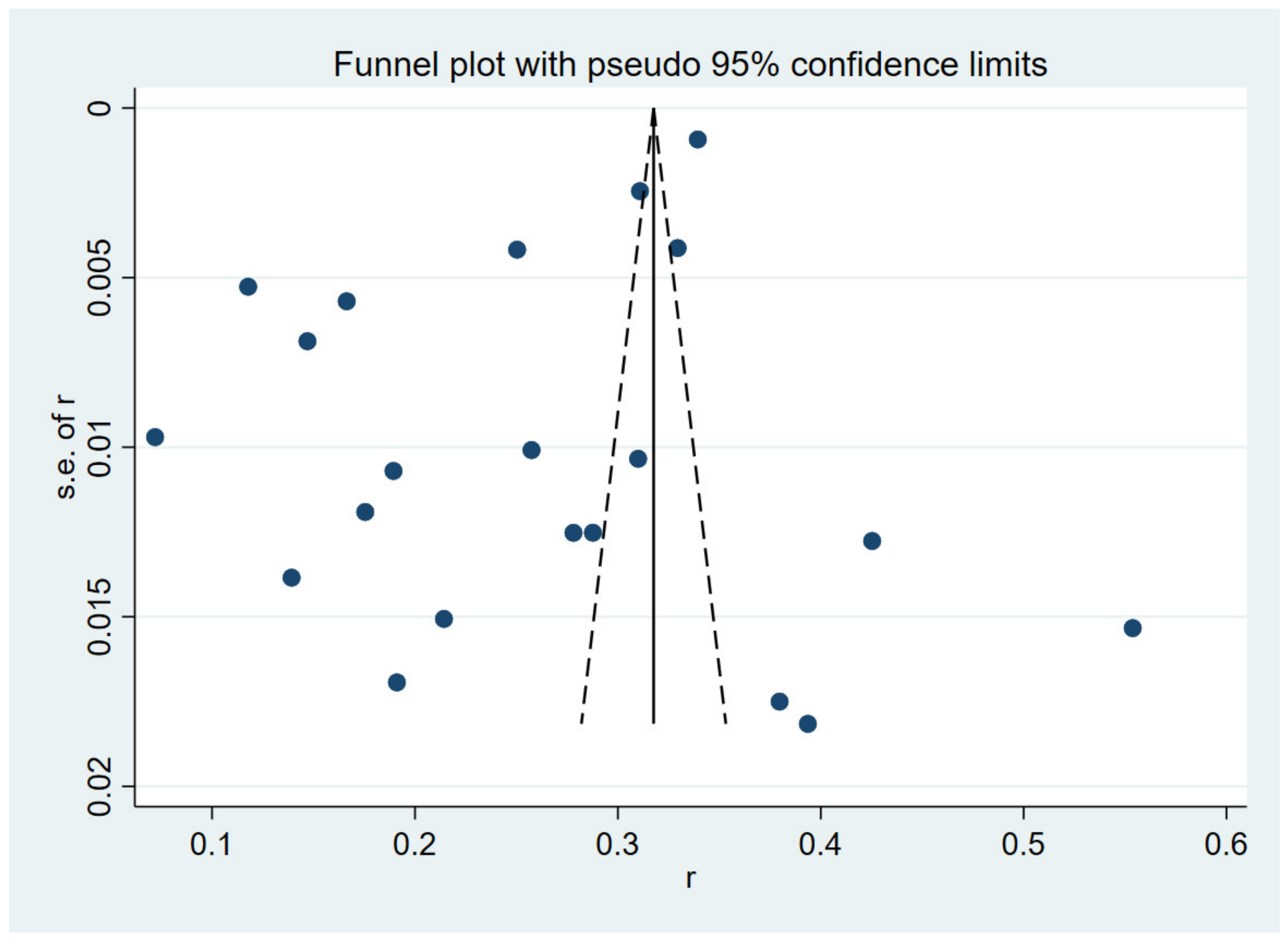
3.5. Heterogeneity and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health-Sector Strategies 2016–2021: Actions for Impact; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. 2016. Available online: http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en (accessed on 5 May 2022).
- Miao, N.; Zheng, H.; Sun, X.; Wang, F.; Zhang, G.; Yin, Z. Acute Hepatitis B—China, 2005−2019. China CDC Wkly. 2020, 2, 559–563. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. Available online: http://www.nhc.gov.cn/jkj/s3578/202204/4fd88a291d914abf8f7a91f6333567e1.shtml (accessed on 4 May 2022).
- Wang, H.; Men, P.; Xiao, Y.; Gao, P.; Lv, M.; Yuan, Q.; Chen, W.; Bai, S.; Wu, J. Hepatitis B infection in the general population of China: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 811. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Smith, H.; Peng, Z.; Xu, B.; Wang, W. Increasing Coverage of Hepatitis B Vaccination in China. Medicine 2016, 95, e3693. [Google Scholar] [CrossRef] [PubMed]
- Cui, F.; Shen, L.; Li, L.; Wang, H.; Wang, F.; Bi, S.; Liu, J.; Zhang, G.; Wang, F.; Zheng, H.; et al. Prevention of Chronic Hepatitis B after 3 Decades of Escalating Vaccination Policy, China. Emerg. Infect. Dis. 2017, 23, 765–772. [Google Scholar] [CrossRef] [Green Version]
- Jing, W.; Liu, J.; Liu, M. Eliminating mother-to-child transmission of HBV: Progress and challenges in China. Front. Med. 2020, 14, 21–29. [Google Scholar] [CrossRef]
- Cui, J.; Cao, L.; Zheng, J.; Cao, L.; Duo, M.; Xiao, Q. Reported coverage of vaccines in the national immunization program of China, 2015. Chin. J. Vacc. Imm. 2017, 06, 601–607. [Google Scholar]
- Cui, F.Q. Technical guide for adult hepatitis B immunization in China. Zhonghua Liu Xing Bing Xue Za Zhi 2011, 32, 1199–1203. [Google Scholar]
- Leidner, A.J.; Murthy, N.; Chesson, H.W.; Biggerstaff, M.; Stoecker, C.; Harris, A.M.; Acosta, A.; Dooling, K.; Bridges, C.B. Cost-effectiveness of adult vaccinations: A systematic review. Vaccine 2019, 37, 226–234. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddaway, N.R.; McGuinness, L.A.; Pritchard, C.C. PRISMA2020: R Package and ShinyApp for Producing PRISMA 2020 Compliant Flow Diagrams, Version 0.0.2; GitHub: San Francisco, CA, USA, 2021. [Google Scholar] [CrossRef]
- Atkins, D.; Fink, K.; Slutsky, J. Better information for better health care: The Evidence-based Practice Center program and the Agency for Healthcare Research and Quality. Ann. Intern. Med. 2005, 142, 1035–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulley, W.R.; Le, S.T.T.; Ives, K.E. Primary seroresponses to double-dose compared with standard-dose hepatitis B vaccination in patients with chronic kidney disease: A systematic review and meta-analysis. Nephrol. Dial. Transpl. 2016, 32, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Dong, Y.; Chen, X.; Liu, Y.; Ma, D.; Liu, X.; Zheng, R.; Mao, X.; Chen, T.; He, W. Prevalence of suicide attempts among Chinese adolescents: A meta-analysis of cross-sectional studies. Compr. Psychiat. 2015, 61, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- George, B.J.; Aban, I.B. An application of meta-analysis based on DerSimonian and Laird method. J. Nucl. Cardiol. 2015, 23, 690–692. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.Q.; Ji, Q.; Huang, H. Analysis of hepatitis B vaccination and hepatitis B virus infection in residents over 20 years old. Chin. J. Prev. Med. 2011, 9, 855–856. [Google Scholar]
- Zhang, X.; Li, H.; Wang, X.; Li, X.; Tang, Y.; Liu, C.; Li, F.; Fu, H.; Liu, J.; Gao, L.; et al. Survey of hepatitis B vaccination coverage in population aged 1~59 years in Gansu Province. China Trop. Med. 2011, 9, 1083–1084. [Google Scholar]
- Zhang, W.; Niu, J.; Li, Z.; Wang, Z. Investigation on Coverage of Hepatitis B Vaccine and Influencing Factor in the Population Aged 15-59 Years in Lanzhou City. Chin. J. Vaccines Immun. 2011, 3, 216–219. [Google Scholar]
- Chen, Y. Effect analysis of adult hepatitis B vaccine vaccination in Huankou Town, Fengxian County. For All Health 2012, 6, 62–63. [Google Scholar]
- OuYang, L. Analysis of Changsha city adults of hepatitis B active vaccine and influencing factors. Natl. Med. Front. China 2013, 8, 113–114. [Google Scholar]
- Chen, X. Current situation and influencing factors of active hepatitis B vaccine vaccination in adults. China Clin. Pract. Med. 2015, 6, 52–53. [Google Scholar]
- Yan, H.; Yan, N. Analysis of the factors affecting active hepatitis B vaccination in adults. J. Qiqihar Univ. Med. 2015, 36, 3063–3064. [Google Scholar]
- Li, Z.; Liu, J.; Shen, Y. Survey of Hepatitis B Immunization and Serological Markers of HBV in Dali. J. Dali Univ. 2015, 14, 13–16. [Google Scholar]
- Su, Y.P.; Wang, B.L.; Liu, X.J.; Liu, H.; Guo, X.H. Influencing factors of vaccination rate of hepatitis B vaccine among people over 20 years old in Tongzhou District, Beijing. Mod. Prev. Med. 2016, 43, 3999–4002. [Google Scholar]
- Gao, P.; Wang, H.; Chen, W.; Sun, Y.; Zhang, W.; Pang, X.; He, X.; Wu, J. A sero-epidemiological study of hepatitis B among general population in Beijing. Chin. J. Epidemiol. 2016, 6, 658–662. [Google Scholar]
- Liu, T.; Zhou, X.; Li, W.; Peng, Y.; Liu, X.; Wang, J.; Ren, T.; Wang, L.; Yuan, P. The prevalence and related factors of HBV infection among adults in Mianyang. Chin. J. Prev. Med. 2017, 51, 837–842. [Google Scholar]
- Liang, Z. Analysis of the factors affecting the active hepatitis B vaccine vaccination in adults. Compr. Med. 2017, 1, 194. [Google Scholar] [CrossRef]
- Ye, X.; Li, X.; Zhou, Y.; Ping, X.; Wu, L.; Huang, H. Awareness of Knowledge of Hepatitis B Prevention and Treatment and Vaccination Rate among Residents of Xingguo County. J. Nanchang Univ. Med. Sci. 2017, 50, 1–3. [Google Scholar]
- Mai, W.; Shen, W.; Jian, M. Prevalence and influencing factors of hepatitis B vaccination among adults in Zhaoqing. Chin. J. Public Health Manag. 2018, 34, 97–99. [Google Scholar]
- Ma, T.; Pan, L.; Gao, Z.; Ma, J.; Wu, Z.; Jin, F.; Han, B.; Li, M.; Zhang, J.; Zhao, Y. Influencing factors of coverage rate of hepatitis B vaccine among adults in Hebei Province. Chin. Prev. Med. 2019, 20, 303–307. [Google Scholar]
- Yang, K.; Fang, D.; Qin, Q.; Jiang, L.; Fan, Y. Investigation on the knowledge of hepatitis B vaccination among residents in Ma’anshan City. Mod. Prev. Med. 2019, 46, 3772–3776. [Google Scholar]
- Shi, W.; Zhou, Y.; Yuan, C.; Yan, R.; Tang, X.; He, H.; Deng, X. Seroepidemiological survey of hepatitis B in healthy population in Zhejiang, 2018. Dis. Surveill. 2020, 35, 904–908. [Google Scholar]
- Wan, Y.; Fan, C.; Liu, Y.; Xu, J.; Zhao, T.; Qiu, J.; Wang, F.; Zhang, W.; Kong, Q.; Zhang, G.; et al. Coverage and influencing factors of hepatitis B vaccination among adults in Heilongjiang and Gansu provinces. Chin. J. Vaccines Immun. 2020, 26, 207–212. [Google Scholar]
- Xu, C. Analysis on the situation and influencing factors of hepatitis B vaccination among adults in Yulin City. Clin. Res. Pract. 2020, 5, 27–28. [Google Scholar]
- Xu, Y.; Wu, Q.; Xu, S.; Xu, J.; Huang, Y. Analysis on hepatitis B vaccination and its influencing factors among adults in Zhejiang Province. Chin. J. Health Educ. 2020, 36, 259–261. [Google Scholar]
- Liang, Y.; Bai, X.; Liu, X.; Zhang, Z.; Pang, X.; Nie, L.; Qiu, W.; Zhao, W.; Hu, G. Hepatitis B Vaccination Coverage Rates and Associated Factors: A Community-Based, Cross-Sectional Study Conducted in Beijing, 2019–2020. Vaccines 2021, 9, 1070. [Google Scholar] [CrossRef]
- Liu, J.; Liang, W.; Jing, W.; Liu, M. Countdown to 2030: Eliminating hepatitis B disease, China. B World Health Organ. 2019, 97, 230–238. [Google Scholar] [CrossRef]
- Williams, W.W.; Lu, P.; O’Halloran, A.; Bridges, C.B.; Kim, D.K.; Pilishvili, T.; Hales, C.M.; Markowitz, L.E.; Centers, F.D.C.A. Vaccination Coverage Among Adults, Excluding Influenza Vaccination—United States, 2013. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 95–102. [Google Scholar]
- Steffen, G.; Sperle, I.; Harder, T.; Sarma, N.; Beermann, S.; Thamm, R.; Bremer, V.; Zimmermann, R.; Dudareva, S. Hepatitis B vaccination coverage in Germany: Systematic review. BMC Infect. Dis. 2021, 21, 817. [Google Scholar] [CrossRef]
- Lu, P.; O’Halloran, A.C.; Williams, W.W.; Nelson, N.P. Hepatitis B vaccination coverage among adults aged ≥ 18 years traveling to a country of high or intermediate endemicity, United States, 2015. Vaccine 2018, 36, 2471–2479. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, S.; Wang, Q.; Shen, H.; Zhang, M.; Zhang, Y.; Yan, D.; Liu, M. Seroepidemiology of hepatitis B virus infection in 2 million men aged 21–49 years in rural China: A population-based, cross-sectional study. Lancet Infect. Dis. 2016, 16, 80–86. [Google Scholar] [CrossRef]
- Tan, S.H.S.; Wang, D.; Tan, W.J.; Allameen, N.A.; Fong, N.P. Facilitators and barriers of Hepatitis B screening and vaccination. Vaccine 2020, 38, 5447–5453. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics of China. Available online: http://www.stats.gov.cn/tjsj/ndsj/2021/indexch.htm (accessed on 4 May 2022).
- Lu, P.; Byrd, K.K.; Murphy, T.V.; Weinbaum, C. Hepatitis B vaccination coverage among high-risk adults 18–49 years, U.S.; 2009. Vaccine 2011, 29, 7049–7057. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Qiu, W.; Liang, Y.; Zhang, W.; Qiu, Q.; Bai, X.; Dai, G.; Ma, H.; Hu, H.; Zhao, W.; et al. Effect of a Community-Based Hepatitis B Virus Infection Detection Combined with Vaccination Program in China. Vaccines 2022, 10, 19. [Google Scholar] [CrossRef]
- Amarasinghe, A.; Davison, L.; Diorditsa, S. Engagement of private providers in immunization in the Western Pacific region. Vaccine 2018, 36, 4958–4962. [Google Scholar] [CrossRef]
- Janssen, R.S.; Bruxvoort, K.; Jacobsen, S.J.; Slezak, J.; David, C.; Hyer, R.; Poland, G.A. Considerations for estimating real-world outcomes and value in vaccination: A case study with adult hepatitis B virus vaccination. Vaccine 2021, 39, 5666–5672. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Year of Publication | Location | Sample Size (N) | No. Vaccinated | Coverage Rate (%) | Age, y | Male, No. (%) | Quality Score | Risk of Bias Assessment |
|---|---|---|---|---|---|---|---|---|---|
| Wang SQ et al. | 2011 | Nanjing City | 3744 | 441 | 11.78 | Mean (SD):47.68 (17.36) | 1632 (43.59) | 4 | high |
| Zhang XS et al. | 2011 | Gansu Province | 1020 | 179 | 17.55 | Range: 20–59 | NA 1 | 4 | high |
| Zhang W et al. | 2011 | Lanzhou City | 1307 | 376 | 28.77 | Range: 20–59 | NA | 6 | middle |
| Chen YX | 2012 | Xuzhou City | 2000 | 620 | 31.00 | Range: 21–60 | 1061 (53.05) | 4 | high |
| OuYang L | 2013 | Changsha City | 769 | 292 | 37.97 | Range: 18–50 | NA | 5 | middle |
| Chen XQ | 2015 | Changzhi City | 724 | 285 | 39.36 | Range: 18–55 | 401 (55.39) | 6 | middle |
| Yan H et al. | 2015 | Qiqihar City | 10,761 | 2694 | 25.03 | NA | 5576 (51.82) | 6 | middle |
| Li ze et al. | 2015 | Dali City | 742 | 159 | 21.43 | NA | NA | 1 | high |
| Su YP et al. | 2016 | Beijing | 709 | 51 | 7.19 | Mean (SD):44.3 (13.4) | 311 (43.86) | 5 | middle |
| Gao P et al. | 2016 | Beijing | 4274 | 711 | 16.64 | NA | NA | 5 | middle |
| Liu TT et al. | 2017 | Mianyang City | 260,950 | 88,564 | 33.94 | Mean (SD):52.96 (15.34) | 113,184 (43.37) | 6 | middle |
| Liang ZS | 2017 | Yancheng City | 1280 | 356 | 27.81 | NA | 695 (54.30) | 4 | high |
| Ye X et al. | 2017 | Ganzhou City | 12,967 | 4272 | 32.95 | Mean (SD):54.64 (14.15) | 7560 (58.30) | 6 | middle |
| Mai W et al. | 2018 | Zhaoqing City | 539 | 103 | 19.11 | Range: 24–59 | 206 (38.22) | 5 | middle |
| Ma TL et al. | 2019 | Hebei Province | 2653 | 390 | 14.70 | Mean (SD):40.9 (11.6) | 1221 (46.02) | 5 | middle |
| Yang K et al. | 2019 | Ma’anshan City | 1880 | 484 | 25.74 | Mean: 42 | 713 (37.93) | 6 | middle |
| Shi W et al. | 2020 | Zhejiang Province | 1341 | 254 | 18.94 | Range: 30–59 | NA | 5 | middle |
| Wan YM et al. | 2020 | Heilongjiang and Gansu Province | 1051 | 582 | 55.38 | Mean (SD):36.93 (10.35) | 429 (40.82) | 6 | middle |
| Xu C | 2020 | Yulin City | 625 | 87 | 13.92 | Range: 18–65 | 268 (42.88) | 6 | middle |
| Xu Y et al. | 2020 | Zhejiang Province | 1500 | 638 | 42.53 | Mean (SD):36.78 (12.3) | 715 (47.67) | 6 | middle |
| Yan L et al. | 2021 | Beijing | 35,735 | 11,110 | 31.09 | Range: 20–100 | 13,464 (37.68) | 6 | middle |
| Subgroup | Number of Studies | Coverage (%) | 95% CI | I2 (%) | Heterogeneous p-Value | Egger’s Test p-Value |
|---|---|---|---|---|---|---|
| Region | ||||||
| Eastern | 10 | 22.06 | 15.35–28.78 | 99.6 | p < 0.001 | 0.047 |
| Middle | 4 | 33.81 | 28.77–38.85 | 95.7 | p < 0.001 | 0.906 * |
| Western | 6 | 23.50 | 17.37–29.64 | 99.4 | p < 0.001 | 0.026 * |
| Gender | ||||||
| Male | 10 | 23.47 | 15.61–31.33 | 99.2 | p < 0.001 | 0.161 |
| Female | 9 | 26.60 | 18.73–34.47 | 99.3 | p < 0.001 | 0.387 * |
| Age group | ||||||
| <40 | 10 | 36.93 | 28.35–45.50 | 99.1 | p < 0.001 | 0.005 |
| ≥40 | 10 | 17.09 | 10.18–24.00 | 99.7 | p < 0.001 | 0.062 |
| Urban/Rural | ||||||
| Urban | 6 | 40.29 | 20.91–59.67 | 99.3 | p < 0.001 | 0.114 * |
| Rural | 6 | 16.54 | 7.80–25.29 | 98.8 | p < 0.001 | 0.034 * |
| Investigation period | ||||||
| 2011–2015 | 8 | 26.53 | 20.25–32.81 | 99.0 | p < 0.001 | 0.906 * |
| 2016–2021 | 13 | 26.12 | 22.04–30.20 | 99.6 | p < 0.001 | 0.069 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, X.; Chen, L.; Liu, X.; Tong, Y.; Wang, L.; Zhou, M.; Li, Y.; Hu, G. Adult Hepatitis B Virus Vaccination Coverage in China from 2011 to 2021: A Systematic Review. Vaccines 2022, 10, 900. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060900
Bai X, Chen L, Liu X, Tong Y, Wang L, Zhou M, Li Y, Hu G. Adult Hepatitis B Virus Vaccination Coverage in China from 2011 to 2021: A Systematic Review. Vaccines. 2022; 10(6):900. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060900
Chicago/Turabian StyleBai, Xinxin, Lu Chen, Xinyao Liu, Yujia Tong, Lu Wang, Minru Zhou, Yanming Li, and Guangyu Hu. 2022. "Adult Hepatitis B Virus Vaccination Coverage in China from 2011 to 2021: A Systematic Review" Vaccines 10, no. 6: 900. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060900