
Public Health Value of a Hypothetical Pneumococcal Conjugate Vaccine (PCV) Introduction: A Case Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Method
2.1. PCVs Pneumococcal Conjugate Vaccines and Innovation
2.2. The Overview of Current Pneumococcal Conjugate Vaccines
2.3. PCV Global Market Analysis
2.4. Introduction of PCV12
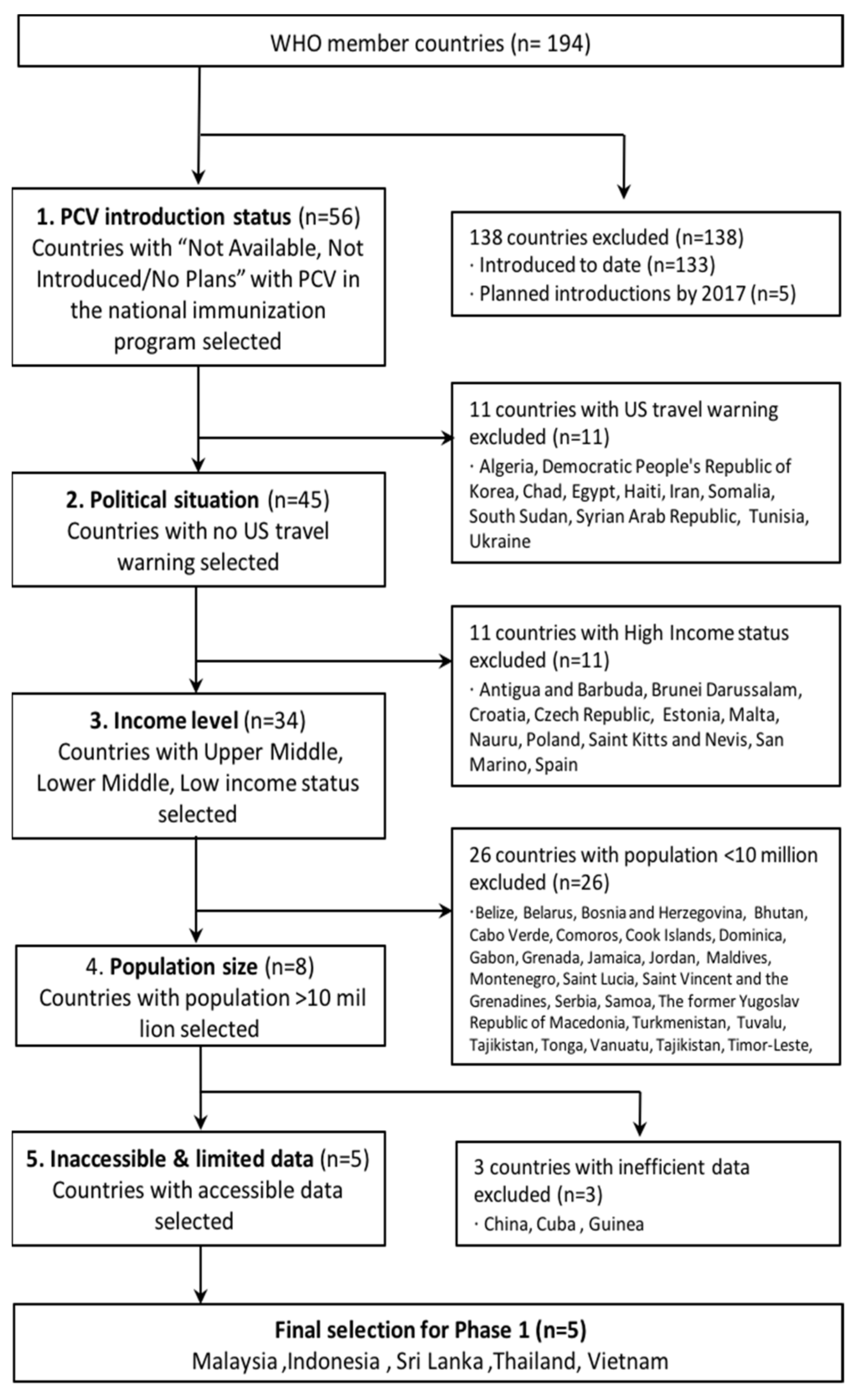
3. Country Selection
3.1. Selection of Country for Case Study
3.2. Stakeholder Meeting
4. Case Study
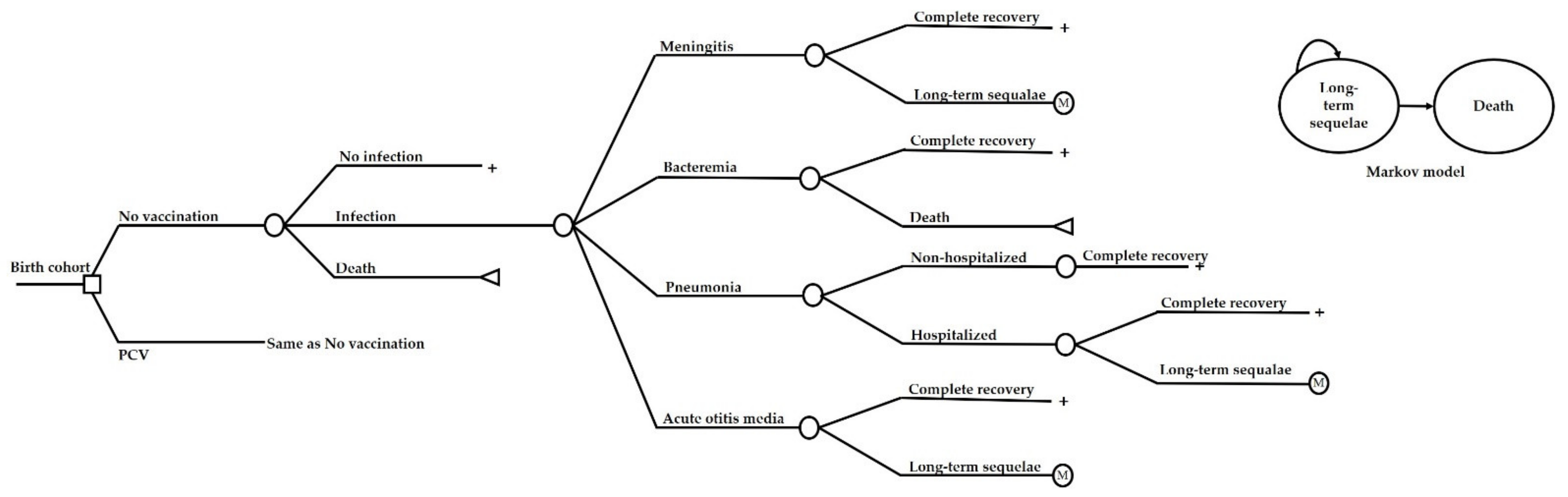
4.1. Economic Analysis
4.2. Vaccination Impact Estimation
4.3. Costs and Outcomes
4.4. Base-Case Analysis
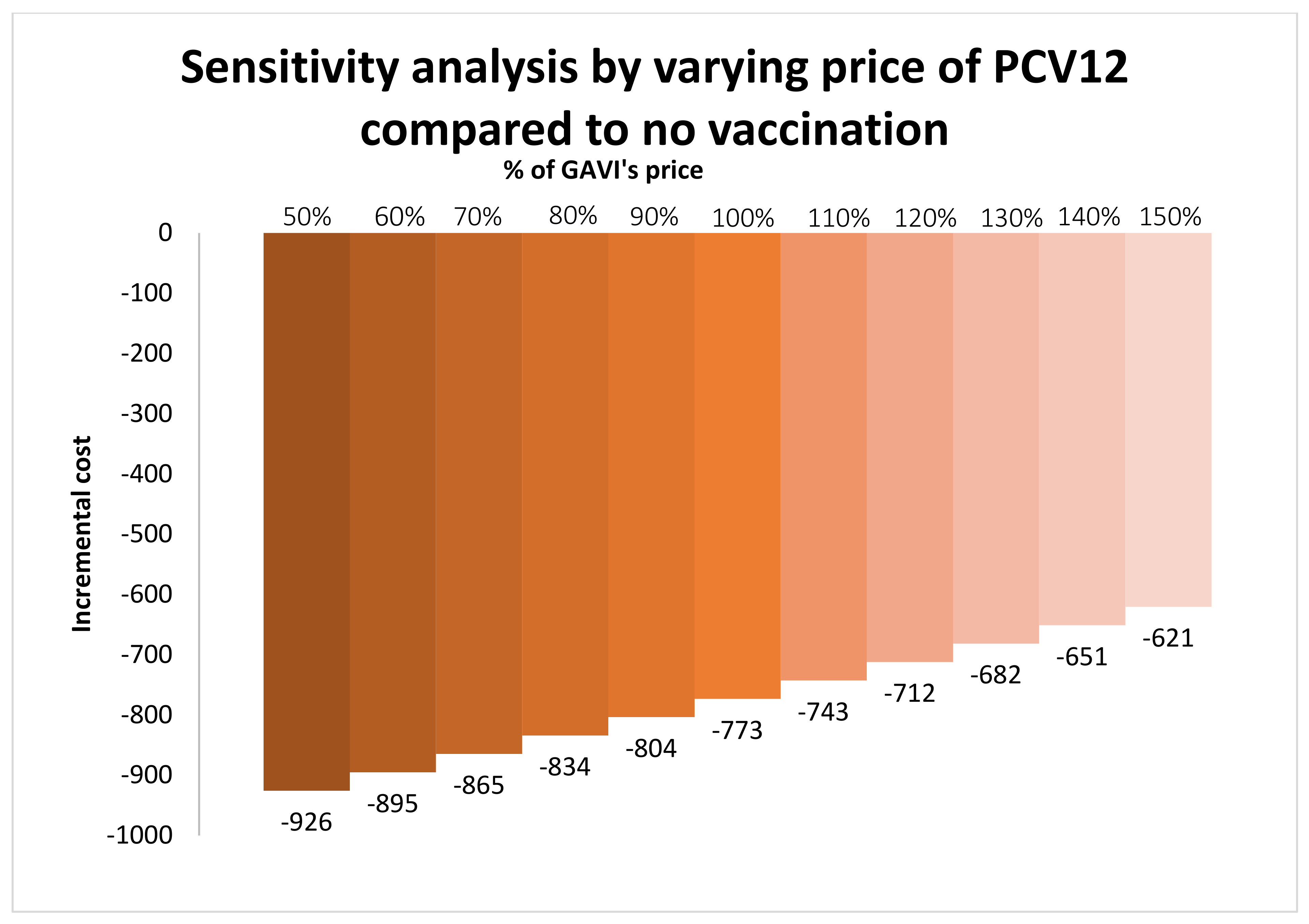
4.5. Sensitivity Analysis
4.6. Budget Impact Analysis
5. Results
5.1. Public Health Value of Vaccine Innovation
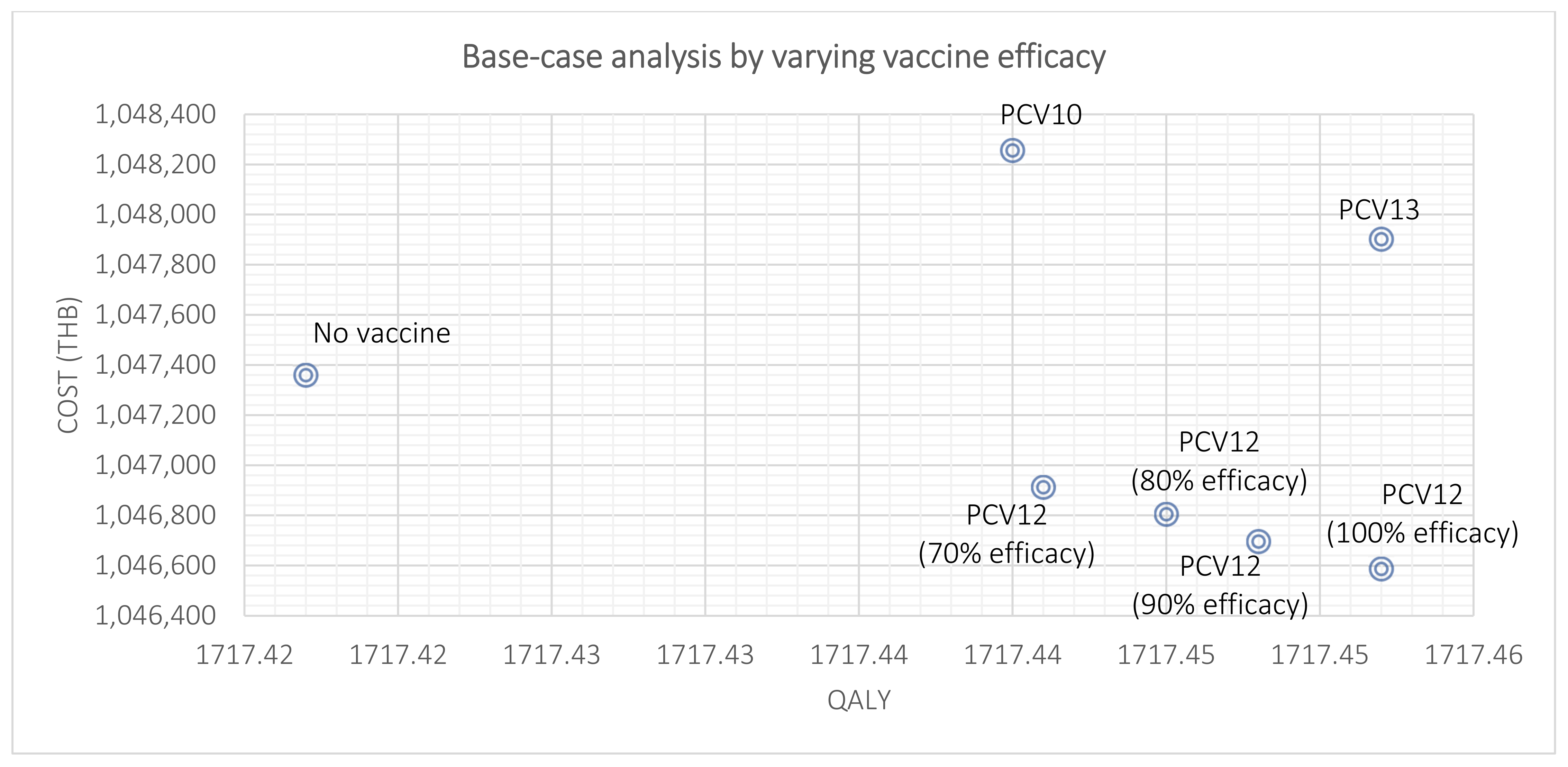
5.1.1. Base-Case Analysis
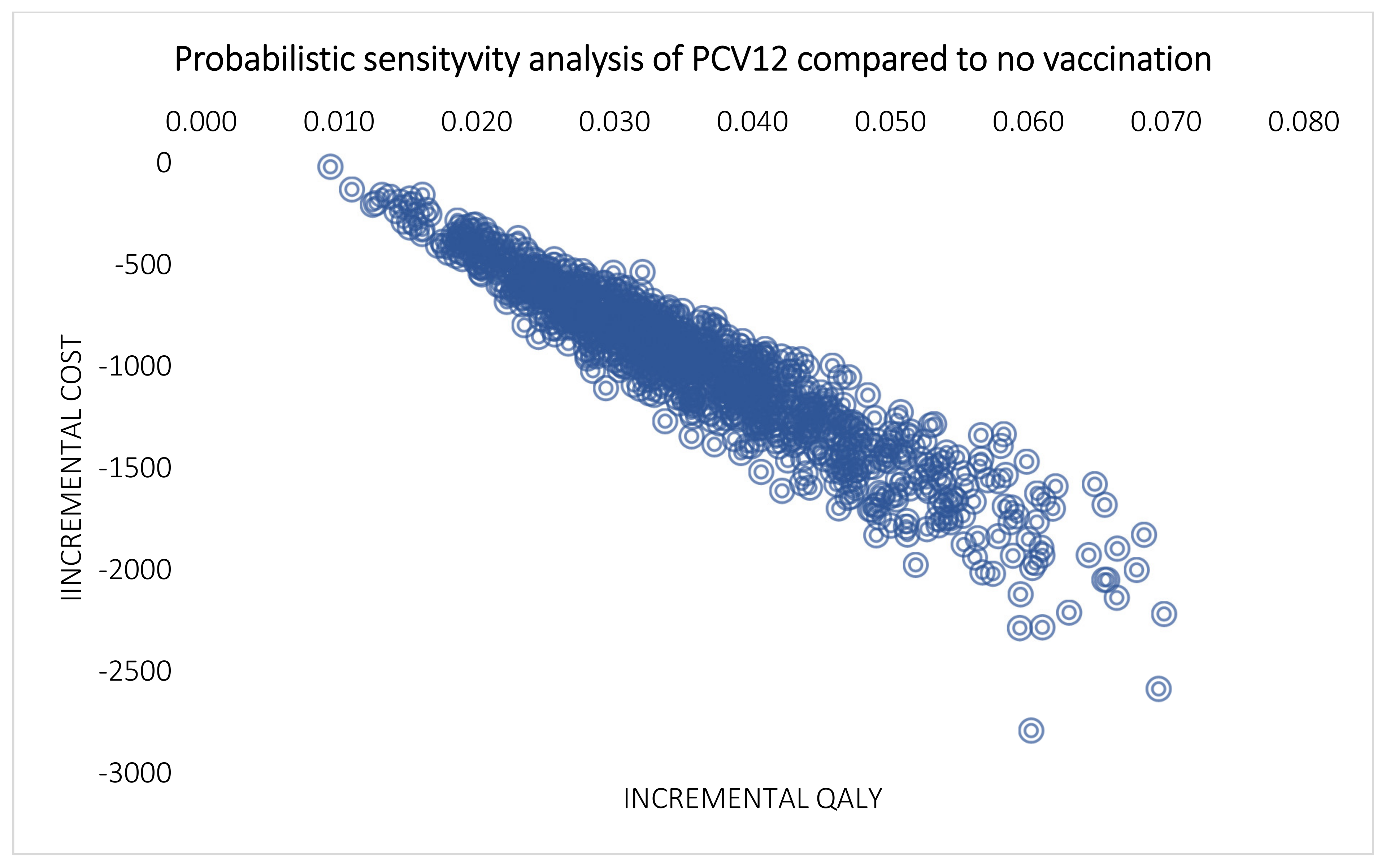
5.1.2. Multivariate Probabilistic Sensitivity Analysis
5.1.3. Scenario Analyses
5.1.4. Budget Impact Analysis
6. Discussion
6.1. Country Case Study–Thailand
6.2. The Public Health Value of Vaccine Innovation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. From the Centers for Disease Control and Prevention. Impact of vaccines universally recommended for children—United States, 1900–1998. JAMA 1999, 281, 1482–1483. [Google Scholar]
- Sepulveda, J. Global health: Towards polio eradication. Nature 2017, 547, 411–412. [Google Scholar] [CrossRef]
- Khan, M.U.; Ahmad, A. Availability and affordability of life-saving vaccines. Lancet Infect. Dis. 2017, 17, 136–137. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, R.T. Product Development Partnerships: Case studies of a new mechanism for health technology innovation. Health Res. Policy Syst. 2011, 9, 33. [Google Scholar] [CrossRef] [Green Version]
- Odevall, L.; Hong, D.; Digilio, L.; Sahastrabuddhe, S.; Mogasale, V.; Baik, Y.; Choi, S.; Kim, J.H.; Lynch, J. The Euvichol story—Development and licensure of a safe, effective and affordable oral cholera vaccine through global public private partnerships. Vaccine 2018, 36, 6606–6614. [Google Scholar] [CrossRef]
- Sim, S.Y.; Jit, M.; Constenla, D.; Peters, D.H.; Hutubessy, R.C.W. A Scoping Review of Investment Cases for Vaccines and Immunization Programs. Value Health 2019, 22, 942–952. [Google Scholar] [CrossRef] [PubMed]
- The investment case for malaria vaccines. PATH Malaria Vaccine Initiative. Available online: https://www.malariavaccine.org/sites/www.malariavaccine.org/files/content/resources/files/PublicFinancialRoIMalVax-GHCMay2006-v1_000.pdf (accessed on 10 June 2022).
- Bloom, D.E.; Brenzel, L.; Cadarette, D.; Sullivan, J. Moving beyond traditional valuation of vaccination: Needs and opportunities. Vaccine 2017, 35 (Suppl. 1), A29–A35. [Google Scholar] [CrossRef]
- Gessner, B.D.; Kaslow, D.; Louis, J.; Neuzil, K.; O’Brien, K.L.; Picot, V.; Pang, T.; Parashar, U.D.; Saadatian-Elahi, M.; Nelson, C.B. Estimating the full public health value of vaccination. Vaccine 2017, 35, 6255–6263. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Full Public Health Value Propositions for Vaccines: Meeting of the Strategic Advisory Group of Experts on Immunization, April 2018: Conclusions and Recommendations; World Health Organization WER: Geneva, Switzerland, 2018; Volume 93, pp. 324–329. Available online: https://www.who.int/publications/i/item/WER9323 (accessed on 30 March 2022).
- Walker, C.L.F.; Rudan, I.; Liu, L.; Nair, H.; Theodoratou, E.; Bhutta, Z.A.; O’Brien, K.; Campbell, H.; Black, R.E. Global burden of childhood pneumonia and diarrhoea. Lancet 2013, 381, 1405–1416. [Google Scholar] [CrossRef]
- Johnson, H.L.; Deloria-Knoll, M.; Levine, O.S.; Stoszek, S.K.; Freimanis Hance, L.; Reithinger, R.; Muenz, L.R.; O’Brien, K.L. Systematic evaluation of serotypes causing invasive pneumococcal disease among children under five: The pneumococcal global serotype project. PLoS Med. 2010, 7, e1000348. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Pneumococcal vaccines WHO position paper—2012—recommendations. Vaccine 2012, 30, 4717–4718. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.; et al. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef]
- Rudan, I.; O’Brien, K.L.; Nair, H.; Liu, L.; Theodoratou, E.; Qazi, S.; Lukšić, I.; Walker, C.L.F.; Black, R.E.; Campbell, H. Epidemiology and etiology of childhood pneumonia in 2010: Estimates of incidence, severe morbidity, mortality, underlying risk factors and causative pathogens for 192 countries. J. Glob. Health 2013, 3, 010401. [Google Scholar] [PubMed]
- World Health Organization. Pneumococcal Conjugate Vaccines in Infants and Children under 5 Years of Age; WHO Position Paper: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Pneumococcal vaccines WHO position paper—2012. Wkly. Epidemiol. Rec. 2012, 87, 129–144. [Google Scholar]
- Chaiyakunapruk, N.; Somkrua, R.; Hutubessy, R.; Henao, A.M.; Hombach, J.; Melegaro, A.; Edmunds, J.W.; Beutels, P. Cost effectiveness of pediatric pneumococcal conjugate vaccines: A comparative assessment of decision-making tools. BMC Med. 2011, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- Gavi the Vaccine Alliance. Base Demand Forecast. “v17”, prepared in 2019 (updated to “v19”, in 2021). Available online: https://www.gavi.org/sites/default/files/2021-12/Gavi-BDF-v19-Public-Summary.pdf (accessed on 10 June 2022).
- AMC Secretariat of Gavi, the Vaccine Alliance. Advance Market Commitment for Pneumococcal Vaccines; Annual Report; Gavi: Geneva, Switzerland, 2018. [Google Scholar]
- Van Zandvoort, K.; Checchi, F.; Diggle, E.; Eggo, R.M.; Gadroen, K.; Mulholland, K.; McGowan, C.R.; Waroux, O.L.P.D.; Rao, V.B.; Satzke, C.; et al. Pneumococcal conjugate vaccine use during humanitarian crises. Vaccine 2019, 37, 6787–6792. [Google Scholar] [CrossRef]
- Unicef. Pneumococcal Conjugate Vaccine: Supply and Demand UpdateJuly 2020. 2020. Available online: https://www.unicef.org/supply/media/4636/file/Pneumococcal-conjugate-vaccine-supply-update-July2020.pdf (accessed on 10 June 2022).
- Permsuwan, U.; Guntawongwan, K.; Buddhawongsa, P. Handling time in economic evaluation studies. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2014, 97 (Suppl. 5), S50–S58. [Google Scholar]
- Chaiyakunapruk, N. Defining the scope of economic evaluation study and selection of comparators. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2008, 91 (Suppl. 2), S16–S20. [Google Scholar]
- Khwannimit, B.; Chayakul, P.; Geater, A. Acute bacterial meningitis in adults: A 20 year review. Southeast Asian J. Trop. Med. Public Health 2004, 35, 886–892. [Google Scholar]
- Muangchana, C.; Chunsuttiwat, S.; Rerks-Ngarm, S.; Kunasol, P. Bacterial meningitis incidence in Thai children estimated by a rapid assessment tool (RAT). Southeast Asian J. Trop. Med. Public Health 2009, 40, 553–562. [Google Scholar]
- World Health Organization. Estimated Hib and Pneumococcal Deaths for Children under 5 Years of Age. 2008. Available online: https://www.who.int/immunization_monitoring/burden/Pneumo_hib_estimates/en/index.html (accessed on 10 February 2016).
- Rhodes, J.; Dejsirilert, S.; Maloney, S.A.; Jorakate, P.; Kaewpan, A.; Salika, P.; Akarachotpong, T.; Prapasiri, P.; Naorat, S.; Areerat, P.; et al. Pneumococcal Bacteremia Requiring Hospitalization in Rural Thailand: An Update on Incidence, Clinical Characteristics, Serotype Distribution, and Antimicrobial Susceptibility, 2005–2010. PLoS ONE 2013, 8, e66038. [Google Scholar] [CrossRef] [PubMed]
- Jordan, H.T.; Prapasiri, P.; Areerat, P.; Anand, S.; Clague, B.; Sutthirattana, S.; Chamany, S.; Flannery, B.; Olsen, S.J. A comparison of population-based pneumonia surveillance and health-seeking behavior in two provinces in rural Thailand. Int. J. Infect. Dis. 2009, 13, 355–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Working Group of Burden of Disease Project. Burden of Disease and Injuries in Thailand 2004; Burden of Disease Thailand Ministry of Public Health: Nonthaburi, Thailand, 2007.
- Kulpeng, W.; Leelahavarong, P.; Rattanavipapong, W.; Sornsrivichai, V.; Baggett, H.C.; Meeyai, A.; Punpanich, W.; Teerawattananon, Y. Cost-utility analysis of 10- and 13-valent pneumococcal conjugate vaccines: Protection at what price in the Thai context? Vaccine 2013, 31, 2839–2847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavia, M.; Bianco, A.; Nobile, C.G.; Marinelli, P.; Angelillo, I.F. Efficacy of pneumococcal vaccination in children younger than 24 months: A meta-analysis. Pediatrics 2009, 123, e1103–e1110. [Google Scholar] [CrossRef] [Green Version]
- Black, S.B.; Shinefield, H.R.; Ling, S.; Hansen, J.; Fireman, B.; Spring, D.; Noyes, J.; Lewis, E.; Ray, P.; Lee, J.; et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than 5 years of age for prevention of pneumonia: Updated analysis using World Health Organization standardized interpretation of chest radiographs. Pediatric Infect. Dis. J. 2006, 25, 779–781. [Google Scholar]
- Palmu, A.A.; Jokinen, J.; Borys, D.; Nieminen, H.; Ruokokoski, E.; Siira, L.; Puumalainen, T.; Lommel, P.; Hezareh, M.; Moreira, M.; et al. Effectiveness of the ten-valent pneumococcal Haemophilus influenzae protein D conjugate vaccine (PHiD-CV10) against invasive pneumococcal disease: A cluster randomised trial. Lancet 2013, 381, 214–222. [Google Scholar] [CrossRef] [Green Version]
- Tregnaghi, M.W.; Saez-Llorens, X.; Lopez, P.; Abate, H.; Smith, E.; Posleman, A.; Calvo, A.; Wong, D.; Cortes-Barbosa, C.; Ceballos, A.; et al. Efficacy of pneumococcal nontypable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) in young Latin American children: A double-blind randomized controlled trial. PLoS Med. 2014, 11, e1001657. [Google Scholar] [CrossRef] [Green Version]
- Baggett, H.C.; Peruski, L.F.; Olsen, S.J.; Thamthitiwat, S.; Rhodes, J.; Dejsirilert, S.; Wongjindanon, W.; Dowell, S.F.; Fischer, J.E.; Areerat, P.; et al. Incidence of pneumococcal bacteremia requiring hospitalization in rural Thailand. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2009, 48 (Suppl. 2), S65–S74. [Google Scholar] [CrossRef]
- Phongsamart, W.; Srifeungfung, S.; Chatsuwan, T.; Nunthapisud, P.; Treerauthaweeraphong, V.; Rungnobhakhun, P.; Sricharoenchai, S.; Chokephaibulkit, K. Changing trends in serotype distribution and antimicrobial susceptibility of Streptococcus pneumoniae causing invasive diseases in Central Thailand, 2009–2012. Hum. Vaccines Immunother. 2014, 10, 1866–1873. [Google Scholar] [CrossRef] [Green Version]
- Shiri, T.; Datta, S.; Madan, J.; Tsertsvadze, A.; Royle, P.; Keeling, M.J.; McCarthy, N.D.; Petrou, S. Indirect effects of childhood pneumococcal conjugate vaccination on invasive pneumococcal disease: A systematic review and meta-analysis. Lancet. Glob. Health 2017, 5, e51–e59. [Google Scholar] [CrossRef] [Green Version]
- Griffin, M.R.; Zhu, Y.; Moore, M.R.; Whitney, C.G.; Grijalva, C.G. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N. Engl. J. Med. 2013, 369, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Orgarnization. V3P Vaccine Product, Price and Procurement Database. 2018. Available online: http://www.who.int/immunization/programmes_systems/procurement/v3p/platform/module1/en/ (accessed on 24 May 2018).
- Chaikledkaew, U.; Teerawattananon, Y.; Kongpittayachai, S.; Suksomboon, N. Thailand’s National Health Technology Assessment Guidelines, 1st ed.; The Graphico Systems: Nonthaburi, Thailand, 2009. [Google Scholar]
- Techathawat, S.; Yoochareon, P.; Varinsathien, P.; Rasjarmrearnsook, A. Wastage of multi-dose measles vaccine survey in public health facilities. Dis. Control. J. 2008, 34, 311–326. [Google Scholar]
- Sangmala, P.; Chaikledkaew, U.; Tanwandee, T.; Pongchareonsuk, P. Economic evaluation and budget impact analysis of the surveillance program for hepatocellular carcinoma in Thai chronic hepatitis B patients. Asian Pac. J. Cancer Prev. 2014, 15, 8993–9004. [Google Scholar] [CrossRef] [Green Version]
- Thavorncharoensap, M.; Teerawattananon, Y.; Natanant, S.; Kulpeng, W.; Yothasamut, J.; Werayingyong, P. Estimating the willingness to pay for a quality-adjusted life year in Thailand: Does the context of health gain matter? Clin. Outcomes Res. 2013, 5, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilokthornsakul, P.; Kengkla, K.; Saokaew, S.; Permsuwan, U.; Techasaensiri, C.; Chotpitayasunondh, T.; Chaiyakunapruk, N. An updated cost-effectiveness analysis of pneumococcal conjugate vaccine among children in Thailand. Vaccine 2019, 37, 4551–4560. [Google Scholar] [CrossRef]
- Briggs, A.; Sculpher, M.; Claxton, K. Decision Modellaing for Health Economic Evaluation; Oxford University Press: Oxford, UK, 2006. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Adjuvant | Conjugation Method | Carrier Protein Content | Serotypes |
|---|---|---|---|---|
| PCV10 (Synflorix) | Alum | Bifunctional spacer | NTHi Protein D: 9–16 μg Tetanus toxoid: 5–10 μg Diphtheria toxoid: 3–6 μg | STs 1, 5, 6B, 7F, 9V, 14, 23F: 1 μg STs 4, 18C, 19F: 3 μg |
| PCV 13 (Prevnar 13) | Alum | Reductive animation | CRM197: 32 μg | ST 6B: 4.4 μg STs 1, 3, 4, 5, 6A, 7F, 9V, 14, 18C, 19A, 19F, 23F: 2.2 μg |
| PCV7 (Prevnar) | Alum | Reductive animation | CRM197: 20 μg | ST 6B: 4 μg STs 4, 9V, 14,18C, 19F, 23F: 2 μg |
| Variable | Target Product Profile (TPP) |
|---|---|
| Type |
|
| Serotypes |
|
| Product Registration Path |
|
| The first NRA approval |
|
| WHO Prequalification Date |
|
| Target Populations |
|
| Target Countries |
|
| Primary Target Delivery Channel |
|
| Efficacy Boundary and Primary Endpoint |
|
| Co-administration |
|
| Presentation |
|
| Formulation |
|
| Doses |
|
| Administration |
|
| Vaccine Volume (cm3/dose) |
|
| Stability |
|
| Parameter Description | Mean | SE | References |
|---|---|---|---|
| Epidemiology parameters | |||
| Annual incidence per 100,000 population for meningitis | 1.36 | 0.195 | Meta-analysis [25,26,27] |
| Annual incidence per 100,000 population for bacteremia | 11.10 | 8.102 | [28] |
| Annual incidence per 100,000 population for all cause pneumonia | 3627 | 570.73 | [29] |
| Annual incidence per 100,000 population for acute otitis media | 601.08 | 3.844 | [30] |
| Proportion of hospitalized pneumonia | 0.6741 | N/A | [29] |
| Epilepsy after pneumococcal meningitis | 0.0821286 | 0.0048154 | NHSO |
| Hearing loss after pneumococcal meningitis | 0.0163027 | 0.002221 | NHSO |
| Neurodevelopmental impairment after pneumococcal meningitis | 0.0018456 | 0.0007528 | NHSO |
| Hearing loss after AOM | 0.0065826 | 0.000957 | NHSO |
| Death after pneumococcal meningitis | 0.032258 | 0.031234 | [31] |
| Death after pneumococcal bacteremia | 0.080000 | 0.036693 | [31] |
| Death after hospitalized pneumonia | 0.014241 | 0.000408 | [31] |
| Vaccine efficacy (PCV7; 3 + 1 schedule) | |||
| IPD caused by vaccine serotype | 89.00% | 5.87% | [32] |
| Clinical pneumonia | 25.50% | 8.72% | [33] |
| AOM | 6.00% | 1.28% | [32] |
| Vaccine efficacy (PCV10; 3 + 1 schedule) | |||
| IPD is caused by vaccine serotype | 100.00% | 0.18% | [34,35] |
| Clinical pneumonia | 21.80% | 6.63% | [35] |
| AOM | 6.00% | 1.28% | [32] |
| Vaccine efficacy (PCV13; 3 + 1 schedule) | |||
| IPD caused by vaccine serotype | 89.00% | 5.87% | [32] |
| Clinical pneumonia | 25.50% | 8.72% | [33] |
| AOM | 6.00% | 1.28% | [32] |
| Vaccine efficacy of PCV10; 2 + 1 schedule against IPD | 92.00% | 10.71% | [34] |
| Vaccine serotype coverage in Thai | |||
| PCV7 serotype coverage in Thai <5 | 74.11% | N/A | Meta-analysis [36,37] |
| PCV7 serotype coverage in Thai 5–64 | 47.82% | N/A | Meta-analysis [36,37] |
| PCV7 serotype coverage in Thai ≥65 | 48.11% | N/A | Meta-analysis [36,37] |
| PCV10 serotype coverage in Thai <5 | 78.72% | N/A | Meta-analysis [36,37] |
| PCV10 serotype coverage in Thai 5–64 | 54.73% | N/A | Meta-analysis [36,37] |
| PCV10 serotype coverage in Thai ≥65 | 55.30% | N/A | Meta-analysis [36,37] |
| PCV13 serotype coverage in Thai <5 | 91.73% | N/A | Meta-analysis [36,37] |
| PCV13 serotype coverage in Thai 5–64 | 76.04% | N/A | Meta-analysis [36,37] |
| PCV13 serotype coverage in Thai ≥65 | 77.60% | N/A | Meta-analysis [36,37] |
| Vaccine serotype coverage US | |||
| PCV7 serotype coverage in aged 10 to 39 | 71.30% | N/A | [37] |
| PCV7 serotype coverage in aged 40 to 64 | 65.40% | N/A | [37] |
| PCV7 serotype coverage in aged ≥65 | 69.70% | N/A | [37] |
| % Reduction in IPD (herd effects) from PCV7 | |||
| % Herd effects in aged 0–4 | 38.00% | 3.83% | [38] |
| % Herd effects in aged 5–18 | 19.00% | 4.85% | [38] |
| % Herd effects in aged 19–49 | 15.00% | 2.80% | [38] |
| % Herd effects in aged 50–64 | 22.00% | 1.79% | [38] |
| % Herd effects in aged ≥65 | 23.00% | 1.28% | [38] |
| % Reduction in pneumonia from PCV7 | |||
| % Herd effects in aged 0–4 | 43.2% | 4.26% | [39] |
| % Herd effects in aged 5–18 | 4.50% | 5.40% | [39] |
| % Herd effects in aged 19–49 | 7.80% | 3.69% | [39] |
| % Herd effects in aged 50–64 | 0.00% | N/A | [39] |
| % Herd effects in aged ≥65 | 6.60% | 3.11% | [39] |
| % Reduction in IPD (herd effects) from PCV13 | |||
| % Herd effects in aged 0–4 | 42.34% | N/A | [38] |
| % Herd effects in aged 5–18 | 36.82% | N/A | [38] |
| % Herd effects in aged 19–49 | 37.10% | N/A | [38] |
| % Herd effects in aged 50–64 | 37.10% | N/A | [38] |
| % Herd effects in aged ≥65 | 40.71% | N/A | [38] |
| Cost parameters | |||
| Vaccine cost | |||
| PCV12 (USD/dose) | 3.05 | - | [40] |
| PCV10 (USD/dose) | 16.0 | - | [40] |
| PCV13 (USD/dose) | 16.2 | - | [40] |
| Direct medical cost | |||
| Cost per episode | |||
| Meningitis aged <=14 | 88,863.7 | 5576.88 | NHSO |
| Meningitis aged 15 to 59 | 83,063.84 | 4728.69 | NHSO |
| Meningitis aged >=60 | 110,488.07 | 6313.6 | NHSO |
| Bacteremia aged <=14 | 53,424.67 | 6526.55 | NHSO |
| Bacteremia aged 15 to 59 | 65,466.53 | 4334.92 | NHSO |
| Bacteremia aged >=60 | 76,565.08 | 3833.83 | NHSO |
| Hospitalized pneumonia aged <=14 | 26,923.18 | 9099 | NHSO |
| Hospitalized pneumonia aged 15 to 59 | 76,660.64 | 23,952 | NHSO |
| Hospitalized pneumonia aged >=60 | 91,201.38 | 31,948 | NHSO |
| Non-hospitalized pneumonia aged <=14 | 333.78 | 54.19 | NHSO |
| Non-hospitalized pneumonia aged 15 to 59 | 771.58 | 169.09 | NHSO |
| Non-hospitalized pneumonia aged >=60 | 640.76 | 84.81 | NHSO |
| AOM aged <=14 | 379.33 | 4.53 | NHSO |
| AOM aged 15 to 59 | 254.7 | 3.69 | NHSO |
| AOM aged >=60 | 500.12 | 11.51 | NHSO |
| Cost per year | |||
| Epilepsy aged <=14 | 5589.81 | 64.15 | NHSO |
| Epilepsy aged 15 to 59 | 7702.81 | 47.18 | NHSO |
| Epilepsy aged >=60 | 14,288.80 | 127.57 | NHSO |
| Hearing loss aged <=14 | 892.19 | 33.82 | NHSO |
| Hearing loss aged 15 to 59 | 957.80 | 14.81 | NHSO |
| Hearing loss aged >=60 | 877.37 | 9.93 | NHSO |
| Neurodevelopmental impairment aged <=14 | 1796.98 | 37.23 | NHSO |
| Neurodevelopmental impairment aged 15 to 59 | 4940.03 | 60.83 | NHSO |
| Neurodevelopmental impairment aged >=60 | 1312.17 | 76.93 | NHSO |
| Chronic lung <=14 | 1519 | 1404 | [31] |
| Chronic lung 15 to 59 | 3576 | 62 | [31] |
| Chronic lung >=60 | 3933 | 31 | [31] |
| Direct non-medical cost | |||
| Direct non-medical cost for meningitis (per episode) | 18,121 | N/A | Calculation |
| Direct non-medical cost for bacteremia (per episode) | 11,687 | N/A | Calculation |
| Direct non-medical cost for pneumonia (per episode) | 5481 | N/A | Calculation |
| Direct non-medical cost for acute otitis media (per episode) | 617 | N/A | Calculation |
| Direct non-medical cost for epilepsy (per year) | 5253 | N/A | Calculation |
| Direct non-medical cost for hearing loss (per year) | 1015 | N/A | Calculation |
| Direct non-medical cost for neurodevelopmental impairment (per year) | 20,535 | N/A | Calculation |
| Direct non-medical cost for chronic lung disease (per year) | 8347 | N/A | Calculation |
| Utility | |||
| Utility for meningitis | 0.9638 | 0.0046 | [31] |
| Utility for bacteremia | 0.9852 | 0.0025 | [31] |
| Utility for pneumonia | 0.9910 | 0.0020 | [31] |
| Utility for acute otitis media | 0.9984 | 0.0001 | [31] |
| Utility for epilepsy | 0.6400 | 0.0738 | [31] |
| Utility for hearing loss | 0.5500 | 0.0554 | [31] |
| Utility for neurodevelopmental impairment-mild mental retardation | 0.6900 | 0.0707 | [31] |
| Utility for neurodevelopmental impairment-severe mental retardation | 0.1000 | 0.1085 | [31] |
| Utility for neurodevelopmental impairment-mental retardation and epilepsy | 0.0001 | 0.0943 | [31] |
| Utility for chronic lung disease | 0.5900 | 0.0575 | [31] |
| Vaccine | Total Cost | LYs | QALYs | Incremental Cost (THB) | Incremental QALY | ICER/QALY |
|---|---|---|---|---|---|---|
| No vaccine | 1,047,360 | 1,718.401 | 1,717.417 | Reference | Reference | Reference |
| PCV10 | 1,048,256 | 1718.418 | 1717.440 | 895 | 0.0228 | 39,322 |
| PCV12 | 1,046,587 | 1718.428 | 1717.452 | −773 | 0.0349 | Cost-saving |
| PCV13 | 1,047,902 | 1718.428 | 1717.452 | 542 | 0.0349 | 15,523 |
| Vaccine | Total Cost | LYs | QALYs | Incremental Cost (THB) | Incremental QALY | ICER/QALY |
|---|---|---|---|---|---|---|
| No vaccine | 1,047,360 | 1718.401 | 1717.417 | Reference | Reference | Reference |
| PCV10 | 1,048,256 | 1718.418 | 1717.440 | 895 | 0.0228 | Dominated by PCV13 |
| PCV13 | 1,047,902 | 1718.428 | 1717.452 | −354 | 0.0121 | Dominated by PCV12 |
| PCV12 | 1,046,587 | 1718.428 | 1717.452 | −1315 | 0.0000 | Cost-saving |
| Scenario | Total Cost | QALYs | Incremental cost (THB) | Incremental QALY | ICER/QALY |
|---|---|---|---|---|---|
| No vaccine | 1,047,360 | 1717.417 | Reference | Reference | Reference |
| Full efficacy | 1,046,587 | 1717.452 | −773 | 0.0349 | Cost-saving |
| 10% reduction | 1,046,696 | 1717.448 | −664 | 0.0314 | Cost-saving |
| 20% reduction | 1,046,805 | 1717.445 | −556 | 0.0279 | Cost-saving |
| 30% reduction | 1,046,913 | 1717.441 | −448 | 0.0244 | Cost-saving |
| Budget Impact Analysis | Year | ||||
|---|---|---|---|---|---|
| 2018 (n = 668,470) | 2019 (n = 653,624) | 2020 (n = 631,355) | 2021 (n = 631,355) | 2022 (n = 631,355) | |
| No consideration of cost offset | 203 M | 199 M | 192 M | 183 M | 171 M |
| With consideration of cost offset * | −884 M | −864 M | −854 M | −796 M | −747 M |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaiyakunapruk, N.; Song, D.; Lynch, J.; Kim, J.H.; Dilokthornsakul, P.; Chotpitayasunondh, T.; Mogasale, V. Public Health Value of a Hypothetical Pneumococcal Conjugate Vaccine (PCV) Introduction: A Case Study. Vaccines 2022, 10, 950. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060950
Chaiyakunapruk N, Song D, Lynch J, Kim JH, Dilokthornsakul P, Chotpitayasunondh T, Mogasale V. Public Health Value of a Hypothetical Pneumococcal Conjugate Vaccine (PCV) Introduction: A Case Study. Vaccines. 2022; 10(6):950. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060950
Chicago/Turabian StyleChaiyakunapruk, Nathorn, Dayoung Song, Julia Lynch, Jerome H. Kim, Piyameth Dilokthornsakul, Tawee Chotpitayasunondh, and Vittal Mogasale. 2022. "Public Health Value of a Hypothetical Pneumococcal Conjugate Vaccine (PCV) Introduction: A Case Study" Vaccines 10, no. 6: 950. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10060950