
Network Analysis of Well-Being Dimensions in Vaccinated and Unvaccinated Samples of University Students from Poland during the Fourth Wave of the COVID-19 Pandemic

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedure
2.2. Measures
2.3. Participants
2.4. Statistical Analysis
3. Results
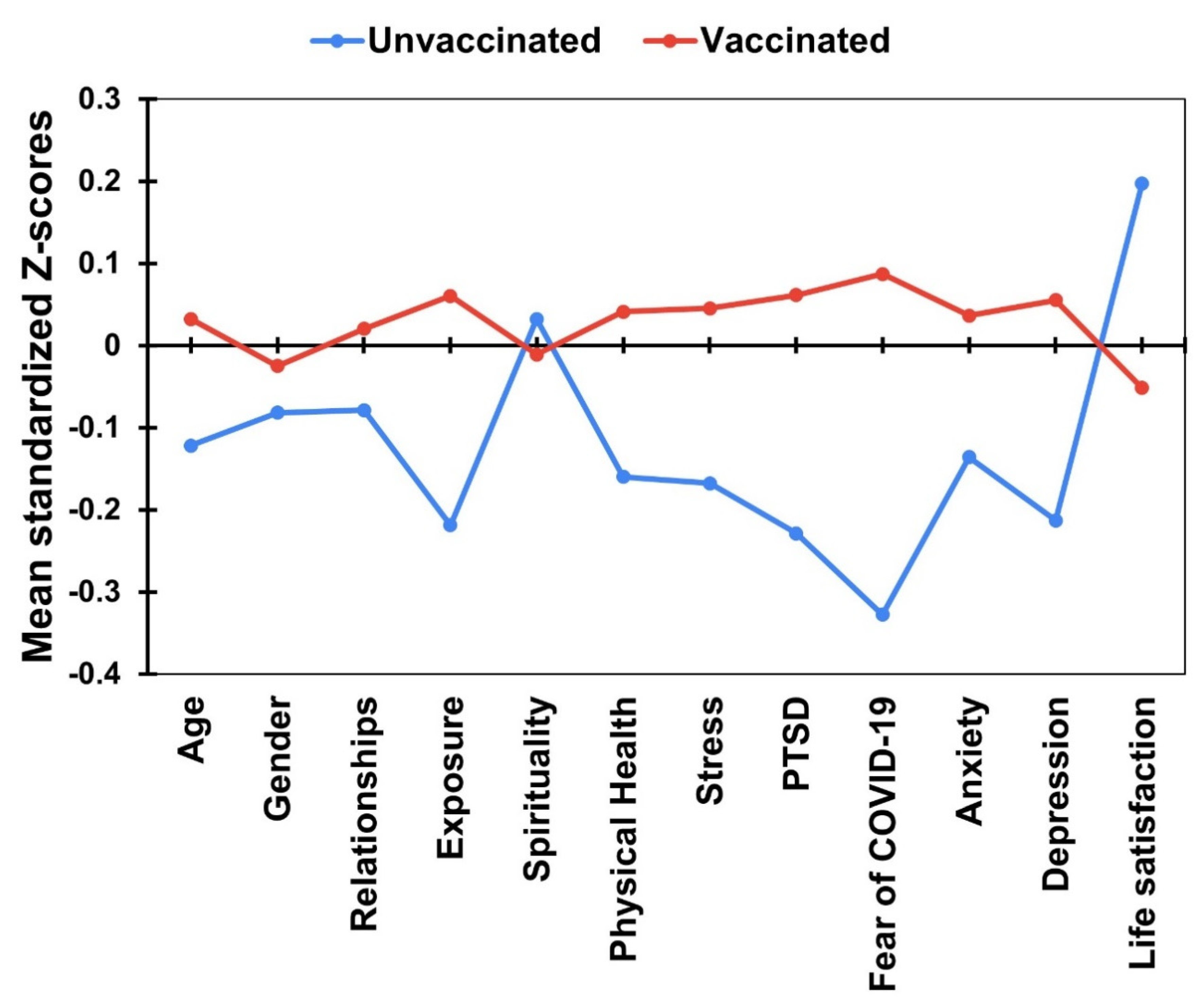
3.1. Differences between the Vaccinated and Unvaccinated Participants in Demographic Variables and Well-Being Dimensions
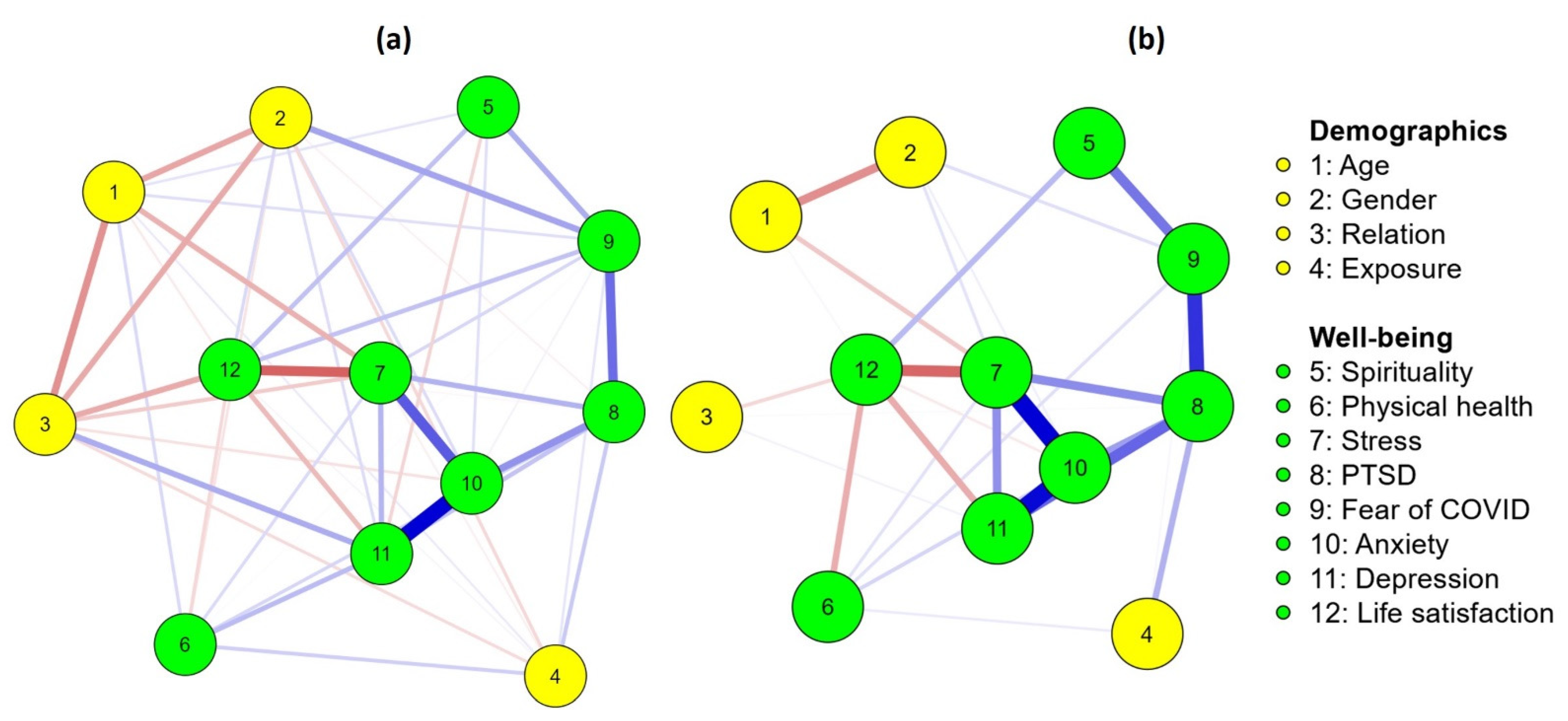
3.2. Association between Demographic Variables and Well-Being Dimensions in Vaccinated and Unvaccinated Samples of University Students
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental Health Issues During and After COVID-19 Vaccine Era. Brain Res. Bull. 2021, 176, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Aknin, L.; De Neve, J.E.; Dunn, E.; Fancourt, D.; Goldberg, E.; Helliwell, J.F.; Jones, S.P.; Karam, E.; Layard, R.; Lyubomirsky, S.; et al. Mental health during the first year of the COVID-19 pandemic: A review and recommendations for moving forward. Perspect. Psychol. Sci. 2022, 17, 915–936. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 2021, 296, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep 2021, 11, 10173. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; Ferracuti, S.; Da Molin, G.; Diella, G.; Montagna, M.T.; Orsi, G.B.; Liguori, G.; Napoli, C. Knowledge and Lifestyle Behaviors Related to COVID-19 Pandemic in People over 65 Years Old from Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 10872. [Google Scholar] [CrossRef]
- Alam, M.D.; Paul, S.K.; Momi, M.; Ni, L.; Xu, Y. Factors associated with psychological outcomes among vaccinated and unvaccinated health care workers against COVID-19 infection in Bangladesh. Front. Med. 2022, 9, 852922. [Google Scholar] [CrossRef]
- Bisht, I.P.; Bisht, R.K.; Sagar, P. Effect of gender and age in fear and stress due to COVID-19. J. Hum. Behav. Soc. Environ. 2021, 31, 70–76. [Google Scholar] [CrossRef]
- Bambra, C.; Albani, V.; Franklin, P. COVID-19 and the gender health paradox. Scand. J. Public. Health. 2021, 49, 17–26. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The prevalence of depressive symptoms, anxiety symptoms and sleep disturbance in higher education students during the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef]
- Fruehwirth, J.C.; Biswas, S.; Perreira, K.M. The COVID-19 pandemic and mental health of first-year college students: Examining the effect of COVID-19 stressors using longitudinal data. PLoS ONE 2021, 16, e0247999. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Benatov, J.; Berger, R.; Korchagina, E.V.; et al. Mental health prevalence and predictors among university students in nine countries during the COVID-19 pandemic: A cross-national study. Sci. Rep. 2021, 11, 18644. [Google Scholar] [CrossRef] [PubMed]
- Rogowska, A.M.; Ochnik, D.; Kuśnierz, C.; Chilicka, K.; Jakubiak, M.; Paradowska, M.; Głazowska, L.; Bojarski, D.; Fijołek, J.; Podolak, M.; et al. Changes in mental health during three waves of the COVID-19 pandemic: A repeated cross-sectional study among Polish university students. BMC Psychiatry 2021, 21, 627. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.S.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Babicki, M.; Malchrzak, W.; Hans-Wytrychowska, A.; Mastalerz-Migas, A. Impact of vaccination on the sense of security, the anxiety of COVID-19 and quality of life among Polish. A nationwide online survey in Poland. Vaccines 2021, 9, 1444. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID Symptom Study app: A prospective, community-based, nested, case-control study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef]
- Fan, Q.; Shi, J.; Yang, Y.; Tang, G.; Jiang, M.; Li, J.; Tang, J.; Li, L.; Wen, X.; Zhang, L.; et al. Clinical characteristics and immune profile alterations in vaccinated individuals with breakthrough Delta SARS-CoV-2 infections. Nat. Commun. 2022, 13, 3979. [Google Scholar] [CrossRef]
- Achrekar, G.C.; Batra, K.; Urankar, Y.; Batra, R.; Iqbal, N.; Choudhury, S.A.; Hooda, D.; Khan, R.; Arora, S.; Singh, A.; et al. Assessing COVID-19 booster hesitancy and its correlates: An early evidence from India. Vaccines 2022, 10, 1048. [Google Scholar] [CrossRef]
- Agrawal, V.; Cantor, J.H.; Sood, N.; Whaley, C.M. The Impact of the COVID-19 Vaccine Distribution on Mental Health Outcomes. National Bureau of Economic Research 2021. Working Paper No. 29593. Available online: http://www.nber.org/papers/w29593 (accessed on 12 July 2022).
- Aron, M.B.; Connolly, E.; Vrkljan, K.; Zaniku, H.R.; Nyirongo, R.; Mailosi, B.; Ruderman, T.; Barnhart, D.A.; on behalf of the Partners in Health Cross-Site COVID-19 Cohort Research Network. Attitudes toward COVID-19 vaccines among patients with complex non-communicable disease and their caregivers in rural Malawi. Vaccines 2022, 10, 792. [Google Scholar] [CrossRef]
- Aw, J.; Seah, S.S.Y.; Seng, B.J.J.; Low, L.L. COVID-19-related vaccine hesitancy among community hospitals’ healthcare workers in Singapore. Vaccines 2022, 10, 537. [Google Scholar] [CrossRef]
- Berni, I.; Menouni, A.; Filali Zegzouti, Y.; Kestemont, M.-P.; Godderis, L.; El Jaafari, S. Factors associated with COVID-19 vaccine acceptance in Morocco: Applying the Health Belief Model. Vaccines 2022, 10, 784. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. Predictors of willingness of the general public to receive a second COVID-19 booster dose or a new COVID-19 vaccine: A cross-sectional study in Greece. Vaccines 2022, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Habib, S.S.; Alamri, M.S.; Alkhedr, M.M.; Alkhorijah, M.A.; Jabaan, R.D.; Alanzi, M.K. Knowledge and attitudes of medical students toward COVID-19 vaccine in Saudi Arabia. Vaccines 2022, 10, 541. [Google Scholar] [CrossRef]
- Koesnoe, S.; Siddiq, T.H.; Pelupessy, D.C.; Yunihastuti, E.; Awanis, G.S.; Widhani, A.; Karjadi, T.H.; Maria, S.; Hasibuan, A.S.; Rengganis, I.; et al. Using integrative behavior model to predict COVID-19 vaccination intention among healthcare workers in Indonesia: A nationwide survey. Vaccines 2022, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, E.; Stengel, A.; Schneider, A.; Goebel-Stengel, M.; Zipfel, S.; Graf, J. How to motivate SARS-CoV-2 convalescents to receive a booster vaccination? Influence on vaccination willingness. Vaccines 2022, 10, 455. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.; Bencherit, D.; Rais, M.A.; Riad, A. COVID-19 vaccine booster hesitancy (VBH) and Its drivers in Algeria: National cross-sectional survey-based study. Vaccines 2022, 10, 621. [Google Scholar] [CrossRef]
- Miyachi, T.; Sugano, Y.; Tanaka, S.; Hirayama, J.; Yamamoto, F.; Nomura, K. COVID-19 vaccine intention and knowledge, literacy, and health beliefs among Japanese university students. Vaccines 2022, 10, 893. [Google Scholar] [CrossRef]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.H.E.M.; Rahman, M.M.; Parsa, A.D.; et al. COVID-19 vaccine acceptance among low- and lower-middle-income countries: A rapid systematic review and meta-analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Haque, M.Z.; Sultana, R.; Alam, M.A.; Browning, M.H.E.M. COVID-19 vaccine acceptance rate and its factors among healthcare students: A systematic review with meta-analysis. Vaccines 2022, 10, 806. [Google Scholar] [CrossRef]
- Tucker, J.S.; D’Amico, E.J.; Pedersen, E.R.; Garvey, R.; Rodriguez, A.; Klein, D.J. COVID-19 vaccination rates and attitudes among young adults with recent experiences of homelessness. J. Adolesc. Health 2022, 70, 504–506. [Google Scholar] [CrossRef]
- Walkowiak, M.P.; Domaradzki, J.; Walkowiak, D. Better late than never: Predictors of delayed COVID-19 vaccine uptake in Poland. Vaccines 2022, 10, 528. [Google Scholar] [CrossRef] [PubMed]
- Wirawan, G.B.S.; Harjana, N.P.A.; Nugrahani, N.W.; Januraga, P.P. Health beliefs and socioeconomic determinants of COVID-19 booster vaccine acceptance: An Indonesian cross-sectional study. Vaccines 2022, 10, 724. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.H.; Zhong, C.C.; Chung, V.C.; Nilsen, P.; Wong, E.L.; Yeoh, E.-k. Barriers and facilitators to receiving the COVID-19 vaccination and development of theoretically-informed implementation strategies for the public: Qualitative study in Hong Kong. Vaccines 2022, 10, 764. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Kobashi, Y.; Kawamura, T.; Shimazu, Y.; Nishikawa, Y.; Omata, F.; Zhao, T.; Yamamoto, C.; Kaneko, Y.; Nakayama, A.; et al. Factors associated with COVID-19 vaccine booster hesitancy: A retrospective cohort study, Fukushima vaccination community survey. Vaccines 2022, 10, 515. [Google Scholar] [CrossRef]
- Montazeri, F.; de Bildt, A.; Dekker, V.; Anderson, G.M. Network analysis of behaviors in the depression and autism realms: Inter-relationships and clinical implications. J. Autism Dev. Disord. 2020, 50, 1580–1595. [Google Scholar] [CrossRef] [PubMed]
- Leme, D.E.; Alves, E.V.; Lemos, V.D.; Fattori, A. Network analysis: A multivariate statistical approach for health science research. Geriatr. Gerontol. Aging 2020, 14, 43–51. [Google Scholar] [CrossRef]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Primers. 2021, 1, 58. [Google Scholar] [CrossRef]
- Reyna, V.F. Risk perception and communication in vaccination decisions: A fuzzy-trace theory approach. Vaccine 2012, 30, 3790–3797. [Google Scholar] [CrossRef]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- Froese, P. Baylor Religion Survey, Wave V (2017)-Instructional Dataset; Baylor Religion Survey: Waco, TX, USA, 2020. [Google Scholar]
- DeSalvo, K.B.; Fisher, W.P.; Tran, K.; Bloser, N.; Merrill, W.; Peabody, J. Assessing measurement properties of two single-item general health measures. Qual. Life Res. 2006, 15, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.J.; Stein, M.B. An abbreviated PTSD checklist for use as a screening instrument in primary care. Behav. Res. Therapy 2005, 43, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.J.; Wilkins, K.; Roy-Byrne, P.P.; Golinelli, D.; Chavira, D.; Sherbourne, C.; Rose, R.D.; Bystritsky, A.; Sullivan, G.; Craske, M.G.; et al. Abbreviated PTSD Checklist (PCL) as a guide to clinical response. Gen. Hosp. Psychiatry 2012, 34, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.; Litz, B.; Herman, D.; Huska, J.; Keane, T. The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. In Proceedings of the Annual Convention of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 25 October 1993. [Google Scholar]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Koltai, J.; Raifman, J.; Bor, J.; McKee, M.; Stuckler, D. COVID-19 vaccination and mental health: A difference-in-difference analysis of the understanding America study. Am. J. Prev. Med. 2022, 62, 679–687. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Vaccination | χ2(1) | p | φ | |
|---|---|---|---|---|---|---|
| Unvaccinated (n = 149) | Vaccinated (n = 557) | |||||
| Gender | 0.01 | 0.925 | –0.004 | |||
| Woman | 539 (76.34%) | 111 (20.59%) | 428 (79.41%) | |||
| Man | 148 (20.96%) | 31 (20.95%) | 117 (79.05%) | |||
| Relationship status | 1.16 | 0.281 | −0.041 | |||
| Single | 254 (35.98%) | 48 (18.90%) | 206 (81.10%) | |||
| In a couple | 452 (64.02%) | 101 (22.35%) | 351 (77.65%) | |||
| Exposure 1 | 6.29 | 0.012 | 0.094 | |||
| No | 386 (54.67%) | 95 (24.61%) | 291 (75.39%) | |||
| Yes | 320 (45.33%) | 54 (16.88%) | 266 (83.12%) | |||
| Exposure 2 | 2.04 | 0.182 | 0.054 | |||
| No | 414 (58.64%) | 95 (22.95%) | 319 (77.05%) | |||
| Yes | 292 (41.36%) | 54 (18.49%) | 238 (81.51%) | |||
| Exposure 3 | 0.02 a | 0.974 | 0.001 | |||
| No | 682 (96.60%) | 144 (21.11%) | 538 (78.89%) | |||
| Yes | 24 (3.40%) | 5 (20.83%) | 19 (79.17%) | |||
| Exposure 4 | 5.43 | 0.020 | 0.088 | |||
| No | 547 (77.48%) | 126 (23.04%) | 421 (76.97%) | |||
| Yes | 159 (22.52%) | 23 (14.47%) | 136 (85.54%) | |||
| Exposure 5 | 7.24 | 0.007 | 0.101 | |||
| No | 177 (25.07%) | 50 (28.25%) | 127 (71.75%) | |||
| Yes | 529 (74.93%) | 99 (18.71%) | 430 (81.29%) | |||
| Exposure 6 | 0.67 | 0.414 | 0.031 | |||
| No | 581 (82.29%) | 126 (21.69%) | 455 (78.31%) | |||
| Yes | 125 (17.71%) | 23 (18.40%) | 102 (81.60%) | |||
| Exposure 7 | 0.41 | 0.525 | 0.024 | |||
| No | 565 (80.03%) | 122 (21.59%) | 443 (78.41%) | |||
| Yes | 141 (19.97%) | 27 (19.15%) | 114 (80.85%) | |||
| Exposure 8 | 0.55 | 0.457 | 0.028 | |||
| No | 341 (48.30%) | 76 (22.29%) | 265 (77.71%) | |||
| Yes | 365 (51.70%) | 73 (20.00%) | 292 (80.00%) | |||
| Variables | Unvaccinated (n = 142) | Vaccinated (n = 545) | t(704) | p | Cohen’s d | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Exposure to COVID-19 | 2.40 | 1.59 | 2.87 | 1.69 | –3.02 | 0.003 | –0.279 |
| Spirituality | 6.78 | 3.34 | 6.64 | 3.19 | 0.46 | 0.643 | 0.043 |
| Physical health | 4.97 | 1.72 | 5.32 | 1.77 | –2.19 | 0.029 | –0.201 |
| Perceived stress | 20.50 | 8.88 | 22.17 | 7.55 | –2.31 | 0.021 | –0.213 |
| Coronavirus-related PTSD | 11.78 | 4.13 | 12.98 | 4.12 | –3.16 | 0.002 | –0.292 |
| Fear of COVID | 11.38 | 4.93 | 13.46 | 4.97 | –4.56 | <0.001 | –0.42 |
| Anxiety | 7.75 | 5.08 | 8.66 | 5.40 | –1.87 | 0.062 | –0.172 |
| Depression | 8.85 | 6.05 | 10.63 | 6.77 | –2.93 | 0.004 | –0.27 |
| Life satisfaction | 22.36 | 6.21 | 20.76 | 6.46 | 2.71 | 0.007 | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogowska, A.M.; Chilicka, K.; Ochnik, D.; Paradowska, M.; Nowicka, D.; Bojarski, D.; Tomasiewicz, M.; Filipowicz, Z.; Grabarczyk, M.; Babińska, Z. Network Analysis of Well-Being Dimensions in Vaccinated and Unvaccinated Samples of University Students from Poland during the Fourth Wave of the COVID-19 Pandemic. Vaccines 2022, 10, 1334. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10081334
Rogowska AM, Chilicka K, Ochnik D, Paradowska M, Nowicka D, Bojarski D, Tomasiewicz M, Filipowicz Z, Grabarczyk M, Babińska Z. Network Analysis of Well-Being Dimensions in Vaccinated and Unvaccinated Samples of University Students from Poland during the Fourth Wave of the COVID-19 Pandemic. Vaccines. 2022; 10(8):1334. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10081334
Chicago/Turabian StyleRogowska, Aleksandra M., Karolina Chilicka, Dominika Ochnik, Maria Paradowska, Dominika Nowicka, Dawid Bojarski, Maciej Tomasiewicz, Zuzanna Filipowicz, Maksymilian Grabarczyk, and Zuzanna Babińska. 2022. "Network Analysis of Well-Being Dimensions in Vaccinated and Unvaccinated Samples of University Students from Poland during the Fourth Wave of the COVID-19 Pandemic" Vaccines 10, no. 8: 1334. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10081334