
Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination
 , , , , , , , , ,
, , , , , , , , ,  , ,
, ,  , and add
Show full author list
, and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fenner, F. Global Eradication of Smallpox. Clin. Infect. Dis. 1982, 4, 916–930. [Google Scholar] [CrossRef]
- Hammarlund, E.; Lewis, M.W.; Carter, S.V.; Amanna, I.; Hansen, S.G.; Strelow, L.I.; Wong, S.W.; Yoshihara, P.; Hanifin, J.M.; Slifka, M.K. Multiple diagnostic techniques identify previously vaccinated individuals with protective immunity against monkeypox. Nat. Med. 2005, 11, 1005–1011. [Google Scholar] [CrossRef]
- Xu, R.; Johnson, A.J.; Liggitt, D.; Bevan, M.J. Cellular and Humoral Immunity against Vaccinia Virus Infection of Mice. J. Immunol. 2004, 172, 6265–6271. [Google Scholar] [CrossRef]
- Xiao, Y.; Isaacs, S.N. Therapeutic Vaccines and Antibodies for Treatment of Orthopoxvirus Infections. Viruses 2010, 2, 2381–2403. [Google Scholar] [CrossRef]
- Noble, J.; Mack, T.M.; Thomas, D.B. A Prospective Study of Serum Antibody and Protection Against Smallpox. Am. J. Trop. Med. Hyg. 1972, 21, 214–218. [Google Scholar]
- Moss, B. Smallpox vaccines: Targets of protective immunity. Immunol. Rev. 2011, 239, 8–26. [Google Scholar] [CrossRef] [PubMed]
- Golden, J.W.; Hooper, J.W. The strategic use of novel smallpox vaccines in the post-eradication world. Expert Rev. Vaccines 2011, 10, 1021–1035. [Google Scholar] [CrossRef]
- Ennis, F.A.; Cruz, J.; Demkowicz, W.E., Jr.; Rothman, A.L.; McClain, D.J. Primary Induction of Human CD8 + Cytotoxic T Lymphocytes and Interferon-γ–Producing T Cells after Smallpox Vaccination. J. Infect. Dis. 2002, 185, 1657–1659. [Google Scholar] [CrossRef]
- Redfield, R.R.; Wright, D.C.; James, W.D.; Jones, T.S.; Brown, C.; Burke, D.S. Disseminated Vaccinia in a Military Recruit with Human Immunodeficiency Virus (HIV) Disease. N. Engl. J. Med. 1987, 316, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Scientific American. I Was Vaccinated against Smallpox 40 Years Ago. Am I Still Protected? 2022. Available online: https://www.scientificamerican.com/article/i-was-vaccinated-against/ (accessed on 20 April 2023).
- Chan, C.E.Z.; Wong, S.K.K.; Yazid, N.B.M.; Ng, O.T.; Marimuthu, K.; Chan, M.; Howe, H.S.; Leo, Y.-S.; Leung, B.P.; Vasoo, S.S.; et al. Residual Humoral Immunity Sustained Over Decades in a Cohort of Vaccinia-Vaccinated Individuals. J. Infect. Dis. 2022, 227, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Combadiere, B.; Boissonnas, A.; Carcelain, G.; Lefranc, E.; Samri, A.; Bricaire, F.; Debre, P.; Autran, B. Distinct Time Effects of Vaccination on Long-Term Proliferative and IFN-γ–producing T Cell Memory to Smallpox in Humans. J. Exp. Med. 2004, 199, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Taub, D.D.; Ershler, W.B.; Janowski, M.; Artz, A.; Key, M.L.; McKelvey, J.; Muller, D.; Moss, B.; Ferrucci, L.; Duffey, P.L.; et al. Immunity from Smallpox Vaccine Persists for Decades: A Longitudinal Study. Am. J. Med. 2008, 121, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Costantino, V.; Trent, M.J.; Sullivan, J.S.; Kunasekaran, M.P.; Gray, R.; MacIntyre, R. Serological Immunity to Smallpox in New South Wales, Australia. Viruses 2020, 12, 554. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Figueiredo, P.; da Silva-Fernandes, A.T.; Mota, B.E.F.; Costa, G.B.; Borges, I.A.; Ferreira, P.C.P.; Abrahão, J.S.; Braga, E.M.; Kroon, E.G.; de Souza Trindade, G. Evaluating anti-Orthopoxvirus antibodies in individuals from Brazilian rural areas prior to the bovine vaccinia era. Mem. Inst. Oswaldo Cruz 2015, 110, 804–808. [Google Scholar] [CrossRef]
- Gushchin, V.A.; Ogarkova, D.A.; Dolzhikova, I.V.; Zubkova, O.V.; Grigoriev, I.V.; Pochtovyi, A.A.; Iliukhina, A.A.; Ozharovskaia, T.A.; Kuznetsova, N.A.; Kustova, D.D.; et al. Estimation of anti-orthopoxvirus immunity in Moscow residents and potential risks of spreading Monkeypox virus. Front. Immunol. 2022, 13, 1023164. [Google Scholar] [CrossRef]
- Hammarlund, E.; Lewis, M.W.; Hansen, S.G.; Strelow, L.I.; Nelson, J.A.; Sexton, G.J.; Hanifin, J.M.; Slifka, M.K. Duration of antiviral immunity after smallpox vaccination. Nat. Med. 2003, 9, 1131–1137. [Google Scholar] [CrossRef]
- Kim, S.-H.; Yeo, S.-G.; Park, K.-H.; Bang, J.-W.; Kim, H.-B.; Kim, N.-J.; Jee, Y.; Cho, H.; Oh, M.-D.; Choe, K.-W. The persistence of humoral and cellular immunities more than three decades after smallpox vaccination. Clin. Microbiol. Infect. 2007, 13, 91–93. [Google Scholar] [CrossRef]
- Poccia, F.; Gioia, C.; Montesano, C.; Martini, F.; Horejsh, D.; Castilletti, C.; Pucillo, L.P.; Capobianchi, M.R.; Ippolito, G. Flow Cytometry and T-Cell Response Monitoring after Smallpox Vaccination. Emerg. Infect. Dis. 2003, 9, 1468–1470. [Google Scholar] [CrossRef]
- Pütz, M.M.; Alberini, I.; Midgley, C.M.; Manini, I.; Montomoli, E.; Smith, G.L. Prevalence of antibodies to Vaccinia virus after smallpox vaccination in Italy. J. Gen. Virol. 2005, 86, 2955–2960. [Google Scholar] [CrossRef]
- Sammartino, J.C.; Cassaniti, I.; Ferrari, A.; Piralla, A.; Bergami, F.; Arena, F.A.; Paolucci, S.; Rovida, F.; Lilleri, D.; Percivalle, E.; et al. Characterization of immune response against monkeypox virus in cohorts of infected patients, historic and newly vaccinated subjects. J. Med. Virol. 2023, 95, e28778. [Google Scholar] [CrossRef]
- Edghill-Smith, Y.; Golding, H.; Manischewitz, J.; King, L.R.; Scott, D.; Bray, M.; Nalca, A.; Hooper, J.W.; Whitehouse, C.A.; Schmitz, J.E.; et al. Smallpox vaccine–induced antibodies are necessary and sufficient for protection against monkeypox virus. Nat. Med. 2005, 11, 740–747. [Google Scholar] [CrossRef]
- McCollum, A.M.; Damon, I.K. Human Monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef]
- Akter, F.; Hasan, T.B.; Alam, F.; Das, A.; Afrin, S.; Maisha, S.; Al Masud, A.; KM, S. Effect of prior immunisation with smallpox vaccine for protection against human Mpox: A systematic review. Rev. Med. Virol. 2023, 33, e2444. [Google Scholar] [CrossRef]
- Fink, D.L.; Callaby, H.; Luintel, A.; Beynon, W.; Bond, H.; Lim, E.Y.; Gkrania-Klotsas, E.; Heskin, J.; Bracchi, M.; Rathish, B.; et al. Clinical features and management of individuals admitted to hospital with monkeypox and associated complications across the UK: A retrospective cohort study. Lancet Infect. Dis. 2022, 23, 589–597. [Google Scholar] [CrossRef]
- Caria, J.; Pinto, R.; Leal, E.; Almeida, V.; Cristóvão, G.; Gonçalves, A.C.; Torres, M.; Santos, M.B.; Pinheiro, H.; Póvoas, D.; et al. Clinical and Epidemiological Features of Hospitalized and Ambulatory Patients with Human Monkeypox Infection: A Retrospective Observational Study in Portugal. Infect. Dis. Rep. 2022, 14, 810–823. [Google Scholar] [CrossRef] [PubMed]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Colavita, F.; Matusali, G.; Mazzotta, V.; Bettini, A.; Lapa, D.; Meschi, S.; Francalancia, M.; Pinnetti, C.; Bordi, L.; Mizzoni, K.; et al. Profiling the acute phase antibody response against mpox virus in patients infected during the 2022 outbreak. J. Med. Virol. 2023, 95, e28851. [Google Scholar] [CrossRef] [PubMed]
- Grifoni, A.; Zhang, Y.; Tarke, A.; Sidney, J.; Rubiro, P.; Reina-Campos, M.; Filaci, G.; Dan, J.M.; Scheuermann, R.H.; Sette, A. Defining antigen targets to dissect vaccinia virus and monkeypox virus-specific T cell responses in humans. Cell Host Microbe 2022, 30, 1662–1670.e4. [Google Scholar] [CrossRef]
- Adamo, S.; Gao, Y.; Sekine, T.; Mily, A.; Wu, J.; Storgärd, E.; Westergren, V.; Filén, F.; Treutiger, C.-J.; Sandberg, J.K.; et al. Memory profiles distinguish cross-reactive and virus-specific T cell immunity to mpox. Cell Host Microbe 2023, 31, 928–936.e4. [Google Scholar] [CrossRef] [PubMed]
- Cohn, H.; Bloom, N.; Cai, G.Y.; Clark, J.J.; Tarke, A.; Bermúdez-González, M.C.; Altman, D.R.; Lugo, L.A.; Lobo, F.P.; Marquez, S.; et al. Mpox vaccine and infection-driven human immune signatures: An immunological analysis of an observational study. Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Rehan, S.T.; Ul Hussain, H.; Nihal, K.; Sukaina, M.; Khan, Z.; Nashwan, A.J. Global Monkeypox Virus Outbreak 2022: A Bibliometric Analysis. Cureus 2023, 15, e37107. [Google Scholar] [CrossRef]
- Criscuolo, E.; Giuliani, B.; Ferrarese, R.; Ferrari, D.; Locatelli, M.; Clementi, M.; Mancini, N.; Clementi, N. Smallpox vaccination-elicited antibodies cross-neutralize 2022-Monkeypox. J. Med. Virol. 2023, 95, e28643. [Google Scholar] [CrossRef]
- Zaeck, L.M.; Lamers, M.M.; Verstrepen, B.E.; Bestebroer, T.M.; van Royen, M.E.; Götz, H.; Shamier, M.C.; van Leeuwen, L.P.M.; Schmitz, K.S.; Alblas, K.; et al. Low levels of monkeypox virus-neutralizing antibodies after MVA-BN vaccination in healthy individuals. Nat. Med. 2022, 29, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Dalton, A.F.; Diallo, A.O.; Chard, A.N.; Moulia, D.L.; Deputy, N.P.; Fothergill, A.; Kracalik, I.; Wegner, C.W.; Markus, T.M.; Pathela, P.; et al. Estimated Effectiveness of JYNNEOS Vaccine in Preventing Mpox: A Multijurisdictional Case-Control Study—United States, August 19, 2022–March 31, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Hazra, A.; Zucker, J.; Bell, E.; Flores, J.; Gordon, L.; Mitjà, O.; Suñer, C.; Lemaignen, A.; Jamard, S.; Nozza, S.; et al. Mpox in people with past infection or a complete vaccination course: A global case series. Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Karem, K.L.; Reynolds, M.; Hughes, C.; Braden, Z.; Nigam, P.; Crotty, S.; Glidewell, J.; Ahmed, R.; Amara, R.; Damon, I.K. Monkeypox-Induced Immunity and Failure of Childhood Smallpox Vaccination to Provide Complete Protection. Clin. Vaccine Immunol. 2007, 14, 1318–1327. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
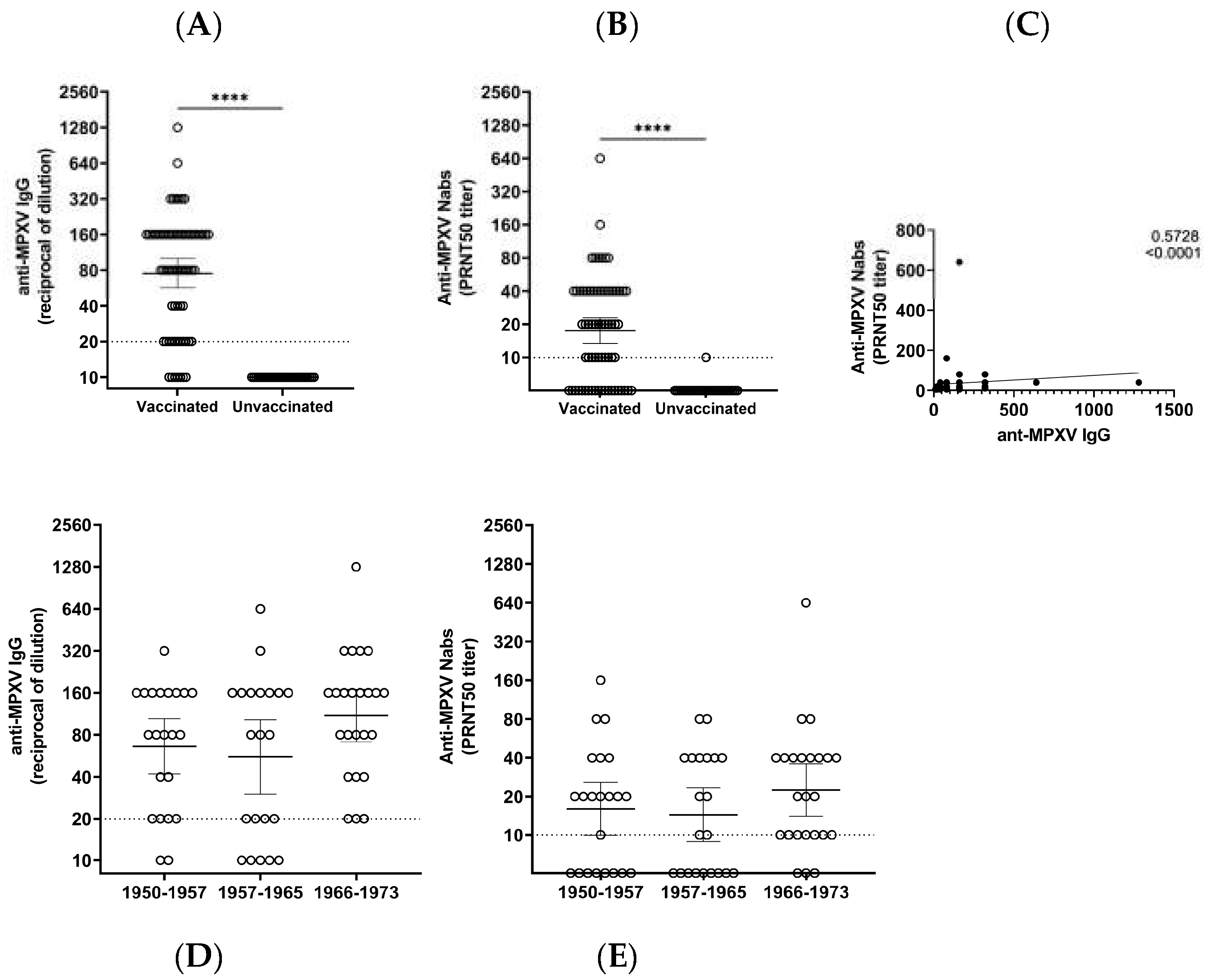
| Born between (Years) | |||
|---|---|---|---|
| 1950–1957 | 1958–1965 | 1966–1973 | |
| N. | 22 | 21 | 24 |
| IgG GMT (95%CI) | 66.2 (41.9–104) | 55.6 (30.2–102.6) | 109.9 (71.4–169.2) |
| IgG % reactive (N) | 90.1 (20) | 76.2 (16) | 100 (24) |
| Nabs GMT (95%CI) | 16.0 (10.0–25.9) | 14.4 (8.9–23.4) | 22.5 (14.0–35.9) |
| NAbs % reactive (N) | 63.6 (14) | 57.1 (12) | 87.5 (21) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matusali, G.; Petruccioli, E.; Cimini, E.; Colavita, F.; Bettini, A.; Tartaglia, E.; Sbarra, S.; Meschi, S.; Lapa, D.; Francalancia, M.; et al. Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination. Vaccines 2023, 11, 1541. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11101541
Matusali G, Petruccioli E, Cimini E, Colavita F, Bettini A, Tartaglia E, Sbarra S, Meschi S, Lapa D, Francalancia M, et al. Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination. Vaccines. 2023; 11(10):1541. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11101541
Chicago/Turabian StyleMatusali, Giulia, Elisa Petruccioli, Eleonora Cimini, Francesca Colavita, Aurora Bettini, Eleonora Tartaglia, Settimia Sbarra, Silvia Meschi, Daniele Lapa, Massimo Francalancia, and et al. 2023. "Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination" Vaccines 11, no. 10: 1541. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11101541