
Impact of Varicella Immunization and Public Health and Social Measures on Varicella Incidence: Insights from Surveillance Data in Shanghai, 2013–2022
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Data Sources
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Varicella Cases
3.2. Coverage Rates of Varicella Vaccination among Children
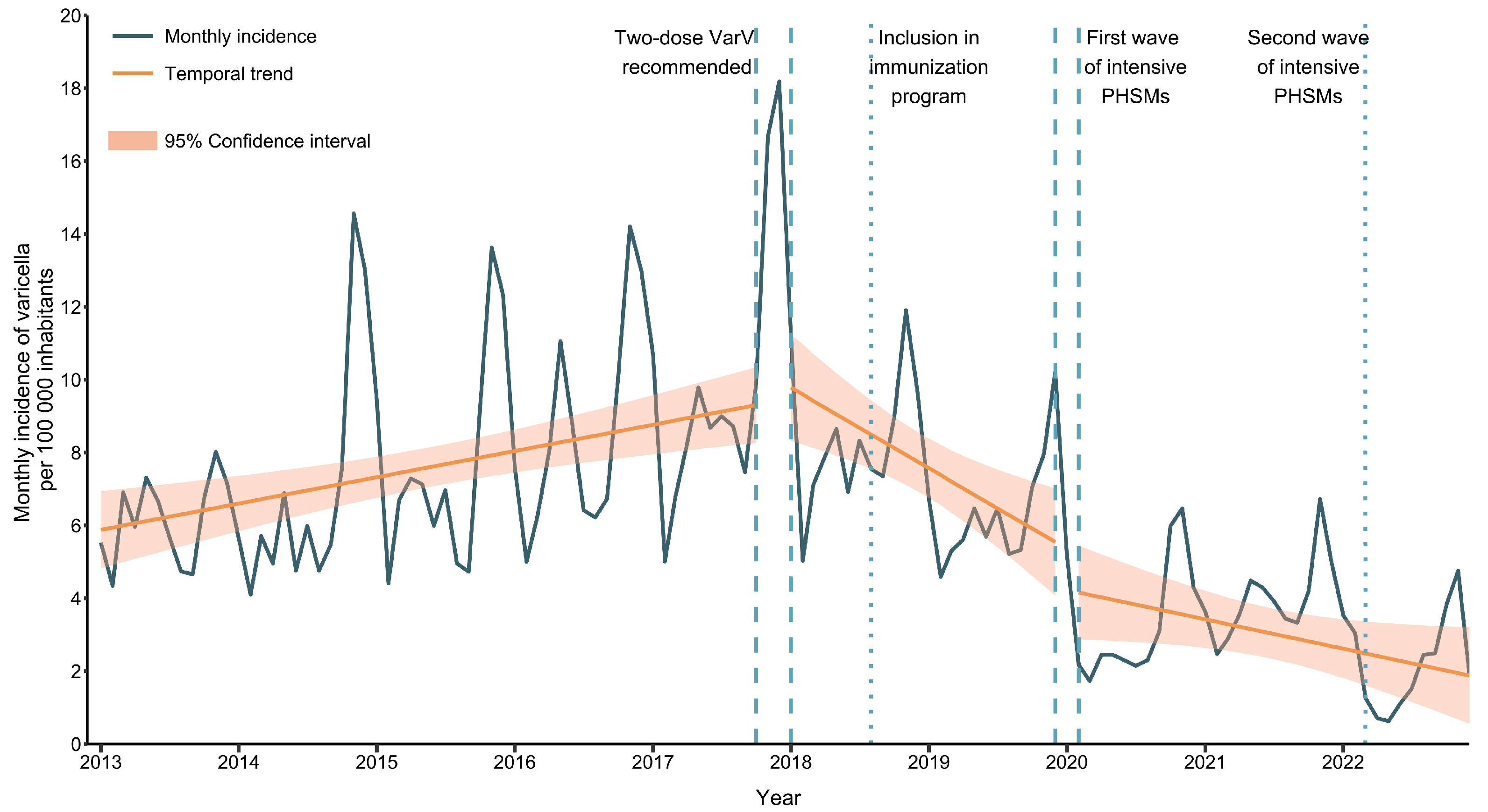
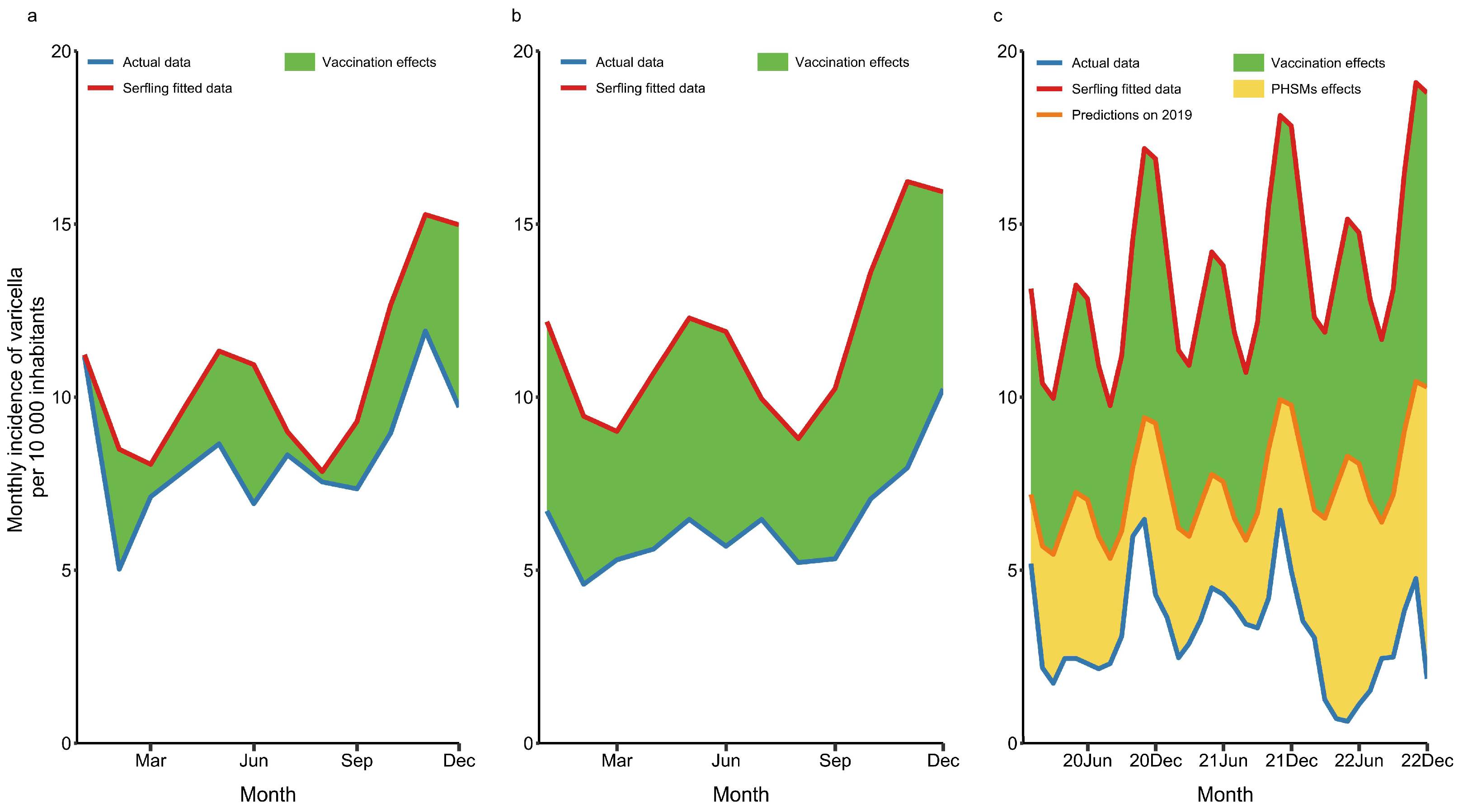
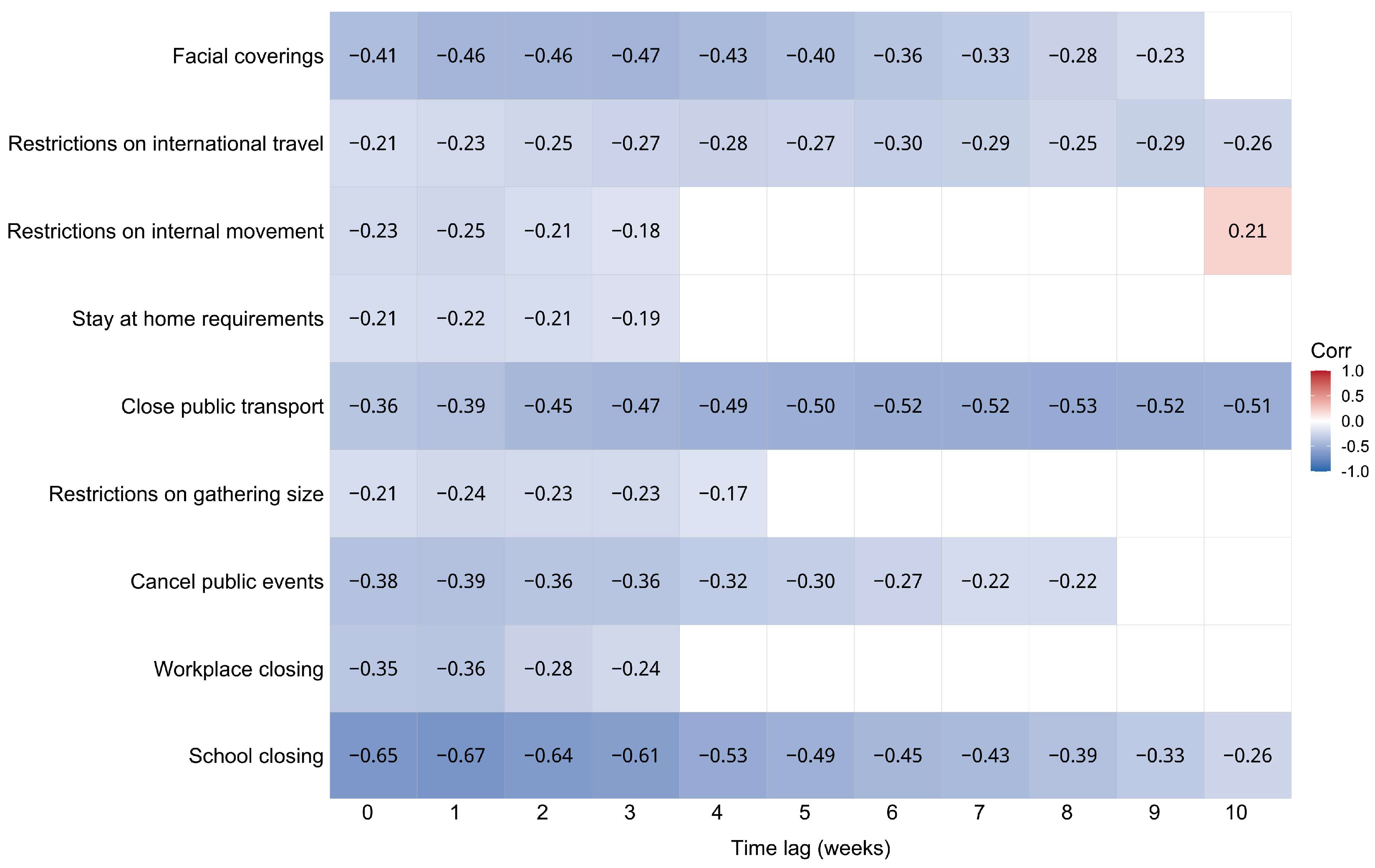
3.3. Association of Two-Dose VarV Program and PHSMs with the Incidence of Varicella
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ross, A.H.; Lenchner, E.; Reitman, G. Modification of Chicken Pox in Family Contacts by Administration of Gamma Globulin. N. Engl. J. Med. 1962, 267, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Seward, J.F.; Zhang, J.X.; Maupin, T.J.; Mascola, L.; Jumaan, A.O. Contagiousness of Varicella in Vaccinated Cases: A Household Contact Study. JAMA 2004, 292, 704. [Google Scholar] [CrossRef] [PubMed]
- Heininger, U.; Seward, J.F. Varicella. Lancet 2006, 368, 1365–1376. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, A.; Zurbruegg, R.P.; Aebi, C. Complications of Varicella in a Defined Central European Population. Arch. Dis. Child. 1998, 79, 472–477. [Google Scholar] [CrossRef]
- Bonhoeffer, J.; Baer, G.; Muehleisen, B.; Aebi, C.; Nadal, D.; Schaad, U.B.; Heininger, U. Prospective Surveillance of Hospitalisations Associated with Varicella-Zoster Virus Infections in Children and Adolescents. Eur. J. Pediatr. 2005, 164, 366–370. [Google Scholar] [CrossRef]
- Galil, K.; Brown, C.; Lin, F.; Seward, J. Hospitalizations for Varicella in the United States, 1988 to 1999. Pediatr Infect. Dis. J. 2002, 21, 931–934. [Google Scholar] [CrossRef]
- Rawson, H.; Crampin, A.; Noah, N. Deaths from Chickenpox in England and Wales 1995-7: Analysis of Routine Mortality Data. BMJ 2001, 323, 1091–1093. [Google Scholar] [CrossRef]
- World Health Organization Varicella and Herpes Zoster Vaccines: WHO Position Paper, June 2014. Wkly Epidemiol. Rec. 2014, 89, 265–287.
- Feng, H.; Zhang, H.; Ma, C.; Zhang, H.; Yin, D.; Fang, H. National and Provincial Burden of Varicella Disease and Cost-Effectiveness of Childhood Varicella Vaccination in China from 2019 to 2049: A Modelling Analysis. Lancet Reg. Health West. Pac. 2023, 32, 100639. [Google Scholar] [CrossRef]
- Zhu, Y.F.; Li, Y.F.; Du, Y.; Zeng, M. Epidemiological Characteristics of Breakthrough Varicella Infection during Varicella Outbreaks in Shanghai, 2008–2014. Epidemiol. Infect. 2017, 145, 2129–2136. [Google Scholar] [CrossRef]
- Seward, J.F.; Watson, B.M.; Peterson, C.L.; Mascola, L.; Pelosi, J.W.; Zhang, J.X.; Maupin, T.J.; Goldman, G.S.; Tabony, L.J.; Brodovicz, K.G.; et al. Varicella Disease After Introduction of Varicella Vaccine in the United States, 1995–2000. JAMA 2002, 287, 606. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.S.; Guris, D.; Zimmerman, L.; Gladden, L.; Moore, T.; Haselow, D.T.; Loparev, V.N.; Schmid, D.S.; Jumaan, A.O.; Snow, S.L. One Dose of Varicella Vaccine Does Not Prevent School Outbreaks: Is It Time for a Second Dose? Pediatrics 2006, 117, e1070–e1077. [Google Scholar] [CrossRef] [PubMed]
- Chaves, S.S.; Gargiullo, P.; Zhang, J.X.; Civen, R.; Guris, D.; Mascola, L.; Seward, J.F. Loss of Vaccine-Induced Immunity to Varicella over Time. N. Engl. J. Med. 2007, 356, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Marin, M.; Marti, M.; Kambhampati, A.; Jeram, S.M.; Seward, J.F. Global Varicella Vaccine Effectiveness: A Meta-Analysis. Pediatrics 2016, 137, e20153741. [Google Scholar] [CrossRef]
- Shapiro, E.D.; Marin, M. The Effectiveness of Varicella Vaccine: 25 Years of Postlicensure Experience in the United States. J. Infect. Dis. 2022, 226, S425–S430. [Google Scholar] [CrossRef]
- Wang, J.; Xu, Z.; Gao, Q. Varicella Outbreaks in Schools and Kindergartens in Shanghai, China from 2011 to 2020. PLoS ONE 2022, 17, e0270630. [Google Scholar] [CrossRef]
- Zha, W.; Pang, F.; Zhou, N.; Wu, B.; Liu, Y.; Du, Y.; Hong, X.; Lv, Y. Research about the Optimal Strategies for Prevention and Control of Varicella Outbreak in a School in a Central City of China: Based on an SEIR Dynamic Model. Epidemiol. Infect. 2020, 148, e56. [Google Scholar] [CrossRef]
- Jackson, C.; Mangtani, P.; Fine, P.; Vynnycky, E. The Effects of School Holidays on Transmission of Varicella Zoster Virus, England and Wales, 1967–2008. PLoS ONE 2014, 9, e99762. [Google Scholar] [CrossRef]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S.; et al. Impact Assessment of Non-Pharmaceutical Interventions against Coronavirus Disease 2019 and Influenza in Hong Kong: An Observational Study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Sullivan, S.G.; Carlson, S.; Cheng, A.C.; Chilver, M.B.; Dwyer, D.E.; Irwin, M.; Kok, J.; Macartney, K.; MacLachlan, J.; Minney-Smith, C.; et al. Where Has All the Influenza Gone? The Impact of COVID-19 on the Circulation of Influenza and Other Respiratory Viruses, Australia, March to September 2020. Eurosurveillance 2020, 25, 2001847. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A Global Panel Database of Pandemic Policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Shanghai Municipal Statistics Bureau Shanghai Statistical Yearbook [Online]. Available online: https://tjj.sh.gov.cn/tjnj/index.html (accessed on 10 May 2023).
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented Regression Analysis of Interrupted Time Series Studies in Medication Use Research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Lopez Bernal, J.; Cummins, S.; Gasparrini, A. Interrupted Time Series Regression for the Evaluation of Public Health Interventions: A Tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Newall, A.T.; Viboud, C.; Wood, J.G. Influenza-Attributable Mortality in Australians Aged More than 50 Years: A Comparison of Different Modelling Approaches. Epidemiol. Infect. 2010, 138, 836–842. [Google Scholar] [CrossRef]
- Procházka, B.; Kynčl, J. Estimating the Baseline and Threshold for the Incidence of Diseases with Seasonal and Long-Term Trends. Cent. Eur. J. Public Health 2015, 23, 352–359. [Google Scholar] [CrossRef]
- Zhou, H.; Burkom, H.; Strine, T.W.; Katz, S.; Jajosky, R.; Anderson, W.; Ajani, U. Comparing the Historical Limits Method with Regression Models for Weekly Monitoring of National Notifiable Diseases Reports. J. Biomed. Inform. 2017, 76, 34–40. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Y.; Zhang, B.; Li, Q. An Evaluation of Voluntary Varicella Vaccination Coverage in Zhejiang Province, East China. Int. J. Environ. Res. Public Health 2016, 13, 560. [Google Scholar] [CrossRef]
- Shu, M.; Zhang, D.; Ma, R.; Yang, T.; Pan, X. Long-Term Vaccine Efficacy of a 2-Dose Varicella Vaccine in China from 2011 to 2021: A Retrospective Observational Study. Front. Public Health 2022, 10, 1039537. [Google Scholar] [CrossRef]
- Zhang, H.; Lai, X.; Mak, J.; Sriudomporn, S.; Zhang, H.; Fang, H.; Patenaude, B. Coverage and Equity of Childhood Vaccines in China. JAMA Netw. Open 2022, 5, e2246005. [Google Scholar] [CrossRef]
- Suo, L.; Lu, L.; Zhao, D.; Pang, X. Impact of a 2-Dose Voluntary Vaccination Strategy on Varicella Epidemiology in Beijing, 2011–2017. Vaccine 2020, 38, 3690–3696. [Google Scholar] [CrossRef]
- Li, Z.; Yao, Y.; Lu, X.; Liu, J.; Huang, Z.; Sun, X.; Lu, Y. Impact of a Two-Dose Varicella Immunization Program on the Incidence of Varicella: A Multi-Year Observational Study in Shanghai, China. Expert Rev. Vaccines 2021, 20, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Riera-Montes, M.; Bollaerts, K.; Heininger, U.; Hens, N.; Gabutti, G.; Gil, A.; Nozad, B.; Mirinaviciute, G.; Flem, E.; Souverain, A.; et al. Estimation of the Burden of Varicella in Europe before the Introduction of Universal Childhood Immunization. BMC Infect. Dis. 2017, 17, 353. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients N (%) | |||
|---|---|---|---|---|
| All Study Periods including Transitions (January 2013–December 2022) 1 | One-Dose VarV Period (January 2013–October 2017) | Early Two-Dose VarV Period (January 2018–December 2019) | Pandemic Period (February 2020–December 2022) | |
| Total number of cases | 19,593 (100) | 11,105 (56.68) | 4513 (23.03) | 2953 (15.07) |
| Sex | ||||
| Female | 8937 (45.61) | 5039 (45.38) | 2096 (46.44) | 1353 (45.82) |
| Male | 10,656 (54.39) | 6076 (54.71) | 2417 (53.56) | 1600 (54.18) |
| Age, years | ||||
| Median (IQR) | 11 (5–24) | 9 (5–22) | 12 (7–26) | 18 (8–29) |
| Age Group | ||||
| 0–4 years | 3594 (18.34) | 2241 (20.18) | 682 (15.11) | 529 (17.91) |
| 5–19 years | 9505 (48.51) | 5695 (51.28) | 2177 (48.24) | 1037 (35.12) |
| 20–29 years | 3782 (19.30) | 2041 (18.38) | 898 (19.90) | 679 (22.99) |
| 30–39 years | 2379 (12.14) | 1025 (9.23) | 675 (14.96) | 573 (19.40) |
| ≥40 years | 333 (1.70) | 103 (0.93) | 81 (1.79) | 135 (4.57) |
| Occupation | ||||
| Scattered children | 2245 (11.46) | 1389 (12.51) | 437 (9.68) | 354 (11.99) |
| Nursery children | 3408 (17.39) | 2290 (20.62) | 611 (13.54) | 285 (9.65) |
| Students | 7748 (39.54) | 4393 (39.56) | 1888 (41.83) | 996 (33.73) |
| Others | 5203 (26.56) | 2538 (22.85) | 1318 (29.20) | 1120 (37.93) |
| Unknown | 989 (5.05) | 495 (4.46) | 259 (5.74) | 198 (6.71) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, L.; Lu, J.; Sun, X.; Li, Z.; Zhang, L.; Lu, Y.; Yao, Y. Impact of Varicella Immunization and Public Health and Social Measures on Varicella Incidence: Insights from Surveillance Data in Shanghai, 2013–2022. Vaccines 2023, 11, 1674. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11111674
Shi L, Lu J, Sun X, Li Z, Zhang L, Lu Y, Yao Y. Impact of Varicella Immunization and Public Health and Social Measures on Varicella Incidence: Insights from Surveillance Data in Shanghai, 2013–2022. Vaccines. 2023; 11(11):1674. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11111674
Chicago/Turabian StyleShi, Liming, Jia Lu, Xiaodong Sun, Zhi Li, Liping Zhang, Yihan Lu, and Ye Yao. 2023. "Impact of Varicella Immunization and Public Health and Social Measures on Varicella Incidence: Insights from Surveillance Data in Shanghai, 2013–2022" Vaccines 11, no. 11: 1674. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11111674