
Identification of an Optimal COVID-19 Booster Allocation Strategy to Minimize Hospital Bed-Days with a Fixed Healthcare Budget
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Constrained Optimization Model
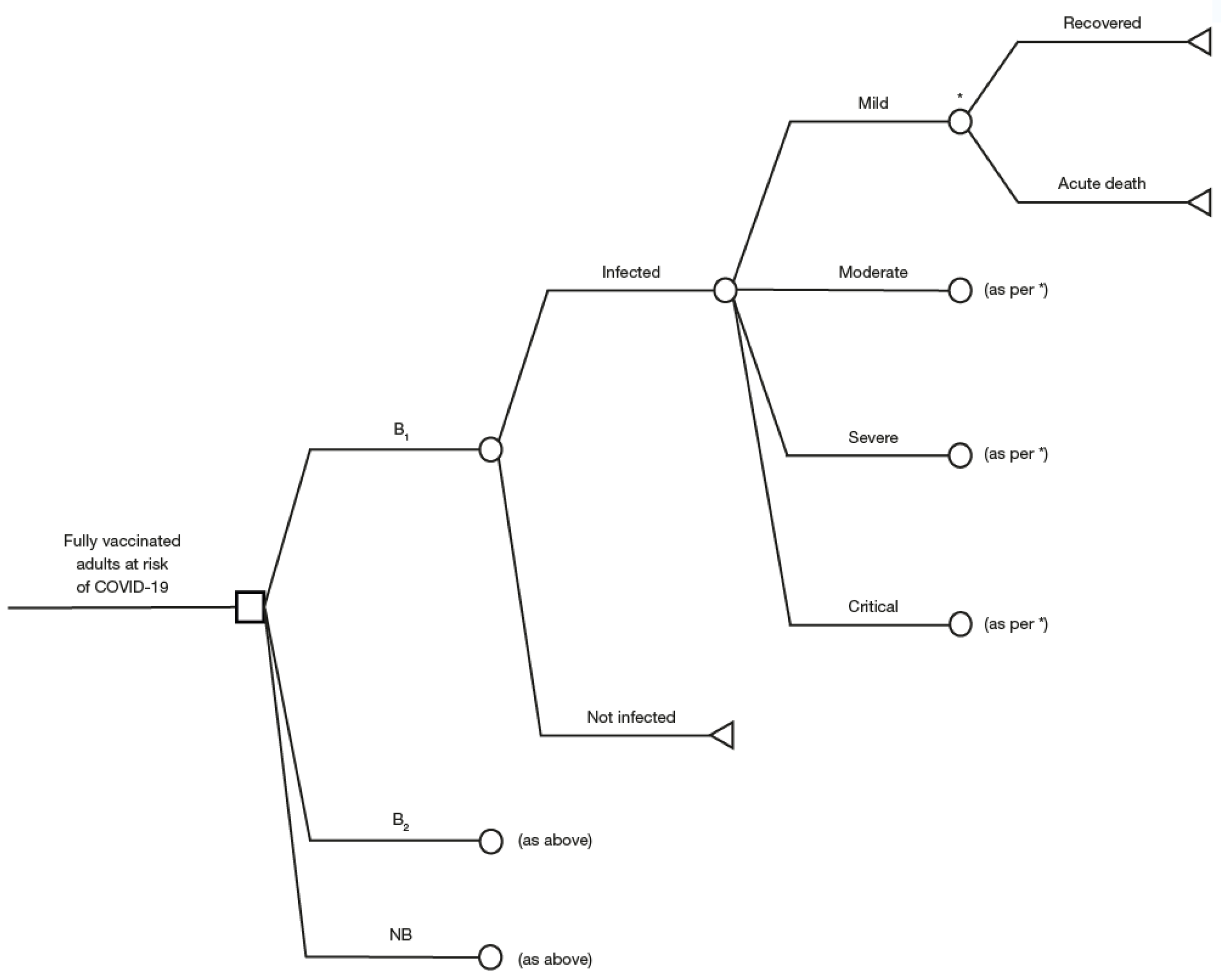
2.2. Decision Tree Model
2.3. Methods for Analysis
3. Results
3.1. Overall Analysis
3.2. Scenario Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Rio, C.; Malani, P.N. COVID-19 in 2022-the beginning of the end or the end of the beginning? JAMA 2022, 327, 2389–2390. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, S.; Zhang, D. Effectiveness of COVID-19 vaccine booster shot compared with non-booster: A meta-analysis. Vaccines 2022, 10, 1396. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 17 June 2022).
- Xylogiannopoulos, K.F.; Karampelas, P.; Alhajj, R. COVID-19 pandemic spread against countries’ non-pharmaceutical interventions responses: A data-mining driven comparative study. BMC Public Health 2021, 21, 1607. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. COVID-19 vaccine effectiveness in New York State. N. Engl. J. Med. 2022, 386, 116–127. [Google Scholar] [CrossRef]
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.G.; Gray, G. Effectiveness of BNT162b2 vaccine against Omicron variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and heterologous COVID-19 booster vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Falsey, A.R.; Frenck, R.W., Jr.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 neutralization with BNT162b2 vaccine dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef]
- Choi, A.; Koch, M.; Wu, K.; Chu, L.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.; Oestreicher, J.; Colpitts, T.; et al. Safety and immunogenicity of SARS-CoV-2 variant mRNA vaccine boosters in healthy adults: An interim analysis. Nat. Med. 2021, 27, 2025–2031. [Google Scholar] [CrossRef] [PubMed]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): A phase 4, non-inferiority, single blind, randomised study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Patalon, T.; Gazit, S.; Pitzer, V.E.; Prunas, O.; Warren, J.L.; Weinberger, D.M. Odds of testing positive for SARS-CoV-2 following receipt of 3 vs 2 doses of the BNT162b2 mRNA vaccine. JAMA Intern Med. 2022, 182, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.G.; Amin, A.B.; Ali, A.R.; Hoots, B.; Cadwell, B.L.; Arora, S.; Avoundjian, T.; Awofeso, A.O.; Barnes, J.; Bayoumi, N.S.; et al. COVID-19 incidence and death rates among unvaccinated and fully vaccinated adults with and without booster doses during periods of Delta and Omicron variant emergence—25 U.S. jurisdictions, April 4–December 25, 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 132–138. [Google Scholar] [CrossRef]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association between 3 doses of mRNA COVID-19 vaccine and symptomatic infection caused by the SARS-CoV-2 Omicron and Delta variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Patel, M.M.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; McNeal, T.; et al. Effectiveness of a third dose of Pfizer-BioNTech and Moderna vaccines in preventing COVID-19 hospitalization among immunocompetent and immunocompromised adults—United States, August–December 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 118–124. [Google Scholar] [CrossRef]
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowley, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a third dose of mRNA vaccines against COVID-19-associated emergency department and urgent care encounters and hospitalizations among adults during periods of Delta and Omicron variant predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 139–145. [Google Scholar] [CrossRef]
- World Health Organization. Interim Statement on the Use of Additional Booster Doses of Emergency Use Listed mRNA Vaccines against COVID-19. Available online: https://www.who.int/news/item/17-05-2022-interim-statement-on-the-use-of-additional-booster-doses-of-emergency-use-listed-mrna-vaccines-against-covid-19 (accessed on 28 October 2022).
- Kraay, A.N.M.; Gallagher, M.E.; Ge, Y.; Han, P.; Baker, J.M.; Koelle, K.; Handel, A.; Lopman, B.A. The role of booster vaccination and ongoing viral evolution in seasonal circulation of SARS-CoV-2. J. R. Soc. Interface 2022, 19, 20220477. [Google Scholar] [CrossRef]
- Richards, F.; Kodjamanova, P.; Chen, X.; Li, N.; Atanasov, P.; Bennetts, L.; Patterson, B.J.; Yektashenas, B.; Mesa-Frias, M.; Tronczynski, K.; et al. Economic burden of COVID-19: A systematic review. Clinicoecon Outcomes Res. 2022, 14, 293–307. [Google Scholar] [CrossRef]
- Wang, Y.; Luangasanatip, N.; Pan-Ngum, W.; Isaranuwatchai, W.; Prawjaeng, J.; Saralamba, S.; Painter, C.; Briones, J.R.; Teerawattananon, Y. Assessing the cost-effectiveness of COVID-19 vaccines in a low incidence and low mortality setting: The case of Thailand at start of the pandemic. Eur. J. Health Econ. 2022, 1–14. [Google Scholar] [CrossRef]
- Crown, W.; Buyukkaramikli, N.; Sir, M.Y.; Thokala, P.; Morton, A.; Marshall, D.A.; Tosh, J.C.; Ijzerman, M.J.; Padula, W.V.; Pasupathy, K.S. Application of constrained optimization methods in health services research: Report 2 of the ISPOR Optimization Methods Emerging Good Practices Task Force. Value Health 2018, 21, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Sauboin, C.; Mihajlovic, J.; Postma, M.J.; Geets, R.; Antic, D.; Standaert, B. Informing decision makers seeking to improve vaccination programs: Case-study Serbia. J. Mark. Access Health Policy 2021, 9, 1938894. [Google Scholar] [CrossRef] [PubMed]
- Standaert, B.; Van Vlaenderen, I.; Van Bellinghen, L.A.; Talbird, S.; Hicks, K.; Carrico, J.; Buck, P.O. Constrained optimization for the selection of influenza vaccines to maximize the population benefit: A demonstration project. Appl. Health Econ. Health Policy 2020, 18, 519–531. [Google Scholar] [CrossRef]
- Mauskopf, J.; Standaert, B.; Connolly, M.P.; Culyer, A.J.; Garrison, L.P.; Hutubessy, R.; Jit, M.; Pitman, R.; Revill, P.; Severens, J.L. Economic analysis of vaccination programs: An ISPOR Good Practices for Outcomes Research Task Force Report. Value Health 2018, 21, 1133–1149. [Google Scholar] [CrossRef]
- Varghese, L.; Ezat Wan Puteh, S.; Schecroun, N.; Jahis, R.; Van Vlaenderen, I.; Standaert, B.A. Applying a constrained optimization portfolio model to aid prioritization of public health interventions in Malaysia. Value Health Reg. Issues 2020, 21, 172–180. [Google Scholar] [CrossRef]
- Demarteau, N.; Breuer, T.; Standaert, B. Selecting a mix of prevention strategies against cervical cancer for maximum efficiency with an optimization program. Pharmacoeconomics 2012, 30, 337–353. [Google Scholar] [CrossRef]
- Demarteau, N.; Morhason-Bello, I.O.; Akinwunmi, B.; Adewole, I.F. Modeling optimal cervical cancer prevention strategies in Nigeria. BMC Cancer 2014, 14, 365. [Google Scholar] [CrossRef]
- Bertsimas, D.; Ivanhoe, J.; Jacquillat, A.; Li, M.; Previero, A.; Lami, O.S.; Bouardi, H.T. Optimizing vaccine allocation to combat the COVID-19 pandemic. medRxiv 2020. [Google Scholar] [CrossRef]
- Buhat, C.A.H.; Lutero, D.S.M.; Olave, Y.H.; Quindala, K.M., 3rd; Recreo, M.G.P.; Talabis, D.; Torres, M.C.; Tubay, J.M.; Rabajante, J.F. Using constrained optimization for the allocation of COVID-19 vaccines in the Philippines. Appl. Health Econ. Health Policy 2021, 19, 699–708. [Google Scholar] [CrossRef]
- Fuady, A.; Nuraini, N.; Sukandar, K.K.; Lestari, B.W. Targeted vaccine allocation could increase the COVID-19 vaccine benefits amidst its lack of availability: A mathematical modeling study in Indonesia. Vaccines 2021, 9, 462. [Google Scholar] [CrossRef]
- Han, S.; Cai, J.; Yang, J.; Zhang, J.; Wu, Q.; Zheng, W.; Shi, H.; Ajelli, M.; Zhou, X.H.; Yu, H. Time-varying optimization of COVID-19 vaccine prioritization in the context of limited vaccination capacity. Nat. Commun. 2021, 12, 4673. [Google Scholar] [CrossRef] [PubMed]
- Matrajt, L.; Eaton, J.; Leung, T.; Brown, E.R. Vaccine optimization for COVID-19: Who to vaccinate first? medRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Matrajt, L.; Eaton, J.; Leung, T.; Dimitrov, D.; Schiffer, J.T.; Swan, D.A.; Janes, H. Optimizing vaccine allocation for COVID-19 vaccines shows the potential role of single-dose vaccination. Nat. Commun. 2021, 12, 3449. [Google Scholar] [CrossRef] [PubMed]
- Shim, E. Optimal allocation of the limited COVID-19 vaccine supply in South Korea. J. Clin. Med. 2021, 10, 591. [Google Scholar] [CrossRef]
- Siqueira, P.G.; Duarte, H.O.; Moura, M.D.C. Risk-based cost-benefit analysis of alternative vaccines against COVID-19 in Brazil: Coronavac vs. Astrazeneca vs. Pfizer. Vaccine 2022, 40, 3851–3860. [Google Scholar] [CrossRef]
- Worldometer. Worldometer Brazil. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/country/brazil/ (accessed on 17 June 2022).
- Szabó De Carvalho, I. Brazil’s handling of COVID-19 is a global emergency. Americas Quarterly, 3 March 2021. Available online: https://www.americasquarterly.org/article/brazils-handling-of-covid-19-is-a-global-emergency/(accessed on 17 June 2022).
- Silva, C.R.D.V.; Bay, O.G.; Martiniano, C.S.; Uchoa, S.A.D.C. Risk communication in the fight against COVID-19 in Brazil: A rhetorical analysis. Physis Rev. De Saúde Coletiva 2021, 31, e310204. [Google Scholar] [CrossRef]
- Stargardter, G. Raging Virus, Few Shots. How Brazil Missed Its Chance to Secure COVID-19 Vaccines. Available online: https://www.reuters.com/article/us-health-coronavirus-brazil-vaccines-in/raging-virus-few-shots-how-brazil-missed-its-chance-to-secure-covid-19-vaccines-idUSKBN29W141 (accessed on 17 June 2022).
- Crown, W.; Buyukkaramikli, N.; Thokala, P.; Morton, A.; Sir, M.Y.; Marshall, D.A.; Tosh, J.; Padula, W.V.; Ijzerman, M.J.; Wong, P.K.; et al. Constrained optimization methods in health services research-an introduction: Report 1 of the ISPOR Optimization Methods Emerging Good Practices Task Force. Value Health 2017, 20, 310–319. [Google Scholar] [CrossRef]
- UK Health Security Agency. COVID-19 Vaccine Surveillance Report. Week 16. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1070356/Vaccine-surveillance-report-week-16.pdf (accessed on 17 June 2022).
- World Health Organization. WHO Guide for Standardization of Economic Evaluations of Immunization Programmes. Available online: https://apps.who.int/iris/bitstream/handle/10665/69981/WHO_IVB_08.14_eng.pdf;jsessionid=F06199A5F716E20AE192D642DB7BC734?sequence=1 (accessed on 17 June 2022).
- WHO Working Group on the Clinical Characterisation and Management of COVID-19 Infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis 2020, 20, e192–e197. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation. COVID-19 Results Briefing. Brazil. Available online: https://www.healthdata.org/sites/default/files/files/135_briefing_Brazil_1.pdf (accessed on 17 June 2022).
- Instituto Brasileiro de Geografia e Estatística. Projeção da população do Brasil e das Unidades da Federação. Available online: https://www.ibge.gov.br/apps/populacao/projecao/ (accessed on 17 June 2022).
- Worldometer. Brazil Population (LIVE). Available online: https://www.worldometers.info/world-population/brazil-population/ (accessed on 17 June 2022).
- Page, K.; Barnett, A.G.; Graves, N. What is a hospital bed day worth? A contingent valuation study of hospital chief executive officers. BMC Health Serv. Res. 2017, 17, 137. [Google Scholar] [CrossRef] [PubMed]
- Sandmann, F.G.; Robotham, J.V.; Deeny, S.R.; Edmunds, W.J.; Jit, M. Estimating the opportunity costs of bed-days. Health Econ. 2018, 27, 592–605. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Z.; Kuan, C.C. Vaccination to reduce severe COVID-19 and mortality in COVID-19 patients: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1770–1776. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Stay Up to Date with COVID-19 Vaccines Including Boosters. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html (accessed on 28 October 2022).
- Ministry of Health Singapore. Extension of Booster Vaccination Programme to Children Aged 5 to 11 Years. Available online: https://www.moh.gov.sg/news-highlights/details/vaccination-our-primary-defence-in-living-with-covid-19#:~:text=The%20EC19V%20has%20therefore%20recommended,begin%20on%2025%20October%202022 (accessed on 28 October 2022).
- Zeiser, F.A.; Donida, B.; da Costa, C.A.; Ramos, G.O.; Scherer, J.N.; Barcellos, N.T.; Alegretti, A.P.; Ikeda, M.L.R.; Muller, A.; Bohn, H.C.; et al. First and second COVID-19 waves in Brazil: A cross-sectional study of patients’ characteristics related to hospitalization and in-hospital mortality. Lancet Reg. Health Am. 2022, 6, 100107. [Google Scholar] [CrossRef] [PubMed]
- Christensen, P.A.; Olsen, R.J.; Long, S.W.; Snehal, R.; Davis, J.J.; Ojeda Saavedra, M.; Reppond, K.; Shyer, M.N.; Cambric, J.; Gadd, R.; et al. Signals of significantly increased vaccine breakthrough, decreased hospitalization rates, and less severe disease in patients with coronavirus disease 2019 caused by the omicron variant of severe acute respiratory syndrome coronavirus 2 in Houston, Texas. Am. J. Pathol. 2022, 192, 642–652. [Google Scholar] [CrossRef]
- Iuliano, A.D.; Brunkard, J.M.; Boehmer, T.K.; Peterson, E.; Adjei, S.; Binder, A.M.; Cobb, S.; Graff, P.; Hidalgo, P.; Panaggio, M.J.; et al. Trends in disease severity and health care utilization during the early omicron variant period compared with previous SARS-CoV-2 high transmission periods—United States, December 2020–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 146–152. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. Comparison of outcomes from COVID infection in pediatric and adult patients before and after the emergence of Omicron. medRxiv 2022. [Google Scholar] [CrossRef]
- Liu, B.; Spokes, P.; He, W.; Kaldor, J. High risk groups for severe COVID-19 in a whole of population cohort in Australia. BMC Infect. Dis. 2021, 21, 685. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Dattani, S.; Roser, M. Brazil: Coronavirus Pandemic Country Profile. Available online: https://ourworldindata.org/coronavirus/country/brazil (accessed on 17 June 2022).
- Ministério da Saúde. Casirivimabe/Imdevimabe Para Pacientes de Alto Risco Infectados Por SARS-CoV-2. Available online: http://conitec.gov.br/images/Relatorios/2021/20210712_Relatorio_635_Regn-Cov2_COVID-19_P1537.pdf (accessed on 17 June 2022).
- American Hospital Association. CDC: Unvaccinated Adults 3–5 Times More Likely to Get Omicron Infection. Available online: https://www.aha.org/news/headline/2022-01-21-cdc-unvaccinated-adults-3-5-times-more-likely-get-omicron-infection (accessed on 9 November 2022).
- Mathieu, E.; Ritchie, A.J.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekiam, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 2 November 2020).
- Clark, A.; Jit, M.; Warren-Gash, C.; Guthrie, B.; Wang, H.H.; Mercer, S.W.; Sanderson, C.; McKee, M.; Troeger, C.; Ong, K.I.; et al. How many are at increased risk of severe COVID-19 disease? Rapid global, regional and national estimates for 2020. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Vlachos, S.; Wong, A.; Metaxa, V.; Canestrini, S.; Lopez Soto, C.; Periselneris, J.; Lee, K.; Patrick, T.; Stovin, C.; Abernethy, K.; et al. Hospital mortality and resource implications of hospitalisation with COVID-19 in London, UK: A prospective cohort study. Crit. Care Res. Pract. 2021, 2021, 8832660. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapoor, R.; Standaert, B.; Pezalla, E.J.; Demarteau, N.; Sutton, K.; Tichy, E.; Bungey, G.; Arnetorp, S.; Bergenheim, K.; Darroch-Thompson, D.; et al. Identification of an Optimal COVID-19 Booster Allocation Strategy to Minimize Hospital Bed-Days with a Fixed Healthcare Budget. Vaccines 2023, 11, 377. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11020377
Kapoor R, Standaert B, Pezalla EJ, Demarteau N, Sutton K, Tichy E, Bungey G, Arnetorp S, Bergenheim K, Darroch-Thompson D, et al. Identification of an Optimal COVID-19 Booster Allocation Strategy to Minimize Hospital Bed-Days with a Fixed Healthcare Budget. Vaccines. 2023; 11(2):377. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11020377
Chicago/Turabian StyleKapoor, Ritika, Baudouin Standaert, Edmund J. Pezalla, Nadia Demarteau, Kelly Sutton, Eszter Tichy, George Bungey, Sofie Arnetorp, Klas Bergenheim, Duncan Darroch-Thompson, and et al. 2023. "Identification of an Optimal COVID-19 Booster Allocation Strategy to Minimize Hospital Bed-Days with a Fixed Healthcare Budget" Vaccines 11, no. 2: 377. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines11020377