Impact of Switch Options on the Economics of Pneumococcal Conjugate Vaccine (PCV) Introduction in Indonesia

 , and
, and
Abstract
:1. Introduction
2. Interchangeability
2.1. Immunogenicity
2.2. Vaccine Safety
2.3. Effectiveness
3. Implementation of PCV Immunization in MICs
4. Advance Market Commitment (AMC)
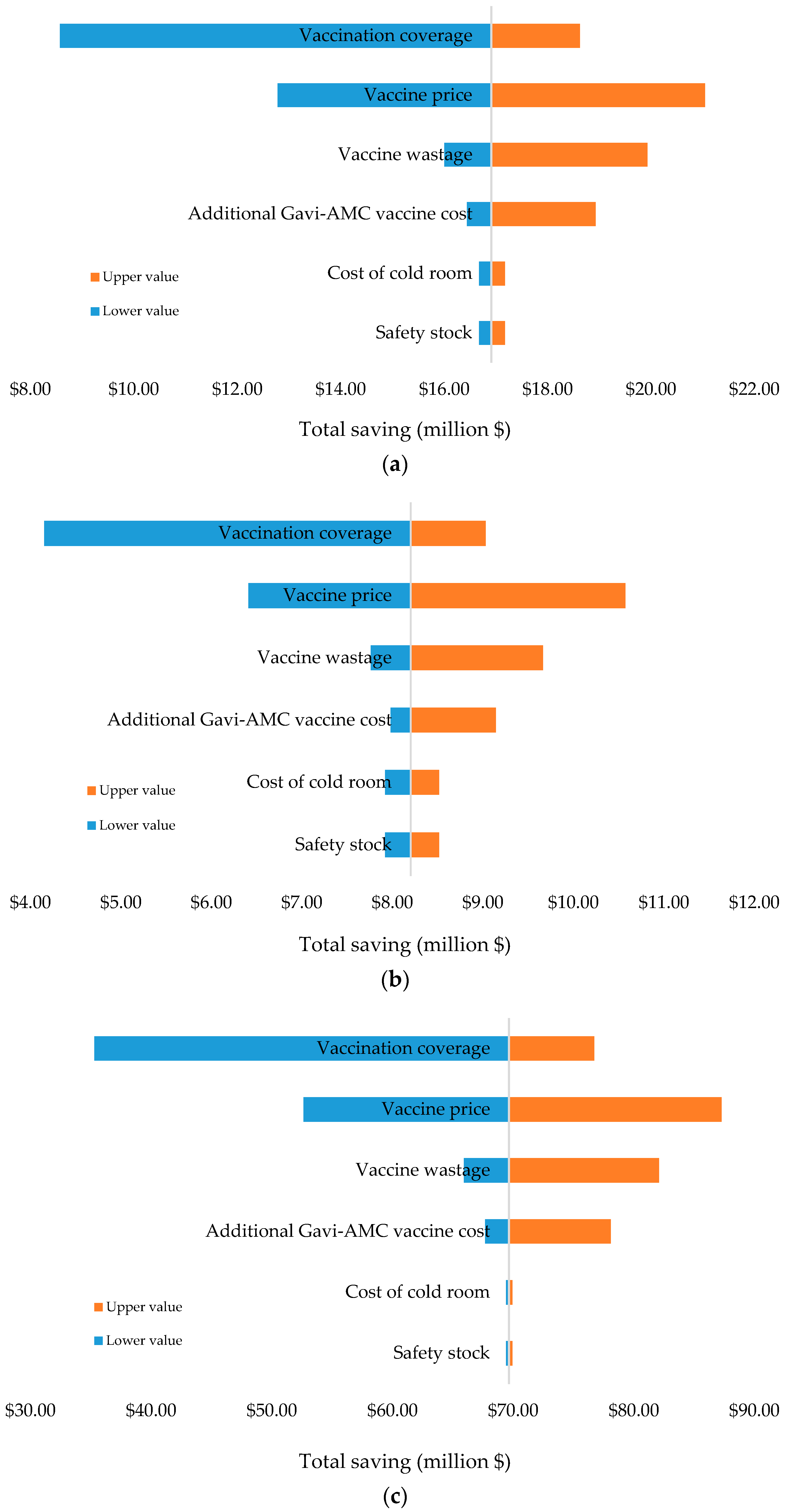
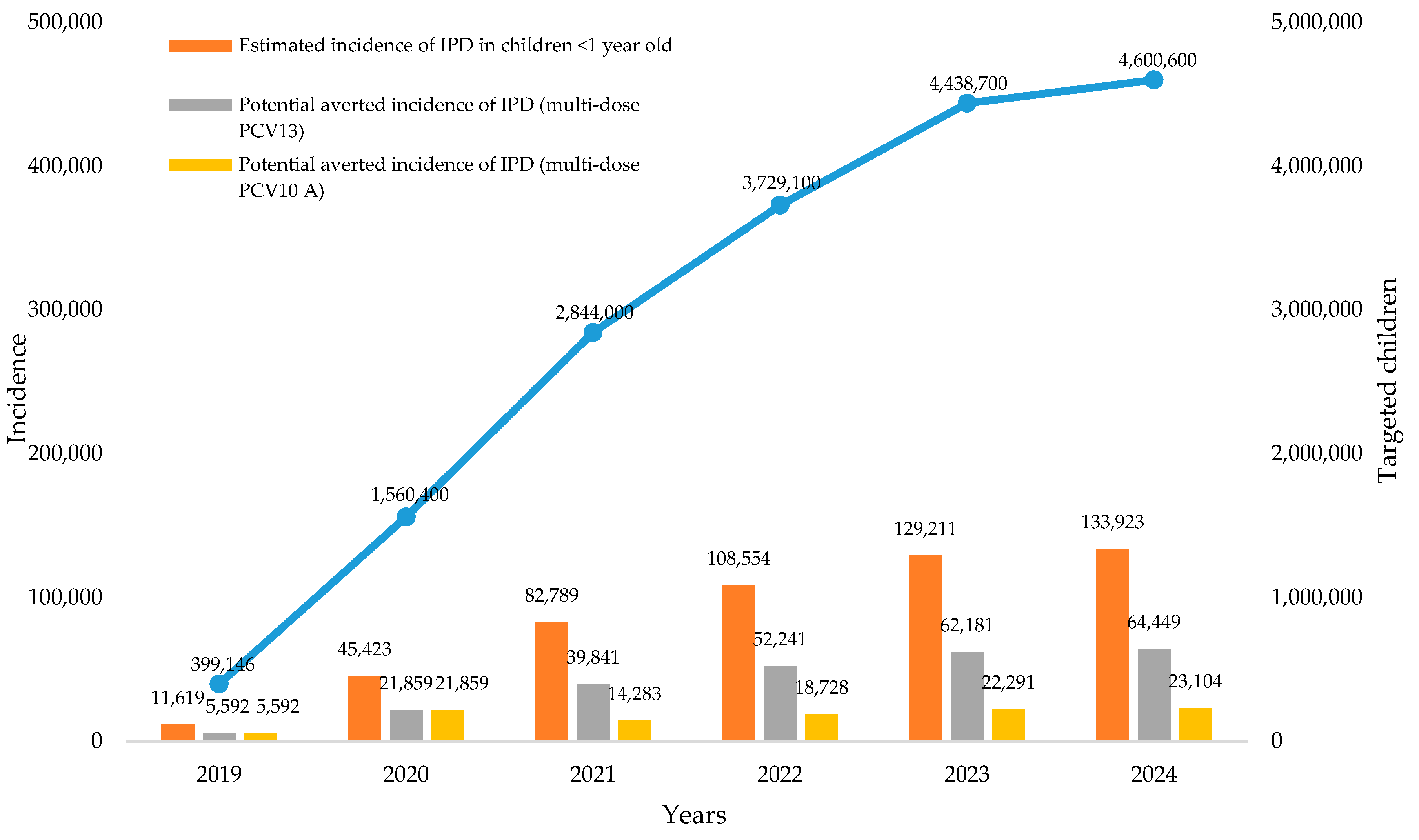
5. Impact of Switch Options on the Economics of PCV Introduction in Indonesia
6. Programmatic Considerations
7. Discussion
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hausdorff, W.P.; Feikin, D.R.; Klugman, K.P. Epidemiological differences among pneumococcal serotypes. Lancet Infect Dis. 2005, 5, 83–93. [Google Scholar] [CrossRef]
- WHO. Pneumococcal conjugate vaccines in infants and children under 5 years of age: WHO position paper—February 2019. Wkly. Epidemiol. Rec. 2019, 94, 85–104. [Google Scholar]
- Maimaiti, N.; Ahmed, Z.; Isa, Z.M.; Ghazi, H.F.; Aljunid, S. Clinical Burden of Invasive Pneumococcal Disease in Selected Developing Countries. Value Health Reg. Issues 2013, 2, 259–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Republic of Indonesia. Indonesia Health Profile 2017; Ministry of Health: Jakarta, Indonesia, 2017.
- UNICEF. One Child Dies of Pneumonia Every 39 Seconds, Agencies Warn. Available online: https://www.unicef.org/indonesia/press-releases/one-child-dies-pneumonia-every-39-seconds-agencies-warn (accessed on 30 March 2020).
- World Health Organization. Treatment and Prevention of Pneumonia. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA63/A63_26-en.pdf (accessed on 30 March 2020).
- SAGE. Current Status of PCV Use and WHO Recommendations. Available online: https://www.who.int/immunization/sage/meetings/2017/october/01_17_October_2017_Presentation_01_OBrien_SAGE_PCV.pdf (accessed on 30 March 2020).
- European Medicines Agency. Synflorix—Summary of Product Characteristics. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000973/WC500054346.pdf (accessed on 30 March 2020).
- European Medicines Agency. Prevenar 13—Summary of Product Characteristics. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001104/WC500057247.pdf (accessed on 30 March 2020).
- Poolman, J.; Frasch, C.; Nurkka, A.; Käyhty, H.; Biemans, R.; Schuerman, L. Impact of the conjugation method on the immunogenicity of Streptococcus pneumoniae serotype 19F polysaccharide in conjugate vaccines. Clin. Vaccine Immunol. 2011, 18, 327–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guevara, J.N.; Borys, D.; DeAntonio, R.; Guzman-Holst, A.; Hoet, B. Interchangeability between pneumococcal conjugate vaccines for pediatric use: A systematic literature review. Expert Rev. Vaccines 2019, 21, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Deceuninck, G.; De Serres, G.; Boulianne, N.; Lefebvre, B.; De Wals, P. Effectiveness of three pneumococcal conjugate vaccines to prevent invasive pneumococcal disease in Quebec, Canada. Vaccine 2015, 33, 2684–2689. [Google Scholar] [CrossRef]
- Diawara, I.; Zerouali, K.; Katfy, K.; Zaki, B.; Belabbes, H.; Najib, J.; Elmdaghri, N. Invasive pneumococcal disease among children younger than 5 years of age before and after introduction of pneumococcal conjugate vaccine in Casablanca, Morocco. Int. J. Infect. Dis. 2015, 40, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Ciapponi, A.; Lee, A.; Bardach, A.; Glujovsky, D.; Rey-Ares, L.; Luisa Cafferata, M.; Valanzasca, P.; Garcia Marti, S. Interchangeability between Pneumococcal Conjugate Vaccines: A Systematic Review and Meta-Analysis. Value Health Reg. Issues 2016, 11, 24–34. [Google Scholar] [CrossRef]
- Su, W.-J.; Lo, H.-Y.; Chang, C.-H.; Chang, L.-Y.; Chiu, C.-H.; Lee, P.-I.; Lu, C.-Y.; Hsieh, Y.-C.; Lai, M.-S.; Lin, T.-Y. Effectiveness of pneumococcal conjugate vaccines of different valences against invasive pneumococcal disease among children in Taiwan: A nationwide study. Pediatr. Infect. Dis. J. 2016, 35, e124–e133. [Google Scholar] [CrossRef]
- Johansson Kostenniemi, U.; Palm, J.; Silfverdal, S.-A. Reductions in otitis and other respiratory tract infections following childhood pneumococcal vaccination. Acta Paediatr. 2018, 107, 1601–1609. [Google Scholar] [CrossRef]
- Gouvernement du Québec. Advice and Prevention—Pneumococcal Conjugate Vaccine. Available online: http://sante.gouv.qc.ca/en/conseils-et-prevention/vaccin-conjugue-contre-le-pneumocoque/ (accessed on 30 March 2020).
- Australian Government, Department of Health. Invasive Pneumococcal Disease in Australia, 2011 and 2012. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/cda-cdi4002k.html (accessed on 30 March 2020).
- Cohen, O.; Knoll, M.; O’Brien, K.; Ramarkrishnan, M.; Constenla, D.; Privor-Dumm, L.; Buss-Younkin, J.; Farrar, J.; Pilishvili, T.; Whitney, C.; et al. Pneumococcal Conjugate Vaccine (PCV) Product Assessment. Available online: https://www.jhsph.edu/ivac/wp-content/uploads/2018/05/pcv-product-assessment-april-25-2017.pdf (accessed on 30 March 2020).
- Hadinegoro, S.R.; Prayitno, A.; Khoeri, M.M.; Djelantik, I.G.; Dewi, N.E.; Indriyani, S.A.; Muttaqin, Z.; Mudaliana, S.; Safari, D. Nasopharyngeal carriage of Streptococcus Pneumoniae in healthy children under five years old in Central Lombok Regency, Indonesia. Southeast Asian J. Trop. Med. Public Health 2016, 47, 485–493. [Google Scholar] [PubMed]
- Dunne, E.M.; Murad, C.; Sudigdoadi, S.; Fadlyana, E.; Tarigan, R.; Indriyani, S.A.K.; Pell, C.L.; Watts, E.; Satzke, C.; Hinds, J.; et al. Carriage of Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, and Staphylococcus aureus in Indonesian children: A cross-sectional study. PLoS ONE 2018, 13, e0195098. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Republic of Indonesia. Comprehensive Multi Year Plan (cMYP) of National Immunization Program 2020–2024; Ministry of Health: Jakarta, Indonesia, 2020.
- Gavi. Indonesia. Available online: https://www.gavi.org/programmes-impact/country-hub/south-east-asia/indonesia (accessed on 22 December 2019).
- Gavi. Gavi-Supported Pneumococcal Conjugate Vaccines Profiles to Support Country Decision Making. Available online: https://www.gavi.org/sites/default/files/document/pcv-profilespdf.pdf (accessed on 22 December 2019).
- Ministry of Health, Republic of Indonesia. Indonesia Health Profile 2018; Ministry of Health: Jakarta, Indonesia, 2018.
- Parmar, D.; Baruwa, E.M.; Zuber, P.; Kone, S. Impact of wastage on single and multi-dose vaccine vials: Implications for introducing pneumococcal vaccines in developing countries. Hum. Vaccines 2010, 6, 270–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Performance, Quality and Safety (PQS) 2007. Available online: www.who.int/immunization_standards/vaccine_quality/pqs_prequalified_devices/en/index.html (accessed on 22 December 2019).
- Choe, Y.J.; Blatt, D.B.; Lee, H.J.; Choi, E.H. Associations between geographic region and immune response variations to pneumococcal conjugate vaccines in clinical trials: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 92, 261–268. [Google Scholar] [CrossRef] [Green Version]
- Ngocho, J.S.; Magoma, B.; Olomi, G.A.; Mahande, M.J.; Msuya, S.E.; de Jonge, M.I.; Mmbaga, B.T. Effectiveness of pneumococcal conjugate vaccines against invasive pneumococcal disease among children under five years of age in Africa: A systematic review. PLoS ONE 2019, 14, e0212295. [Google Scholar] [CrossRef]
- Ewald, H.; Briel, M.; Vuichard, D.; Kreutle, V.; Zhydkov, A.; Gloy, V. The Clinical Effectiveness of Pneumococcal Conjugate Vaccines: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Dtsch. Arztebl. Int. 2016, 113, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Sings, H.L.; De Wals, P.; Gessner, B.D.; Isturiz, R.; Laferriere, C.; McLaughlin, J.M.; Pelton, S.; Schmitt, H.J.; Suaya, J.A.; Jodar, L. Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine Against Invasive Disease Caused by Serotype 3 in Children: A Systematic Review and Meta-analysis of Observational Studies. Clin. Infect. Dis. 2019, 68, 2135–2143. [Google Scholar] [CrossRef]
- Alicino, C.; Paganino, C.; Orsi, A.; Astengo, M.; Trucchi, C.; Icardi, G.; Ansaldi, F. The impact of 10-valent and 13-valent pneumococcal conjugate vaccines on hospitalization for pneumonia in children: A systematic review and meta-analysis. Vaccine 2017, 35, 5776–5785. [Google Scholar] [CrossRef]
- Immunization Economics. Cost-Effectiveness and Budget Impact Analyses of PCV in Indonesia. Available online: http://immunizationeconomics.org/baselposter/suwantika (accessed on 8 May 2020).
- WHO. Pneumococcal vaccines WHO position paper–2012–recommendations. Vaccine 2012, 30 (Suppl. 32), 4717–4718. [Google Scholar] [CrossRef]
- WHO. Sustainable Access to Vaccines in Middle-Income Countries (MICs): A Shared Partner Strategy. Available online: https://www.who.int/immunization/sage/meetings/2015/april/Cernuschi_MIC_Strategy_SAGE_Apr2015.pdf?ua=1 (accessed on 8 December 2019).
- World Bank. The World Bank in Middle Income Countries. Available online: https://www.worldbank.org/en/country/mic/overview (accessed on 10 November 2019).
- WHO. Global Immunization Data 2015. Available online: http://www.who.int/immunization/newsroom/press/immunization_coverage_july_2016/en/ (accessed on 8 November 2019).
- Gavi. Pneumococcal Vaccine Support. Available online: http://www.gavi.org/support/nvs/pneumococcal/ (accessed on 8 November 2019).
- Tricarico, S.; McNeil, H.C.; Cleary, D.W. Pneumococcal conjugate vaccine implementation in middle-income countries. Pneumonia 2017, 9, 1–15. [Google Scholar] [CrossRef] [Green Version]
- CDC. CDC Vaccine Price List. Available online: https://www.cdc.gov/vaccines/programs/vfc/awardees/vaccine-management/price-list/index.html (accessed on 6 November 2019).
- World Bank. Data Bank. Available online: http://databank.worldbank.org/data/reports.aspx?Code=SP.POP.TOTL&id=af3ce82b&report_name=Popular_indicators&populartype=series&ispopular=y (accessed on 28 October 2019).
- Gavi. Historic Partnership between Gavi and India to Save Millions of Lives. Available online: http://www.gavi.org/library/news/press-releases/2016/historic-partnership-between-gavi-and-india-to-save-millions-of-lives/ (accessed on 28 October 2019).
- Hu, J.; Sun, X.; Huang, Z.; Wagner, A.L.; Carlson, B.; Yang, J.; Tang, S.; Li, Y.; Boulton, M.L.; Yuan, Z. Streptococcus pneumoniae and Haemophilus influenzae type b carriage in Chinese children aged 12–18 months in Shanghai, China: A cross-sectional study. BMC Infect. Dis. 2016, 16, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaddar, M.; Schmitt, S.; Makinen, M.; Milstien, J. Global support for new vaccine implementation in middle-income countries. Vaccine 2013, 31, B81–B96. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; Morris, D.E.; Clarke, S.C. Vaccination in Southeast Asia–reducing meningitis, sepsis and pneumonia with new and existing vaccines. Vaccine 2014, 32 (Suppl. 33), 4119–4123. [Google Scholar] [CrossRef] [PubMed]
- WHO. An Approach to Middle Income Countries: Options and Potential Impacts. Available online: https://www.who.int/immunization/sage/2_An_Approach_Middle_Income_Countries_Full_Paper.pdf (accessed on 28 October 2019).
- WHO. Advanced Market Commitments for Vaccines. Available online: https://www.who.int/immunization/newsroom/amcs/en/ (accessed on 30 March 2020).
- Cernuschi, T.; Furrer, E.; Schwalbe, N.; Jones, A.; Berndt, E.R.; McAdams, S. Advance market commitment for pneumococcal vaccines: Putting theory into practice. Bull. World Health Organ. 2011, 89, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Barder, O.; Kremer, M.; Levine, R. Making Markets for Vaccines: Ideas to Action (Working Group Report). Available online: http://www.cgdev.org/section/initiatives/_archive/vaccinedevelopment/chapters (accessed on 28 October 2019).
- Gavi. An Advance Market Commitment for Pneumococcal Vaccines (Joint Donor Statement). Available online: http://www.gavialliance.org/library/documents/amc/iwg-joint-donor-statement/ (accessed on 25 October 2019).
- Gavi. Advance Market Commitment for Pneumococcal Vaccines (Annual Report 1 April 2010–31 March 2011). Available online: http://www.gavialliance.org/library/gavi-documents/amc/2011-pneumococcal-amc-annual-report/ (accessed on 25 October 2019).
- UNICEF. The Advance Market Commitment for Pneumococcal Vaccine. Available online: http://www.unicef.org/supply/index_60990.html (accessed on 25 October 2019).
- Gavi. Advance Market Commitment for Pneumococcal Vaccine. Available online: https://www.gavi.org/sites/default/files/document/2015-pneumococcal-amc-annual-reportpdf.pdf (accessed on 20 October 2019).
- IFFIm. International Finance Facility for Immunisation. Available online: http://www.iffim.org/Funding-Gavi/Results/Pneumococcal-vaccine/ (accessed on 5 March 2020).
- Gavi. AVI Project Review. Available online: http://www.gavi.org/results/evaluations/avi-project-review/ (accessed on 20 October 2019).
- WHO; UNICEF. Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025. Available online: https://apps.who.int/iris/bitstream/handle/10665/79200/9789241505239_eng.pdf;jsessionid=5B5EA4F6490A1D258DA1279A52BFA765?sequence=1 (accessed on 4 February 2020).
- WHO. Benefits of Immunization. Available online: http://www.who.int/immunization/programmes_systems/supply_chain/benefits_of_immunization/en/ (accessed on 1 December 2013).
- WHO. Global Vaccine Action Plan Secretariat Annual Report 2015. Available online: http://www.who.int/immunization/global_vaccine_action_plan/gvap_ (accessed on 20 October 2019).
- PAHO. 2015. Available online: http://www.paho.org/HQ/index.php?option=com_content&view=article&id=1864%3A2014-paho-revolving-fund&catid=839%3Arevolving-fund&Itemid=4135&lang=ensecretariat_report_2015.pdf (accessed on 20 October 2019).
- PATH. Pneumonia and Pneumococcus Vaccine Development. Available online: http://sites.path.org/vaccinedevelopment/pneumonia-and-pneumococcus/vaccine-development/ (accessed on 20 October 2019).
- UNICEF. Vaccine Price List. Available online: www.unicef.org/supply/files/Product_Menu_0507.pdf (accessed on 25 December 2019).
- O’Brien, K.L.; Wolfson, L.J.; Watt, J.P.; Henkle, E.; Deloria-Knoll, M.; McCall, N.; Lee, E.; Mulholland, K.; Levine, O.S.; Cherian, T.; et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: Global estimates. Lancet 2009, 374, 893–902. [Google Scholar] [CrossRef]
- UNICEF. Handling Fees. Available online: https://www.unicef.org/supply/index_62330.html (accessed on 30 March 2020).
- WHO. Principles and Considerations for Adding a Vaccine to a National Immunization Programme: From Decision to Implementation and Monitoring. Available online: https://apps.who.int/iris/bitstream/handle/10665/111548/9789241506892_eng.pdf?sequence=1 (accessed on 10 October 2019).
- World Bank, Gavi. AMC Pilot Proposal 2006. Available online: www.vaccineamc.org/files/AMCPilotProposal.pdf (accessed on 22 December 2019).
- Usuf, E.; Mackenzie, G.; Ceesay, L.; Sowe, D.; Kampmann, B.; Roca, A. Vaccine wastage in the Gambia: A prospective observational study. BMC Public Health 2018, 18, 864. [Google Scholar] [CrossRef] [Green Version]
- WHO Vaccine Management Handbook. How to Calculate Vaccine Volumes and Cold Chain Capacity Requirements; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Chaiyakunapruk, N.; Somkrua, R.; Hutubessy, R.; Henao, A.M.; Hombach, J.; Melegaro, A.; Edmunds, J.W.; Beutels, P. Cost effectiveness of pediatric pneumococcal conjugate vaccines: A comparative assessment of decision-making tools. BMC Med. 2011, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- Saokaew, S.; Rayanakorn, A.; Wu, D.B.; Chaiyakunapruk, N. Cost effectiveness of pneumococcal vaccination in children in low-and middle-income countries: A systematic review. Pharmacoeconomics 2016, 34, 1211–1225. [Google Scholar] [CrossRef]
- Gavi. Indonesia Set to Introduce PCV into Routine Immunisation Programme. Available online: https://www.gavi.org/news/media-room/indonesia-protect-four-million-children-year-against-pneumonia (accessed on 8 May 2020).
- Trück, J.; Jawad, S.; Goldblatt, D.; Roalfe, L.; Snape, M.D.; Voysey, M.; Pollard, A.J. The antibody response following a booster with either a 10- or 13-valent pneumococcal conjugate vaccine in toddlers primed with a 13-valent pneumococcal conjugate vaccine in early infancy. Pediatr. Infect. Dis. J. 2016, 35, 787–793. [Google Scholar] [CrossRef] [Green Version]
- Los Santos, A.M.; Rodríguez-Weber, M.A.; Sánchez-Márquez, P.; Carreño-Manjarrez, R.; Cervantes-Apolinar, M.Y.; Ruiz-Guiñazú, J.; Ortega-Barria, E.; Borys, D. Immunogenicity of a 2+1 Infant Vaccination Series with 13-Valent Pneumococcal Conjugate Vaccine (PCV13) Followed by Pneumococcal Non-Typeable Haemophilus influenzae Protein D Conjugate Vaccine (PHiD-CV): A Randomized Trial Exploring Interchangeability of PCVs. Open Forum. Infect. Dis. 2017, 4 (suppl. 1), S538–S539. [Google Scholar]
- Urbancikova, I.; Prymula, R.; Goldblatt, D.; Roalfe, L.; Prymulova, K.; Kosina, P. Immunogenicity and safety of a booster dose of the 13-valent pneumococcal conjugate vaccine in children primed with the 10-valent or 13-valent pneu- mococcal conjugate vaccine in the Czech Republic and Slovakia. Vaccine 2017, 35, 5186–5193. [Google Scholar] [CrossRef] [PubMed]
- Dolhain, J.; Janssens, W.; Mesaros, N.; Hanssens, L.; Fierens, F. Hexavalent vaccines: Increasing options for policy-makers and providers. A review of the data supporting interchangeability (substitution with vaccines containing fewer antigens) and mixed schedules from the same manufacturer. Expert Rev. Vaccines 2018, 17, 513–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, S. Interchangeability of vaccines. Pediatr. Infect. Dis. J. 2001, 20, S23–S29. [Google Scholar] [CrossRef] [PubMed]
- WHO. Rabies vaccines: WHO position paper—April 2018. Wkly. Epidemiol. Rec. 2018, 93, 201–220. [Google Scholar]
- WHO. Measles vaccines: WHO position paper—April 2017. Wkly. Epidemiol. Rec. 2017, 92, 205–227. [Google Scholar]
- WHO. Pneumococcal Conjugate Vaccine (PCV) Review of Impact Evidence (PRIME): Summary of Findings from Systematic Review. Available online: https://www.who.int/immunization/sage/meetings/2017/october/3_FULL_PRIME_REPORT_2017Sep26.pdf?ua=1 (accessed on 25 October 2019).
- WHO. Pneumococcal vaccines WHO position paper—2012. Wkly. Epidemiol. Rec. 2012, 87, 129–144. [Google Scholar]
- PAHO. Final Report of the Technical Advisory Group on Vaccine-Preventable Diseases. Available online: https://www.paho.org/hq/dmdocuments/2011/vaccination-tag19-2011-FinalReport-Eng.pdf (accessed on 27 February 2019).
- WHO. Meeting of the Strategic Advisory Group of Experts on immunization, October 2017—Conclusions and recommendations. Wkly. Epidemiol. Rec. 2017, 92, 729–747. [Google Scholar]
- Desmet, S.; Verhaegen, J.; Van Ranst, M.; Peetermans, W.; Lagrou, K. Switch in a childhood pneumococcal vaccination programme from PCV13 to PCV10: A defendable approach? Lancet Infect. Dis. 2018, 18, 830–831. [Google Scholar] [CrossRef] [Green Version]
- Desmet, S.; Peetermans, W.; Lagrou, K. Switch in childhood pneumococcal vaccine in Belgium. Lancet Infect. Dis. 2018, 18, 945–946. [Google Scholar] [CrossRef] [Green Version]
- Izurieta, P.; Breuer, T. Interpretation of the switch in a childhood pneumococcal vaccination programme from PCV13 to PCV10 in Belgium. Lancet Infect. Dis. 2018, 18, 831–832. [Google Scholar] [CrossRef] [Green Version]
- Mrkvan, T.; Pelton, S.I.; Ruiz-Guinazu, J.; Palmu, A.A.; Borys, D. Effectiveness and impact of the 10-valent pneumococcal conjugate vaccine, PHiD-CV: Review of clinical trials and post-marketing experience. Expert Rev. Vaccines 2018, 17, 797–818. [Google Scholar] [CrossRef] [PubMed]
- Tsaban, G.; Ben-Shimol, S. Indirect (herd) protection, following pneumococcal conjugated vaccines introduction: A systematic review of the literature. Vaccine 2017, 35, 2882–2891. [Google Scholar] [CrossRef] [PubMed]
- Institut National de Santé Publique du Québec (Comité sur l’immu- nisation du Québec). Scientific Advisory on the Optimal Schedule for Childhood Immunization Against Pneumococcal Disease in Québec. Available online: https://www.inspq.qc.ca/sites/default/files/publications/2379_opinion_optimal_schedule_childhood_immunization_pneumococcal_disease.pdf (accessed on 25 August 2019).
- de Oliveira, L.H.; Camacho, L.A.; Coutinho, E.S.; Martinez-Silveira, M.S.; Carvalho, A.F.; Ruiz-Matus, C.; Toscano, C.M. Impact and effectiveness of 10 and 13-valent pneumococcal conjugate vaccines on hospitalization and mortality in children aged less than 5 years in Latin American countries: A systematic review. PLoS ONE 2016, 11, e0166736. [Google Scholar] [CrossRef] [PubMed]
- Domingues, C.M.; Verani, J.R.; Montenegro Renoiner, E.I.; de Cunto Brandileone, M.C.; Flannery, B.; de Oliveira, L.H.; Santos, J.B.; de Moraes, J.C.; Brazilian Pneumococcal Conjugate Vaccine Effectiveness Study Group. Effectiveness of ten-valent pneumococcal conjugate vaccine against invasive pneumococcal disease in Brazil: A matched case-control study. Lancet Respir. Med. 2014, 2, 464–471. [Google Scholar] [CrossRef]
- Jokinen, J.; Rinta-Kokko, H.; Siira, L.; Palmu, A.A.; Virtanen, M.J.; Nohynek, H.; Virolainen-Julkunen, A.; Toropainen, M.; Nuorti, J.P. Impact of ten-valent pneumococcal conjugate vaccination on invasive pneumococcal disease in Finnish children–a population-based study. PLoS ONE 2015, 10, e0120290. [Google Scholar] [CrossRef] [PubMed]
- Rinta-Kokko, H.; Palmu, A.A.; Auranen, K.; Pekka Nuorti, J.; Toropainen, M.; Siira, L.; Virtanen, M.J.; Nohynek, H.; Jokinen, J. Long-term impact of 10-valent pneumococcal conjugate vaccination on invasive pneumococcal disease among children in Finland. Vaccine 2018, 36, 1934–1940. [Google Scholar] [CrossRef] [Green Version]
- Verani, J.R.; Domingues, C.M.; de Moraes, J.C. Indirect cohort analysis of 10-valent pneumococcal conjugate vaccine effectiveness against vaccine-type and vaccine-related invasive pneumococcal disease. Vaccine 2015, 33, 6145–6148. [Google Scholar] [CrossRef]
- Andrews, N.J.; Waight, P.A.; Burbidge, P.; Pearce, E.; Roalfe, L.; Zancolli, M.; Slack, M.; Ladhani, S.N.; Miller, E.; Goldblatt, D. Serotype-specific effectiveness and correlates of protection for the 13-valent pneumococcal conjugate vaccine: A post licensure indirect cohort study. Lancet Infect. Dis. 2014, 14, 839–846. [Google Scholar] [CrossRef]
- Dominguez, A.; Ciruela, P.; Hernandez, S.; García-García, J.J.; Soldevila, N.; Izquierdo, C.; Moraga-Llop, F.; Díaz, A.; de Sevilla, M.F.; González-Peris, S.; et al. Effectiveness of the 13-valent pneumococcal conjugate vaccine in preventing invasive pneumococcal disease in children aged 7-59 months. A matched case-control study. PLoS ONE 2017, 12, e0183191. [Google Scholar] [CrossRef]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Holtzman, C.; Harrison, L.H.; Schaffner, W.; Zansky, S.M.; Rosen, J.B.; Reingold, L.; et al. Effectiveness of 13-valent pneumococcal conjugate vaccine for prevention of invasive pneumococcal disease in children in the USA: A matched case-control study. Lancet Respir. Med. 2016, 4, 399–406. [Google Scholar] [CrossRef]
- van der Linden, M.; Falkenhorst, G.; Perniciaro, S.; Fitzner, C.; Imohl, M. Effectiveness of Pneumococcal Conjugate Vaccines (PCV7 and PCV13) against invasive pneumococcal disease among children under two years of age in Germany. PLoS ONE 2016, 11, e0161257. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, R.; van der Linden, M.; Imohl, M.; von Kries, R. Vaccine effectiveness of PCV13 in a 3+1 vaccination schedule. Vaccine 2016, 34, 2062–2065. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, S.N.; Andrews, N.J.; Southern, J.; Jones, C.E.; Amirthalingam, G.; Waight, P.A.; England, A.; Matheson, M.; Bai, X.; Findlow, H.; et al. Antibody responses after primary immunization in infants born to women receiving a pertussis- containing vaccine during pregnancy: Single arm observational study with a historical comparator. Clin. Infect. Dis. 2015, 61, 1637–1644. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | PCV13 | PCV10 A | PCV10 B | ||
|---|---|---|---|---|---|
| 1 Dose/Vial | 4 Dose/Vial | 4 Dose/Vial | 1 Dose/Vial | 5 Dose/Vial | |
| Serotypes | 1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, 23F | 1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F, 23F | 1, 5, 6A, 6B, 7F, 9V, 14, 19A, 19F, 23F | ||
| WHO Prequalification | 2010 | 2016 | 2017 | 2020 | 2020 |
| Price per dose | $3.30 */$20.83 ** | $2.90 * | $3.05 * | $3.50 * | $2.00 * |
| Doses per fully immunized child | 3 | 3 | 3 | 3 | 3 |
| Indicative wastage rate | 5% | 8% | 8% | 5% | 8% |
| Shelf-life | 36 months at 2–8 ℃ | 36 months at 2–8 ℃ | 36 months at 2–8 ℃ | 36 months at 2–8 ℃ | 36 months at 2–8 ℃ |
| Cold chain volume per dose *** | 12.6 cm³ | 3.9 cm³ | 2.7 cm³ | 17.0 cm³ | 3.7 cm³ |
| Cost of cold room (per cm³) **** | $0.0013 | $0.0013 | $0.0013 | $0.0013 | $0.0013 |
| Handling open vials | N.A. | Opened vials may be kept for use in subsequent immunization sessions (up to 28 days from the withdrawals of the first injection if held at 2 to 8 ℃) | Opened vials may be kept for use in subsequent immunization sessions (up to 28 days from the withdrawals of the first injection if held at 2 to 8 ℃) | N.A. | Opened vials may be kept for use in subsequent immunization sessions (up to 28 days from the withdrawals of the first injection if held at 2 to 8 ℃) |
| Parameter | Value | Reference |
|---|---|---|
| Vaccine price | ||
| PCV13—1 dose/vial (Government contract price) | Base value = $20.83 (Min = $18.94; Max = $61.00) | [22] |
| PCV13—1 dose/vial (UNICEF price) * | Base value = $3.30 (Lower = $2.48; Upper = $4.13) | [61] |
| PCV13—4 doses/vial (UNICEF price) * | Base value = $2.90 (Lower = $2.18; Upper = $3.63) | [61] |
| PCV10 A—4 doses/vial (UNICEF price) * | Base value = $3.05 (Lower = $2.29; Upper = $3.81) | [61] |
| PCV10 B—5 doses/vial (UNICEF price) * | Base value = $2.00 (Lower = $1.50; Upper = $2.50) | [61] |
| Additional cost | ||
| Total additional cost ** | Base value = 23.0% (Min = 19.5%, Max = 38.0%) | |
| Vaccine wastage | ||
| Single-dose/vial | Median = 5.0% (Min = 1%; Max = 10%) | [26] |
| Multi-dose/vial | Median = 7.0% (Min = 1%; Max = 27%) | [26] |
| Safety stock | ||
| Total safety stock | Base value = 5% (Min = 0%; Max = 10%) | |
| Vaccine coverage | ||
| National coverage | Base value = 90.8% (Min = 46%, Max = 100%) | [25] |
| Cost of cold room | ||
| Cost per cm3 *** | Base value = $0.0013 (Min = $0.0005; Max = $0.0022) | [26,27] |
| IPD in children <1 years old | ||
| Incidence rate (per 100,000 population) | 2911 (Range = 2265–3622) | [62] |
| Risk reduction for IPD | ||
| PCV13 | Odds Ratio = 0.53 (95% CI; 0.36–0.78) | [30] |
| PCV10 A | Odds Ratio = 0.19 (95% CI; 0.11–0.33) | [30] |
| PCV10 B | N.A. |
| 2019 | 2020 | 2021 | 2022 | 2023 | 2024 |
|---|---|---|---|---|---|
| District/Province | District/Province | District/Province | District/Province | District/Province | District/Province |
| NTB | NTB | NTB | NTB | NTB | Indonesia |
| Bangka Belitung | Bangka Belitung | Bangka Belitung | Bangka Belitung | Bangka Belitung | |
| Kota Bogor | Jawa Barat | Jawa Barat | Jawa Barat | Jawa Barat | |
| Kota Bekasi | Jawa Timur | Jawa Timur | Jawa Timur | Jawa Timur | |
| Kota Surabaya | DKI Jakarta | DKI Jakarta | DKI Jakarta | ||
| Gresik | Banten | Banten | Banten | ||
| Sidoarjo | DI Yogyakarta | DI Yogyakarta | DI Yogyakarta | ||
| Jawa Tengah | Jawa Tengah | Jawa Tengah | |||
| Lampung | Lampung | Lampung | |||
| Sumatera Selatan | Sumatera Selatan | Sumatera Selatan | |||
| Bengkulu | Bengkulu | ||||
| Jambi | Jambi | ||||
| Riau | Riau | ||||
| Kepulauan Riau | Kepulauan Riau | ||||
| Sumatera Barat | Sumatera Barat | ||||
| Sumatera Utara | Sumatera Utara | ||||
| DI Aceh | DI Aceh | ||||
| Bali | Bali | ||||
| Gorontalo | |||||
| Sulawesi Utara | |||||
| Sulawesi Barat | |||||
| Sulawesi Tengah | |||||
| Sulawesi Selatan | |||||
| Sulawesi Tenggara | |||||
| Kalimantan Utara | |||||
| Kalimantan Barat | |||||
| Kalimantan Tengah | |||||
| Kalimantan Selatan | |||||
| Kalimantan Timur | |||||
| District | |||||
| Province | |||||
| Nationwide |
| Scenario | Year | Vaccine | Presentation | Price |
|---|---|---|---|---|
| Base-case | 2019–2023 | PCV13 | 1 dose/vial | Contract and Gavi-AMC price * |
| 2024 | PCV13 | 4 doses/vial | Gavi-AMC price | |
| Multi-dose PCV13 | 2019–2020 | PCV13 | 1 dose/vial | Contract price |
| 2021–2024 | PCV13 | 4 doses/vial | Gavi-AMC price | |
| Multi-dose PCV10 A | 2019–2020 | PCV13 | 1 dose/vial | Contract price |
| 2021–2024 | PCV10 A | 4 doses/vial | Gavi-AMC price | |
| Multi-dose PCV10 B | 2019–2020 | PCV13 | 1 dose/vial | Contract price |
| 2021–2024 | PCV10 B | 5 doses/vial | Gavi-AMC price |
| Cost | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | Total |
|---|---|---|---|---|---|---|---|
| Vaccine cost | |||||||
| Base case | $24,916,689 | $97,407,970 | $35,218,736 | $46,179,392 | $54,966,739 | $50,065,979 | $308,755,504 |
| Multi-dose PCV13 | $24,916,689 | $97,407,970 | $30,949,799 | $40,581,890 | $48,304,104 | $50,065,979 | $292,226,430 |
| Multi-dose PCV10 A | $24,916,689 | $97,407,970 | $32,550,650 | $42,680,953 | $50,802,592 | $52,655,598 | $301,014,452 |
| Multi-dose PCV10 B | $24,916,689 | $97,407,970 | $21,344,689 | $27,987,510 | $33,313,175 | $34,528,261 | $239,498,294 |
| Cold chain cost | |||||||
| Base case | $19,590 | $76,586 | $142,124 | $186,356 | $221,817 | $71,162 | $717,636 |
| Multi-dose PCV13 | $19,590 | $76,586 | $43,991 | $57,682 | $68,658 | $71,162 | $337,669 |
| Multi-dose PCV10 A | $19,590 | $76,586 | $30,079 | $39,440 | $46,945 | $48,658 | $261,299 |
| Multi-dose PCV10 B | $19,590 | $76,586 | $41,359 | $54,231 | $64.550 | $66,904 | $323,220 |
| Total saving | |||||||
| Multi-dose PCV13 | $0 | $0 | $4,367,071 | $5,726,176 | $6,815,794 | $0 | $16,909,042 |
| Multi-dose PCV10 A | $0 | $0 | $2,780,131 | $3,645,354 | $4,339,018 | −$2,567,15 | $8,197,389 |
| Multi-dose PCV10 B | $0 | $0 | $13,974,813 | $18,324,007 | $21,810,831 | $15,541,975 | $69,651,626 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwantika, A.A.; Zakiyah, N.; Kusuma, A.S.W.; Abdulah, R.; Postma, M.J. Impact of Switch Options on the Economics of Pneumococcal Conjugate Vaccine (PCV) Introduction in Indonesia. Vaccines 2020, 8, 233. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020233
Suwantika AA, Zakiyah N, Kusuma ASW, Abdulah R, Postma MJ. Impact of Switch Options on the Economics of Pneumococcal Conjugate Vaccine (PCV) Introduction in Indonesia. Vaccines. 2020; 8(2):233. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020233
Chicago/Turabian StyleSuwantika, Auliya A., Neily Zakiyah, Arif S. W. Kusuma, Rizky Abdulah, and Maarten J. Postma. 2020. "Impact of Switch Options on the Economics of Pneumococcal Conjugate Vaccine (PCV) Introduction in Indonesia" Vaccines 8, no. 2: 233. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020233