ImmunizziAMO: A School-Based Field Trial to Teach New Generations the Importance of Vaccination through Games and to Fight Vaccine Hesitancy in Italy

 , , ,
, , ,
Abstract
:1. Introduction
- to increase knowledge about communicable diseases and the concept of herd immunity;
- to make vaccination understood as a prevention tool;
- to change behaviors through reliable sources of information;
- to promote the achievement of high vaccination coverage.
2. Materials and Methods
2.1. Day 1
- Are bacteria and viruses dangerous?
- How do you defend the human body from bacteria and viruses?
- What do antibodies do?
- What does the vaccine do to the child?
- Do you think the vaccine protects against disease?
- How long does the vaccine protect you?
- Does the mother pass antibodies to her child?
- Do you think vaccinated children protect unvaccinated children?
2.2. Day 2
2.3. Day 3
- “I defend myself” to find out how the immune memory generated by the vaccine works. A puzzle game explaining how the antibody binds to the antigen.
- “If I protect myself, I protect you” about the concept of herd immunity consisting of a game of stamps and inks to create a poster to take to school.
- “I wash my hands” on the importance of washing hands. It was explained how long do germs and bacteria live? The concept of contamination was shown with Petri dishes and microscopes
- “I present to you the vaccine” a fun quiz to learn together how to defend ourselves by developing defenses immunity. At the end of the game, a certificate was given to everyone.
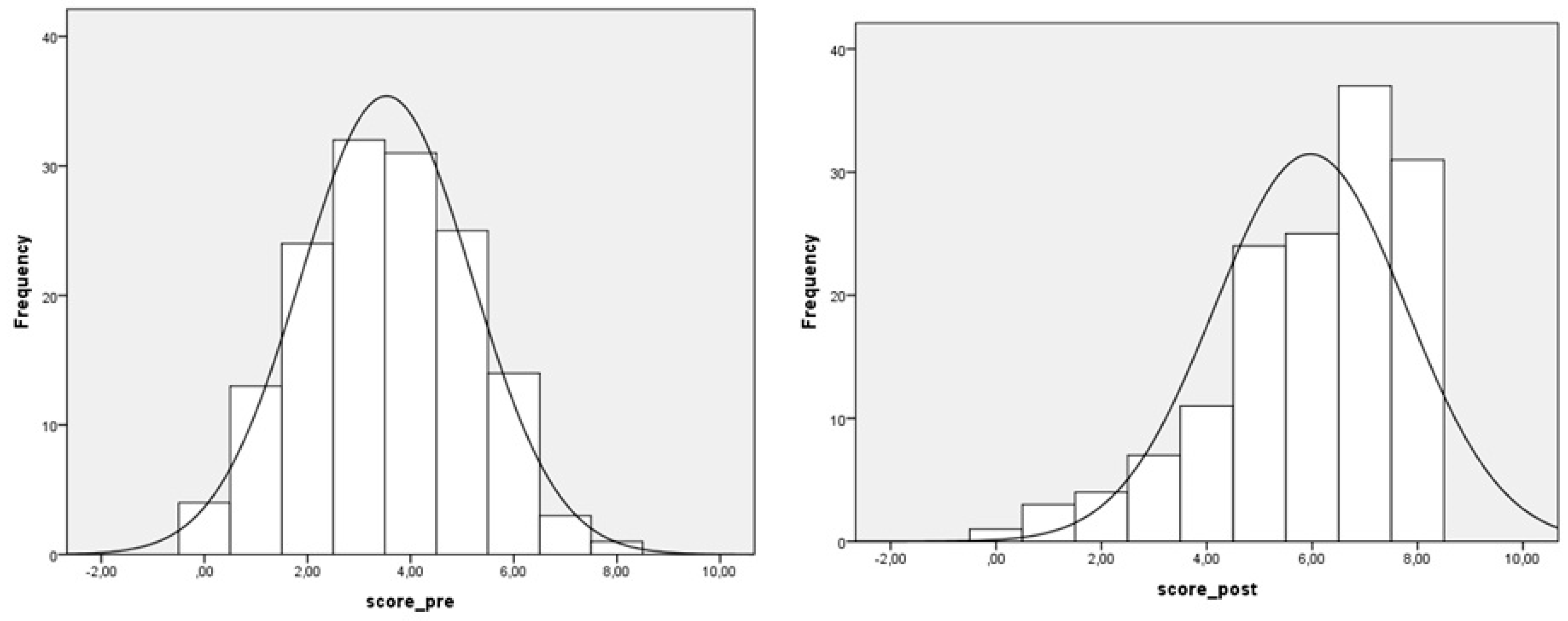
2.4. Sample Size and Statistical Analysis
- Mean score pre-intervention: 4.00 points
- Mean score pre-intervention: 5.00 points
- SD: 2.00 points
- Significance: 0.05
- Power: 80%
3. Results
3.1. Descriptive Analysis of the Sample
3.2. Analysis of Knowledge
4. Discussion
- game-based health promotion interventions are effective with young children, as well as adolescents and young adults;
- game-based health promotion interventions can be tailored to educate about infectious diseases;
- positive effects on mental health and social behavior of children to be taken into account;
- long-and short-term interventions may gain similar efficacy.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statement
Note
References
- Ministero della Giustizia. LEGGE 31 luglio 2017, n. 11. In Conversione in Legge, Con Modificazioni, del Decreto-Legge 7 Giugno 2017, n. 73, Recante Disposizioni Urgenti In Materia Di Prevenzione Vaccinale. Available online: http://www.gazzettaufficiale.it/eli/gu/2017/08/05/182/sg/pdf (accessed on 6 June 2020).
- Bozzola, M.; Spina, G.; Russo, R.; Bozzola, M.; Corsello, G.; Villani, A. Mandatory vaccinations in European countries, undocumented information, false news and the impact on vaccination uptake: The position of the Italian pediatric society. Ital. J. Pediatr. 2018, 44, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Law 31-7-2017 - Disposizioni Urgenti In Materia Di Prevenzione Vaccinale. Available online: https://www.gazzettaufficiale.it/eli/id/2017/08/05/17A05515/sg (accessed on 6 June 2020).
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Copertura Vaccinale in Italia [Internet]. Available online: https://www.epicentro.iss.it/vaccini/dati_ita (accessed on 7 March 2020).
- Nowak, G.J.; Gellin, B.G.; MacDonald, N.E.; Butler, R.; SAGE Working Group on Vaccine Hesitancy. Addressing vaccine hesitancy: The potential value of commercial and social marketing principles and practices. Vaccine 2015, 33, 4204–4211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskola, J.; Duclos, P.; Schuster, M.; MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. How to deal with vaccine hesitancy? Vaccine 2015, 33, 4215–4217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Torre, G.; Sinopoli, A.; Sestili, C.; D’Egidio, V.; Bella, O.D.; Cocchiara, R.A.; Sciarra, I.; Saulle, R.; Backhaus, I.; Mannocci, A. “GiochiAMO”: A school-based smoking and alcohol prevention program for children - A pilot randomized field trial. Part 2. Ann. di Ig. 2018, 30, 273–284. [Google Scholar]
- D’Egidio, V.; Lia, L.; Sinopoli, A.; Backhaus, I.; Mannocci, A.; Saulle, R.; Sestili, C.; Cocchiara, R.; Bella, O.D.; Yordanov, T.; et al. Results of the Italian project “GiochiAMO” to improve nutrition and PA among children. J. Public Health 2019. [Google Scholar]
- Cocchiara, R.A.; Sestili, C.; Bella, O.D. “ GiochiAMO,” a Gaming Intervention to Prevent Smoking and Alcohol Habits Among Children. Games Health J. 2020, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Masala, D.; De Santis, M.G.; Mannocci, A.; D’Egidio, V.; La Torre, G. Pedagogical-educational-didactic interpretation of the Game “ GiochiAMO … sano”. Ital. J. Health Educ. Sports Incl. Didact. 2017, 2, 61–65. [Google Scholar]
- Celata, F.; Lucciarini, S. Atlante delle Disuguaglianze A Roma [Atlas of Inequalities in Rome]; Camera di Commercio Industria Artigianato e Agricoltura di Roma: Rome, Italy, 2016. [Google Scholar]
- McPhee, S.J.; Nguyen, T.; Euler, G.L.; Mock, J.; Wong, C.; Lam, T.; Buu, C. Successful promotion of hepatitis B vaccinations among Vietnamese-American children ages 3 to 18: Results of a controlled trial. Pediatrics 2003, 111, 1278–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chantler, T.; Karafillakis, E.; Wodajo, S.; Demissie, S.D.; Sile, B.; Mohammed, S.; Larson, H.J. ‘We all work together to vaccinate the child’: A formative evaluation of a community-engagement strategy aimed at closing the immunization gap in North-West Ethiopia. Int. J. Environ. Res. Public Health 2018, 15, 667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagneur, A.; Quach, C.; Boucher, F.D.; Tapiero, B.; De Wals, P.; Farrands, A.; Dubé, È. Promoting vaccination in the province of Québec: The PromoVaQ randomized controlled trial protocol. BMC Public Health 2019, 19, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owais, A.; Hanif, B.; Siddiqui, A.R.; Ajmal, A.; Zaidi, A.K. Does improving maternal knowledge of vaccines impact infant immunization rates? A community-based randomized-controlled trial in Karachi, Pakistan. BMC Public Health 2011, 11, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyhan, B.; Reifler, J.; Richey, S.; Freed, G.L. Effective messages in vaccine promotion: A randomized trial. Pediatrics 2014, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartolini, R.M.; Winkler, J.L.; Penny, M.E.; Lamontagne, D.S. Parental Acceptance of HPV Vaccine in Peru: A Decision Framework. PLoS ONE 2012, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, L.; Bonhomme, L.-A.; Cooper, S.C.; Joseph, J.G.; Zimet, G.D. Educational interventions to increase HPV vaccination acceptance: A systematic review. Vaccine 2014, 32, 1901–1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, C.; Restivo, V.; Ventura, G.; D’Angelo, C.; Randazzo, M.A.; Casuccio, N.; Palermo, M.; Casuccio, A.; Vitale, F. Increased vaccination coverage among adolescents and young adults in the district of Palermo as a result of a public health strategy to counteract an ‘epidemic panic. ’ Int. J. Environ. Res. and Public Health 2018, 15, 1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansell, A.H.; Giacobbi, J.P.R.; Voelker, D.K. A Scoping Review of Sport-Based Health Promotion Interventions With Youth in Africa. Health Promot. Pract. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Question | Pre-Intervention | Post-Intervention |
|---|---|---|
| 1 | 83 (48.5%) | 115 (80.3%) |
| 2 | 57 (33.3%) | 91 (63.9%) |
| 3 | 75 (43.9%) | 108 (75.5%) |
| 4 | 102 (59.6%) | 114 (79.6%) |
| 5 | 60 (35.1%) | 75 (52.7%) |
| 6 | 94 (55%) | 105 (73.3%) |
| 7 | 57 (33.3%) | 114 (79.6%) |
| 8 | 67 (39.2%) | 130 (91%) |
| Group | Mean | SD | p Value |
|---|---|---|---|
| First classes | 2.55 | 2.23 | 0.619 |
| Second classes | 2.36 | 2.12 | |
| Podere Rosa school | 2.41 | 2.18 | 0.666 |
| San Cleto school | 2.61 | 2.17 | |
| Females | 2.58 | 2.33 | 0.740 |
| Males | 2.32 | 2.06 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Torre, G.; D’Egidio, V.; Sestili, C.; Cocchiara, R.A.; Cianfanelli, S.; Di Bella, O.; Lia, L.; Dorelli, B.; Cammalleri, V.; Backhaus, I.; et al. ImmunizziAMO: A School-Based Field Trial to Teach New Generations the Importance of Vaccination through Games and to Fight Vaccine Hesitancy in Italy. Vaccines 2020, 8, 280. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020280
La Torre G, D’Egidio V, Sestili C, Cocchiara RA, Cianfanelli S, Di Bella O, Lia L, Dorelli B, Cammalleri V, Backhaus I, et al. ImmunizziAMO: A School-Based Field Trial to Teach New Generations the Importance of Vaccination through Games and to Fight Vaccine Hesitancy in Italy. Vaccines. 2020; 8(2):280. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020280
Chicago/Turabian StyleLa Torre, Giuseppe, Valeria D’Egidio, Cristina Sestili, Rosario Andrea Cocchiara, Sara Cianfanelli, Ornella Di Bella, Lorenza Lia, Barbara Dorelli, Vittoria Cammalleri, Insa Backhaus, and et al. 2020. "ImmunizziAMO: A School-Based Field Trial to Teach New Generations the Importance of Vaccination through Games and to Fight Vaccine Hesitancy in Italy" Vaccines 8, no. 2: 280. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020280