Impact of a Catch-Up Strategy of DT-IPV Vaccination during Hospitalization on Vaccination Coverage among People Over 65 Years of Age in France: The HOSPIVAC Study (Vaccination during Hospitalization)

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Randomization Procedure
2.3. Sample Size Calculation
2.4. Data Sources
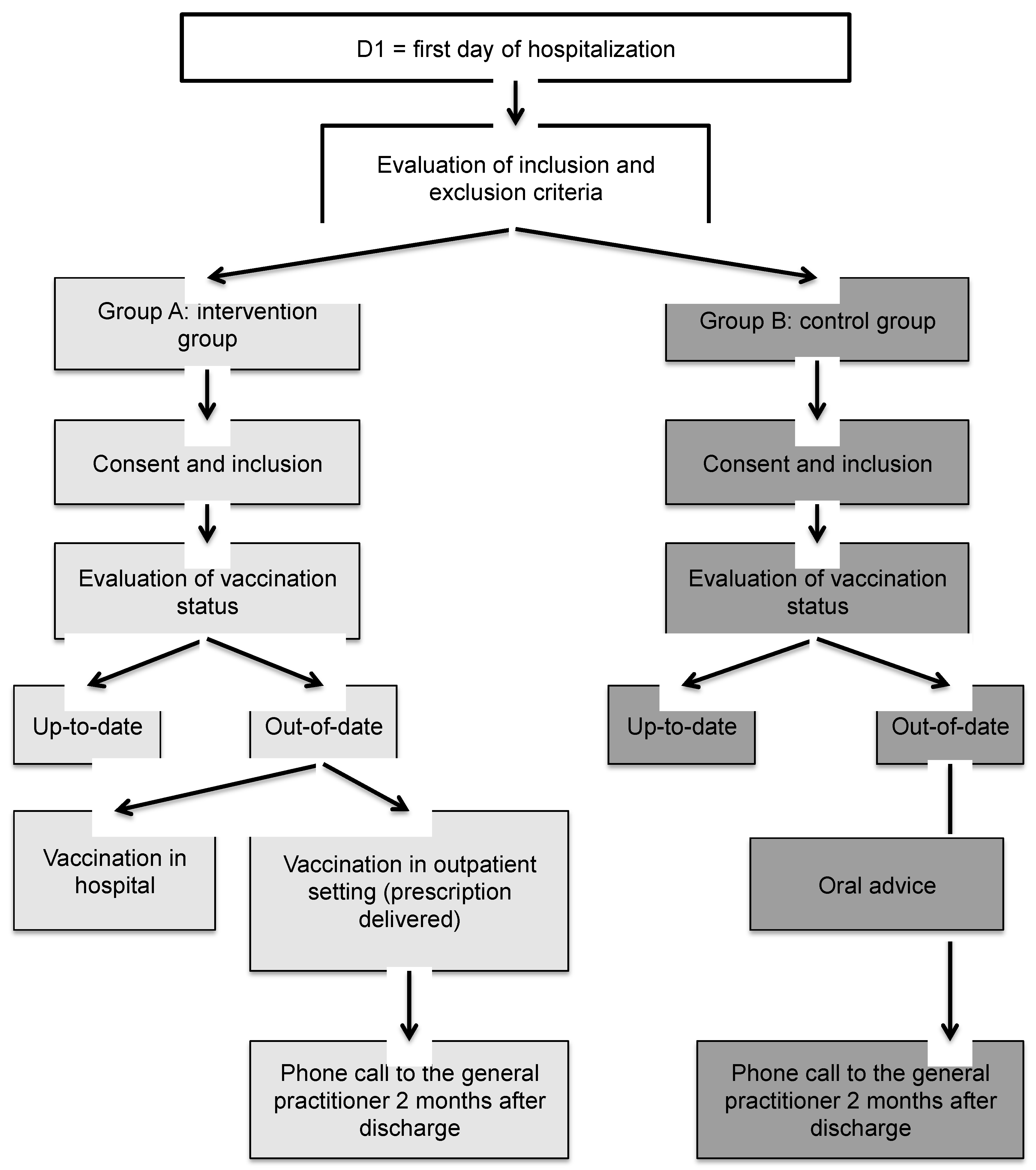
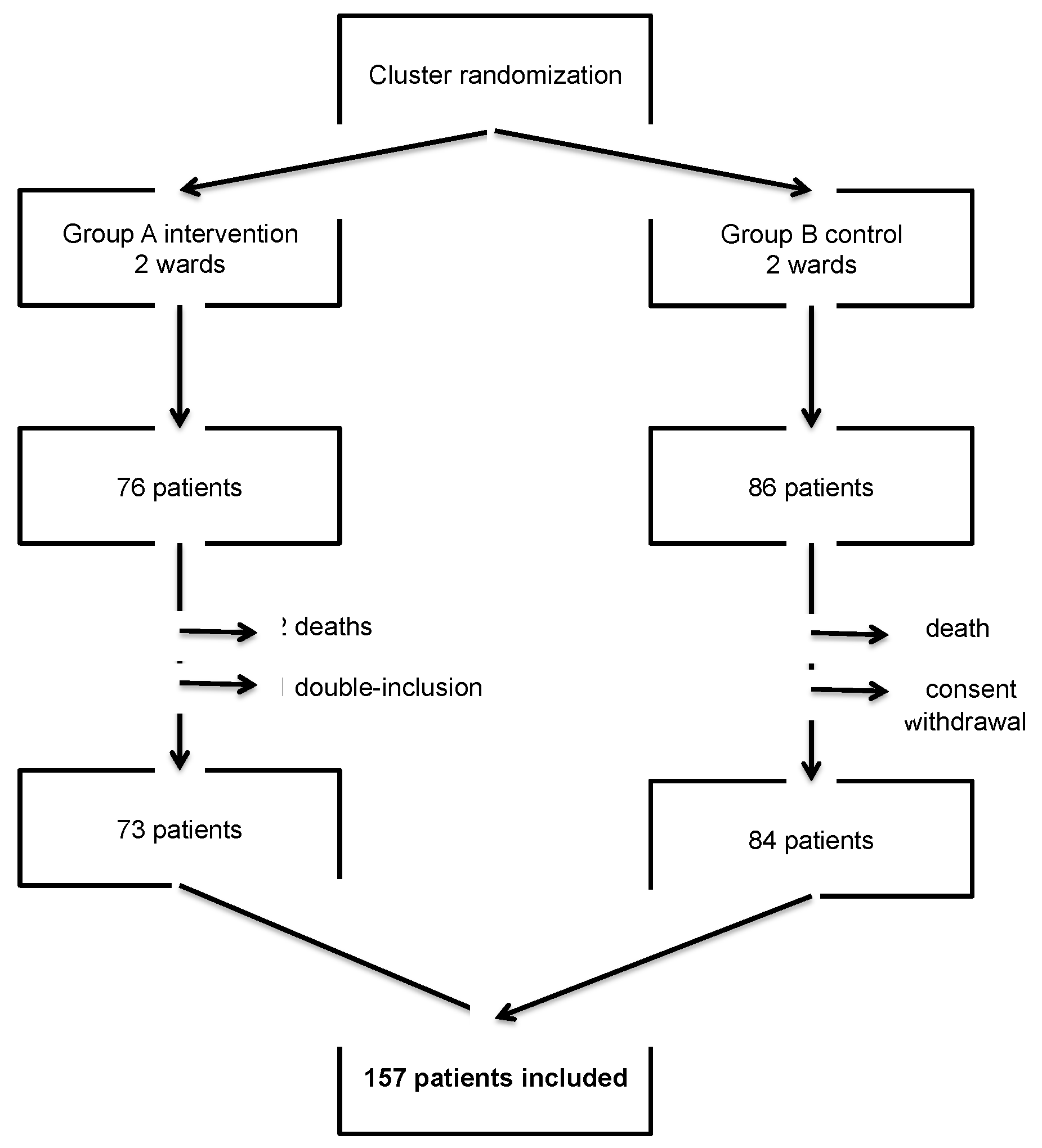
2.5. Flow Chart
2.6. Statistical Analysis
2.7. Vaccines
2.8. Ethical Issues
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fine, P.; Eames, K.; Heymann, D.L. “Herd immunity”: A rough guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, B.; Schirmer, M.; Matteucci Gothe, R.; Siebert, U.; Fuchs, D.; Grubeck-Loebenstein, B. Recall Responses to Tetanus and Diphtheria Vaccination Are Frequently Insufficient in Elderly Persons. Borrow R, editor. PLoS ONE 2013, 8, e82967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SPF. Enquête Nationale de Couverture Vaccinale, France, Janvier 2011. Couverture Vaccinale Contre la Grippe Saisonnière Dans les Groupes Cibles et Mesure de l’efficacité Vaccinale. Couverture Vaccinale par Les Vaccins Diphtérie-Tétanos-Poliomyélite (dTP) et. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-a-prevention-vaccinale/diphterie/documents/rapport-synthese/enquete-nationale-de-couverture-vaccinale-france-janvier-2011.-couverture-vaccinale-contre-la-grippe-saisonniere-dans-les-groupes-cibles-et-mesur (accessed on 25 April 2020).
- Célant, N.; Guillaume, S.; Rochereau, T. Enquête sur la Santé et la Protection Sociale 2012. Available online: https://www.irdes.fr/recherche/2014/rapport-556-enquete-sur-la-sante-et-la-protection-sociale-2012.html (accessed on 25 April 2020).
- HCSP. Vaccination des Personnes âgées: Recommandations. Paris: Haut Conseil de la Santé Publique; 2016 Mar. Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=559 (accessed on 25 April 2020).
- Guthmann, J.-P.; Fonteneau, L.; Antona, D.; Lévy-Bruhl, D. Factors associated with tetanus vaccination coverage in adults in France and with knowledge of vaccination status. Med. Mal. Infect. 2010, 40, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Goirand, L.; Charrel, M.; Dell’Accio, P.; Stahl, J.-P.; Da Silva, É.; Billette de Villemeur, A. La couverture vaccinale des adultes: Enquêtes dans quatre populations d’Isère (France), 2002–2003. Santé Publique 2012, 24, 329. [Google Scholar] [CrossRef]
- Products-Data Briefs-Number 281—June 2017. 2019. Available online: https://www.cdc.gov/nchs/products/databriefs/db281.htm (accessed on 25 April 2020).
- La, E.M.; Trantham, L.; Kurosky, S.K.; Odom, D.; Aris, E.; Hogea, C. An analysis of factors associated with influenza, pneumoccocal, Tdap, and herpes zoster vaccine uptake in the US adult population and corresponding inter-state variability. Hum. Vaccin. Immunother. 2018, 14, 430–441. [Google Scholar] [CrossRef]
- À l’horizon 2050, plus d’un Quart de Personnes âgées de 65 ans ou plus dans les Pays de la Loire. Available online: https://www.insee.fr/fr/statistiques/2868681#graphique-Figure_2 (accessed on 25 April 2020).
- Kyaw, M.H.; Greene, C.M.; Schaffner, W.; Ray, S.M.; Shapiro, M.; Barrett, N.L.; Gershman, K.; Craig, A.S.; Roberson, A.; Zell, E.R.; et al. Adults with invasive pneumococcal disease: Missed opportunities for vaccination. Am. J. Prev. Med. 2006, 31, 286–292. [Google Scholar] [CrossRef]
- Arencibia Jiménez, M.; Navarro Gracia, J.F.; Delgado de Los Reyes, J.A.; Pérez Torregrosa, G.; López Parra, D.; López García, P. Missed opportunities in antipneumococcal vaccination. Can something more be done for prevention? Arch. Bronconeumol. 2014, 50, 93–98. [Google Scholar] [CrossRef]
- Lu, P.-J.; O’Halloran, A.; Ding, H.; Srivastav, A.; Williams, W.W. Uptake of Influenza Vaccination and Missed Opportunities Among Adults with High-Risk Conditions, United States, 2013. Am. J. Med. 2016, 129, 636.e1–636.e11. [Google Scholar] [CrossRef] [Green Version]
- Djibo, D.A.; Peddecord, K.M.; Wang, W.; Ralston, K.; Sawyer, M.H. Factors Associated With Missed Opportunities for Influenza Vaccination: Review of Medical Records in a Diverse Sample of Primary Care Clinics, San Diego County, 2010-2011. J. Prim. Care Community Health 2015, 6, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Restrepo-Méndez, M.C.; Barros, A.J.D.; Wong, K.L.M.; Johnson, H.L.; Pariyo, G.; Wehrmeister, F.C.; Victora, C.G. Missed opportunities in full immunization coverage: Findings from low- and lower-middle-income countries. Glob Health Action 2016, 9. [Google Scholar] [CrossRef] [Green Version]
- Fu, L.Y.; Zook, K.; Gingold, J.; Gillespie, C.W.; Briccetti, C.; Cora-Bramble, D.; Joseph, J.G.; Moon, R.Y. Frequent vaccination missed opportunities at primary care encounters contribute to underimmunization. J. Pediatr. 2015, 166, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Williams, W.W.; Lu, P.-J.; O’Halloran, A.; Kim, D.K.; Grohskopf, L.A.; Pilishvili, T.; Skoff, H.T.; Nelson, N.P.; Harpaz, R.; Markowitz, L.E.; et al. Surveillance of Vaccination Coverage Among Adult Populations—United States, 2014. MMWR Surveill Summ. 2016, 65, 1–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Professionnels de Santé Au 1er Janvier 2017 | Insee. Available online: https://www.insee.fr/fr/statistiques/2012677#tableau-TCRD_068_tab1_departements (accessed on 25 April 2020).
- Etudes-Qualitatives.pdf. Available online: http://concertation-vaccination.fr/wp-content/uploads/2016/11/Etudes-qualitatives.pdf (accessed on 25 April 2020).
- Diphtérie. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-a-prevention-vaccinale/diphterie (accessed on 25 April 2020).
- Antona, D.; Maine, C.; Lévy-Bruhl, D. Le tétanos en France entre 2012 et 2017. Bull Epidémiol Hebd. 2018, 42, 828–833. [Google Scholar]
- Rapport-de-la-concertation-citoyenne-sur-la-vaccination.pdf. Available online: http://concertation-vaccination.fr/wp-content/uploads/2016/11/Rapport-de-la-concertation-citoyenne-sur-la-vaccination.pdf (accessed on 25 April 2020).
- Pahud, B.; Clark, S.; Herigon, J.C.; Sherman, A.; Lynch, D.A.; Hoffman, A.; Jackson, M.A. A pilot program to improve vaccination status for hospitalized children. Hosp. Pediatr. 2015, 5, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Eval_Interventions_Ameliorer_Pratiques_Guide.pdf. Available online: https://www.has-sante.fr/upload/docs/application/pdf/eval_interventions_ameliorer_pratiques_guide.pdf (accessed on 25 April 2020).
- Weinberger, B. Adult vaccination against tetanus and diphtheria: The European perspective: Adult vaccination against tetanus and diphtheria. Clin. Exp. Immunol. 2017, 187, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Baratin, D.; Del Signore, C.; Thierry, J.; Caulin, E.; Vanhems, P. Evaluation of adult dTPaP vaccination coverage in France: Experience in Lyon city, 2010–2011. BMC Public Health 2012, 12, 940. [Google Scholar] [CrossRef] [Green Version]
- Klett-Tammen, C.J.; Krause, G.; Seefeld, L.; Ott, J.J. Determinants of tetanus, pneumococcal and influenza vaccination in the elderly: A representative cross-sectional study on knowledge, attitude and practice (KAP). BMC Public Health 2015, 16, 121. [Google Scholar] [CrossRef] [Green Version]
- DMP: Découvrir le DMP. Available online: https://www.dmp.fr/ps/je-decouvre (accessed on 25 April 2020).
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy. Hum. Vaccin. Immunother. 2013, 1, 1763–1773. [Google Scholar] [CrossRef]
- Halperin, B.A.; MacDougall, D.; MacKinnon-Cameron, D.; Li, L.; McNeil, S.A.; Langley, J.M.; Halperin, S.A. Universal tetanus, diphtheria, acellular pertussis (Tdap) vaccination of adults: What the Canadian public knows and wants to know. Vaccine 2015, 33, 6840–6848. [Google Scholar] [CrossRef]
- Gautier, A.; Fournier, C.; Beck, F. Pratiques et opinions des médecins généralistes en matière de prévention. Santé Publique 2011, 77, 5–10. [Google Scholar]
- Vaccination à l’officine-Les Pharmaciens—Ordre National des Pharmaciens. Available online: http://www.ordre.pharmacien.fr/Les-pharmaciens/Champs-d-activites/Vaccination-a-l-officine (accessed on 25 April 2020).
- Nowalk, M.P.; Lin, C.J.; Pavlik, V.N.; Brown, A.E.; Zhang, S.; Moehling, K.K.; Raviotta, J.M.; South-Paul, J.E.; Hawk, M.; Ricci, E.M.; et al. Using the 4 PillarsTM Practice Transformation Program to increase adult Tdap immunization in a randomized controlled cluster trial. Vaccine 2016, 34, 5026–5033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leidner, A.J.; Murthy, N.; Chesson, H.W.; Biggerstaff, M.; Stoecker, C.; Harris, A.M.; Acosta, A.; Dooling, K.; Bridges, C. Cost-effectiveness of adult vaccinations: A systematic review. Vaccine 2019, 37, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Zimmerman, R.K.; Nowalk, M.P.; Lin, C.J. Cost-Effectiveness of the 4 Pillars Practice Transformation Program to Improve Vaccination of Adults Aged 65 and Older. J. Am. Geriatr. Soc. 2017, 65, 763–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A = 73 | Group B = 84 | p | |
|---|---|---|---|
| Sex n (%) | |||
| Female | 48 (65.8%) | 47 (55.9%) | 0.210 |
| Male | 25 (34.2%) | 37 (44.1%) | |
| Mean age (min–max) | |||
| 78.1 (65–96) | 81.4 (65–97) | 0.994 | |
| Family situation n (%) 1 | |||
| Couple | 30 (41.1%) | 49 (58.3%) | 0.012 |
| Single | 37 (50.7%) | 34 (40.5%) | |
| Unknown | 6 (8.2%) | ||
| Residence n (%) 1 | |||
| Personal home | 70 (95.9%) | 77 (91.7%) | 0.456 |
| Community residence | 3 (4.1%) | 6 (7.2%) | |
| Complementary health insurance n (%) | |||
| Yes | 73 (100%) | 79 (94%) | 0.106 |
| No | 0 | 3 (3.6%) | |
| No information | 0 | 2 (2.4%) | |
| Group A = 73 | Group B = 84 | p | |
|---|---|---|---|
| Consultation with the general practitioner within the previous year n (%) 1 | |||
| Yes | 71 (97.3%) | 82 (98.8%) | 0.486 |
| No | 2 (2.7%) | 1 (1.2%) | |
| Hospitalization within the previous year n (%) 2 | |||
| Yes | 37 (51.4%) | 48 (57.8%) | 0.421 |
| No | 35 (48.6%) | 35 (42.2%) | |
| Impression of being in good health n (%) | |||
| Yes | 36 (49.3%) | 41 (48.8%) | 0.306 |
| No | 29 (39.7%) | 39 (46.4%) | |
| Don’t know | 8 (11%) | 4 (4.8%) | |
| Confidence in the general practitioner 1 | |||
| Yes | 62 (84.9%) | 74 (89.2%) | 0.06 |
| No | 3 (4.1%) | 7 (8.4%) | |
| Don’t know | 8 (11%) | 2 (2.4%) | |
| Sufficient information on vaccination status provided by the general practitioner n (%) 3 | |||
| Yes | 38 (53.5%) | 37 (44.6%) | 0.469 |
| No | 30 (42.3%) | 40 (48.2%) | |
| Don’t know | 3 (4.2%) | 6 (7.2%) | |
| Sufficient information about vaccination provided by the general practitioner n (%) 3 | |||
| Yes | 31 (43.7%) | 33 (39.8%) | 0.513 |
| No | 34 (47.9%) | 46 (55.4%) | |
| Don’t know | 6 (8.4%) | 4 (4.8%) | |
| Confidence in vaccination n (%) 1 | |||
| Yes | 59 (80.8%) | 68 (81.9%) | 0.646 |
| No | 8 (11%) | 11 (13.3%) | |
| Don’t know | 6 (8.2%) | 4 (4.8%) | |
| Group A = 73 | Group B = 84 | p | |
|---|---|---|---|
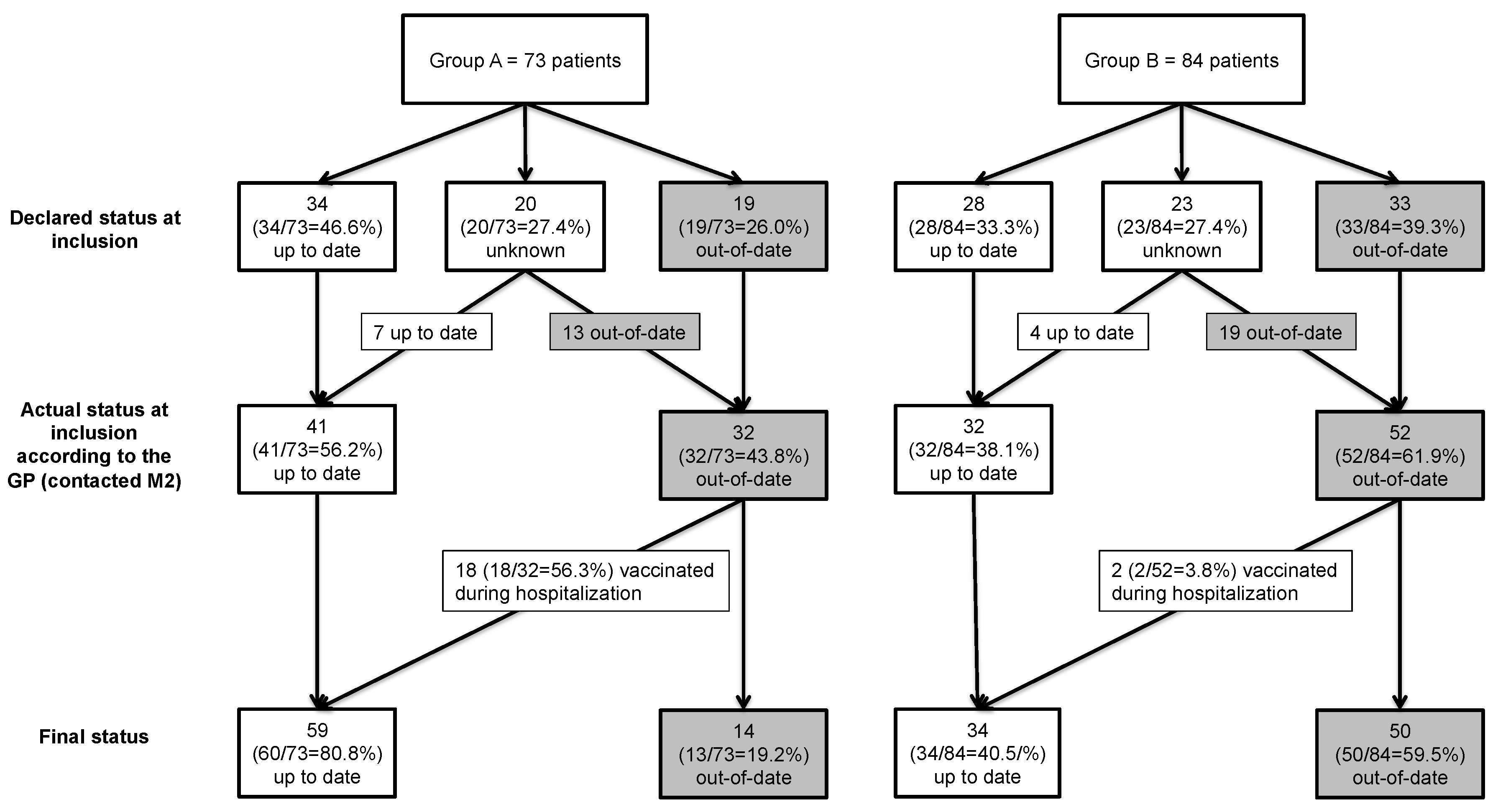
| Vaccination coverage based on actual vaccination status at inclusion (%) | |||
| 56.2% | 38.1% | 0.024 | |
| Vaccination coverage at the end of the study (%) | |||
| 80.8% | 40.5% | ||
| Increase in vaccination coverage (%) | |||
| 24.6% | 2.4% | <0.001 | |
| Factors Studied | Crude OR | (95% CI) * | p ** | Adjusted OR | (95% CI) * | p ** |
|---|---|---|---|---|---|---|
| Sex | 0.786 | 0.424 | ||||
| Female | ref | ref | ||||
| Male | 0.92 | [0.48–1.74] | 0.97 | [0.36–1.54] | ||
| Age | 0.031 | 0.116 | ||||
| 0.96 | [0.92–1] | 0.97 | [0.92–1] | |||
| Consultation with general practitioner in the preceding year | 0.633 | |||||
| No | ref | |||||
| Yes | 1.78 | [0.16–20] | ||||
| Hospitalization during the preceding year | 0.32 | |||||
| No | ref | |||||
| Yes | 1.38 | [0.73–2.61] | ||||
| Impression of being in good health | 0.9 | |||||
| No | ref | |||||
| Yes | 1.1 | [0.57–2.12] | 0.767 | |||
| Don’t know | 0.85 | [0.25–2.95] | 0.467 | |||
| Confidence in general practitioner | 0.53 | |||||
| No | ref | |||||
| Yes | 2.14 | [0.53–8.61] | 0.286 | |||
| Don’t know | 2.33 | [0.37–14.6] | 0.365 | |||
| Sufficient information about vaccination provided by the general practitioner | 0.00001 | 0.00001 | ||||
| No | ref | ref | ||||
| Yes | 5.4 | [2.64–11.05] | 0.0001 | 5.07 | [2.45–10.51] | |
| Don’t know | 6.15 | [1.46–25.93] | 0.013 | 6.57 | [1.52–28.32] | |
| Confidence in vaccination | 0.076 | NS | ||||
| No | ref | |||||
| Yes | 2.84 | [0.97–8.37] | 0.058 | |||
| Don’t know | 1.2 | [0.22–6.53] | 0.833 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanchi, S.; Vaux, J.; Toqué, J.M.; Hery, L.; Laforest, S.; Piccoli, G.B.; Crochette, N. Impact of a Catch-Up Strategy of DT-IPV Vaccination during Hospitalization on Vaccination Coverage among People Over 65 Years of Age in France: The HOSPIVAC Study (Vaccination during Hospitalization). Vaccines 2020, 8, 292. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020292
Blanchi S, Vaux J, Toqué JM, Hery L, Laforest S, Piccoli GB, Crochette N. Impact of a Catch-Up Strategy of DT-IPV Vaccination during Hospitalization on Vaccination Coverage among People Over 65 Years of Age in France: The HOSPIVAC Study (Vaccination during Hospitalization). Vaccines. 2020; 8(2):292. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020292
Chicago/Turabian StyleBlanchi, Sophie, Justine Vaux, Jean Marc Toqué, Ludovic Hery, Servane Laforest, Giorgina Barbara Piccoli, and Nicolas Crochette. 2020. "Impact of a Catch-Up Strategy of DT-IPV Vaccination during Hospitalization on Vaccination Coverage among People Over 65 Years of Age in France: The HOSPIVAC Study (Vaccination during Hospitalization)" Vaccines 8, no. 2: 292. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8020292