Pneumococcal Vaccination for Children in Asian Countries: A Systematic Review of Economic Evaluation Studies

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
3. Results
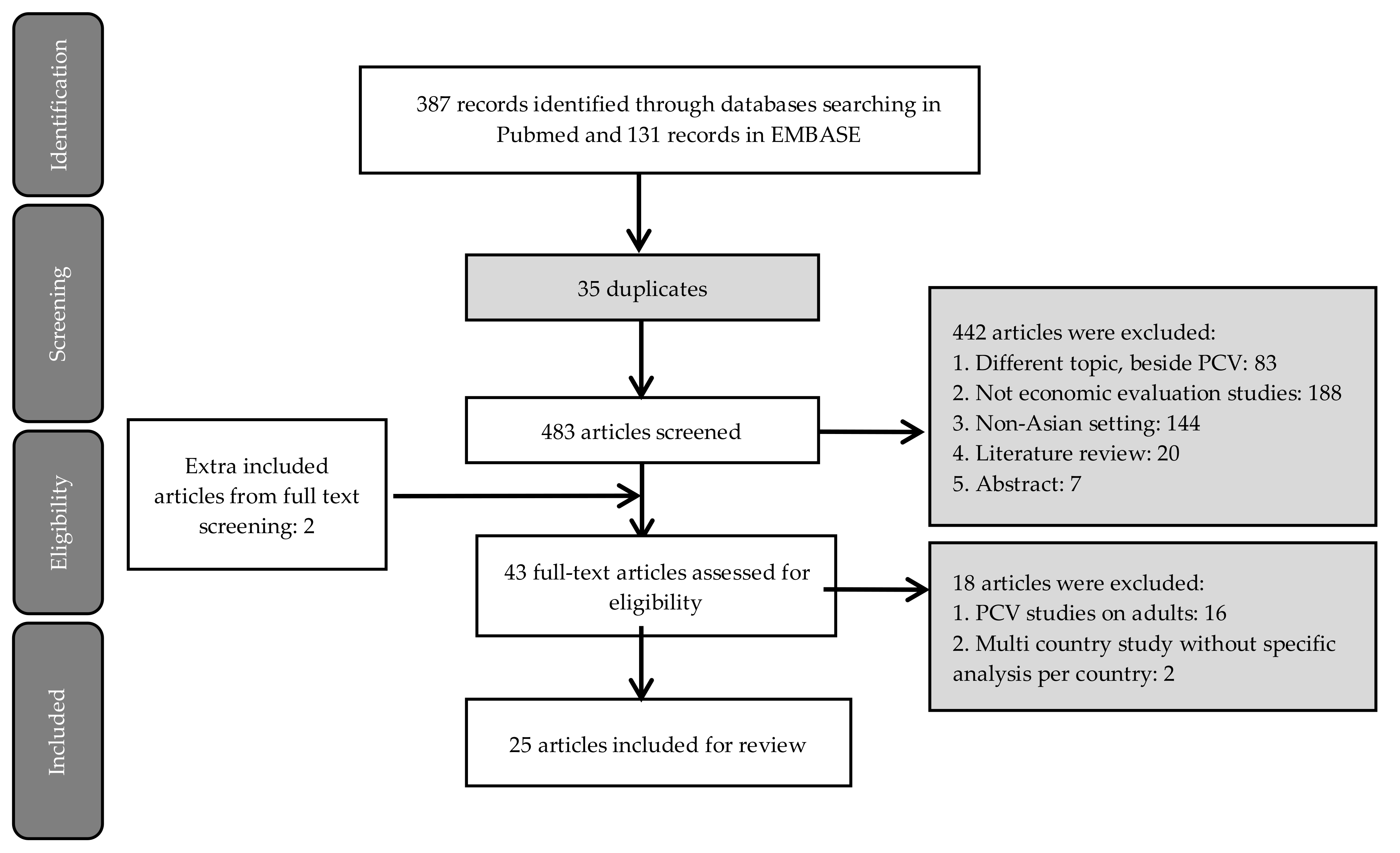
3.1. Systematic Search
3.2. Characteristics of Included Studies
3.2.1. Study Design
3.2.2. Cost Component
3.2.3. Study Findings
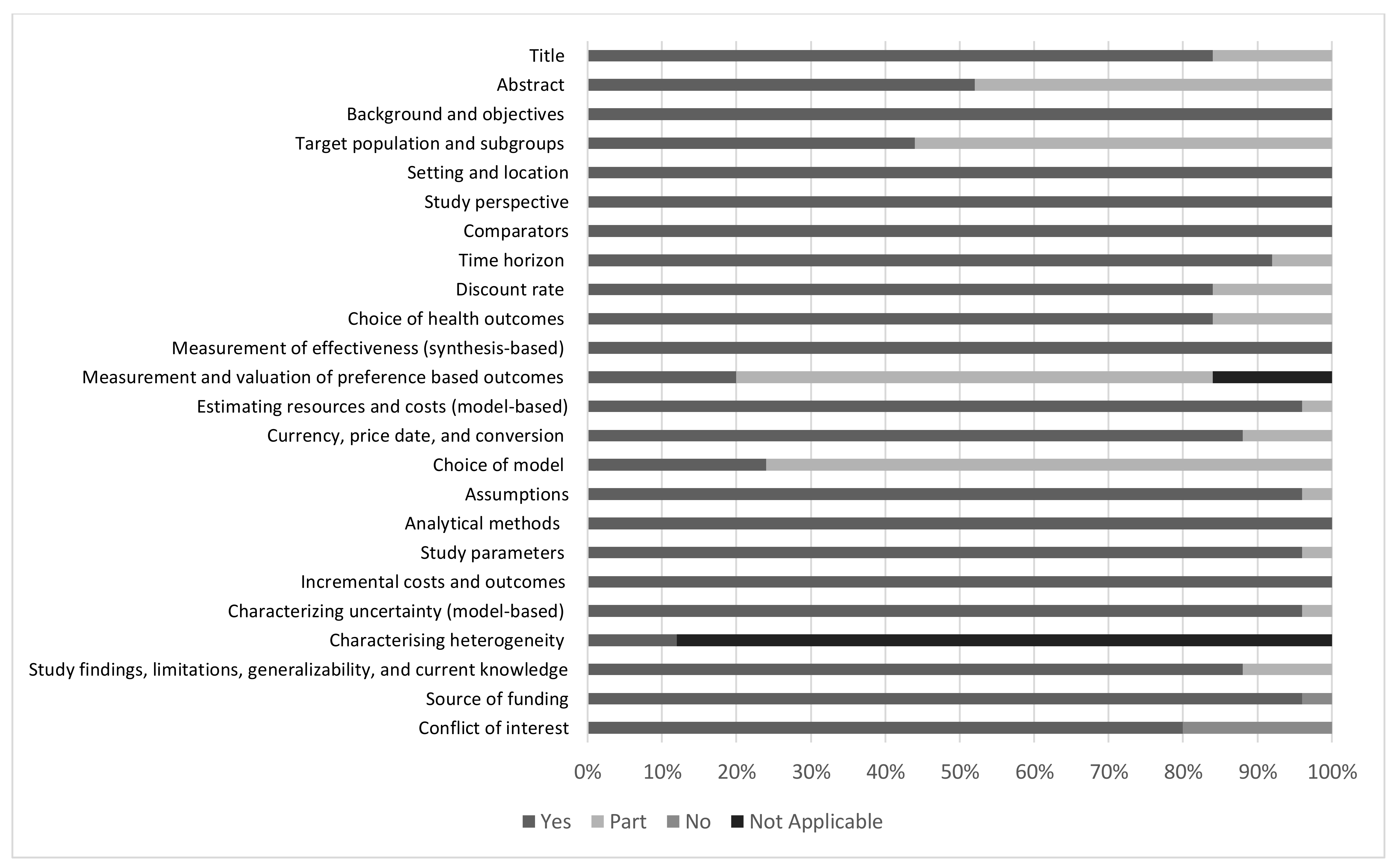
3.2.4. Quality of Reporting
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Li, Y.; An, Z.; Yin, D.; Liu, Y.; Huang, Z.; Ma, Y.; Li, H.; Li, Q.; Wang, H. Disease burden of community acquired pneumonia among children under 5 year old in China: A population based survey. Hum. Vaccines Immunother. 2017, 13, 1681–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Pneumonia Fact Sheet. 2016. Available online: http://www.who.int/mediacentre/factsheets/fs331/en/ (accessed on 30 July 2020).
- Hussain, M.; Melegaro, A.; Pebody, R.G.; George, R.; Edmunds, W.J.; Talukdar, R.; Martin, S.A.; Efstratiou, A.; Miller, E. A longitudinal household study of Streptococcus pneumoniae nasopharyngeal carriage in a UK setting. Epidemiol. Infect. 2005, 133, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Bogaert, D.; De Groot, R.; Hermans, P. Streptococcus pneumoniae colonisation: The key to pneumococcal disease. Lancet Infect. Dis. 2004, 4, 144–154. [Google Scholar] [CrossRef]
- Bravo, L.C. Overview of the disease burden of invasive pneumococcal disease in Asia. Vaccine 2009, 27, 7282–7291. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.L.; Wolfson, L.J.; Watt, J.P.; Henkle, E.; Deloria-Knoll, M.; McCall, N.; Lee, E.; Mulholland, K.; Levine, O.S.; Cherian, T. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: Global estimates. Lancet 2009, 374, 893–902. [Google Scholar] [CrossRef]
- Tan, T.Q. Pediatric Invasive Pneumococcal Disease in the United States in the Era of Pneumococcal Conjugate Vaccines. Clin. Microbiol. Rev. 2012, 25, 409–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feikin, D.R.; Hammitt, L.L.; Murdoch, D.R.; O’Brien, K.L.; Scott, J.A.G. The Enduring Challenge of Determining Pneumonia Etiology in Children: Considerations for Future Research Priorities. Clin. Infect. Dis. 2017, 64, S188–S196. [Google Scholar] [CrossRef]
- Maimaiti, N.; Ahmed, Z.; Isa, Z.M.; Ghazi, H.F.; Aljunid, S.M. Clinical Burden of Invasive Pneumococcal Disease in Selected Developing Countries. Value Health Reg. Issues 2013, 2, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Ho, Y.-C.; Lee, P.-L.; Wang, Y.-C.; Chen, S.-C.; Chen, K.-T. The economic burden of childhood invasive pneumococcal diseases and pneumonia in Taiwan: Implications for a pneumococcal vaccination program. Hum. Vaccines Immunother. 2015, 11, 1081–1087. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.L.; Moulton, L.H.; Reid, R.; Weatherholtz, R.; Oski, J.; Brown, L.; Kumar, J.; Parkinson, A.; Hu, D.; Hackell, J.; et al. Efficacy and safety of seven-valent conjugate pneumococcal vaccine in American Indian children: Group randomised trial. Lancet 2003, 36, 355–361. [Google Scholar] [CrossRef]
- Fireman, B.; Black, S.; Shinefield, H.R.; Lee, J.; Lewis, E.; Ray, P. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatr. Infect. Dis. J. 2003, 22, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.; Madhi, S.A. Review on the immunogenicity and safety of PCV-13 in infants and toddlers. Expert Rev. Vaccines 2011, 10, 951–980. [Google Scholar] [CrossRef] [PubMed]
- Temple, B.; Toan, N.T.; Dai, V.T.T.; Bright, K.; Licciardi, P.V.; Marimla, R.A.; Nguyen, C.D.; Uyen, D.Y.; Balloch, A.; Huu, T.N.; et al. Immunogenicity and reactogenicity of ten-valent versus 13-valent pneumococcal conjugate vaccines among infants in Ho Chi Minh City, Vietnam: A randomised controlled trial. Lancet Infect. Dis. 2019, 19, 497–509. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Pneumococcal vaccines: WHO position paper—2012. Available online: https://www.who.int/immunization/position_papers/PP_pneumococcal_April_2012_summary.pdf?u (accessed on 30 July 2020).
- Rudan, I.; O’Brien, K.L.; Nair, H.; Liu, L.; Theodoratou, E.; Qazi, S.; Lukšić, I.; Walker, C.L.F.; Black, R.E.; Campbell, H. Epidemiology and etiology of childhood pneumonia in 2010: Estimates of incidence, severe morbidity, mortality, underlying risk factors and causative pathogens for 192 countries. J. Glob. Health 2013, 3, 10401. [Google Scholar] [CrossRef]
- Kumar, R.; Arora, N.; Santosham, M. South Asia symposium on pneumococcal disease and the promise of vaccines—Meeting report. Vaccine 2016, 34, 2622–2626. [Google Scholar] [CrossRef] [Green Version]
- Le, C.F.; Jefferies, J.M.; Yusof, M.Y.M.; Sekaran, S.D.; Clarke, S.C. The epidemiology of pneumococcal carriage and infections in Malaysia. Expert Rev. Anti-Infect. Ther. 2012, 10, 707–719. [Google Scholar] [CrossRef]
- Kim, J.J. The Role of Cost-Effectiveness in U.S. Vaccination Policy. N. Engl. J. Med. 2011, 365, 1760–1761. [Google Scholar] [CrossRef]
- Shiragami, M.; Mizukami, A.; Leeuwenkamp, O.; Mrkvan, T.; Delgleize, E.; Kurono, Y.; Iwata, S. Cost-Effectiveness Evaluation of the 10-Valent Pneumococcal Non-typeable Haemophilus influenzae Protein D Conjugate Vaccine and 13-Valent Pneumococcal Vaccine in Japanese Children. Infect. Dis. Ther. 2014, 4, 93–112. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, U.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- The World Bank. PPP Conversion Factor. Available online: http://data.worldbank.org/indicator/PA.NUS.PPP (accessed on 30 July 2020).
- The World Bank. Inflation, GDP Deflator. Available online: https://data.worldbank.org/indicator/ny.gdp.defl.zs (accessed on 30 July 2020).
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)—Explanation and Elaboration: A Report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013, 16, 231–250. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.-H.; Leeuwenkamp, O.; Oh, K.-B.; Lee, Y.E.; Kim, C.-M. Cost-effectiveness analysis of infant pneumococcal vaccination with PHiD-CV in Korea. Hum. Vaccines Immunother. 2017, 14, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Maurer, K.A.; Chen, H.-F.; Wagner, A.L.; Hegde, S.T.; Patel, T.; Boulton, M.L.; Hutton, D.W. Cost-effectiveness analysis of pneumococcal vaccination for infants in China. Vaccine 2016, 34, 6343–6349. [Google Scholar] [CrossRef]
- Wu, D.B.C.; Rinaldi, F.; Huang, Y.C.; Chang, J.A.; Chang, C.J. Economic evaluation of universal 7-valent pneumococcal conjugate vaccination in Taiwan: A cost-effectiveness analysis. J. Formos. Med. Assoc. 2013, 112, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.K.C.; Chia Wu, B.D.; Topachevskyi, O.; Delgleize, E.; DeAntonio, R. The health economic impact of universal infant vaccination with the 10-valent pneumococcal nontypeable haemophilus influenzae protein d conjugate vaccine as compared with 13-valent pneumococcal conjugate vaccine in Hong Kong. Value Heal. Reg. Issues 2013, 2, 64–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.K.C.; Rinaldi, F.; Chan, M.K.; Chan, S.T.; So, T.M.; Hon, E.K.; Lee, V.W.Y. Economic Evaluation of Universal Infant Vaccination with 7vPCV in Hong Kong. Value Health 2009, 12, S42–S48. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.; Shi, Q.; Song, S.; Du, L.; He, J.; Chen, C.-I.; Caldwell, R.; Wang, B.; Roberts, C.S. Estimating the Cost-Effectiveness of the 7-Valent Pneumococcal Conjugate Vaccine in Shanghai, China. Value Heal. Reg. Issues 2014, 3, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Haasis, M.A.; Ceria, J.A.; Kulpeng, W.; Teerawattananon, Y.; Alejandria, M. Do Pneumococcal Conjugate Vaccines Represent Good Value for Money in a Lower-Middle Income Country? A Cost-Utility Analysis in the Philippines. PLoS ONE 2015, 10, e0131156. [Google Scholar] [CrossRef]
- Che, D.; Zhou, H.; He, J.; Wu, B. Modeling the impact of the 7-valent pneumococcal conjugate vaccine in Chinese infants: An economic analysis of a compulsory vaccination. BMC Health Serv. Res. 2014, 14, 56. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, R.; Roberts, C.S.; An, Z.; Chen, C.-I.; Wang, B.C.M. The health and economic impact of vaccination with 7-valent pneumococcal vaccine (PCV7) during an annual influenza epidemic and influenza pandemic in China. BMC Infect. Dis. 2015, 15, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljunid, S.M.; Maimaiti, N.; Ahmed, Z.; Nur, A.M.; Isa, Z.M.; Azmi, S.; Sulong, S. Economic Impact of Pneumococcal Protein-D Conjugate Vaccine (PHiD-CV) on the Malaysian National Immunization Programme. Value Health Reg. Issues 2014, 3, 146–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; He, J.; Wu, B.; Che, D. Cost-effectiveness analysis of routine 13-valent pneumococcal conjugate vaccinations in Chinese infants. Hum. Vaccines Immunother. 2018, 14, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.H.; Nievera, M.C.; Carlos, J.; Lucero, M.; Bibera, G.; Atienza, M.I.; Topachevskyi, O.; Navarro-Locsin, C.G. Cost-Effectiveness Analysis of Pneumococcal Vaccination with the Pneumococcal Polysaccharide NTHi Protein D Conjugate Vaccine in the Philippines. Value Heal. Reg. Issues 2014, 3, 156–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorji, K.; Phuntsho, S.; Kumluang, S.; Khuntha, S.; Kulpeng, W.; Rajbhandari, S.; Teerawattananon, Y. Pempa Towards the introduction of pneumococcal conjugate vaccines in Bhutan: A cost-utility analysis to determine the optimal policy option. Vaccine 2018, 36, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, S.-L.; Kondo, M.; Okubo, I. Economic evaluation of vaccination programme of 13-valent pneumococcal conjugate vaccine to the birth cohort in Japan. Vaccine 2013, 31, 2762–2771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshi, S.-L.; Kondo, M.; Okubo, I. Economic evaluation of vaccination programme of 7-valent pneumococcal conjugate vaccine to the birth cohort in Japan. Vaccine 2012, 30, 3320–3328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamoorthy, Y.; Eliyas, S.K.; Nair, N.P.; Sakthivel, M.; Sarveswaran, G.; Chinnakali, P. Impact and cost effectiveness of pneumococcal conjugate vaccine in India. Vaccine 2019, 37, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Shen, K.; Wasserman, M.D.; Liu, N.; Yang, Y.-H.; Yang, J.; Guzauskas, G.F.; Wang, B.C.M.; Hilton, B.; Farkouh, R. Estimating the cost-effectiveness of an infant 13-valent pneumococcal conjugate vaccine national immunization program in China. PLoS ONE 2018, 13, e0201245. [Google Scholar] [CrossRef]
- Wu, D.B.-C.; Roberts, C.; Lee, V.W.Y.; Hong, L.-W.; Tan, K.K.; Mak, V.; Lee, K.K.C. Cost-effectiveness analysis of infant universal routine pneumococcal vaccination in Malaysia and Hong Kong. Hum. Vaccin. Immunother. 2016, 12, 403–416. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.B.-C.; Chang, C.-J.; Huang, Y.-C.; Wen, Y.-W.; Wu, C.-L.; Fann, C.S.-J. Cost-effectiveness analysis of pneumococcal conjugate vaccine in Taiwan: A transmission dynamic modeling approach. Value Health 2012, 15, S15–S19. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.J.; Saha, A.; Zhang, X.-H. Cost-effectiveness analysis of a universal mass vaccination program with a PHiD-CV 2 + 1 schedule in Malaysia. Cost Eff. Resour. Alloc. 2017, 15, 17. [Google Scholar] [CrossRef] [Green Version]
- Sundaram, N.; Chen, C.; Yoong, J.; Luvsan, M.-E.; Fox, K.; Sarankhuu, A.; La Vincente, S.F.; Jit, M. Cost-effectiveness of 13-valent pneumococcal conjugate vaccination in Mongolia. Vaccine 2017, 35, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Sohn, H.S.; Suh, D.-C.; Jang, E.; Kwon, J.-W. Economic Evaluation of Childhood 7-Valent Pneumococcal Conjugate Vaccination in Korea. J. Manag. Care Pharm. 2010, 16, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Kulpeng, W.; Leelahavarong, P.; Rattanavipapong, W.; Sornsrivichai, V.; Baggett, H.C.; Meeyai, A.; Punpanich, W.; Teerawattananon, Y. Cost-utility analysis of 10- and 13-valent pneumococcal conjugate vaccines: Protection at what price in the Thai context? Vaccine 2013, 31, 2839–2847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, X.; Tobe, R.G.; Liu, X.; Mori, R. Cost-effectiveness and Health Benefits of Pediatric 23-valent Pneumococcal Polysaccharide Vaccine, 7-valent Pneumococcal Conjugate Vaccine and Forecasting 13-valent Pneumococcal Conjugate Vaccine in China. Pediatr. Infect. Dis. J. 2016, 35, e353–e361. [Google Scholar] [CrossRef]
- Countries Eligible for Support. 2018. Available online: http://www.gavi.org/support/sustainability/countries-eligible-for-support/ (accessed on 30 July 2020).
- Lee, K.; Chow, D.; Lee, V.W.Y. Pin24 an Initial Cost-Effectiveness Analysis of the New 13-Valent Pneumococcal Conjugate Vaccine (PCV-I 3) Versus PCV-7 in the Public Sector of Hong Kong. Value Heal. 2010, 13, A190. [Google Scholar] [CrossRef]
- Song, J.Y.; Choi, J.Y.; Lee, J.S.; Bae, I.-G.; Kim, Y.-K.; Sohn, J.W.; Jo, Y.M.; Choi, W.S.; Lee, J.; Park, K.H.; et al. Clinical and economic burden of invasive pneumococcal disease in adults: A multicenter hospital-based study. BMC Infect. Dis. 2013, 13, 202. [Google Scholar] [CrossRef] [Green Version]
- WHO-CHOICE. Making choices in health: Who guide to cost-effectiveness analysis. Rev. Española Salud Pública 2004, 78, 409–410. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, D.; Luttjeboer, J.; Westra, T.A.; Wilschut, J.C.; Suwantika, A.A.; Daemen, T.; Atthobari, J.; Wilffert, B.; Postma, M.J. The cost–effectiveness of HPV vaccination in addition to screening: A Dutch perspective. Expert Rev. Vaccines 2014, 14, 589–604. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Goldie, S.J. Cost-effectiveness analyses of vaccination programmes: A focused review of modelling approaches. Pharmacoeconomics 2008, 26, 191–215. [Google Scholar] [CrossRef]
- Lugnér, A.K.; Mylius, S.D.; Wallinga, J. Dynamic versus static models in cost-effectiveness analyses of anti-viral drug therapy to mitigate an influenza pandemic. Health Econ. 2009, 19. [Google Scholar] [CrossRef]
- Harboe, Z.B.; Dalby, T.; Weinberger, D.; Benfield, T.; Mølbak, K.; Slotved, H.-C.; Suppli, C.H.; Konradsen, H.B.; Valentiner-Branth, P. Impact of 13-Valent Pneumococcal Conjugate Vaccination in Invasive Pneumococcal Disease Incidence and Mortality. Clin. Infect. Dis. 2014, 59, 1066–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Review of Vaccine Price Data. Available online: https://www.euro.who.int/__data/assets/pdf_file/0009/284832/Review-vaccine-price-data.pdf?ua=1 (accessed on 30 July 2020).
- Rozenbaum, M.; Sanders, E.A.M.; Van Hoek, A.J.; Jansen, A.G.S.C.; Van Der Ende, A.; Dobbelsteen, G.V.D.; Rodenburg, G.D.; Hak, E.; Postma, M.J. Cost effectiveness of pneumococcal vaccination among Dutch infants: Economic analysis of the seven valent pneumococcal conjugated vaccine and forecast for the 10 valent and 13 valent vaccines. BMJ 2010, 340, c2509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmu, A.A.; Jokinen, J.; Nieminen, H.; Rinta-Kokko, H.; Ruokokoski, E.; Puumalainen, T.; Borys, R.; Lommel, P.; Traskine, M.; Moreira, M.; et al. Effect of pneumococcal Haemophilus influenzae protein D conjugate vaccine (PHiD-CV10) on outpatient antimicrobial purchases: A double-blind, cluster randomised phase 3–4 trial. Lancet Infect. Dis. 2014, 14, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Daniel, M.; Qureishi, A.; Lee, Y.; Belfield, K.; Birchall, J.P. Update on otitis media—Prevention and treatment. Infect. Drug Resist. 2014, 7, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saokaew, S.; Rayanakorn, A.; Wu, D.B.-C.; Chaiyakunapruk, N. Cost Effectiveness of Pneumococcal Vaccination in Children in Low- and Middle-Income Countries: A Systematic Review. Pharmacoeconomics 2016, 34, 1211–1225. [Google Scholar] [CrossRef]
- Chen, C.; Liceras, F.C.; Flasche, S.; Sidharta, S.; Yoong, J.; Sundaram, N.; Jit, M. Effect and cost-effectiveness of pneumococcal conjugate vaccination: A global modelling analysis. Lancet Glob. Health 2019, 7, e58–e67. [Google Scholar] [CrossRef] [Green Version]
- Woods, B.; Revill, P.; Sculpher, M.; Claxton, K. Country-Level Cost-Effectiveness Thresholds: Initial Estimates and the Need for Further Research. Value Health 2016, 19, 929–935. [Google Scholar] [CrossRef] [Green Version]
- Suwantika, A.A.; Zakiyah, N.; Kusuma, A.S.W.; Abdulah, R.; Postma, M.J. Impact of Switch Options on the Economics of Pneumococcal Conjugate Vaccine (PCV) Introduction in Indonesia. Vaccines 2020, 8, 233. [Google Scholar] [CrossRef]
- Friedberg, M.; Saffran, B.; Stinson, T.J.; Nelson, W.; Bennett, C.L. Evaluation of conflict of interest in economic analyses of new drugs used in oncology. JAMA 1999, 282, 1453–1457. [Google Scholar] [CrossRef] [Green Version]
- Garattini, L.; Koleva, D.; Casadei, G. Modeling in pharmacoeconomic studies: Funding sources and outcomes. Int. J. Technol. Assess. Health Care 2010, 26, 330–333. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Country | Model Type | Type of Vaccine(s) | Time Horizon | Inclusion of Herd Effect | Outcome Measure(s) | Sensitivity Analysis |
|---|---|---|---|---|---|---|---|
| Lee et al., (2009) [29] | Hong Kong | Decision tree | PCV-7 | 10 year | Yes | LYs | One-way |
| Sohn et al., (2010) [46] | Korea | Decision tree | PCV-7 | 5 year | No | LYs | One-way and PSA |
| Wu et al., (2012) [43] | Taiwan | Age-structured transmission dynamic model | PCV-13 | 10 year | Yes | LYs | One-way and PSA |
| Hoshi et al., (2012) [39] | Japan | Markov | PCV-7 | 5 year | Yes | LYs and QALYs | One-way |
| Lee et al., (2013) [28] | Hong Kong | Decision tree | PCV-10 and PCV-13 | 10 year | Yes | LYs and QALYs | One-way, two-way, and PSA |
| Kulpeng et al., (2013) [47] | Thailand | Markov | PCV-10 and PCV-13 | Lifetime | Yes | QALYs | One-way and PSA |
| Wu et al., (2013) [27] | Taiwan | Decision tree | PCV-7 | 10 year | Yes | LYs | One-way |
| Hoshi et al., (2013) [38] | Japan | Markov | PCV-13 | 5 year | Yes | LYs and QALYs | One-way and PSA |
| Shiragami et al., (2014) [20] | Japan | Markov | PCV-10 and PCV-13 | 5 year | Yes | QALYs | One-way and PSA |
| Zhang et al., (2014) [36] | The Philippines | Markov | PCV-10 and PCV-13 | Lifetime | Yes | QALYs | One-way and PSA |
| Hu et al., (2014) [30] | China | Decision tree | PCV-7 | 1 year | Yes | LYs, QALYs, pneumonia-related Illness | One-way |
| Aljunid et al., (2014) [34] | Malaysia | Markov | PCV-10 and PCV-13 | Lifetime | Yes | LYs and QALYs | One way |
| Che et al., (2014) [32] | China | Decision-tree | PCV-7 | 5 year | Yes | QALYs | One-way and PSA |
| Haasis et al., (2015) [31] | The Phillipines | Markov | PCV-10 and PCV-14 | Lifetime (CUA) and 5 year (BIA) | Yes | QALYs | One way |
| Caldwell et al., (2015) [33] | China | Decision tree | PCV-7 | 1 year | Yes | LYs and QALYs | One-way |
| Maurer et al., (2016) [26] | China | Markov | PCV-7, PCV-10, and PCV-13 | Lifetime | Yes | QALYs | One way, two-way, and PSA |
| Mo et al., (2016) [48] | China | Markov | PCV 7, PCV 13, PPV 23 | Lifetime | Yes | QALYs, mortality | One-way and PSA |
| Wu et al., (2016) [42] | Malaysia and Hong Kong | Markov | PCV-10 and PCV-13 | 10 year | Yes | LYs and QALYs | One-way and PSA |
| Sundaram et al., (2017) [45] | Mongolia | Age-stratified decision tree | PCV-13 | 30 year (CEA) 10 year (BIA) | Yes | DALYs | One-way |
| Wang et al., (2017) [44] | Malaysia | Markov | PCV-10 and PCV-13 | 10 year | No | QALYs | One-way and PSA |
| Zhang et al., (2018) [25] | Korea | Markov | PCV-10 and PCV-13 | 10 year | No | QALYs | One-way and PSA |
| Dorji et al., (2018) [37] | Bhutan | Markov | PCV-10 and PCV-13 | 1 year | Yes | QALYs, pneumococcal-related Illness, mortality | One-way and PSA |
| Zhou et al., (2018) [35] | China | Markov | PCV-13 | Lifetime | Yes | QALYs | One-way and PSA |
| Shen et al., (2018) [41] | China | Decision tree | PCV-13 | 1 year | Yes | LYs, QALYs, mortality | One-way |
| Khrisnamoorty et al., (2019) [40] | India | Decision tree | PCV-13 | 10 year | No | DALYs, pneumococcal-related Illness, mortality | PSA |
| Reference | Perspective | Discount Rates | Costs Data | Willingness to Pay Threshold (International $ 2018) | Main Findings | Most Influential Parameter in Sensitivity Analysis | |||
|---|---|---|---|---|---|---|---|---|---|
| Cost | Outcome | Direct Costs | Indirect Costs | ||||||
| Medical | Non-Medical | ||||||||
| [29] | Payer and Societal | 5% | 5% | Direct acute cost per infection, and long-term cost per disability | Transportation cost for outpatient visits and hospital stays | Productivity loss of caregiver | 1–3 times GDP per capita | PCV-7 would be cost saving compared to no vaccination | Vaccine cost, herd effect, and incidence of pneumonia |
| [46] | Societal | 5% | 5% | Treatment of pneumococcal diseases and clinical sequelae (e.g., prescribed medications, medical procedures, and diagnostic tests) | Transportation cost for outpatient visits and hospital stays | Productivity loss of caregiver owing to pneumococcal disease morbidity | ICER below 360,000 | PCV-7 would not be cost-effective compared to no vaccination | Annual incidence of pneumonia, AOM, and bacteremia |
| [43] | Payer and Societal | 3% | 3% | Hospitalization, health-care professional consultation, ICU admissions, medications, and diagnostic tests for IPD, pneumonia, AOM | NR | Productivity loss of patient due to non-fatal pneumococcal diseases and pneumococcal death and caregiver time | 1–3 times GDP per capita | PCV-13 would be cost-effective | Vaccine price, recovery rate, incidence of pneumonia and the vaccine-immunity period |
| [39] | Societal | 3% | 3% | Treatment of pneumococcal diseases and meningitis sequelae | NR | Productivity loss of caregiver for vaccine uptake and medical treatment, and for taking care of a child with sequelae | 1–3 times GDP per capita | PCV-7 would be cost-effective | Vaccine effectiveness in reducing AOM, care-giver’s productivity loss |
| [28] | Payer | 5% | 5% | Pneumococcal-related disease cost, hospitalization, outpatient cost of pneumonia, and AOM (e.g., GP and complications) | NA | NA | 1 time GDP per capita | PCV-10 would be cost-saving compared to PCV-13 | Cost for inpatient myringotomy and changes in AOM-Related parameters |
| [47] | Societal | 3% | 3% | Treatment cost per episode of meningitis, hospitalization due to pneumonia-related illness | Transportation and accommodation | Productivity loss of caregiver | 1 time GDP per capita | PCV10 and PCV13 would not be cost-effective | Discount rate, change in duration of vaccine protection, and the incidence of pneumonia |
| [27] | Payer and Societal | 3% | 3% | Treatment of pneumococcal-related disease (i.e., hospitalization, healthcare professional consultation fees, intensive care admissions, medications, and diagnostic tests) | NR | Productivity loss of patient due to non-fatal pneumococcal diseases and pneumococcal death and caregiver time | 1–3 times GDP per capita | PCV-7 would be cost effective compared to no vaccination | Vaccine price, herd effect on pneumonia, and mortality rate of pneumonia |
| [38] | Societal | 3% | 3% | Treatment of pneumococcal diseases and meningitis sequelae | NR | Productivity loss of caregiver for vaccine uptake and medical treatment, and for taking care of a child with sequelae | 1–3 times GDP per capita JPY | PCV-13 would be a socially acceptable option compared to current PCV-7 vaccination if PCV-13 had additional protection against AOM compared to PCV-7 and cost PCV-13 per dose is 1.7 times less than that of PCV-7 | Vaccine effectiveness in reducing AOM |
| [20] | Health care provider and societal | 3% | 3% | Treatment cost, admission days and outpatient visits | NR | Wages lost due to acute episodes | ICER below 45.000 | PCV-10 would be cost saving compared to PCV-13 | PCV-10 efficacy against AOM, percentage reduction in myringotomy, and changes in other AOM-related parameters |
| [36] | Government | 5% | 5% | Hospitalization, inpatient/outpatient diagnostic tests, medication/vaccine costs, and health care professionals’ fees | NA | NA | 1–3 times GDP per capita | PCV-10 would be cost effective compared with no vaccination and cost-saving compared to PCV-13 | Percent reduction in CAP hospitalization, hospitalization for CAP, and vaccine efficacy |
| [30] | Payer | 5% | 5% | Hospitalization and physician consultation fees, diagnostic tests, and medication expenses for pneumococcal-related diseases | NA | NA | Max 3 times GDP per capita | PCV-7 would be cost-effective | Percent reduction in disease incidence among the unvaccinated population, vaccine price, vaccine coverage level |
| [34] | Government | 5% | 5% | Outpatient treatment and hospitalization cost | NA | NA | 1 time GDP per capita | PCV-10 would be cost effective compared to no vaccination and cost-saving compared to PCV-13 | GP visits for AOM and PCV-10 efficacy |
| [32] | Societal | 3% | 3% | Medical cost of meningitis, bacteremia, pneumonia, AOM, long-term cost of sequelae | NR | Productivity loss of caregiver | 1 time GDP per capita | PCV-7 would not be cost effective | Cost of PCV-7 per dose, the reduction of IPD for herd immunity in adults and annual incidence of IPD in children |
| [31] | Health system | 3,5% | 3,5% | Cost per episode of meningitis, bacteremia and sepsis, all-cause pneumonia hospitalization, all-cause pneumonia outpatients | NA | NA | 1 time GDP per capita | CUA: both PCV-10 and PCV-13 would be cost-effective compared to vaccination. PCV13 achieved better value for money compared to PCV10. BIA: cost of national PCV immunization program is expected to be higher than current healthcare budget. | Vaccine cost, exclusion of herd effect, and vaccine efficacy |
| [33] | Payer | 3% | 3% | Hospitalization, physician consultation, diagnostic tests, nursing and medication expenses for all-cause pneumonia and pneumococcal-related illness | NA | NA | 1–3 times GDP per capita | PCV7 would be cost-effective during a typical influenza season and cost-saving during an influenza pandemic | Variation in the herd effect and vaccine coverage |
| [26] | Payer | 3% | 3% | Treatment of pneumonia-related illness and complications | _ | NR | 1–3 times GDP per capita | PCV-13 would be cost-saving compared to PCV-7 and PCV-10 | Utility of AOM, the cost of PCV-13, incidence of pneumonia and AOM |
| [48] | Societal | 3% | 3% | Treatment of pneumonia-related illness | NR | NR | 1–3 times GDP per capita | PPV-23 would be the most cost-effective vaccine, followed by PCV-13 | Efficacy of PPV-23 against pneumonia, cost of PCV-13, and cost of PCV-7 |
| [42] | Payer and Societal | 3% | 3% | Treatment of pneumococcal-related illness and lifetime cost of meningitis sequelae | NR | Productivity loss | 1–3 times GDP per capita | PCV-13 would be cost saving compared to PCV-10, under both payer and societal perspective in both countries | In Malaysia: PCV-10 and PCV-13 coverage In Hongkong: direct cost of treating hospitalized pneumonia and case-fatality ratio (CFR) of hospitalized pneumonia In Malaysia: PCV-10 and PCV-13 coverage In Hongkong: direct cost of treating hospitalized pneumonia and CFR of hospitalized pneumonia |
| [45] | Health system and societal | 3% | 3% | Hospitalization and health center consultation costs | NR | Productivity loss | 1 time GDP per capita | CEA: PCV-13 would be cost-effective compared to no vaccination. BIA: PCV-13 would reduce direct cost to the healthcare budget and societal cost | Vaccine serotype coverage, disease burden, vaccine efficacy |
| [44] | Government | 3% | 3% | Hospitalization due to pneumonia-related illness and complications and GP consultation | NA | NA | 1–3 times GDP per capita | PCV-10 would be cost effective compared to no vaccination and cost-saving compared to PCV-13 | PCV-10 efficacy against AOM and disutility weight for AOM |
| [25] | Government | 5% | 5% | Hospitalization and outpatient due to pneumonia-related illness and GP consultation | NA | NA | 1 time GDP per capita | PCV-10 would be cost-saving compared to PCV-13 | Disutility for outpatient AOM, PCV-13% reduction in myringotomy, and GP visits for AOM. |
| [37] | Government | 3% | 3% | Treatment of pneumococcal-related illness, hospitalization due to pneumonia, and treatment of meningitis sequelae | NA | NA | 1 time GDP per capita | Both PCV-10 and PCV-13 are cost-effective, with PCV-13 yields better health outcomes in terms of episodes of pneumococcal disease, number of deaths, and would incur a lower five-year budget. | Variation in coverage, duration of vaccine protection, excluding indirect vaccine effects (herd protection), and discount rate |
| [35] | Health system and societal | 5% | 5% | Treatment of pneumococcal-related illness and lifetime cost of meningitis sequelae | NR | Productivity lost | 1 time GDP per capita | PCV-13 would be cost effective | CAP-related parameters (annual incidence of CAP, case-fatality of hospitalized CAP and S. pneumoniae isolation rate for pneumonia) and cost of PCV-13 |
| [41] | Payer | 3% | 3% | Treatment of pneumococcal-related illness, all-cause otitis media, and hospitalization due to pneumonia | NA | NA | 1–3 times GDP per capita | PCV-13 would be cost-effective at a threshold of 1–3 GDP per capita when considering direct vaccine effects only or indirect effects for rare invasive disease cases only. When indirect effects for the more frequently occurring inpatient pneumonia was included, the results are highly cost-effective at 1 times GDP per capita | incidence rates of inpatient pneumonia |
| [40] | Government | 3% | 3% | Hospitalization and outpatient due to pneumococcal-related illness | NA | NA | 1 time GDP per capita | PCV-13 would be cost effective | Vaccine cost |
| Author, Year/Country | PCV7 | PCV10 | PCV13 | PPV23 | Administration Cost |
|---|---|---|---|---|---|
| Lee, 2009/Hongkong | 112.52 | − | − | − | 2.72 |
| Sohn, 2010/Korea | 94.18 | − | − | − | − |
| Wu, 2012/Taiwan | − | − | 107.01 | − | 5.49 |
| Hoshi, 2012/Japan | 92.09 | − | − | − | − |
| Lee, 2013/Hong Kong | − | 52.64 | 52.64 | − | − |
| Kulpeng, 2013/Thailand | − | 127.56 | 170.97 | − | (6.38–8.55) |
| Wu, 2013/Taiwan | − | 91.55 | − | − | 5.48 |
| Hoshi, 2013/Japan | 92.34 | − | 120.04 | − | − |
| Shiragami, 2014/Japan | − | 69.67 | 69.67 | − | 37.74 |
| Zhang, 2014/The Philippines | − | 48.51 | 48.51 | − | − |
| Hu, 2014/China | 253.02 | − | − | − | 2.94 |
| Aljunid, 2014/Malaysia | − | 173.04 | 173.04 | − | − |
| Che, 2014/China | 146.25 | − | − | − | 2.14 |
| Haasis, 2015/The Philippines | − | 36.73 | 41.20 | − | − |
| Caldwell, 2015/China | 253.02 | − | − | − | 2.94 |
| Maurer, 2016/China | 157.37 | 157.37 | 157.37 | − | 2.16 |
| Mo, 2016/China | 147.14 | 147.14 | − | 32.51 | 1.71 |
| Wu, 2016/Malaysia-Hongkong | − | 59.29 (Malaysia) 26.95 (Hongkong) | 59.29 (Malaysia) 44.19 (Hongkong) | − | − |
| Sundaram, 2017/Mongolia | − | − | 3.56 | − | 0.15 |
| Wang, 2017/Malaysia | − | 36.92 | 36.92 | − | − |
| Zhang, 2018/Korea | − | 57.16 | 57.16 | − | 18.53 |
| Dorji, 2018/Bhutan | − | 3.19 | 3.71 | − | 3.91 |
| Zhou, 2018/China | − | − | ~61.45 | − | − |
| Shen, 2018/China | − | − | 172.44 | − | − |
| Krishnamoorthy, 2019/India | − | − | 3.45–71.14 | − | 0.03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakiyah, N.; Insani, W.N.; Suwantika, A.A.; van der Schans, J.; Postma, M.J. Pneumococcal Vaccination for Children in Asian Countries: A Systematic Review of Economic Evaluation Studies. Vaccines 2020, 8, 426. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8030426
Zakiyah N, Insani WN, Suwantika AA, van der Schans J, Postma MJ. Pneumococcal Vaccination for Children in Asian Countries: A Systematic Review of Economic Evaluation Studies. Vaccines. 2020; 8(3):426. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8030426
Chicago/Turabian StyleZakiyah, Neily, Widya N. Insani, Auliya A. Suwantika, Jurjen van der Schans, and Maarten J. Postma. 2020. "Pneumococcal Vaccination for Children in Asian Countries: A Systematic Review of Economic Evaluation Studies" Vaccines 8, no. 3: 426. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8030426