Behavioral Differences in the Preference for Hepatitis B Virus Vaccination: A Discrete Choice Experiment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Participants
2.2. Study Design
2.3. Behavioral Factors
2.4. Control Variables
2.5. Statistical Analyses
3. Results
3.1. Respondent Characteristics
3.2. General Preference for HBV Vaccine
3.3. Behavioral Factors’ Differences in Preference for Vaccine
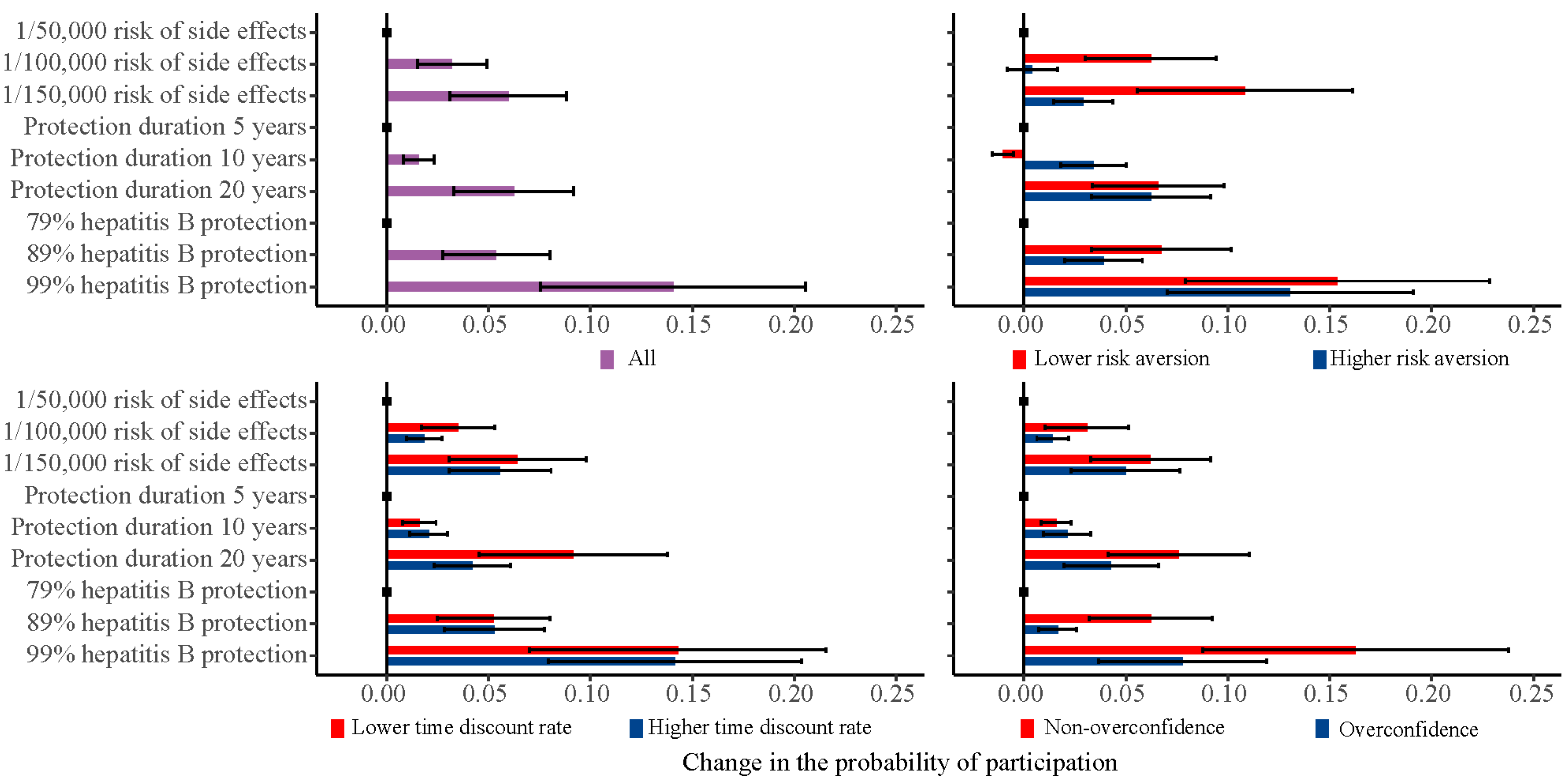
3.4. Change in the Probability of Participation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. World Immunization Week 2012. Available online: https://www.who.int/immunization/newsroom/events/immunization_week/2012/further_information/en/ (accessed on 11 October 2019).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Betsch, C.; Böhm, R.; Chapman, G.B. Using behavioral insights to increase vaccination policy effectiveness. Policy Insights Behav. Brain Sci. 2015, 2, 61–73. [Google Scholar] [CrossRef]
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association between vaccine refusal and vaccine-preventable diseases in the United States: A Review of Measles and Pertussis. JAMA 2016, 315, 1149. [Google Scholar] [CrossRef] [Green Version]
- Lo, N.C.; Hotez, P.J. Public health and economic consequences of vaccine hesitancy for Measles in the United States. JAMA Pediatr. 2017, 171, 887. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Measles Cases and Outbreaks. Available online: https://www.cdc.gov/measles/cases-outbreaks.html (accessed on 11 October 2019).
- Cappelen, A.; Mæstad, O.; Tungodden, B. Demand for Childhood Vaccination—Insights from Behavioral Economics. J. Dev. Stud. 2010, 37, 349–364. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Hendrix, K.S.; Finnell, S.M.E.; Zimet, G.D.; Sturm, L.A.; Lane, K.A.; Downs, S.M. Vaccine message framing and parents’ intent to immunize their infants for MMR. Pediatrics 2014, 134, e675–e683. [Google Scholar] [CrossRef] [Green Version]
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing vaccination: Putting psychological science into action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahrabani, S.; Gafni, A.; Ben-Zion, U. Low flu shot rates puzzle-some plausible behavioral explanations. Am. Econ. 2008, 52, 66–72. [Google Scholar] [CrossRef]
- Chapman, G.B.; Coups, E.J. Time preferences and preventive health behavior: Acceptance of the Influenza Vaccine. Med. Decis. Mak. 1999, 19, 307–314. [Google Scholar] [CrossRef]
- Chapman, G.B. Short-term cost for long-term benefit: Time preference and cancer control. Health Psychol. 2005, 24, S41–S48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matjasko, J.L.; Cawley, J.H.; Baker-Goering, M.M.; Yokum, D.V. Applying behavioral economics to public health policy. Am. J. Prev. Med. 2016, 50, S13–S19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsui, Y.; Benzion, U.; Shahrabani, S.; Din, G.Y. A policy to promote influenza vaccination: A behavioral economic approach. Health Policy 2010, 97, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, Y.; Benzion, U.; Shahrabani, S. Economic and behavioral factors in an individual’s decision to take the influenza vaccination in Japan. J. Soc. Econ. 2012, 41, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Buttenheim, A.M.; Fiks, A.G.; Burson, R.C., II; Wang, E.; Coffin, S.E.; Metlay, J.P.; Feemster, K.A. A behavioral economics intervention to increase pertussis vaccination among infant caregivers: A randomized feasibility trial. Vaccine 2016, 34, 839–845. [Google Scholar] [CrossRef]
- Böhm, R.; Meier, N.W.; Groß, M.; Korn, L.; Betsch, C. The willingness to vaccinate increases when vaccination protects others who have low responsibility for not being vaccinated. J. Behav. Med. 2019, 42, 381–391. [Google Scholar] [CrossRef]
- Russo, E.J.; Schoemaker, P.J.H. Managing overconfidence. Sloan Manag. Rev. 1992, 33, 7–17. [Google Scholar]
- Phillips, K.A.; Van, B.S.; Marshall, D.; Walsh, J.; Thabane, L. A review of studies examining stated preferences for cancer screening. Prev. Chronic Dis. 2006, 3, A75. [Google Scholar]
- World Health Organization. WHO Technical Consultation on a Comprehensive National Hepatitis Programme in China with a Focus on Viral Hepatitis B and C Treatment, Beijing, China, 21 February 2014: Meeting Report; WHO Regional Office for the Western Pacific: Manila, Philippines, 2014; p. 31. [Google Scholar]
- National Health Commission. China Health Yearbook; China Union Medical University Press: Beijing, China, 2018. [Google Scholar]
- Hadler, S.C.; Fuqiang, C.; Averhoff, F.; Taylor, T.; Fuzhen, W.; Li, L.; Xiaofeng, L.; Weizhong, Y. The impact of hepatitis B vaccine in China and in the China GAVI Project. Vaccine 2013, 31, J66–J72. [Google Scholar] [CrossRef]
- Zhu, D.; Wang, J.; Wangen, K.R. Hepatitis B vaccination coverage rates among adults in rural China: Are economic barriers relevant? Vaccine 2014, 32, 6705–6710. [Google Scholar] [CrossRef]
- Guo, N.; Zhang, G.; Zhu, D.; Wang, J.; Shi, L. The effects of convenience and quality on the demand for vaccination: Results from a discrete choice experiment. Vaccine 2017, 35, 2848–2854. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Chen, W. Assessment of total economic burden of chronic Hepatitis B (CHB)-related diseases in Beijing and Guangzhou, China. Value Health 2009, 12, S89–S92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Xu, A.; Wang, J.; Zhang, L.; Song, L.; Li, R.; Zhang, S.; Zhuang, G.; Lu, M. Direct economic burden of hepatitis B virus related diseases: Evidence from Shandong, China. BMC Health Serv. Res. 2013, 13, 37. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Chao, J.; Zhu, L.; Song, L.; Li, X.; Liu, P. Direct economic burden and influencing factors in patients with Hepatitis B virus related diseases in Jiangsu, China. Asia Pac. J. Public Health 2015, 27, 41S–48S. [Google Scholar] [CrossRef]
- Ryan, M. Discrete choice experiments in health care. BMJ 2004, 328, 360–361. [Google Scholar] [CrossRef]
- Ryan, M.; Bate, A.; Eastmond, C.J.; Ludbrook, A. Use of discrete choice experiments to elicit preferences. Qual. Saf. Health Care 2001, 10, i55–i60. [Google Scholar] [CrossRef]
- Liao, Q.; Lam, W.W.T.; Wong, C.K.H.; Lam, C.; Chen, J.; Fielding, R. The relative effects of determinants on Chinese adults’ decision for influenza vaccination choice: What is the effect of priming? Vaccine 2019, 37, 4124–4132. [Google Scholar] [CrossRef]
- De Bekker-Grob, E.W.; Hofman, R.; Donkers, B.; van Ballegooijen, M.; Helmerhorst, T.J.M.; Raat, H.; Korfage, I.J. Girls’ preferences for HPV vaccination: A discrete choice experiment. Vaccine 2010, 28, 6692–6697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Bekker-Grob, E.W.; Donkers, B.; Jonker, M.F.; Stolk, E.A. Sample size requirements for discrete-choice experiments in healthcare: A practical guide. Patient Patient Cent. Outcomes Res. 2015, 8, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Hole, A.R.; Kolstad, J.R. Mixed logit estimation of willingness to pay distributions: A comparison of models in preference and WTP space using data from a health-related choice experiment. Empir. Econ. 2012, 42, 445–469. [Google Scholar] [CrossRef]
- Janssen, E.M.; Hauber, A.B.; Bridges, J.F.P. Conducting a discrete-choice experiment study following recommendations for good research practices: An application for eliciting patient preferences for diabetes treatments. Value Health 2018, 21, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, D.; Shi, X.; Nicholas, S.; Ye, X.; Chen, S.; He, P. Preferences for hearing aid attributes among people with moderate or greater hearing loss in rural China: A discrete choice experiment. Patient Prefer Adher. 2020, 14, 643–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.S.; Johnson, F.R.; Poulos, C.; Messonnier, M.L. Mothers’ preferences and willingness to pay for vaccinating daughters against human papillomavirus. Vaccine 2010, 28, 1702–1708. [Google Scholar] [CrossRef]
- De Bekker-Grob, E.W.; Veldwijk, J.; Jonker, M.; Donkers, B.; Huisman, J.; Buis, S.; Swait, J.; Lancsar, E.; Witteman, C.L.M.; Bonsel, G.; et al. The impact of vaccination and patient characteristics on influenza vaccination uptake of elderly people: A discrete choice experiment. Vaccine 2018, 36, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- Veldwijk, J.; Lambooij, M.S.; Bruijning-Verhagen, P.C.J.; Smit, H.A.; Wit, G.A.D. Parental preferences for rotavirus vaccination in young children: A discrete choice experiment. Vaccine 2014, 32, 6277–6283. [Google Scholar] [CrossRef]
- Svenson, O. Are we all less risky and more skillful than our fellow drivers? Acta Psychol. 1981, 47, 143–148. [Google Scholar] [CrossRef]
- Dunning, D. Essays in social psychology. In Self-Insight: Roadblocks and Detours on the Path to Knowing Thyself; Psychology Press: New York, NY, USA, 2005; ISBN 978-1-84169-074-2. [Google Scholar]
- Larson, E.; Vail, D.; Mbaruku, G.M.; Kimweri, A.; Freedman, L.P.; Kruk, M.E. Moving toward patient-centered care in Africa: A discrete choice experiment of preferences for delivery care among 3,003 Tanzanian women. PLoS ONE 2015, 10, e0135621. [Google Scholar] [CrossRef] [Green Version]
- Böhm, R.; Betsch, C.; Korn, L. Selfish-rational non-vaccination: Experimental evidence from an interactive vaccination game. J. Econ. Behav. Organ. 2016, 131, 183–195. [Google Scholar] [CrossRef]


{kind=link}
| Attributes | Levels |
|---|---|
| Risk of serious side-effects | 1/50,000; 1/100,000; 1/150,000 |
| Protection duration (years) | 5; 10; 20 |
| Protection rate against HBV (%) | 79; 89; 99 |
| Out-of-pocket cost (RMB) | 0; 30; 60; 90 |
| Characteristics | All Sample (N = 353) |
|---|---|
| Socioeconomic factors | |
| Sex | |
| Female | 164 (46.5) |
| Male | 189 (53.5) |
| Age group | |
| Under 40 | 213 (60.3) |
| 41+ | 140 (39.7) |
| Education level | |
| Low education | 131 (37.1) |
| High education | 222 (62.9) |
| RMB income group (monthly) | |
| ≤2000 | 145 (41.1) |
| 2001+ | 208 (58.9) |
| Health status | |
| Poor | 153 (43.3) |
| Good | 200 (56.7) |
| Perceived risk of HBV infection | |
| Low | 185 (52.4) |
| High | 168 (47.6) |
| Perceived severity of HBV | |
| Low | 126 (35.7) |
| Moderate | 92 (26.1) |
| High | 135 (38.2) |
| Behavioral factors | |
| Risk aversion | |
| Higher | 193 (53.82) |
| Lower | 163 (46.18) |
| Time discount rate | |
| Higher | 171 (48.44) |
| Lower | 182 (51.56) |
| Overconfidence | |
| Yes | 98 (27.76) |
| No | 255 (72.24) |
| Model 1 | Model 2 | |
|---|---|---|
| Constant | 7.558(0.830) *** | 6.990(1.467) *** |
| Attribute | ||
| Out-of-pocket cost | −0.010(0.003) *** | −0.010(0.003) *** |
| Risk of side-effects (ref. = 1/50,000) | ||
| 1/100,000 | 0.215(0.096) * | 0.226(0.097) * |
| 1/150,000 | 0.418(0.097) *** | 0.415(0.092) *** |
| Protection duration (ref. = 5 years) | ||
| 10 years | 0.109(0.096) | 0.110(0.095) |
| 20 years | 0.456(0.095) *** | 0.439(0.092) *** |
| Protection rate (ref. = 79%) | ||
| 89% | 0.363(0.096) *** | 0.365(0.094) *** |
| 99% | 0.993(0.107) *** | 0.977(0.103) *** |
| Socioeconomic factors | ||
| Neither × Male | 0.311(0.668) | |
| Neither × Age 40+ | −3.079(0.799) *** | |
| Neither × High education | 0.290(0.822) | |
| Neither × Income 2000 RMB+ | 0.344(0.892) | |
| Neither × Good health status | −0.235(0.511) | |
| Neither × High risk of infection | −1.070(0.580) | |
| Neither × Perceived moderate severity | −0.229(0.695) | |
| Neither × Perceived high severity | −1.738(0.656) ** | |
| Behavioral factors | ||
| Neither × Lower risk aversion | 2.049(0.497) *** | |
| Neither × Lower time discount rate | −1.185(0.594) * | |
| Neither × Non-overconfidence degree | −1.166(0.558) * |
| Model 3 Lower Risk Aversion | Model 4 Lower Time Discount Rate | Model 5 Non-Overconfidence | |
|---|---|---|---|
| Constant | 7.870 (0.940) *** | 6.976 (0.915) *** | 6.597 (0.684) *** |
| Attribute | |||
| Out-of-pocket cost | −0.011 (0.004) ** | −0.010 (0.004) ** | −0.024 (0.006) *** |
| Risk of side-effects (ref. = 1/50,000) | |||
| 1/100,000 | 0.030 (0.139) | 0.114 (0.118) | 0.098 (0.168) |
| 1/150,000 | 0.202 (0.127) | 0.341 (0.118) ** | 0.347 (0.172) * |
| Protection duration (ref. = 5 years) | |||
| 10 years | 0.240 (0.129) | 0.127 (0.120) | 0.147 (0.174) |
| 20 years | 0.443 (0.126) *** | 0.258 (0.116) * | 0.298 (0.168) |
| Protection rate (ref. = 79%) | |||
| 89% | 0.267 (0.130) * | 0.315 (0.121) ** | 0.114 (0.177) |
| 99% | 0.916 (0.142) *** | 0.859 (0.133) *** | 0.547 (0.184) ** |
| Interaction terms | |||
| Out-of-pocket cost × covariate | −0.001 (0.005) | 0.000 (0.005) | 0.018 (0.006) ** |
| Risk of side-effects (ref. = 1/50,000) | |||
| 1/100,000 × covariate | 0.433 (0.208) * | 0.143 (0.182) | 0.136 (0.209) |
| 1/150,000 × covariate | 0.598 (0.198) ** | 0.131 (0.192) | 0.121 (0.211) |
| Protection duration (ref. = 5 years) | |||
| 10 years × covariate | −0.319 (0.198) | −0.009 (0.181) | −0.029 (0.211) |
| 20 years × covariate | 0.054 (0.191) | 0.413 (0.176) * | 0.283 (0.204) |
| Protection rate (ref. = 79%) | |||
| 89% × covariate | 0.220 (0.197) | 0.059 (0.181) | 0.343 (0.213) |
| 99% × covariate | 0.218 (0.204) | 0.177 (0.192) | 0.669 (0.227) ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, N.; Wang, J.; Nicholas, S.; Maitland, E.; Zhu, D. Behavioral Differences in the Preference for Hepatitis B Virus Vaccination: A Discrete Choice Experiment. Vaccines 2020, 8, 527. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8030527
Guo N, Wang J, Nicholas S, Maitland E, Zhu D. Behavioral Differences in the Preference for Hepatitis B Virus Vaccination: A Discrete Choice Experiment. Vaccines. 2020; 8(3):527. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8030527
Chicago/Turabian StyleGuo, Na, Jian Wang, Stephen Nicholas, Elizabeth Maitland, and Dawei Zhu. 2020. "Behavioral Differences in the Preference for Hepatitis B Virus Vaccination: A Discrete Choice Experiment" Vaccines 8, no. 3: 527. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines8030527