1. Introduction
Maternal immunization has been proven safe and effective in protecting the mother and/or the offspring from the complications of pertussis and influenza [
1]. Passive immunity provided through maternal Tdap (Tetanus, diphtheria, acellular pertussis) vaccination is the main measure that protects infants from pertussis during their first months of life, when they are not able to obtain an optimal vaccine response and are at risk of severe and potentially fatal disease [
2]. Influenza vaccination, in addition to eliciting antibody response in the newborn during the first weeks of life, protects the mother and the pregnancy from influenza-related complications [
1] (maternal pneumonia, preterm birth, low birthweight). The reviews of several years of surveillance revealed no data that could raise concerns about Tdap and influenza vaccines, either for the fetus or the mother [
3,
4]. Despite all such evidence, the vaccination rate in pregnant women is globally disappointingly low [
5]. In Italy, the National Immunization Plan includes as part of the free routine care of pregnancy both the Tdap vaccination during the third trimester of each pregnancy, in addition to the flu vaccination for all pregnant women during the epidemic season [
6,
7,
8,
9]. Despite this, national vaccination coverage among Italian pregnant women is still negligible [
10,
11,
12,
13] and even lower than that reported in English-speaking countries. The COVID-19 pandemic has posed a major challenge for healthcare services [
14] and has shifted the attention of public opinion on the dangers of communicable diseases, therefore renewing interest and confidence in preventive measures, especially vaccines’ immunization. The offer of COVID-19 vaccines during pregnancy (and/or lactation) is currently supported by the Center for Disease Control [
15], the American College of Obstetricians and Gynecologists [
16], the Society for Maternal–Fetal Medicine [
17] and the Royal College Of Obstetricians and Gynaecologists [
18]. This guidance was endorsed by the Società Italiana di Ginecologia ed Ostetricia [
19,
20]. However, COVID-19 vaccine uptake in pregnant women may be a critical challenge, due to both maternal hesitancy and evolving information offered by healthcare staff [
21]. The aim of this survey was to investigate vaccine uptake or hesitancy and their determinants in a group of pregnant women that experienced their first half of pregnancy (pre-COVID pandemic) during the 2019–2020 influenza seasonal epidemic and their third trimester (recommended trimester to perform Tdap immunization) during the novel coronavirus spread. They represent a unique model to investigate if the SARS-CoV-2 outbreak might have changed attitudes towards vaccination in the same pregnant patients. We consider these data useful to maximize SARS-CoV-2 vaccination uptake in the pregnant population.
3. Results
During the inclusion period, 520 deliveries were recorded. A total of 195 women (37.5%) completed and returned the questionnaire and were therefore included in the analysis.
The sociodemographic characteristics of the women included are shown in
Table 1. The majority (70.2%) of the women were Italian; however, almost one third of the participants were of a different ethnicity, mainly Chinese (11.8%). More than half (54.3%) of the women were multiparous; 80.5% of them had a medium–high level of education, and 66.7% were in employment.
Eighty-four (43%) women had a pre-existing comorbidity or experienced a pregnancy complication. Almost half (42%) underwent at least one prenatal visit every month. A total of 152 (80%) women received prenatal care at a public hospital outpatient clinic/counselling center, mainly (169 cases, 87%) by a gynecologist–obstetrician. A total of 186 (95.4%) women declared they planned to have their newborns vaccinated following the national schedules for immunization in childhood, only three patients stated they would not adhere to this schedule and only six stated that they needed to further consider this choice (total nine patients—4.6%). When asked about the reliability of their healthcare providers, the majority of women answered they trusted the information received from their gynecologist/midwife (chosen 173 times).
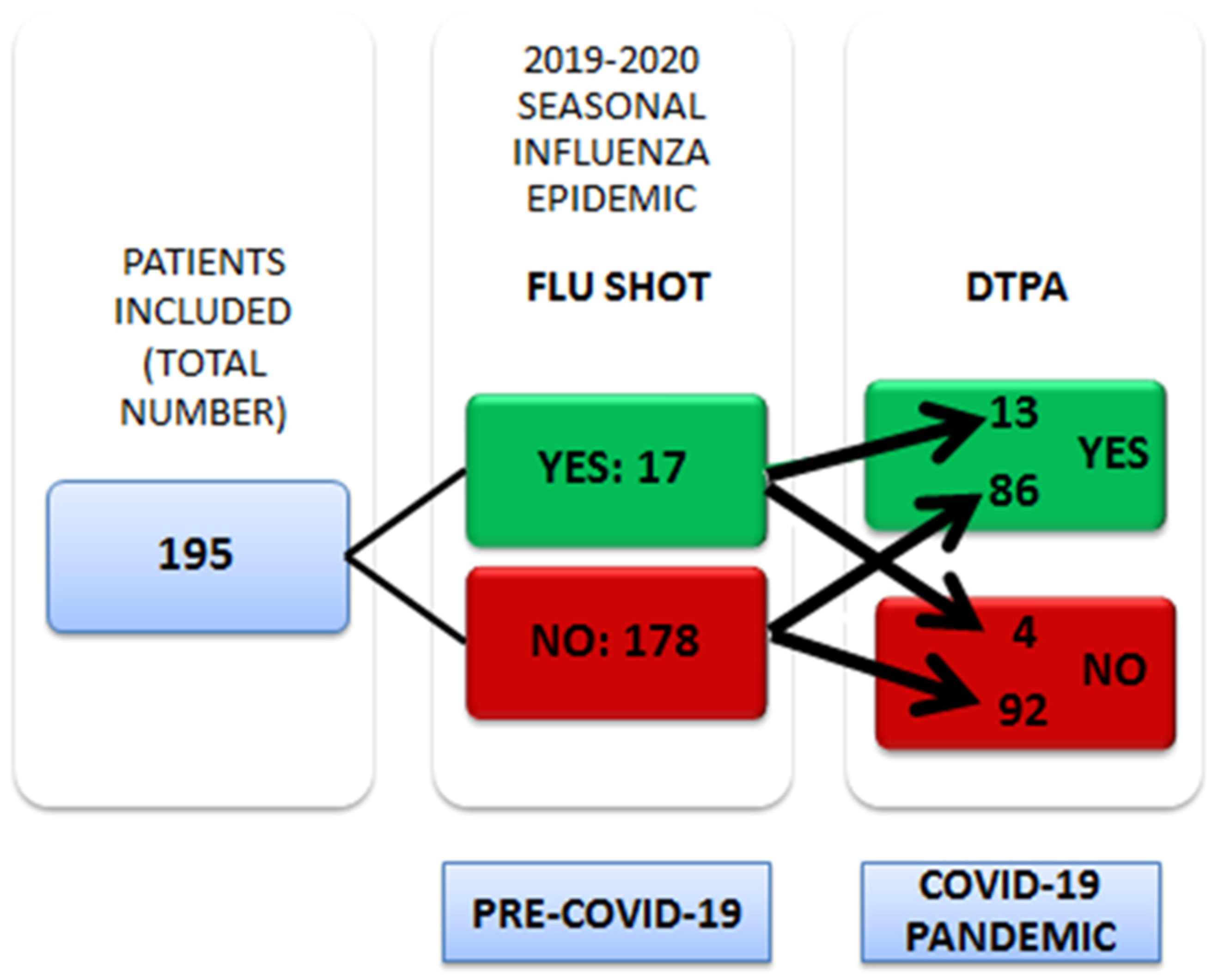
With regard to flu immunization, only 17 patients (8.7%) reported they had been vaccinated—during the pre-pandemic period.
As far as pertussis immunization is concerned, more than half of the same women questioned (99 cases, 50.8%) reported they had been vaccinated—during the COVID-19 pandemic. Only 13 patients received both vaccines during pregnancy. The trend of the uptake of immunization in pregnancy before and during the COVID-19 pandemic in our sample is shown in
Figure 1.
Of the 17 pregnant women who accepted the flu vaccine, four subsequently did not perform the Tdap immunization because they had not received a recommendation from healthcare providers (4/4). Out of the 13 women who received the flu vaccine first and the Tdap later, 11 were recommended the pertussis immunization and two were aware that the vaccine protects their newborn from pertussis complications.
Of the 99 patients who performed the Tdap vaccine, 13 had previously received the flu vaccine and 86 had not. Out of the 86 pregnant women who accepted the pertussis vaccination after missing the flu vaccine, 69 chose to schedule this vaccine because they were recommended it, and 13 because they wanted to protect their offspring from pertussis complications. Out of the 96 women that have not received the Tdap vaccine, 30 (31.2%) stated that lockdown measures and fear of contracting COVID-19 reduced their access to vaccines. Of these women, 22 (73.3%) declared they would accept being vaccinated if the vaccine were administered during a prenatal visit/ hospitalization, and that the ideal place (19 answers, 63%) to be administered a vaccine is where routine antenatal visits are performed.
The main reasons to be vaccinated or to refuse immunization for each subgroup of patients are reported in
Table 2,
Table 3,
Table 4,
Table 5,
Table 6 and
Table 7. Both for the flu shot and Tdap, pregnant patients were more likely to accept the vaccines if they were recommended by a healthcare provider, whereas the main reason not to be vaccinated was the lack of such a recommendation.
Thirty-eight (19.5%) women received the recommendation for the flu vaccine, mainly from an obstetrician–gynecologist (23 women, 60.5%), and 28 women did not accept the vaccine despite the recommendation. The main reason not to be vaccinated in this group was that they did not think the vaccine was necessary for pregnant women/newborns (answer chosen 10 times). Seven women were administered the flu vaccine although they were not recommended it. The main reason to be vaccinated in this group was that they undergo such a vaccination every year. Indeed, to be vaccinated in the season 2018–2019 was consistently associated with being vaccinated the following year as well (p 0.0001). On the other hand, flu vaccination uptake in the previous season was not associated with a higher acceptance of Tdap in pregnancy (p 0.5152).
A total of 117 (60%) women stated they had been recommended the administration of the Tdap vaccine during pregnancy, mainly from an obstetrician–gynecologist (85 cases, 72.6%); 23 women did not accept the Tdap vaccine although they were recommended it. The main reasons not to be vaccinated in this group were that they did not think the vaccine was effective (chosen four times) or necessary (chosen four times) for pregnant women/newborns. Five women were administered the vaccine against pertussis although they were not recommended it. In this group, the main reason to be vaccinated was that they wanted to protect their babies against pertussis (chosen five times).
Considering only pregnant women recommended for flu and/or Tdap immunization, 73% (28 out of 38) refused the flu shot and 19% (23 out of 117) did not accept the administration of Tdap during pregnancy.
Considering the 28 patients who refused flu immunization despite the recommendation, 25 received the Tdap vaccine recommendation and among this group 18 (72%) accepted it.
With regard to the knowledge about the flu shot and Tdap, most women included in our study were aware that these vaccines protect the pregnant woman and the newborn from influenza and pertussis complications, and that they are harmless to the fetus (
Table 8 and
Table 9).
Ethnicity varied significantly among patients who received the influenza vaccine and those who did not (
p 0.019), as well as those who received the Tdap vaccine and those who did not (
p 0.0001).
Table 10 and
Table 11 contain detailed data on ethnic variations among individuals who received or refused influenza and Tdap vaccines.
4. Discussion
Pregnant women who gave birth in 2020 constitute a unique model to investigate whether and how the SARS-CoV-2 pandemic might have changed the approach toward maternal immunization. These women were expected to be recommended for and receive the flu vaccine during the seasonal influenza epidemic in the 2019–2020 winter (pre-pandemic) [
9,
22], and to be recommended for and receive the Tdap in their third trimester [
8,
23].
The population surveyed showed a low vaccine hesitancy rate and a high level of trust in healthcare providers, as demonstrated by the very low percentage of women that declared they were not willing to have their newborns vaccinated in adherence to the national schedules for immunization in childhood—less than 5%—and by the high proportion of women who declared that they rely on the obstetrician–gynecologist/midwife responsible for their prenatal care.
In the pre-COVID-19 era, less than 20% of the women in our sample were recommended the influenza vaccine, and only 9% were actually administered it. During the COVID-19 pandemic, in the midst of the first Italian lockdown, 60% of the women sampled were recommended to receive the Tdap vaccine, and more than 50% received it. It is extremely difficult to compare these percentages with pre-existing literature regarding vaccine uptake in pregnancy among Italian women due to the lack of a reliable national database. The percentage of Italian maternal immunization reported in the literature is very low. The influenza vaccination rate reported by Napolitano et al. [
10] (2017) is about 10%, and D’Alessandro and co-authors [
12] (2018) point out that only 1.4% of their sample were immunized against seasonal influenza. With regard to the Tdap vaccine, Marchetti et al. [
11] (2018) reported that 52.2% of 600 pregnant women interviewed were willing to receive the vaccine. In the group analyzed by Vilca and co-authors [
13] (2020), only 6.5% and 4.8% of the women were vaccinated against flu and pertussis, respectively. In our survey, the most striking piece of data is that in the same women before and after the coronavirus outbreak, the vaccination uptake increased more than fivefold. We explain such a substantial difference between the pre-COVID-19 and the COVID-19 era by a different sensitivity toward infectious disease complications and the preventive measures thereof.
Indeed, our survey shows that healthcare providers were more inclined to recommend the Tdap than the flu vaccine due to increased attention paid to communicable diseases. Another possible reason for this is that although maternal immunization is included in the agenda of the routine care of pregnancy, healthcare providers might have had less time to provide information in the pre-COVID-19 era due to busy schedules, whereas schedules with appointments far apart in the first Italian lockdown, i.e., allowing for more time between one patient and the following one in order to avoid crowding, made it possible to better inform patients on safety and the importance of maternal immunization. Lastly, obstetricians/gynecologists and midwives may feel insecure about recommending the flu vaccine in the first trimester, since they may erroneously fear teratogenicity at this gestational age.
The crucial role of healthcare providers in informing women about the safety and effectiveness of maternal immunization has been well reported in the literature [
24,
25,
26]. Doctors/midwives should not only inform pregnant women as to the availability of the vaccines, but also provide them with information on possible pertussis and influenza complications, and how immunization can protect both the mother and the offspring; moreover, they should recommend vaccinations at the appropriate gestational age and schedule the immunization if the patient is willing to receive it [
8,
9].
Among those women who were recommended influenza and pertussis immunizations but who did not receive them, the belief that these were not necessary in pregnancy was the main reason not to follow the recommendation. These unfounded opinions underline the importance of correct and effective information provision on the topic. Information was, however, successful in the majority of cases of our sample, as demonstrated by the high number of correct answers about vaccine knowledge, higher than what was previously reported in the Italian population [
11]. Belonging to a foreign ethnicity was associated with a lower likelihood to accept vaccinations despite recommendations, suggesting that linguistic barriers could have affected maternal immunization counselling. Other factors may be involved in the lower uptake of maternal immunization in foreign patients (lack of belief in vaccination, difficulty in returning to vaccine or antenatal care sites for appointment, or other cultural or socio-economic barriers). For this reason, it is important to organize specific training for obstetricians and midwives regarding the benefits and safety of maternal immunization, aiming to provide timely and coherent information to patients.
Concerns about vaccine safety were not a major issue in our sample population, unlike what is reported in the literature [
27,
28]. On the other hand, having been vaccinated in the previous years was positively associated with receiving the influenza vaccination in pregnancy. This was documented by other authors [
24] as well, who therefore recommend to vaccinate non-pregnant young women for influenza in order to ensure that they will receive the vaccine when they become pregnant too. Despite the fact that some authors were concerned about a possible decrease in immunization rates [
29,
30] during the COVID-19 pandemic, our data demonstrate that vaccinations were perceived as an essential form of care. Those patients who declared that fear of contracting SARS-CoV-2 prevented them from scheduling their vaccination also stated they would accept being vaccinated during a consultation included in standard prenatal care. It is indeed reported in the literature that on-site vaccination is associated with a higher vaccination uptake [
31], and that a strategy to improve access to vaccination is to have fewer appointments and to make the vaccination coincide with antenatal routine checks [
32,
33].
The limitations of our study are that only 37% of eligible women returned the questionnaire and took part in the survey, which could make the sample susceptible to selection biases (women with a higher vaccine uptake may be more willing to complete the questionnaire). Moreover, vaccine uptake was self-reported, hence misrecollections cannot be ruled out. The main strength of our paper is that we analyzed immunization uptake rates in the same set of patients before and after the COVID-19 outbreak.
The new challenge is COVID-19 vaccine immunization in pregnancy. COVID-19 vaccination administered in pregnancy provides both maternal and newborn passive immunization [
34], as demonstrated from the transplacental passage of specific antibodies, similarly to what occurs in natural infection [
35]. Preliminary data reported by Blakeway [
36] about COVID-19 vaccine acceptance among pregnant patients revealed that less than one third of pregnant women accepted COVID-19 vaccination. The author’s conclusion points out the need for clear communication to improve awareness among pregnant women and healthcare professionals on vaccine safety, along with strategies to address vaccine hesitancy. Obstetrical staff should be trained to meet the need for precise information regarding the benefits, efficacy and safety of the COVID-19 vaccine as well as flu and Tdap vaccines in order to gain ethically and legally viable informed consent [
37]. It is indeed likely that healthcare providers who are not sufficiently trained will not be able to obtain a satisfactory vaccine uptake, especially in a setting such as that of COVID-19 vaccination, in which hesitancy may be greater due to the perceived shortened testing time and the amplification of adverse effects in the public opinion [
36]. A good level of training, awareness and involvement of the staff is therefore necessary in order to maximize vaccine uptake in the pregnant population [
38].
5. Conclusions
Our survey has found out that the pregnant population do not always receive proper information regarding maternal immunization and its benefits and safety. Pregnant patients are more prone to accepting vaccination if the recommendation comes from obstetrical staff; therefore, counselling should become an integral part of pregnancy care. To be really effective, the vaccine proposal should come from well-trained staff and proper information should be given, also with the aim of obtaining legally and ethically valid consent.
Our survey also highlights how COVID-19 has put the threats posed by infectious diseases in the spotlight, thus creating an environment favorable to recommending vaccination for pregnant women. In order to increase the coverage for flu and Tdap immunization during pregnancy, recommendations should be offered and discussed by obstetrical staff, and vaccinations should be performed during routine prenatal care. Raising awareness in that regard will go a long way towards reducing COVID-19 vaccination hesitancy in the pregnant population.
In conclusion, the COVID-19 lesson has raised awareness regarding the role of vaccines in preventable diseases, positively changing attitudes toward immunization in pregnancy.


 ,
, 


{kind=link}