
The Use of Digital Technologies to Support Vaccination Programmes in Europe: State of the Art and Best Practices from Experts’ Interviews

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
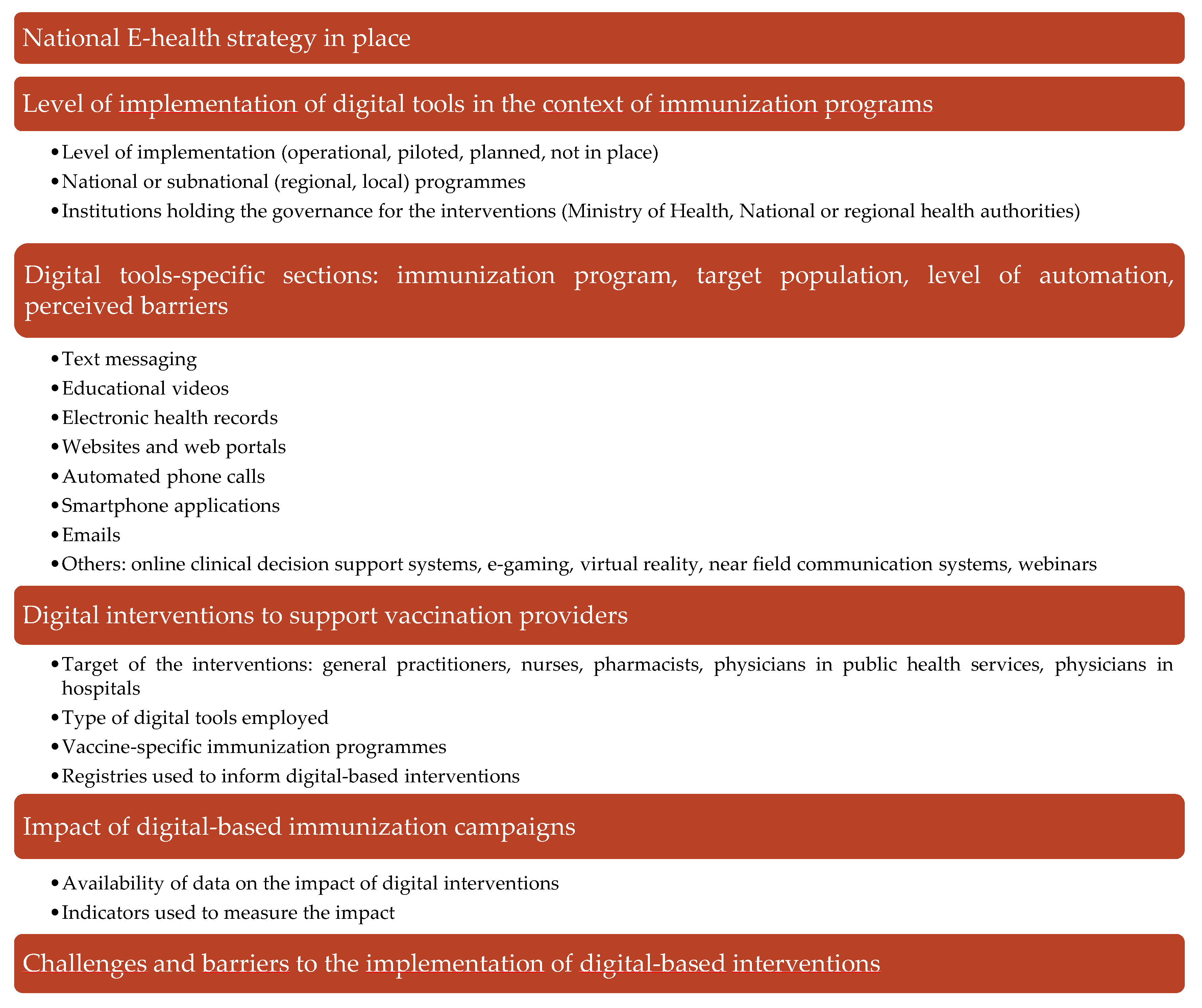
Survey Development and Administration
3. Results
3.1. eHealth Strategies in Europe
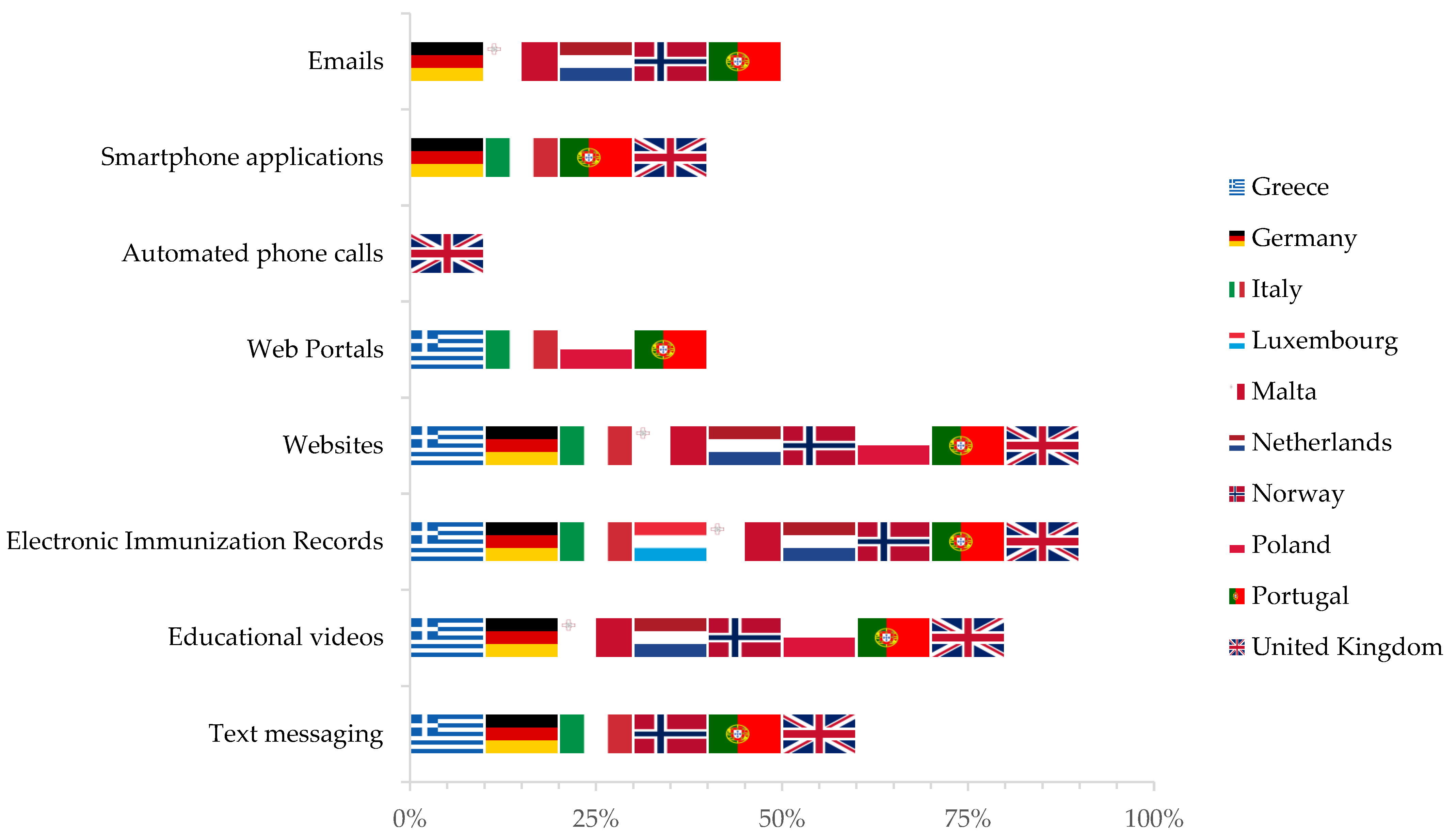
3.2. Digital Tools Employed in the Context of Immunisation Programmes
3.2.1. Electronic Immunisation Records and Immunisation Information Systems (IIS)
3.2.2. Text Messages and Email-Based Systems
3.2.3. Smartphone Applications
3.2.4. Educational Videos, Websites, and Portals
3.2.5. Other Digital Technologies
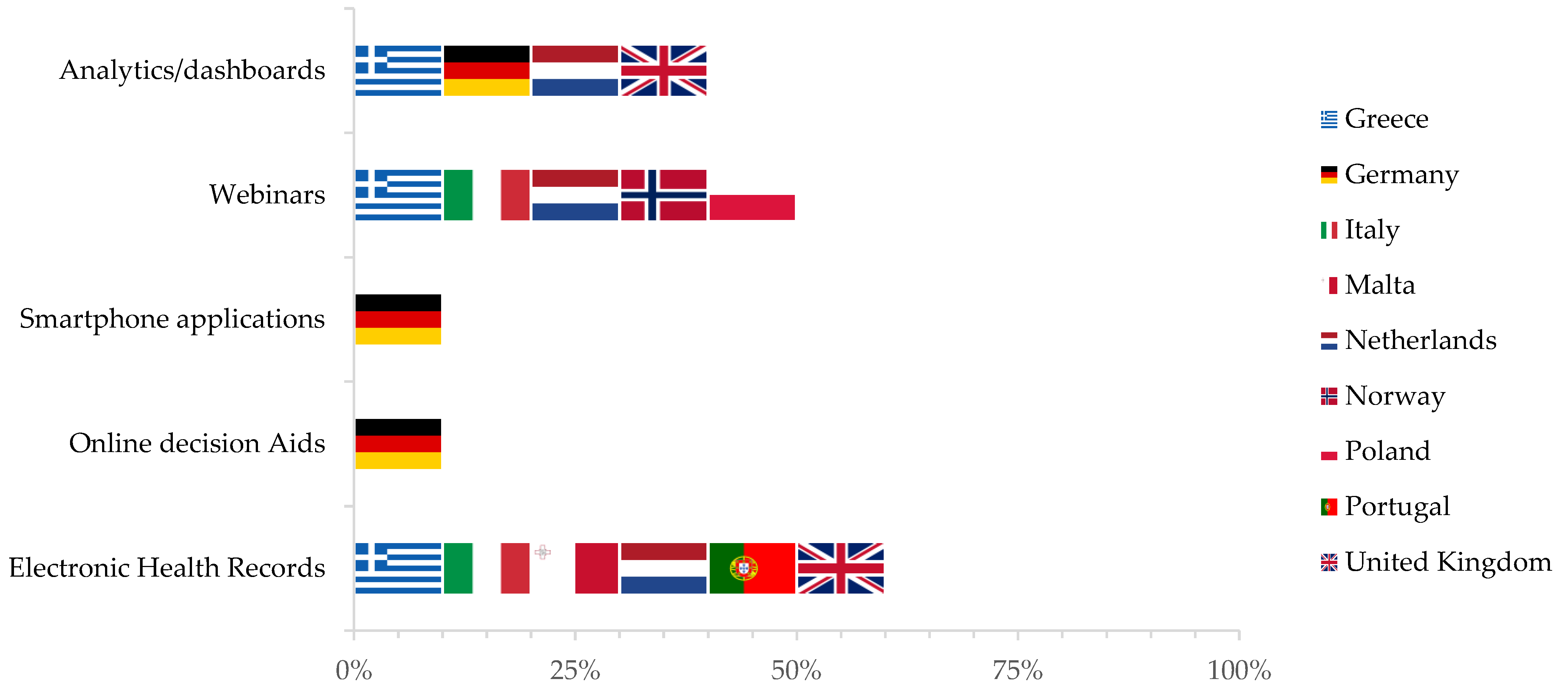
3.3. Digital Tools to Support Healthcare Providers in the Delivery of Vaccinations
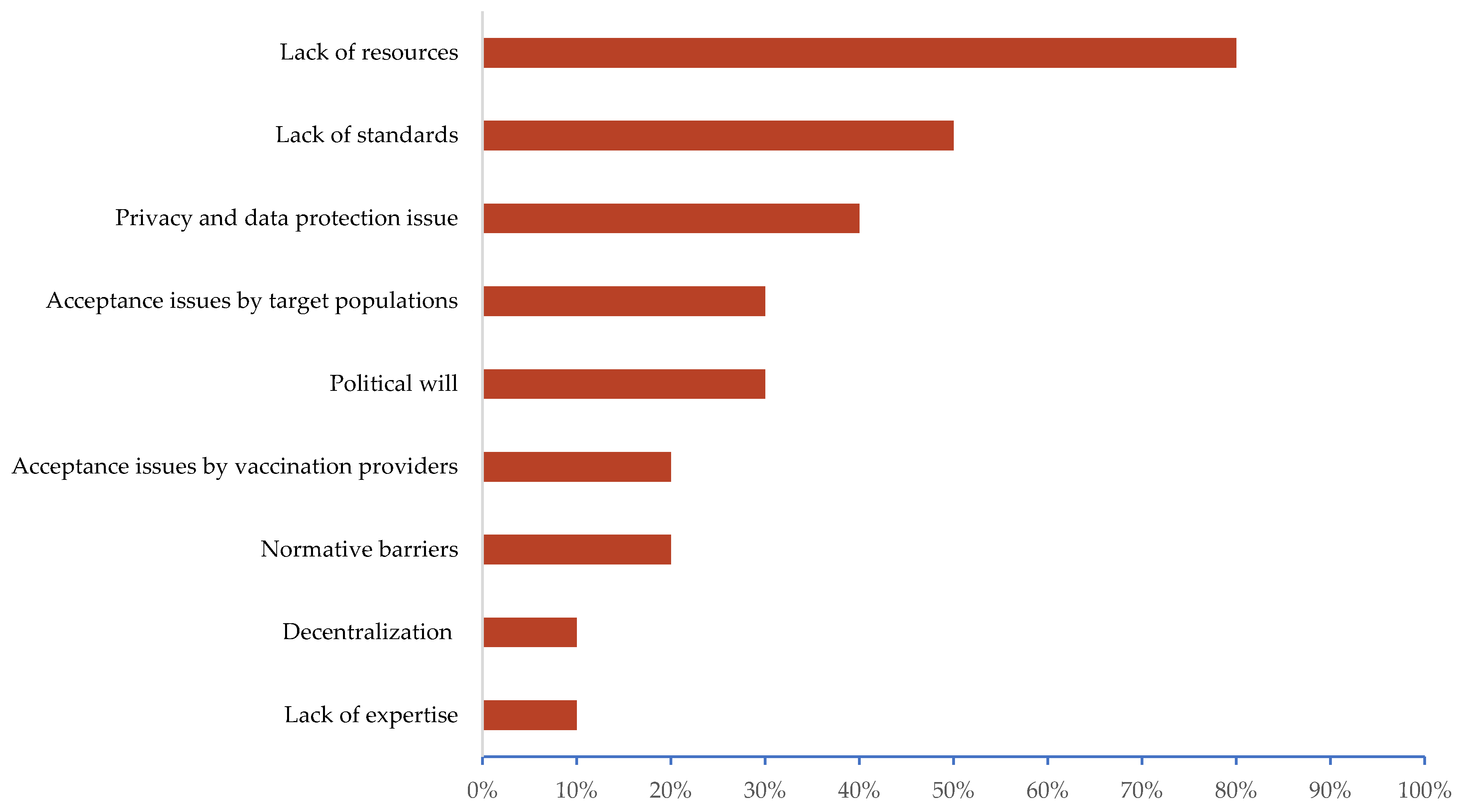
3.4. Perceived Challenges and Barriers in the Development of Digital Tools-Based Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef]
- Audisio, R.A.; Icardi, G.; Isidori, A.M.; Liverani, C.A.; Lombardi, A.; Mariani, L.; Mennini, F.S.; Mitchell, D.A.; Peracino, A.; Pecorelli, S.; et al. Public health value of universal HPV vaccination. Crit. Rev. Oncol./Hematol. 2016, 97, 157–167. [Google Scholar] [CrossRef]
- Wallinga, J.; Heijne, J.C.; Kretzschmar, M. A measles epidemic threshold in a highly vaccinated population. PLoS Med. 2005, 2, e316. [Google Scholar] [CrossRef]
- Sinclair, D.R.; Grefenstette, J.J.; Krauland, M.G.; Galloway, D.D.; Frankeny, R.J.; Travis, C.; Burke, D.S.; Roberts, M.S. Forecasted Size of Measles Outbreaks Associated with Vaccination Exemptions for Schoolchildren. JAMA Netw. Open 2019, 2, e199768. [Google Scholar] [CrossRef]
- Wald, J.S.; Haque, S.N.; Rizk, S.; Webb, J.R.; Brown, S.; Ebron, S.; Lehmann, C.U.; Frisse, M.; Shorte, V.A.; Lomotan, E.A.; et al. Enhancing Health IT functionality for children: The 2015 children’s ehr format. Pediatrics 2018, 141, e20163894. [Google Scholar] [CrossRef] [Green Version]
- Walker, R.D.; Yasuda, K.; Hammer, L.D.; Harlor, A.D., Jr.; Itkin, P.G.; Jakubec, P.J.; Leeds, A.J. Immunization information systems. Pediatrics 2006, 118, 1293–1295. [Google Scholar]
- Bonanni, P.; Ferro, A.; Guerra, R.; Iannazzo, S.; Odone, A.; Pompa, M.G.; Rizzuto, E.; Signorelli, C. Vaccine coverage in Italy and assessment of the 2012–2014 National Immunization Prevention Plan. Epidemiol. Prev. 2015, 39, 146–158. [Google Scholar]
- World Health Organization; Regional Office for Europe. The European Immunization Agenda 2030. Available online: https://www.euro.who.int/en/health-topics/health-policy/european-programme-of-work/flagship-initiatives/the-european-immunization-agenda-2030 (accessed on 27 September 2021).
- Burioni, R.; Odone, A.; Signorelli, C. Lessons from Italy’s policy shift on immunization. Nature 2018, 555, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odone, A.; Bucci, D.; Croci, R.; Riccò, M.; Affanni, P.; Signorelli, C. Vaccine hesitancy in COVID-19 times. An update from Italy before flu season starts. Acta Biomed. 2020, 91, e2020031. [Google Scholar] [PubMed]
- Murthy, B.P.; Zell, E.; Kirtland, K.; Jones-Jack, N.; Harris, L.; Sprague, C.; Schultz, J.; Le, Q.; Bramer, C.A.; Kuramoto, S. Impact of the COVID-19 Pandemic on Administration of Selected Routine Childhood and Adolescent Vaccinations—10 US Jurisdictions, March–September 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 840. [Google Scholar] [CrossRef] [PubMed]
- Gostin, L.O.; Hodge, J.G., Jr.; Bloom, B.R.; El-Mohandes, A.; Fielding, J.; Hotez, P.; Kurth, A.; Larson, H.J.; Orenstein, W.A.; Rabin, K. The public health crisis of underimmunisation: A global plan of action. Lancet Infect. Dis. 2020, 20, e11–e16. [Google Scholar] [CrossRef]
- Larson, H.J.; Wilson, R.; Hanley, S.; Parys, A.; Paterson, P. Tracking the global spread of vaccine sentiments: The global response to Japan’s suspension of its HPV vaccine recommendation. Hum. Vaccines Immunother. 2014, 10, 2543–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wangia, V. Testing an extended theoretical framework to explain variance in use of a public health information system. Online J. Public Health Inf. 2012, 4, ojphi–v4i3. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccines Immunother. 2013, 9, 1802–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzola, E.; Spina, G.; Tozzi, A.E.; Villani, A. Global Measles Epidemic Risk: Current Perspectives on the Growing Need for Implementing Digital Communication Strategies. Risk Manag. Healthc. Policy 2020, 13, 2819–2826. [Google Scholar] [CrossRef]
- Signorelli, C.; Iannazzo, S.; Odone, A. The imperative of vaccination put into practice. Lancet. Infect. Dis. 2018, 18, 26–27. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Moretti, M.; Lopalco, P.L. Countering vaccine hesitancy through immunization information systems, a narrative review. Hum. Vaccines Immunother. 2019, 15, 2508–2526. [Google Scholar] [CrossRef]
- Chen, L.; Tang, H.; Liao, S.; Hu, Y. e-Health Campaigns for Promoting Influenza Vaccination: Examining Effectiveness of Fear Appeal Messages from Different Sources. Telemed. J. E-Health 2020, 20, 763–770. [Google Scholar] [CrossRef]
- Dumit, E.M.; Novillo-Ortiz, D.; Contreras, M.; Velandia, M.; Danovaro-Holliday, M.C. The use of eHealth with immunizations: An overview of systematic reviews. Vaccine 2018, 36, 7923–7928. [Google Scholar] [CrossRef]
- Poorman, E.; Gazmararian, J.; Parker, R.M.; Yang, B.; Elon, L. Use of text messaging for maternal and infant health: A systematic review of the literature. Matern. Child Health J. 2015, 19, 969–989. [Google Scholar] [CrossRef] [PubMed]
- Police, R.L.; Foster, T.; Wong, K.S. Adoption and use of health information technology in physician practice organisations: Systematic review. Inf. Prim. Care 2010, 18, 245–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groom, H.; Hopkins, D.P.; Pabst, L.J.; Murphy Morgan, J.; Patel, M.; Calonge, N.; Coyle, R.; Dombkowski, K.; Groom, A.V.; Kurilo, M.B.; et al. Immunization information systems to increase vaccination rates: A community guide systematic review. J. Public Health Manag. Pract. 2015, 21, 227–248. [Google Scholar] [CrossRef]
- Francis, D.B.; Cates, J.R.; Wagner, K.P.G.; Zola, T.; Fitter, J.E.; Coyne-Beasley, T. Communication technologies to improve HPV vaccination initiation and completion: A systematic review. Patient Educ. Couns. 2017, 100, 1280–1286. [Google Scholar] [CrossRef]
- Ohannessian, R.; Yaghobian, S.; Verger, P.; Vanhems, P. A systematic review of serious video games used for vaccination. Vaccine 2016, 34, 4478–4483. [Google Scholar] [CrossRef]
- Atkinson, K.M.; Wilson, K.; Murphy, M.S.Q.; El-Halabi, S.; Kahale, L.A.; Laflamme, L.L.; El-Khatib, Z. Effectiveness of digital technologies at improving vaccine uptake and series completion—A systematic review and meta-analysis of randomized controlled trials. Vaccine 2019, 37, 3050–3060. [Google Scholar] [CrossRef]
- Frascella, B.; Oradini-Alacreu, A.; Balzarini, F.; Signorelli, C.; Lopalco, P.L.; Odone, A. Effectiveness of email-based reminders to increase vaccine uptake: A systematic review. Vaccine 2020, 38, 433–443. [Google Scholar] [CrossRef]
- Balzarini, F.; Frascella, B.; Oradini-Alacreu, A.; Gaetti, G.; Lopalco, P.L.; Edelstein, M.; Azzopardi-Muscat, N.; Signorelli, C.; Odone, A. Does the use of personal electronic health records increase vaccine uptake? A systematic review. Vaccine 2020, 38, 5966–5978. [Google Scholar] [CrossRef]
- Eurostat. Digital Economy and Society—Overview. Available online: https://ec.europa.eu/eurostat/web/digital-economy-and-society/overview (accessed on 27 September 2021).
- European Commission. Communication on Enabling the Digital Transformation of Health and Care in the Digital Single Market; Empowering Citizens and Building a Healthier Society. Available online: https://digital-strategy.ec.europa.eu/en/library/communication-enabling-digital-transformation-health-and-care-digital-single-market-empowering (accessed on 27 September 2021).
- Nictiz. eHealth in the Netherlands. Policies, Developments and Status of Cross-Enterprise Information Exchange in Dutch Healthcare. 2014. Available online: https://joinup.ec.europa.eu/sites/default/files/document/2014-12/eHealth%20in%20the%20Netherlands%20-%20Policies%2C%20developments%20and%20status%20of%20cross-enterprise%20information%20exchange%20in%20Dutch%20healthcare.pdf (accessed on 27 September 2021).
- eHealth Initiative in Italy Section in Italian Ministry of Health Website. Available online: http://www.salute.gov.it/portale/temi/p2_5.jsp?lingua=italiano&area=eHealth&menu=iniziative (accessed on 27 September 2021).
- Sicurello, F. Medical Informatics and Telemedicine: 50 Years of Developments. Available online: http://www.iiimb.me/files/3-06-05-20--telemedicine-Sicurello--50-years.pdf (accessed on 27 September 2021).
- Wagner, A.L.; Eccleston, A.M.; Potter, R.C.; Swanson, R.G.; Boulton, M.L. Vaccination Timeliness at Age 24 Months in Michigan Children Born 2006–2010. Am. J. Prev. Med. 2018, 54, 96–102. [Google Scholar] [CrossRef]
- Urquhart, G.A.; Williams, W.; Tobias, J.; Welch, F.J. Immunization information systems use during a public health emergency in the United States. J. Public Health Manag. Pract. 2007, 13, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Models of Child Health Appraised (MOCHA) Project. Available online: https://www.childhealthservicemodels.eu/ (accessed on 27 September 2021).
- Vaghefi, I.; Hughes, J.B.; Law, S.; Lortie, M.; Leaver, C.; Lapointe, L. Understanding the Impact of Electronic Medical Record Use on Practice-Based Population Health Management: A Mixed-Method Study. JMIR Med. Inf. 2016, 4, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alderwick, H.; Dixon, J. The NHS long term plan. BMJ 2019, 364, l84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valluru, N.; Gaidos, J. Improving health maintenance in veterans with inflammatory bowel disease using a template in the computerized patient record system. Gastroenterology 2017, 152, S787–S788. [Google Scholar] [CrossRef]
- Fragidis, L.L.; Chatzoglou, P. The Use of Electronic Health Record in Greece: Current Status. In Proceedings of the 2011 IEEE 11th International Conference on Computer and Information Technology, Pafos, Cyprus, 31 August–2 September 2011; pp. 475–480. [Google Scholar]
- eRedBook. Available online: https://www.eredbook.org.uk (accessed on 27 September 2021).
- Utidjian, L.; Kirkendall, E.; Shelov, E. Clinical Decision Support in the Pediatric Hospital Setting. Curr. Treat. Options Pediatrics 2015, 1, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Bonanni, P.; Azzari, C.; Castiglia, P.; Chiamenti, G.; Conforti, G.; Conversano, M.; Corsello, G.; Ferrera, G.; Ferro, A.; Icardi, G. The 2014 lifetime immunization schedule approved by the Italian scientific societies. Italian Society of Hygiene, Preventive Medicine, and Public Health. Italian Society of Pediatrics. Italian Federation of Pediatric Physicians. Italian Federation of General Medical Physicians. Arezzo Service of Legal Medicine. Epidemiol. E Prev. 2014, 38, 131–146. [Google Scholar]
- D’Ancona, F.; Gianfredi, V.; Riccardo, F.; Iannazzo, S. Immunisation Registries at regional level in Italy and the roadmap for a future Italian National Registry. Ann. Ig. Med. Prev. E Comunita 2018, 30, 77–85. [Google Scholar]
- Anagrafe Nazionale Vaccini, Italian Registry of Vaccination. Available online: http://www.salute.gov.it/portale/vaccinazioni/dettaglioContenutiVaccinazioni.jsp?lingua=italiano&id=5067&area=vaccinazioni&menu=vuoto (accessed on 27 September 2021).
- Valluru, N.; Kang, L.; Gaidos, J.K.J. Health Maintenance Documentation Improves for Veterans with IBD Using a Template in the Computerized Patient Record System. Dig. Dis. Sci. 2018, 63, 1782–1786. [Google Scholar] [CrossRef]
- Wilson, R.M.; Brown, D.R.; Carmody, D.P.; Fogarty, S. HPV Vaccination Completion and Compliance with Recommended Dosing Intervals Among Female and Male Adolescents in an Inner-City Community Health Center. J. Community Health 2015, 40, 395–403. [Google Scholar] [CrossRef]
- Wilson, M.; Brown, B.; Miles, M.; Prasada, S. A multicomponent curriculum can improve pneumococcal vaccination knowledge and clinical practice among internal medicine residents. Chest 2017, 152, A568. [Google Scholar] [CrossRef]
- Wilson, K.; Atkinson, K.M.; Bell, C.P. Travel vaccines enter the digital age: Creating a virtual immunization record. Am. J. Trop. Med. Hyg. 2016, 94, 485–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffens, M.S.; Dunn, A.G.; Leask, J.; Wiley, K.E. Using social media for vaccination promotion: Practices and challenges. Digit. Health 2020, 6, 2055207620970785. [Google Scholar] [CrossRef]
- Wilson, S.E.; Quach, S.; MacDonald, S.E.; Naus, M.; Deeks, S.L.; Crowcroft, N.S.; Mahmud, S.M.; Tran, D.; Kwong, J.; Tu, K.; et al. Methods used for immunization coverage assessment in Canada, a Canadian Immunization Research Network (CIRN) study. Hum. Vaccines Immunother. 2017, 13, 1928–1936. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.E.; Quach, S.; MacDonald, S.E.; Naus, M.; Deeks, S.L.; Crowcroft, N.S.; Mahmud, S.M.; Tran, D.; Kwong, J.C.; Tu, K.; et al. Immunization information systems in Canada: Attributes, functionality, strengths and challenges. A Canadian Immunization Research Network study. Can. J. Public Health 2017, 107, e575–e582. [Google Scholar] [CrossRef]
- Kolff, C.A.; Scott, V.P.; Stockwell, M.S. The use of technology to promote vaccination: A social ecological model based framework. Hum. Vaccines Immunother. 2018, 14, 1636–1646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derrough, T.; Olsson, K.; Gianfredi, V.; Simondon, F.; Heijbel, H.; Danielsson, N.; Kramarz, P.; Pastore-Celentano, L. Immunisation Information Systems—Useful tools for monitoring vaccination programmes in EU/EEA countries, 2016. Eurosurveillance 2017, 22, 30519. [Google Scholar] [CrossRef]
- Scobie, H.M.; Edelstein, M.; Nicol, E.; Morice, A.; Rahimi, N.; MacDonald, N.E.; Danovaro-Holliday, C.M.; Jawad, J. Improving the quality and use of immunization and surveillance data: Summary report of the Working Group of the Strategic Advisory Group of Experts on Immunization. Vaccine 2020, 38, 7183–7197. [Google Scholar] [CrossRef]
- Ferro, A.; Odone, A.; Siddu, A.; Colucci, M.; Anello, P.; Longone, M.; Marcon, E.; Castiglia, P.; Bonanni, P.; Signorelli, C. Monitoring the web to support vaccine coverage: Results of two years of the portal VaccinarSì. Epidemiol. Prev. 2015, 39, 88–93. [Google Scholar]
- Odone, A.; Signorelli, C. When vaccine hesitancy makes headlines. Vaccine 2017, 35, 1209–1210. [Google Scholar] [CrossRef]
- Gianfredi, V.; Grisci, C.; Nucci, D.; Parisi, V.; Moretti, M. Communication in health. Recenti Prog. Med. 2018, 109, 374–383. [Google Scholar]
- Abdullahi, L.H.; Kagina, B.M.; Ndze, V.N.; Hussey, G.D.; Wiysonge, C.S. Improving vaccination uptake among adolescents. Cochrane Database Syst. Rev. 2020, 1, CD011895. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Odone, A.; Fiacchini, D.; Rosselu, R.; Battista, T.; Signorelli, C. Trust and reputation management, branding, social media management nelle organizzazioni sanitarie: Sfide e opportunity per la comunita igienistica italiana. J. Prev. Med. Hyg. 2019, 60, E108–E109. [Google Scholar]
- Tozzi, A.E.; Gesualdo, F.; D’Ambrosio, A.; Pandolfi, E.; Agricola, E.; Lopalco, P. Can Digital Tools Be Used for Improving Immunization Programs? Front. Public Health 2016, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Ferrari, A.; Spagnoli, F.; Visciarelli, S.; Shefer, A.; Pasquarella, C.; Signorelli, C. Effectiveness of interventions that apply new media to improve vaccine uptake and vaccine coverage. Hum. Vaccines Immunother. 2015, 11, 72–82. [Google Scholar] [CrossRef] [Green Version]
- Odone, A.; Buttigieg, S.; Ricciardi, W.; Azzopardi-Muscat, N.; Staines, A. Public health digitalization in Europe. Eur. J. Public Health 2019, 29, 28–35. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Digital Solutions during the Pandemic. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/digital-solutions-during-pandemic_en (accessed on 27 September 2021).
- Burgess, R.A.; Osborne, R.H.; Yongabi, K.A.; Greenhalgh, T.; Gurdasani, D.; Kang, G.; Falade, A.G.; Odone, A.; Busse, R.; Martin-Moreno, J.M.; et al. The COVID-19 vaccines rush: Participatory community engagement matters more than ever. Lancet (Lond. Engl.) 2021, 397, 8–10. [Google Scholar] [CrossRef]
- Esteban-Navarro, M.-Á.; García-Madurga, M.-Á.; Morte-Nadal, T.; Nogales-Bocio, A.-I. The Rural Digital Divide in the Face of the COVID-19 Pandemic in Europe—Recommendations from a Scoping Review. Informatics 2020, 7, 54. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for Europe; European Observatory on Health Systems and Policies; Rechel, B.; Richardson, E.; McKee. The Organization and Delivery of Vaccination Services in the European Union: Prepared for the European Commission. Available online: https://apps.who.int/iris/handle/10665/330345 (accessed on 27 September 2021).
- Rigby, M.; Kühne, G.; Greenfield, R.; Majeed, A.; Blair, M.E. Extent of use of electronic records in Children’s Primary Care and Public Health in Europe. Stud. Health Technol. Inform. 2018, 247, 930–934. [Google Scholar] [PubMed]
- World Health Organization; Regional Office for Europe. European Programme of Work 2020–2025: United Action for Better Health. Available online: https://apps.who.int/iris/handle/10665/339209 (accessed on 27 September 2021).
- Cella, P.; Voglino, G.; Barberis, I.; Alagna, E.; Alessandroni, C.; Cuda, A.; D’Aloisio, F.; Dallagiacoma, G.; De Nitto, S.; Di Gaspare, F.; et al. Resources for assessing parents’ vaccine hesitancy: A systematic review of the literature. J. Prev. Med. Hyg. 2020, 61, E340–E373. [Google Scholar] [PubMed]
| 1 | Vaccination Coverage |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Greece | Germany | Italy | Luxembourg | Malta | The Netherlands | Norway | Poland | Portugal | United Kingdom | |
|---|---|---|---|---|---|---|---|---|---|---|
| Population 1 | 10,724,599 | 83,019,213 | 60,359,546 | 613,894 | 493,559 | 17,282,163 | 5,383,212 | 37,972,812 | 10,276,617 | 66,647,112 |
| Younger than 15 years | 14.33% | 13.60% | 13% | 16.06% | 13.68% | 15.85% | 17.55% | 15.36% | 13.70% | 17.9% |
| From 15 to 64 years | 63.63% | 64.86% | 64% | 69.55 | 67.65% | 64.97% | 65.21% | 66.98% | 64.47% | 63.7% |
| 65 years or over | 22.04% | 21.54% | 23% | 14.39% | 18.68% | 19.18% | 17.24% | 17.66% | 21.84% | 18.4% |
| Socio economic indicators 1 | ||||||||||
| Real GDP per capita (2019) | 18,150 | 35,840 | 28,860 | 83,640 | 22,040 | 41,870 | 69,870 | 12,980 | 18,540 | 32,980 |
| Unemployment rate (2019) | 17.3% | 3.2% | 10% | 5.6% | 3.4% | 3.4% | 3.35% | 3.3% | 6.5% | 3.8% |
| Population (15–64 years) with tertiary education (ISCED 2011 levels 5–8) | 27.8% | 25.9% | 17.4% | 41% | 26.1% | 34.8% | 37.7% | 28.2% | 23.8% | 40.6% |
| Vaccination Coverage | ||||||||||
| DTP1 (2019) 2 | 99% | 99% | 95% | 99% | 98% | n.a. | 99% | n.a. | n.a. | n.a. |
| MCV1 (2019) 2 | 97% | 97% | 94% | 99% | 96% | 94% | 97% | 93% | 99% | 91% |
| Influenza (2017) 3 | n.a. | 34.8% | 52% | n.a. | n.a. | 64.1% | 26.9% | 6.87% | 60% | n.a. |
| Indicators of digitalization 1 | ||||||||||
| Household-level internet access | 79% | 95% | 85% | 95% | 86% | 98% | 98% | 87% | 81% | 96% |
| Individuals’ internet use | 76% | 94% | 78% | 97% | 78% | 96% | 99% | 82% | 76% | 96% |
| Digital inclusion of individuals | 74% | 91% | 74% | 93% | 85% | 95% | 98% | 78% | 73% | 95% |
| E-government activities of individuals, via websites | 52% | 59% | 23% | 60% | 50% | 81% | 87% | 40% | 41% | 63% |
| Individuals who have basic or above basic overall digital skills | 79% | 70% | 42% | 65% | 42% | 79% | 83% | 44% | 52% | 74% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odone, A.; Gianfredi, V.; Sorbello, S.; Capraro, M.; Frascella, B.; Vigezzi, G.P.; Signorelli, C. The Use of Digital Technologies to Support Vaccination Programmes in Europe: State of the Art and Best Practices from Experts’ Interviews. Vaccines 2021, 9, 1126. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101126
Odone A, Gianfredi V, Sorbello S, Capraro M, Frascella B, Vigezzi GP, Signorelli C. The Use of Digital Technologies to Support Vaccination Programmes in Europe: State of the Art and Best Practices from Experts’ Interviews. Vaccines. 2021; 9(10):1126. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101126
Chicago/Turabian StyleOdone, Anna, Vincenza Gianfredi, Sebastiano Sorbello, Michele Capraro, Beatrice Frascella, Giacomo Pietro Vigezzi, and Carlo Signorelli. 2021. "The Use of Digital Technologies to Support Vaccination Programmes in Europe: State of the Art and Best Practices from Experts’ Interviews" Vaccines 9, no. 10: 1126. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101126