
Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunization Programs in Europe: A Systematic Review of the Literature


Abstract
:1. Introduction
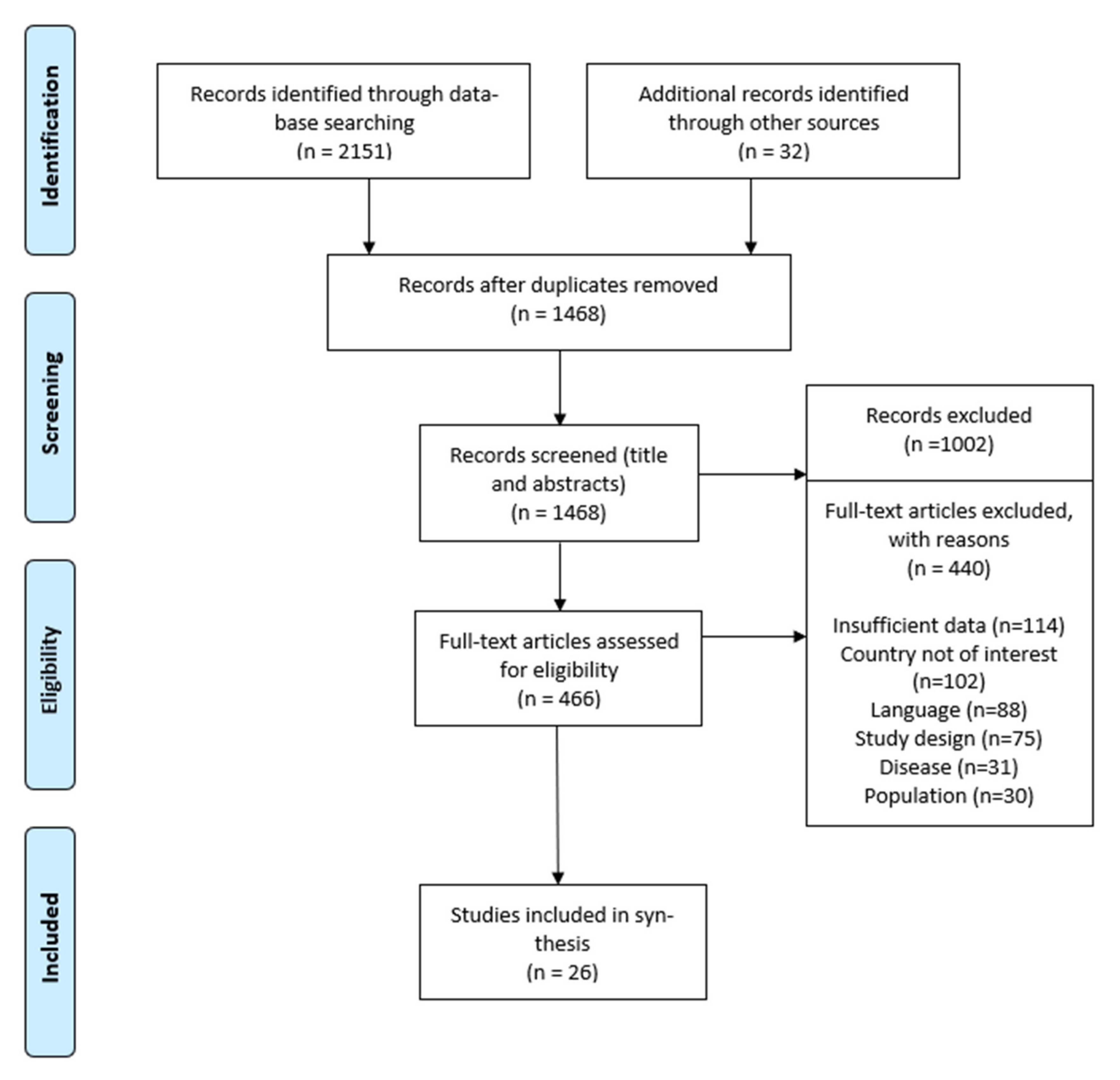
2. Methods
2.1. Eligibility Criteria
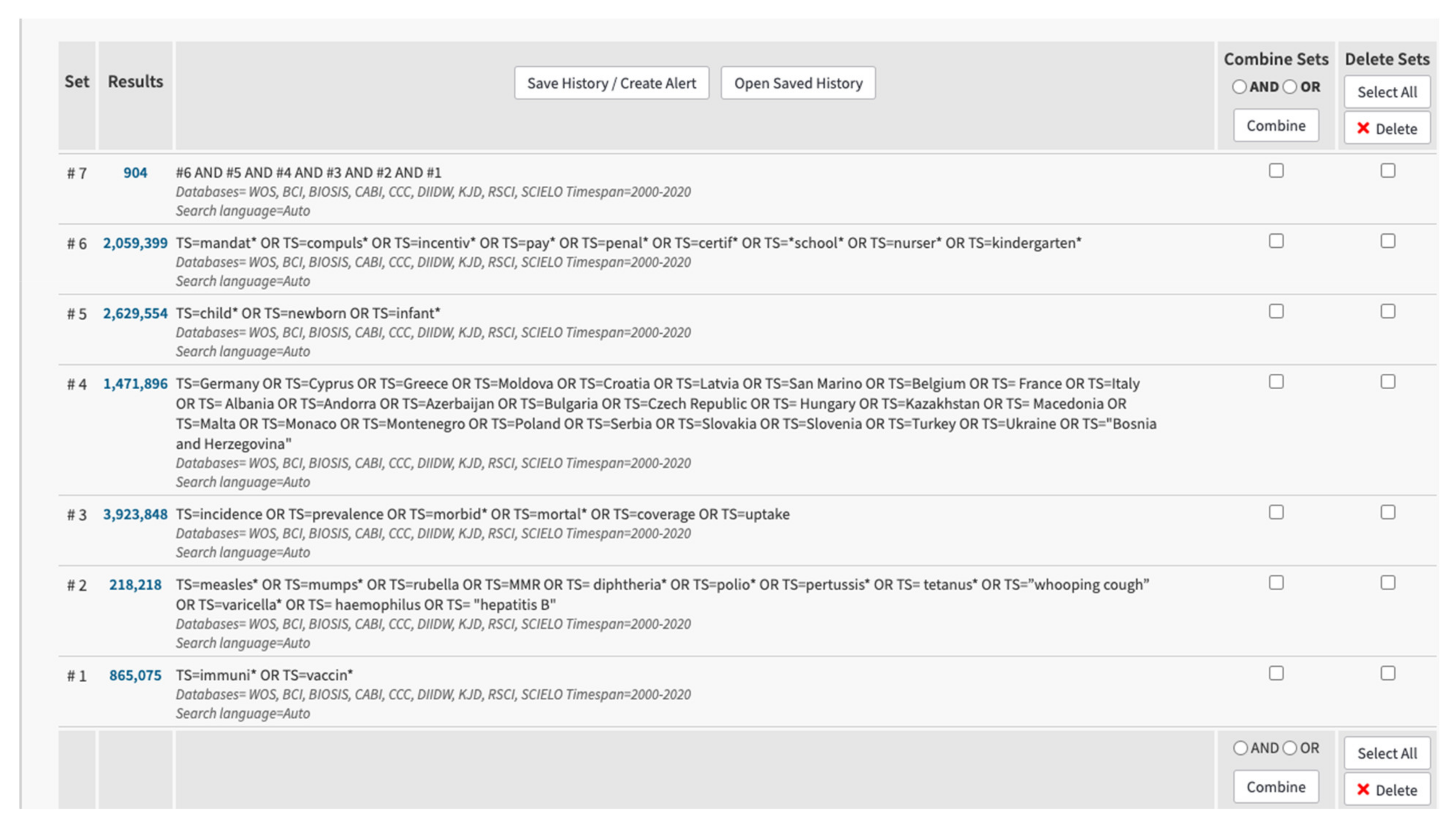
2.2. Information Sources
2.3. Study Selection, Data Collection, and Analysis
3. Results
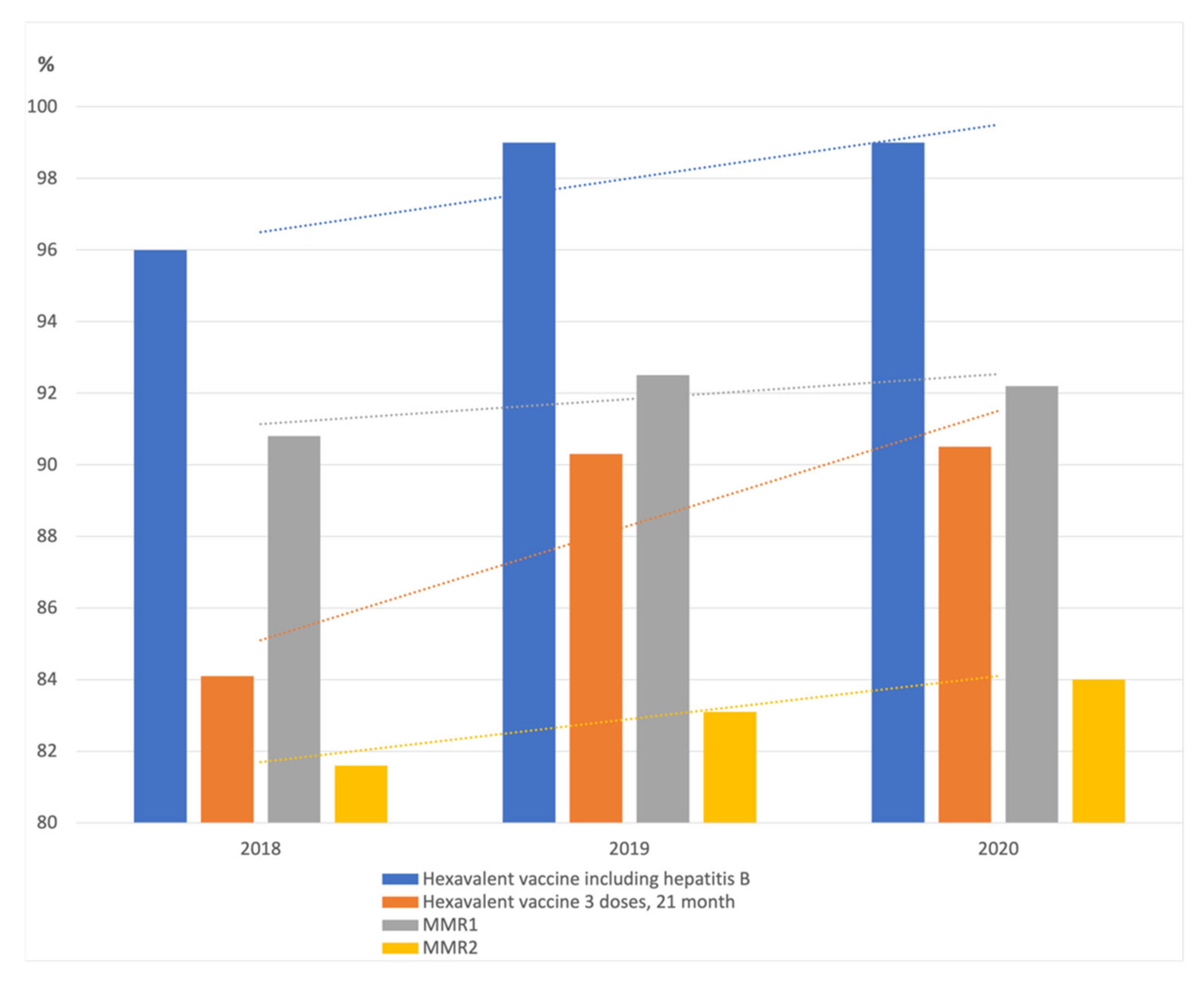
3.1. France
3.2. Germany
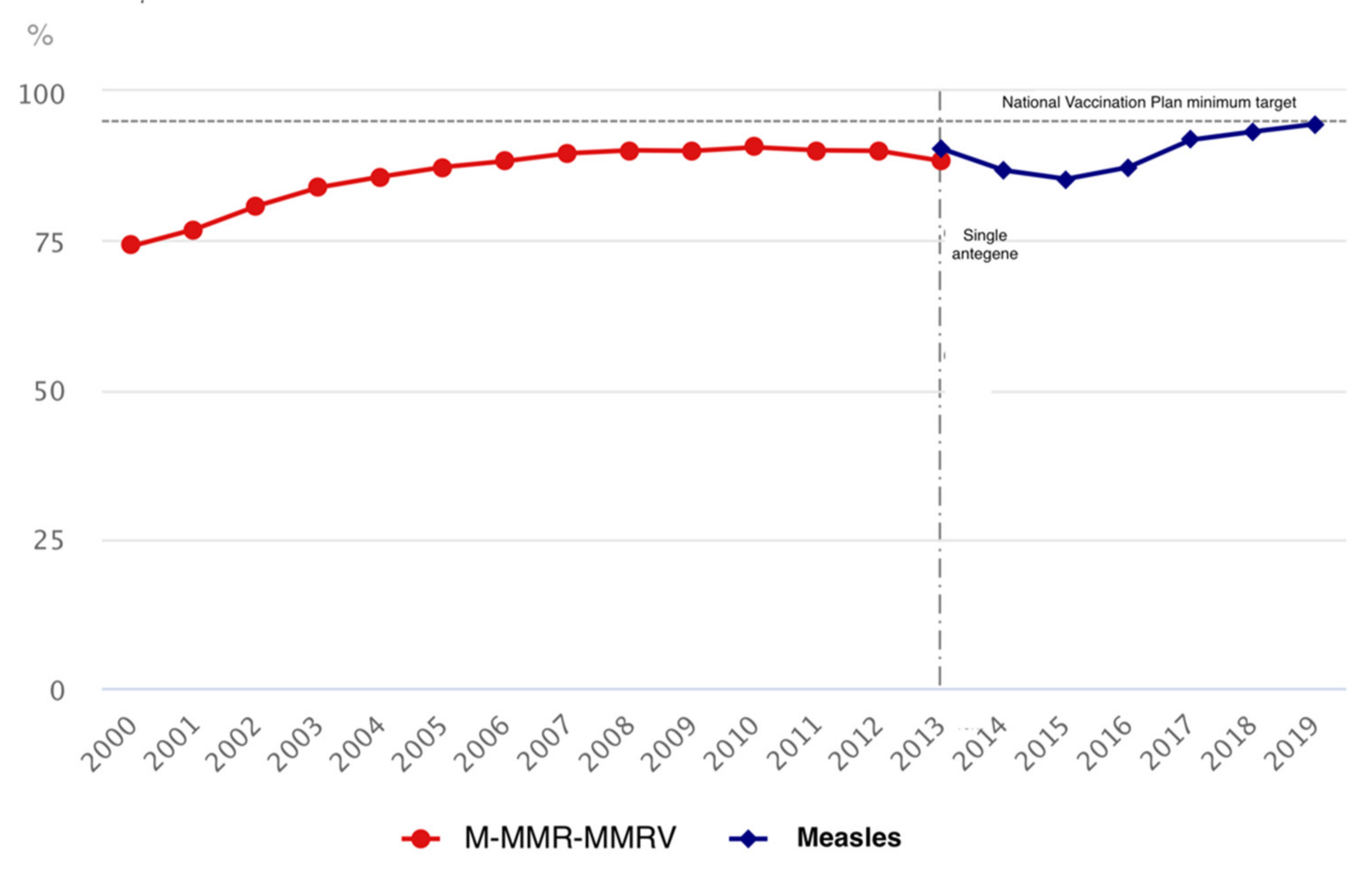
3.3. Italy
3.4. Latvia
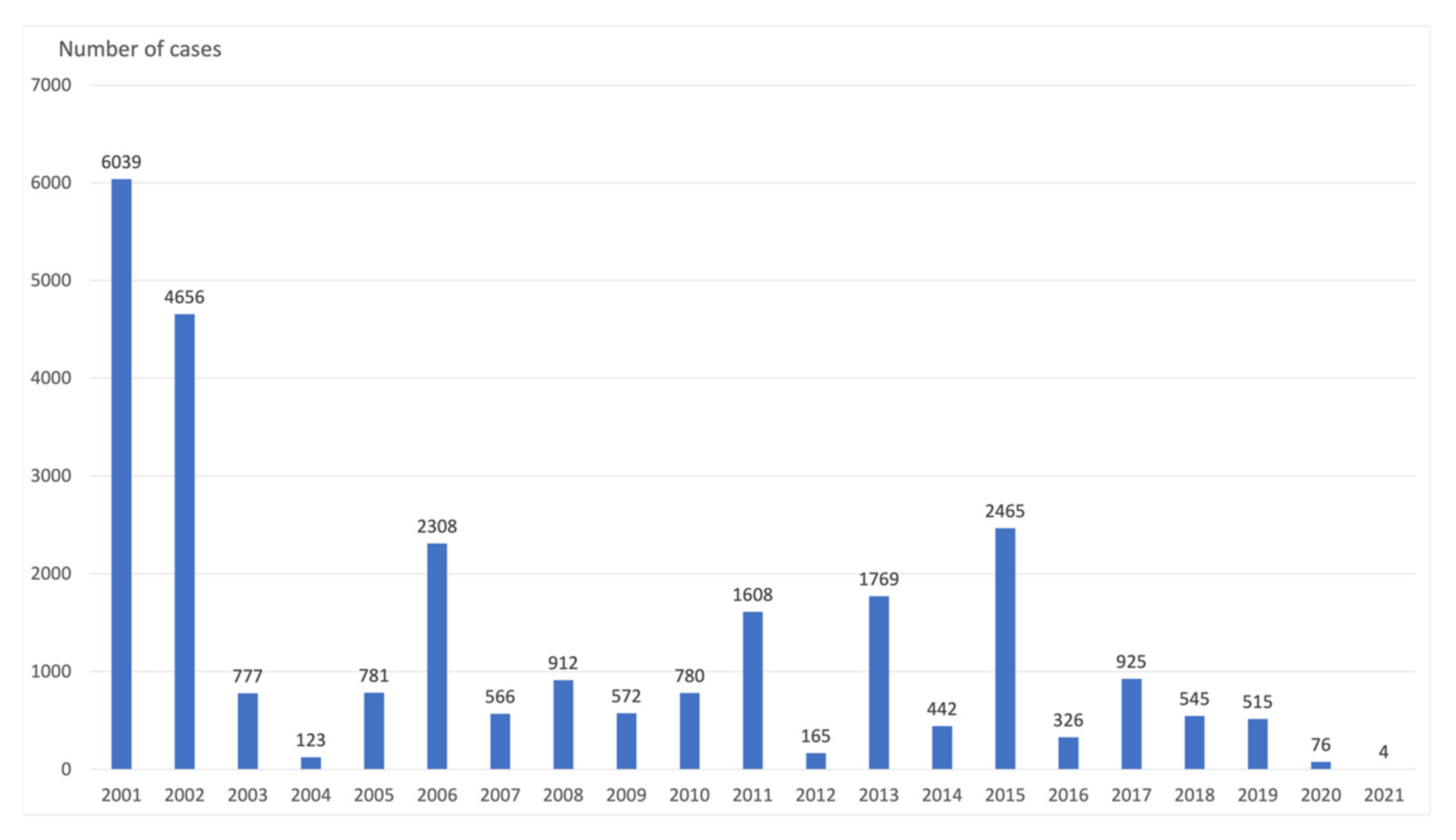
3.5. Moldova
3.6. Serbia
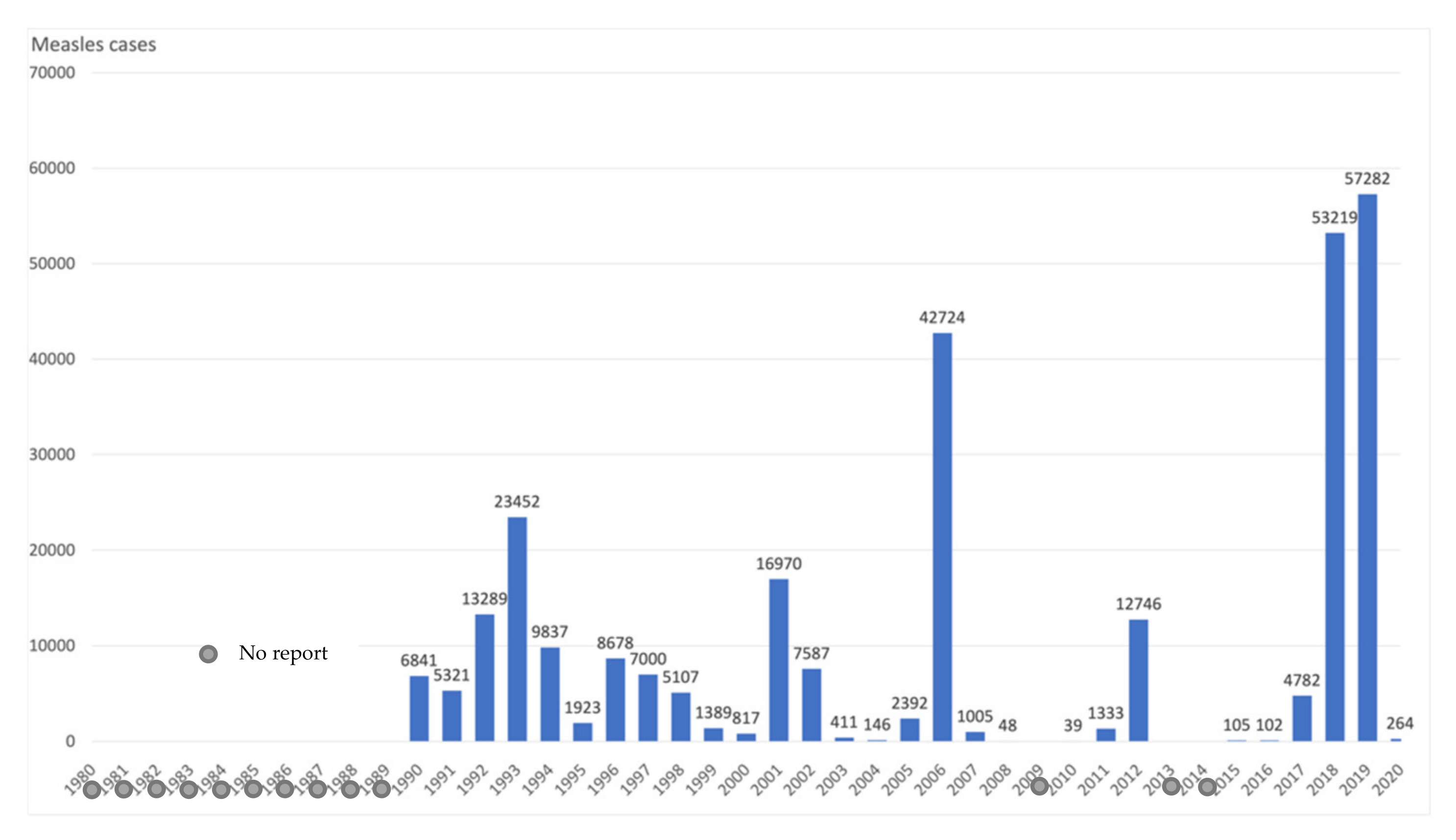
3.7. Ukraine
3.8. Impact of COVID-19 Pandemic on Vaccination Coverage and Incidence of the Vaccine-Preventable Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Example Search Strategy from MEDLINE
- Immunization/(51045);
- immuni*. mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (458065);
- exp Vaccination/(86424);
- vaccin*. mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (385553);
- Immunization Programs/(11077);
- 1 or 2 or 3 or 4 or 5 (708621);
- exp Measles-Mumps-Rubella Vaccine/(2766);
- exp Measles Vaccine/(8937);
- exp Mumps Vaccine/(3788);
- exp Poliovirus Vaccines/(7514);
- exp Rubella Vaccine/(5147);
- Vaccines, Combined/(2361);
- Pertussis Vaccine/(5204);
- Diphtheria-Tetanus Vaccine/(398);
- Diphtheria-Tetanus-Pertussis Vaccine/(2897);
- Chickenpox Vaccine/(2054);
- Hepatitis B Vaccines/(9349);
- Haemophilus Vaccines/(2991);
- measles*. mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (28284);
- mumps*. mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (11217);
- rubella.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (16142);
- MMR.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplemen-tary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (8295);
- diphtheria*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (22281);
- polio*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplemen-tary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (36359);
- pertussis*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (30518);
- tetanus*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (29199);
- whooping cough.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (9574);
- varicella*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (14853);
- haemophilus.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (29227);
- hepatitis B.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (101028);
- 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 (283610);
- exp Epidemiology/(27044);
- inciden*.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (1010003);
- prevalence.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (729539);
- Vaccination Coverage/(1296);
- coverage.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (132429);
- uptake.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (392943);
- 32 or 33 or 34 or 35 or 36 or 37 (2162074);
- Germany.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (199711);
- Cyprus.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (2292);
- Greece.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (25388);
- Moldova.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (1042);
- Croatia.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (9361);
- Latvia.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (2035);
- San Marino.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (115);
- Belgium.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (27470);
- France.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (129353);
- Italy.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplemen-tary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (124903);
- Albania.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (1394);
- Andorra.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (71);
- Azerbaijan.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (2015);
- Bulgaria.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (8195);
- Czech Republic.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (11565);
- Hungary.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (23035);
- Kazakhstan.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (3718);
- Macedonia.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (1391);
- Malta.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplemen-tary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (1609);
- Monaco.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (415);
- Montenegro.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism sup-plementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (887);
- Poland.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (57784);
- Serbia.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (5550);
- Slovakia.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (4886);
- Slovenia.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (4551);
- Turkey.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (54574);
- Ukraine.mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supple-mentary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (17769);
- Bosnia and Herzegovina. mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms] (2868);
- 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 (679377);
- 6 and 31 and 38 and 67 (2312);
- limit 68 to “all child (0 to 18 years)” (1521);
- limit 69 to year = “2000 -Current” (1174).
Appendix B

References
- World Health Organization. Ten Threats to Global Health in 2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 10 September 2021).
- Gualano, M.R.; Olivero, E.; Voglino, G.; Corezzi, M.; Rossello, P.; Vicentini, C.; Bert, F.; Siliquini, R. Knowledge, attitudes and beliefs towards compulsory vaccination: A systematic review. Hum. Vaccines Immunother. 2019, 15, 918–931. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. EpiData 7/2020. 2020. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/vaccines-and-immunization/publications/surveillance-and-data/who-epidata/2020/epidata-72020 (accessed on 20 August 2021).
- Will, R.C.; Ramamurthy, T.; Sharma, N.C.; Veeraraghavan, B.; Sangal, L.; Haldar, P.; Pragasam, A.K.; Vasudevan, K.; Kumar, D.; Das, B.; et al. Spatiotemporal persistence of multiple, diverse clades and toxins of Corynebacterium diphtheriae. Nat. Commun. 2021, 12, 1–8. [Google Scholar] [CrossRef]
- DW News. Coronavirus: Thousands Protest against Restrictions across Europe. Available online: https://www.dw.com/en/coronavirus-thousands-protest-against-restrictions-across-europe/a-58627841 (accessed on 20 August 2021).
- Causey, K.; Fullman, N.; Sorensen, R.J.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef]
- Robert Koch Institut. Aktuelle Statistik meldepflichtiger Infektionskrankheiten 53. Woche 2020. Epidemiol. Bull. 2021, 1, 26–29. [Google Scholar]
- Public Health Center of the Ministry of Health of Ukraine. Infectious Diseases Morbidity of the Population of Ukraine. Available online: https://phc.org.ua/kontrol-zakhvoryuvan/inshi-infekciyni-zakhvoryuvannya/infekciyna-zakhvoryuvanist-naselennya-ukraini (accessed on 20 August 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.D.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Rader, T.; Shokraneh, F.; Thomas, J.; et al. Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.0; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley: Hoboken, NJ, USA, 2019; Available online: www.training.cochrane.org/handbook (accessed on 20 August 2021).
- Cohen, R.; Martinot, A.; Gaudelus, J.; Subtil, D.; Stahl, J.-P.; Pujol, P.; Picquet, V.; Lepetit, H.; Longfier, L.; Leboucher, B. Infant mandatory vaccinations: Confirmation of a positive impact. Méd. Mal. Infect. 2020, 50, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Lévy-Bruhl, D.; Fonteneau, L.; Vaux, S.; Barret, A.-S.; Antona, D.; Bonmarin, I.; Che, D.; Quelet, S.; Coignard, B. Assessment of the impact of the extension of vaccination mandates on vaccine coverage after 1 year, France, 2019. Eurosurveillance 2019, 24, 1900301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taine, M.; Offredo, L.; Drouin, J.; Toubiana, J.; Weill, A.; Zureik, M.; Dray-Spira, R. Mandatory Infant Vaccinations in France During the COVID-19 Pandemic in 2020. Front. Pediatr. 2021, 9, 666848. [Google Scholar] [CrossRef] [PubMed]
- Matysiak-Klose, D.; Santibanez, S.; Mankertz, A. Siedler A: Stand der Elimination der Masern und Röteln in Deutschland—erste erfreuliche Ergebnisse erzielt. Epid. Bull. 2021, 15, 3–7. [Google Scholar] [CrossRef]
- Neugebauer, M.; Ebert, M.; Vogelmann, R. Evaluation of the new German measles protection act: An online survey. Z. Evid. Fortbild. Qual. Gesundhwes. 2020, 158–159, 74–80. [Google Scholar] [CrossRef]
- Robert Koch Institut. Aktuelle Statistik Meldepflichtiger Infektionskrankheiten 21. Woche 2021. Epidemiol. Bull. 2021, 22, 15–18. [Google Scholar]
- Adamo, G.; Baccolini, V.; Massimi, A.; Barbato, D.; Cocchiara, R.; Di Paolo, C.; Mele, A.; Cianfanelli, S.; Angelozzi, A.; Castellani, F.; et al. Towards elimination of measles and rubella in Italy: Progress and challenges. PLoS ONE 2019, 14, e0226513. [Google Scholar] [CrossRef]
- Costantino, C.; Casuccio, A.; Sannasardo, C.E.; Vella, C.; Scarpitta, F.; Randazzo, M.A.; Foresta, A.; Casuccio, N.; Ventura, G.; Bono, S.E.; et al. Public health strategies adopted to manage the increase of accesses to vaccination services, as a result of the application of the law 119/2017. Acta Biomed. 2020, 91, 35–40. [Google Scholar] [CrossRef]
- Gianfredi, V.; D’Ancona, F.; Maraglino, F.; Cenci, C.; Iannazzo, S. Polio and measles: Reasons of missed vaccination in Italy, 2015-2017. Ann. Med. Prev. 2019, 31, 191–201. [Google Scholar]
- Gori, D.; Costantino, C.; Odone, A.; Ricci, B.; Ialonardi, M.; Signorelli, C.; Vitale, F.; Fantini, M.P. The impact of mandatory vaccination law in Italy on mmr coverage rates in two of the largest italian regions (Emilia-romagna and sicily): An effective strategy to contrast vaccine hesitancy. Vaccines 2020, 8, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signorelli, C.; Odone, A.; Cella, P.; Iannazzo, S. Childhood vaccine coverage in Italy after the new law on mandatory immunization. Ann. Ig. 2018, 30, 1–10. [Google Scholar] [PubMed]
- Signorelli, C.; Odone, A. Four Italian experiences on vaccination policies: Results and lessons. Ann. Med. Prev. 2019, 31, 36–44. [Google Scholar]
- Zanella, B.; Boccalini, S.; Bonito, B.; Del Riccio, M.; Tiscione, E.; Bonanni, P.; Bechini, A.; Working Group DHS; Working Group AOUMeyer; Working Group AUSLTC. Increasing measles seroprevalence in a sample of pediatric and adolescent population of tuscany (Italy): A vaccination campaign success. Vaccines 2020, 8, 512. [Google Scholar] [CrossRef]
- Heininger, U.; André, P.; Chlibek, R.; Kristufkova, Z.; Kutsar, K.; Mangarov, A.; Mészner, Z.; Nitsch-Osuch, A.; Petrovic, V.; Prymula, R.; et al. Comparative Epidemiologic Characteristics of Pertussis in 10 Central and Eastern European Countries, 2000–2013. PLoS ONE 2016, 11, e0155949. [Google Scholar] [CrossRef] [PubMed]
- Kantsone, I.; Lucenko, I.; Perevoscikovs, J. More than 20 years after re-emerging in the 1990s, diphtheria remains a public health problem in Latvia. Eurosurveillance 2016, 21, 30414. [Google Scholar] [CrossRef] [Green Version]
- Wagner, K.S.; White, J.M.; Lucenko, I.; Mercer, D.; Crowcroft, N.S.; Neal, S.; Efstratiou, A. Diphtheria in the postepidemic period, Europe, 2000-2009. Emerg. Infect. Dis. 2012, 18, 217–225. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Vaccine-Preventable Diseases: Monitoring System. 2020 Global Summary. 2020. Available online: http://apps.who.int/immunization_monitoring/globalsummary/ (accessed on 20 September 2021).
- Bukova, V.; Melnik, A.; Tsurcan, L.; Cheban, A.; Gutsu, V. Pertussis Outbreak Analysis in the Republic of Moldova. Epidemiol. Vaccinal Prev. 2017, 3, 96–101. [Google Scholar] [CrossRef] [Green Version]
- Melnik, A.A.; Bukova, V.E.; Tsurcan, L.P.; Furtuna, N.I. Characteristics of the Epidemiological Situation of Measles in the Period of its Elimination in Republic of Moldova. Epidemiol. Vaccinal Prev. 2019, 18, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Patić, A.; Štrbac, M.; Petrović, V.; Milošević, V.; Ristić, M.; Hrnjaković Cvjetković, I.; Medić, S. Seroepidemiological study of rubella in Vojvodina, Serbia: 24 years after the introduction of the MMR vaccine in the national immunization programme. PLoS ONE 2020, 15, e0227413. [Google Scholar] [CrossRef]
- Ristić, M.; Milošević, V.; Medić, S.; Malbaša, J.D.; Rajčević, S.; Boban, J.; Petrovic, V. Sero-epidemiological study in prediction of the risk groups for measles outbreaks in Vojvodina, Serbia. PLoS ONE 2019, 14, e0216219. [Google Scholar] [CrossRef] [Green Version]
- Public Health Center of the Ministry of Health of Ukraine. Vaccination Coverage. Available online: https://phc.org.ua/kontrol-zakhvoryuvan/imunizaciya/okhoplennya-scheplennyami (accessed on 20 September 2021).
- Legifrance. Décret n° 2018-42 du 25 Janvier 2018 Relatif à la Vaccination Obligatoire. In Off. J. French Republic; 2018. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000036543886 (accessed on 20 August 2021).
- Gesetz für den Schutz vor Masern und zur Stärkung der Impfprävention vom 20.02.2020. BGBl 2020, I, 148–157.
- Legge 31 Luglio 2017, n. 119. Conversione in Legge, con Modificazioni, del Decreto-Legge 7 Giugno 2017, n. 73, Recante Disposizioni Urgenti in Materia di Prevenzione Vaccinale. (17G00132). GU Serie Generale n. 182 del 05-08-2017. 2017. Available online: http://www.gazzettaufficiale.it/eli/id/2017/08/5/17G00132/sg (accessed on 20 August 2021).
- Vaccination Regulations. Cabinet Regulation No. 330. Adopted 26 September 2000. Available online: www.vvc.gov.lv/export/sites/default/docs/LRTA/Citi/Cab._Reg._No._330_-_Vaccination_Regulations.doc (accessed on 20 August 2021).
- Law of the Republic of Moldova. Law on State Supervision on Health. 2009. Available online: http://cis-legislation.com/document.fwx?rgn=27147 (accessed on 20 August 2021).
- Zakon o Zaštiti Stanovništva od Zaraznih Bolesti. Službeni Glasnik RS. 2016. Available online: http://www.pravno-informacioni-sistem.rs/SlGlasnikPortal/eli/rep/sgrs/skupstina/zakon/2016/15/8/reg (accessed on 20 August 2021).
- Law of Ukraine on Protecting the Population from Infectious Diseases. Available online: http://search.ligazakon.ua/l_doc2.nsf/link1/T001645.html (accessed on 20 August 2021).
- Lee, C.; Robinson, J.L. Systematic review of the effect of immunization mandates on uptake of routine childhood immunizations. J. Infect. 2016, 72, 659–666. [Google Scholar] [CrossRef]
- Adams, J.; Bateman, B.; Becker, F.; Cresswell, T.; Flynn, D.; McNaughton, R.J.; Oluboyede, Y.; Robalino, S.; Ternent, L.; Sood, B.G.; et al. Effectiveness and acceptability of parental financial incentives and quasi-mandatory schemes for increasing uptake of vaccinations in preschool children: Systematic review, qualitative study, and discrete choice experiment. Health Technol. Assess. 2015, 19, 1–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechini, A.; Boccalini, S.; Ninci, A.; Zanobini, P.; Sartor, G.; Bonaccorsi, G.; Grazzini, M.; Bonanni, P. Childhood vaccination coverage in Europe: Impact of different public health policies. Expert Rev. Vaccines 2019, 18, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Trentini, F.; Poletti, P.; Melegaro, A.; Merler, S. The introduction of “No jab, No school” policy and the refinement of measles immunisation strategies in high-income countries. BMC Med. 2019, 17, 86. [Google Scholar] [CrossRef] [PubMed]
- Vaz, O.M.; Ellingson, M.; Weiss, P.; Jenness, S.M.; Bardají, A.; Bednarczyk, R.A.; Omer, S.B. Mandatory vaccination in Europe. Pediatrics 2020, 145, e20190620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brujić, M. “Stick without a Carrot”: An Anthropological Analysis of the Daily Press on Mandatory MMR Immunization in Serbia. Issues Ethnol. Anthr. 2020, 15, 979–1006. [Google Scholar] [CrossRef]
- De Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Gallup, Inc. Over 1 Billion Worldwide Unwilling to Take COVID-19 Vaccine. Available online: https://news.gallup.com/poll/348719/billion-unwilling-COVID-vaccine.aspx (accessed on 20 August 2021).
- CNN. Russia Says People Can Decline Its Vaccine. But for Many, They’ll Get Fired if They Do. Available online: https://edition.cnn.com/2021/06/29/europe/russia-vaccine-voluntary-compulsory-cmd-intl/index.html (accessed on 20 August 2021).
- Decreto—Legge 31 1 Aprile 2021, n. 44. Misure Urgenti Per Il Contenimento Dell’epidemia da COVID-19, in Materia di Vaccinazioni Anti SARS-CoV-2, di Giustizia e di Concorsi Pubblici. (21G00056) (GU Serie Generale n.79 del 01-04-2021). Available online: https://www.gazzettaufficiale.it/eli/id/2021/04/01/21G00056/sg (accessed on 20 August 2021).
- BBC. France COVID: Vaccinations Mandatory for All Health Workers. Available online: https://www.bbc.com/news/world-europe-57814163 (accessed on 20 August 2021).
- El País. España Ya Ha Completado la Vacunación de más de la Mitad de Sus Habitantes. Available online: https://elpais.com/sociedad/2021-07-19/espana-ya-ha-completado-la-vacunacion-de-mas-de-la-mitad-de-sus-habitantes.html (accessed on 20 August 2021).












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Population | Study Period | Study Design | Vaccine/ Disease | Intervention | Outcomes | Results | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cohen R. et al. (2020) [11] | France | 1500 mothers of 0 to 17-month-old infants | 2017–2019 | Survey | Pertussis Hib HepB Measles- mumps- rubella (MMR) | Change from recommended to mandatory vaccination against 8 diseases for all children born from Jan 2018 | VC | VC against pertussis and Hib was high and stable in 2019 (≥ 94%) compared to previous years. Among 250 children aged 6 to 8 months old, HepB VC, significantly increased from 88.7% in 2017 to 96.6% in 2019 (P < 0.01). Among 250 children aged 9 to 11-month-old, HepB VC significantly increased from 87.8% to 95.7% between 2017 and 2019 (P < 0.01). Among 250 children aged 15 to 17 months, HepB VC significantly increased between 2017 and 2019 (from 86.1% to 93.0%, P < 0.05). MMR VC increased from 85.5% in 2017 to 89.5% in 2019. | |||||
| Lévy-Bruhl D. et al. (2019) [12] | France | Children born in 2015–2018 in France | 2016–2018 | Registry analysis | Hexavalent HepB MMR | Change from recommended to mandatory vaccination against 8 diseases for all children born from Jan 2018 | VC | Increase of VC against HepB from around 92% in 2017 to 98% in 2018. The increase in MMR first dose VC between 2017 and 2018 was 3.0%. This compared with a 0.3% gain in coverage between 2016 and 2017. The proportion of children under 1 year old, receiving a hexavalentvaccine increased from 93.1% in 2017 to 98.6% in 2018. | |||||
| Taine M. et al. (2021) [13] | France | Children ≤24 months old | 2019–2020 | Registry analysis | Penta/HexavalentMMR | Change from recommended to mandatory vaccination against 8 diseases for all children born from Jan 2018 | VC, Vaccine dispensation | During the first 4 weeks of the first lockdown, the observed priming dose counts substantially decreased (RD: from −5.7% (95% CI −6.1; −5.2) for penta/hexavalent to −25.2% (95% CI −25.6; −24.8) for MMR), as did the booster counts (RD:−15.3% (95%CI −15.9; −14.7)) for penta/hexavalent. During 2020, MMR priming doses had the greatest shortfalls (n = 84,893). The number of booster dispensations between March 16 and December 20, 2020 had shortfalls reaching 21,140 doses of penta/hexavalent (RD −4.5% (95% CI −4.8; −4.2)). | |||||
| Matysiak-Klose D. et al. (2021) [14] | Germany | The population of Germany | 2018–2021 | Registry analysis | Rubella Measles | The law for protection against measles and to strengthen vaccination prevention in force since 1 March 2020. | Incidence | The number of reported rubella cases had consolidated at a low level in 2018 and 2019 (n = 58). In 2020: 18 rubella cases. In December 2020 Germany was granted an interruption of the endemic transmission for 36 months with retroactive effect for the years 2017 to 2019 and thus, the status of elimination of the rubella. 2018 (n = 545 measles cases) and 2019 (n = 515 measlescases). In 2020, 76 measles cases registered, decrease by 85.5% compared to previous years since 2016. | |||||
| Neugebauer M. et al. (2020) [15] | Germany | 1594 adults | 20 October 2019 to 24 April 2020 | Survey | Measles | The law for protection against measles and to strengthen vaccination prevention in force since 1 March 2020. | Incidence, VC | 19.3% of the participants were affected by the Measles Protection Act. Of these, only 77.5% had an immunity against measles, 14.0% wanted to be fully vaccinated against measles when the measles protection law came into force, whereby an immunity of 91.5% could be achieved. Assuming that participants with an unclear vaccination status or measles disease are immune, an immunity of > 95% is achieved. 86.4% of the children (2–17 years) had immune protection. The willingness of parents to have their children vaccinated because of the sanctions of the Measles Protection Act was only 0.8%. | |||||
| Robert Koch Institute (2021) [7] | Germany | The population of Germany | 2019–2020 | Registry analysis | Diphtheria Pertussis HepB Hib Measles Mumps Rubella Varicella | The law for protection against measles and to strengthen vaccination prevention in force since 1 March 2020. | Incidence | Cases n | 2019 | 2020 | |||
| Measles | 515 | 75 | |||||||||||
| Rubella | 18 | 7 | |||||||||||
| Diphtheria | 15 | 16 | |||||||||||
| Pertussis | 10,315 | 3451 | |||||||||||
| HepB | 8941 | 6695 | |||||||||||
| Hib | 955 | 480 | |||||||||||
| Mumps | 593 | 338 | |||||||||||
| Varicella | 22,681 | 11,250 | |||||||||||
| Robert Koch Institute (2021) [16] | Germany | The population of Germany | 2020–2021 | Registry analysis | Diphtheria Pertussis HepB Hib Measles Mumps Rubella Varicella | The law for protection against Measles and to strengthen vaccination prevention in force since March 1, 2020. | Incidence | Cases n | Jan–May 2020 | Jan–May 2021 | |||
| Measles | 75 | 4 | |||||||||||
| Rubella | 4 | 2 | |||||||||||
| Diphtheria | 9 | 0 | |||||||||||
| Pertussis | 2895 | 290 | |||||||||||
| HepB | 2942 | 3061 | |||||||||||
| Hib | 387 | 77 | |||||||||||
| Mumps | 265 | 38 | |||||||||||
| Varicella | 7300 | 2200 | |||||||||||
| Adamo G. et al. (2019) [17] | Italy | The population of Italy | 2013–2018 | Registry analysis | Measles Rubella | Extension of the number of mandatory vaccinations, for school attendance, from four to ten in July 2017. | Incidence, VC | In 2017, measles incidence increased to 88.4/106 population. In 2018, measles incidence was 43.3 /106 population. Rubella: incidence remained relatively low over the period considered. Congenital rubella syndrome: one case has been reported in Italy since 2014. Vaccination coverage for measles-containing vaccine increased by 5.7 percentage points in 2018 compared to 2016 with regard to the 1st dose (87.3% in 2016 vs 93.0% in 2018) and by 6.6 percentage points with regard to the 2nd dose (82.2% in 2016 vs 88.9% in 2018). Similar trend observed for the first and second doses of rubella-containing vaccine. | |||||
| Costantino C. et al. (2020) [18] | Italy | Children < 7 years old in Palermo | 2016–2018 | Registry analysis | Hexavalent Measles-mumps-rubella-varicella (MMRV) | Extension of the number of mandatory vaccinations, for school attendance, from four to ten in July 2017. | VC | Full cycle hexavalent coverage rates showed an increase of 1.4% and 2.5% at 24 and 36 months respectively, from 2016 to 2018. Moreover, in the same period, a 7.2% and a 10.5% increase of adherence to first dose of MMRV were observed at 24 and 36 months, respectively. Vaccination coverage rates for full vaccination cycle of MMRVin the Palermo Local Health Unit, among 6 years old children, showed an increase from 61% to 89.7% (+28.7%) from 2016 to 2018. | |||||
| Gianfedi V. et. al. (2019) [19] | Italy | Children < 24 months of age | 2015–2017 | Survey | Measles Polio | Extension of the number of Mandatory vaccinations, for school attendance, from four to ten in July 2017. | VC | Decrease in missed vaccination after the introduction of mandatory law for both polio and measles (−4.1%) with the consequent increase of VC. For measles vaccination the reason “found/contacted, but did not attend the appointment” was the most frequent (mean value 3.2%; 3.7% in 2015, 3.7% in 2016, and 2.3% in 2017), followed by “definitive informed dissent” (mean value 2.9%; 4.0% in 2015, 3.0% in 2016 and 1.8% in 2017). | |||||
| Gori D. et al. (2020) [20] | Italy | Children < 8 years old in Emilia- Romagna and Sicily regions | 2009–2018 | Registry analysis | MMR | Extension of the number of Mandatory vaccinations, for school attendance, from four to ten in July 2017. | VC | Observed 4.1% increase in Emilia-Romagna and 6.4% increase in Sicily in VC for MMR in 2017, and an additional 2.5% in Emilia-Romagna and 5.3% in Sicily in 2018. Both regions showed similar results; they achieved the lowest coverage rates in 2015 and showed an increase in the VC after the introduction of mandatory vaccinations. In 2018, both reached the starting point before the decrease. | |||||
| Signorelli C. et al. (2018) [21] | Italy | The population of Italy | 2000–2017 | Registry analysis | Polio Tetanus Diphtheria Pertussis HepB Hib Measles Mumps Rubella | Extension of the number of Mandatory vaccinations, for school attendance, from four to ten in July 2017. | VC | VC has increased since 2016 for both mandatory and recommended childhood vaccines. The increase has been consistent—although at different rates—in all regions and is highest for MMR, as compared to other vaccines. | |||||
| VC | 2016 | 2017 | |||||||||||
| Polio | 93.3 | 94.5 | |||||||||||
| Tetanus | 93.7 | 94.6 | |||||||||||
| Diphtheria | 93.6 | 94.6 | |||||||||||
| Pertussis | 93.6 | 94.6 | |||||||||||
| HepB | 93 | 94.3 | |||||||||||
| Hib | 93.1 | 94.2 | |||||||||||
| Measles | 87.3 | 91.7 | |||||||||||
| Mumps | 87.2 | 91.6 | |||||||||||
| Rubella | 87.2 | 91.6 | |||||||||||
| Signorelli C. et al. (2019) [22] | Italy | Children ≤ 24 months of age in Italy | 2000–2018 | Registry analysis | Poliomyelitis MMR |
| VC |
| |||||
| Zanella B. et al. (2020) [23] | Italy | Pediatric and adolescent (1–18 years) residents of the province of Florence | December 2017– April 2018 | Retrospective | Measles | Since 2017, the anti-measles Vaccination Became Compulsory in minors (0–16 years) for school attendance. | Seropreva-lence | No measles notification was reported. The overall seropositivity was 88.5%, and highest immunity level was found in the 5–9-year-old subjects (97.9%). Comparing these results with two serosurveys carried out in 2003 and 2005–2006, the current study highlighted a dramatic decrease in susceptibility towards measles (8.5%), with a lower value than in 2003 (30.8%) and in 2005–2006 (25.5%). The recent decrease in the susceptibility towards measles in the pediatric and adolescent population of Tuscany, together with the increased measles seroprevalence, is mainly due to all the preventive measures implemented in Italy. | |||||
| Heininger U. et al. (2016) [24] | Multi-country. Data on Latvia extracted | The population of Latvia | 2000–2013 | Registry analysis | Pertussis | Adoption in 2000 of “Vaccine Regulation” No. 330 which specifies that vaccination shall be mandatory for children against 10 vaccine-preventable diseases. | Incidence, VC | VC: From 1958 to 2004: 89.7–94.7% From 2005 to 2009: 92.3–98.1% Since 2010: 90.0–97.9% Approximately ten-fold decrease in the reported annual pertussis incidence rate between 2000 and 2011, before a dramatic increase in 2012. Over the period, the annual incidence of reported pertussis cases ranged from 0.4 to 13 cases per 100,000 population. | |||||
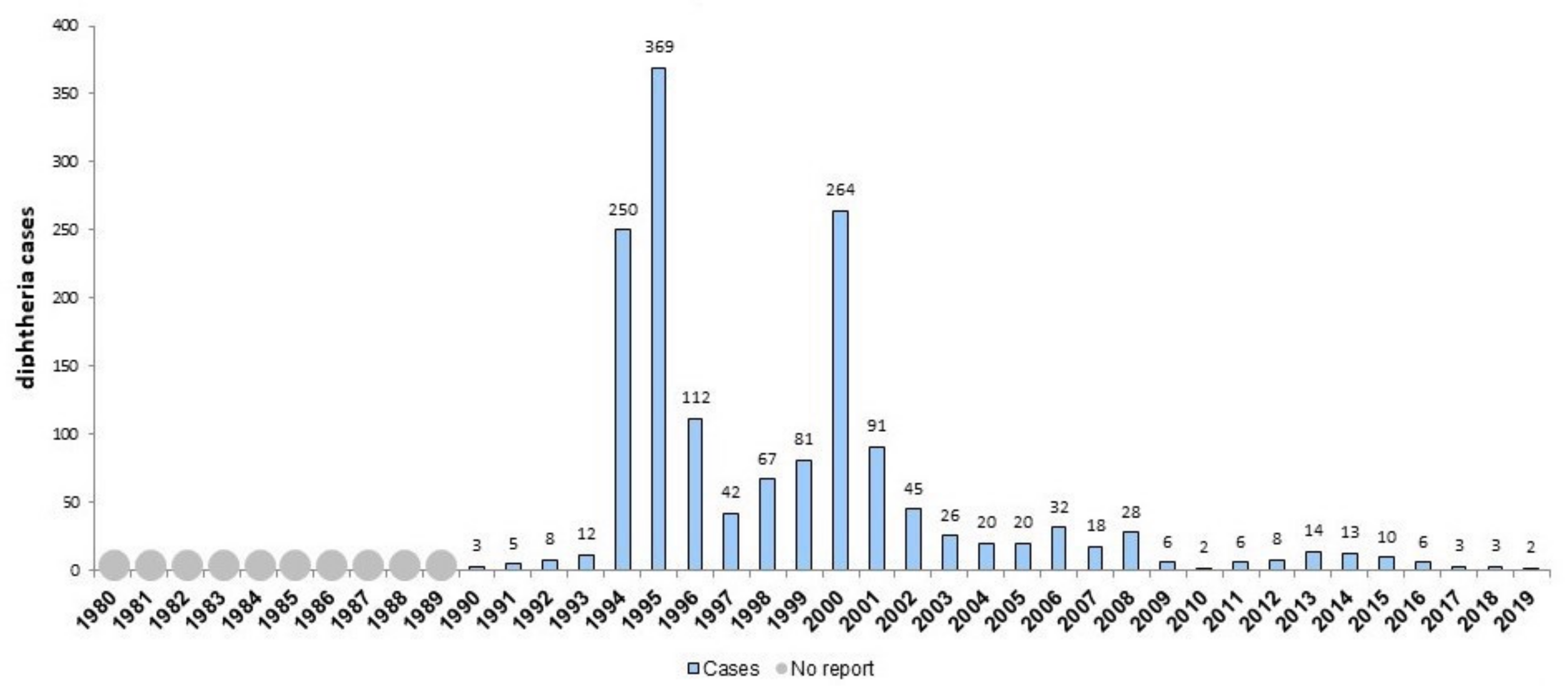
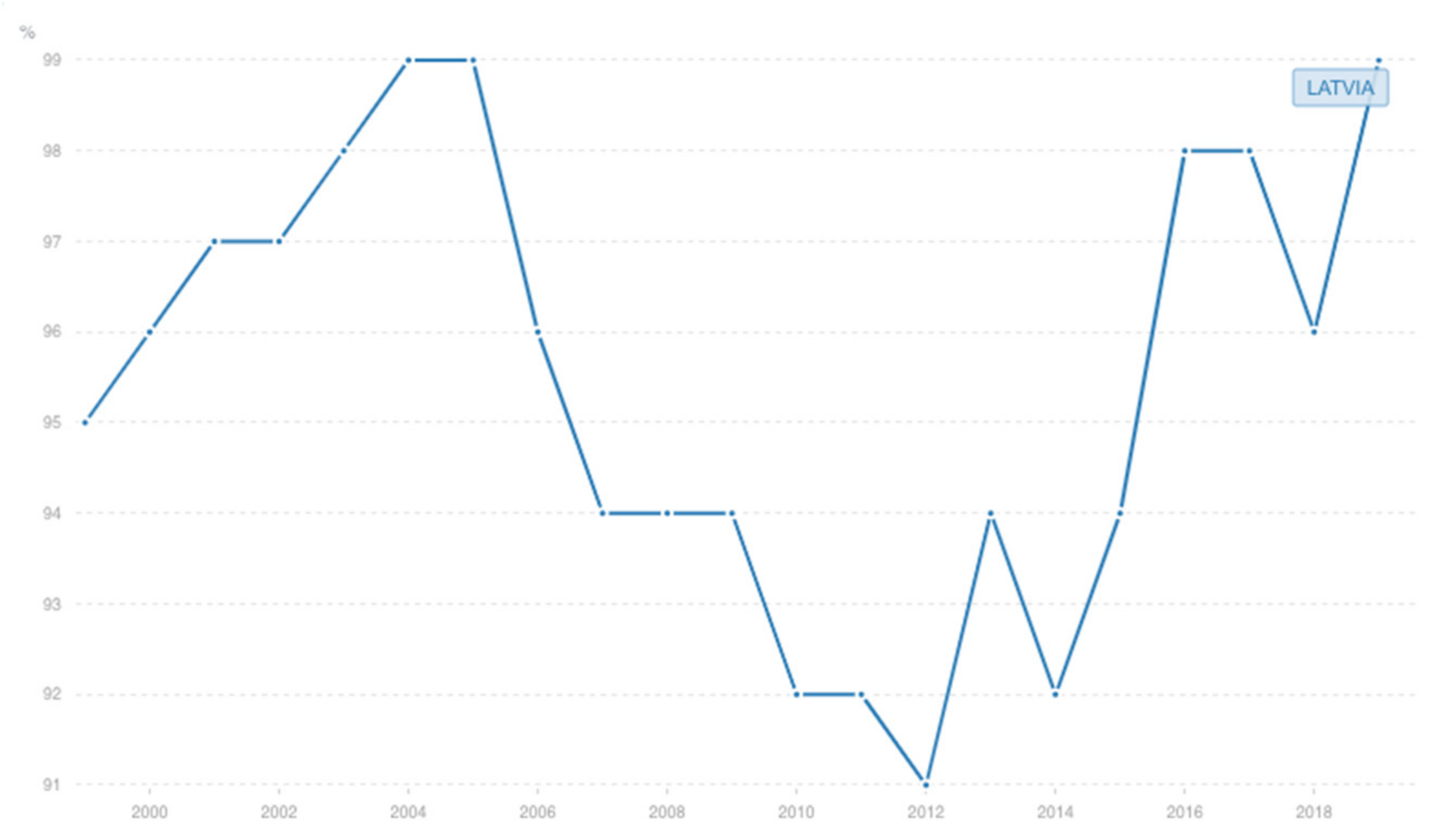
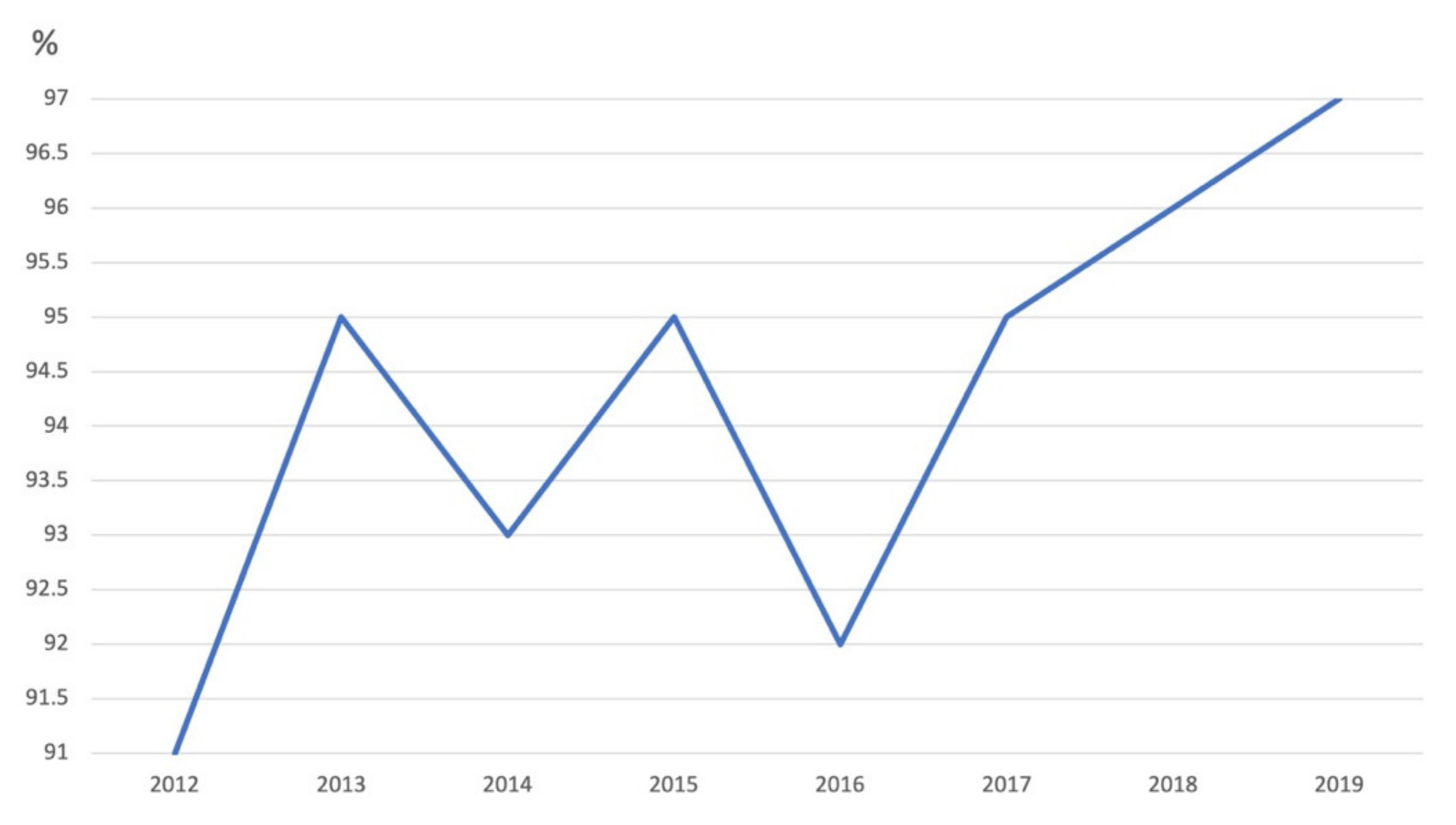
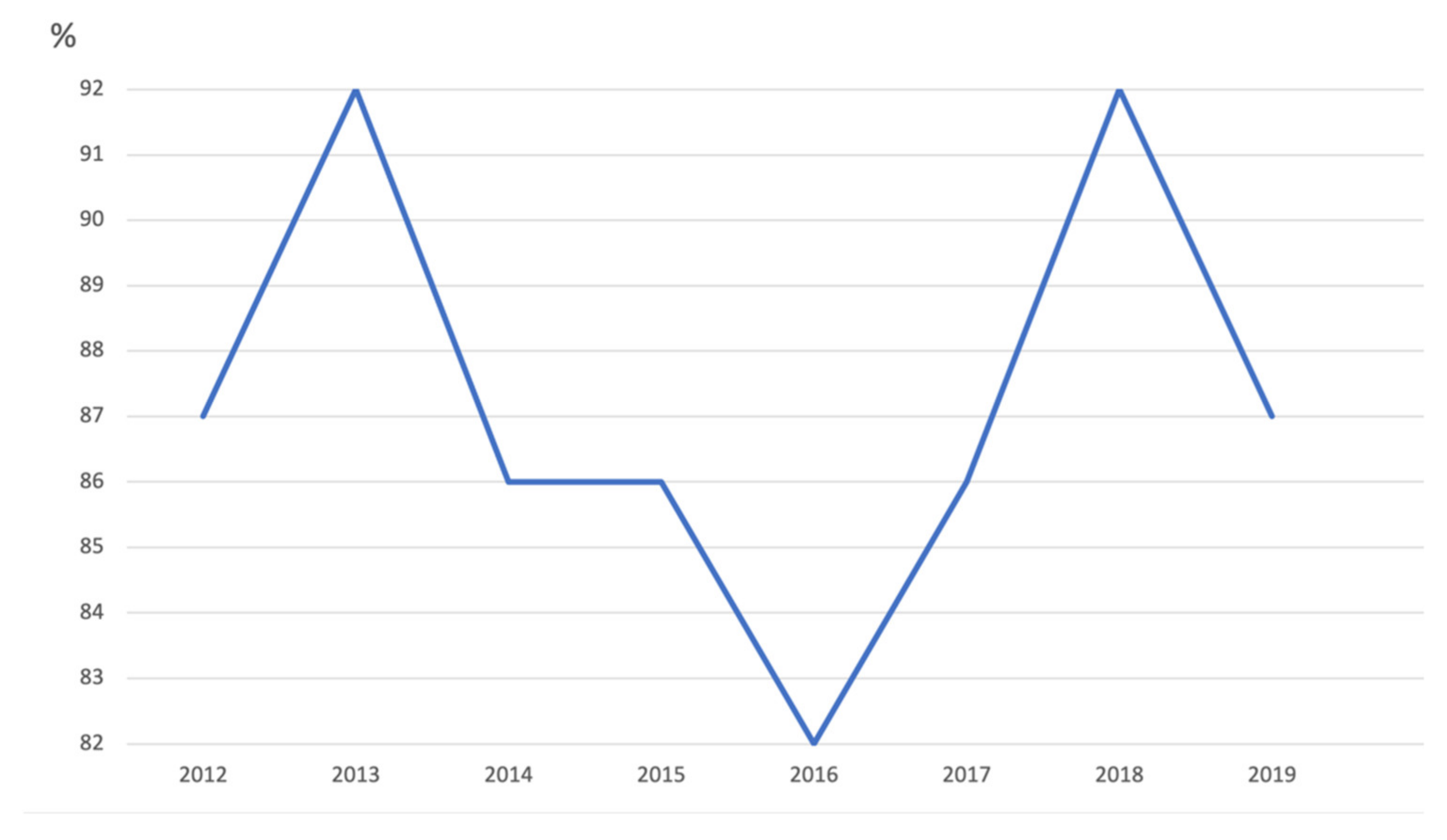
| Kantsone I. et al. (2016) [25] | Latvia | The population of Latvia | 1994–2014 | Registry analysis | Diphtheria | Adoption in 2000 of “Vaccine Regulation” No. 330 which specifies that vaccination shall be mandatory for children against 10 vaccine-preventable diseases. | Incidence, VC | Increasing incidence observed in 2000 (11.1/100,000). From 2000 to 2014, childhood VC with a third dose ranged from 91% to 98% and with a fifth dose from 92% to 98%. From 2000 to 2014, VC for adolescents (sixth dose at 15 years) ranged from 86% to 96%, decrease in coverage occurred from 96% in 2007 to 86% in 2014. Incidence increased from 0.1 per 100,000 inhabitants in 2010 to 0.7 in 2013. No cases in children were observed from 2009 to 2011, but new cases have emerged since 2012. Most cases occurred in adults. | |||||
| Wagner K. et al. (2012) [26] | Multi-country. Data on Latvia extracted | The population of Latvia | 2000–2009 | Registry analysis | Diphtheria | Adoption in 2000 of “Vaccine Regulation” No. 330 which specifies that vaccination shall be mandatory for children against 10 vaccine-preventable diseases. | Incidence, N of deaths | Diphtheria incidence decreased in Latvia from 111.22/million in 2000 to 2.67/million in 2009. During 2000–2009, a total of 32 deaths caused by diphtheria were reported in Latvia. 64 patients in Latvia recorded as fully vaccinated had classic respiratory diphtheria symptoms. Most of these patients were infected during a military outbreak in 2000 and would have been scheduled for primary vaccinations during the 1980s, when changes led to less intensive vaccination of children in the former Soviet Union. | |||||
| World Health Organization (2020) [27] | Latvia | The population of Latvia | 1980–2019 | Registry analysis | Diphtheria Tetanus Pertussis (DTP) HepB Hib Measles Mumps Rubella Polio Measles- containing vaccine (MCV) | Adoption in 2000 of “Vaccine Regulation” No. 330 which specifies that vaccination shall be mandatory for children against 10 vaccine-preventable diseases. | VC, incidence | VC | 2002 | 2001 | 2000 | 1999 | 1998 |
| DTP1 | 99 | 100 | 100 | 93 | 99 | ||||||||
| DTP3 | 97 | 97 | 96 | 95 | 94 | ||||||||
| HepB3 | 98 | 96 | 95 | 94 | 9 | ||||||||
| Hib3 | 87 | 84 | 79 | 76 | 47 | ||||||||
| MCV1 | 98 | 98 | 97 | 97 | 97 | ||||||||
| Pol3 | 98 | 97 | 96 | 95 | 94 | ||||||||
| Cases n | |||||||||||||
| Diphtheria | 45 | 91 | 264 | 81 | 67 | ||||||||
| Measles | - | 1 | 0 | 0 | 3 | ||||||||
| Mumps | 231 | 6834 | 1949 | 41 | - | ||||||||
| Pertussis | 159 | 160 | 135 | 55 | 149 | ||||||||
| Rubella | 2578 | 358 | 62 | 91 | - | ||||||||
| Tetanus | 1 | 2 | 3 | 1 | |||||||||
| Bukova V. et al. (2017) [28] | Moldova | The population of Moldova | 1993–2016 | Registry analysis | Pertussis | From 2009 children are required to receive all vaccines in the national schedule to enroll in kindergartens and schools. | Incidence, VC | Reduction of incidence in 2009–2010 from 48 to 31 cases with increase in incidence in the following years. In 2009–2013 vaccination coverage was above 90%, and under 90% in the following years. The lowest incidence for the analyzed years was observed in 2005–2010—within 24 to 48 cases annually. Progressive reduction of the vaccine coverage observed in 2008–2015, from 95.4 to 89.7%, caused an increase in the incidence. | |||||
| Melnik A. et al. (2019) [29] | Moldova | The population of Moldova | 2000–2018 | Registry analysis | Measles | From 2009 children are required to receive all vaccines in the national schedule to enroll in kindergartens and schools. | Incidence, VC | In 2003–2017, the incidence dropped sharply, with a total of 181 cases of measles reported. No measles cases were reported in 2008–2011 and in 2015–2017. MMR1 VC: gradual decrease in 2003–2017, the lowest rate is observed in 2017—87.1%. In 2009–2012 VC was stable at the level of 90%. Moldova achieved the status of a country that eliminated measles in 2008–2017. Among the cases, children from one to ten years predominate (66.1%), cases among children under one year old (8.2%), adolescents (17.5%) and adults (8.2%). | |||||
| World Health Organization (2020) [27] | Moldova | The population of Moldova | 1980–2019 | Registry analysis | Diphtheria Tetanus Pertussis HepB Hib Measles Mumps Rubella Polio | From 2009 children are required to receive all vaccines in the national schedule to enroll in kindergartens and schools. | VC, incidence | VC | 2011 | 2010 | 2009 | 2008 | 2007 |
| DTP1 | 96 | 93 | 95 | 96 | 95 | ||||||||
| DTP3 | 93 | 90 | 94 | 90 | 92 | ||||||||
| HepB3 | 96 | 98 | 95 | 97 | 95 | ||||||||
| Hib3 | 78 | 63 | 94 | - | - | ||||||||
| MCV1 | 91 | 97 | 91 | 95 | 96 | ||||||||
| MVC2 | 97 | 98 | 98 | 97 | 95 | ||||||||
| Pol3 | 96 | 97 | 95 | 96 | 93 | ||||||||
| Cases n | |||||||||||||
| Diphtheria | 0 | 0 | 1 | 0 | 0 | ||||||||
| Measles | 0 | 0 | 0 | 0 | 10 | ||||||||
| Mumps | 143 | 144 | 292 | 29783 | 1757 | ||||||||
| Pertussis | 102 | 31 | 47 | 30 | 36 | ||||||||
| Rubella | 0 | 0 | 1 | 1 | 3 | ||||||||
| Tetanus | 0 | 2 | 0 | 0 | 0 | ||||||||
| Patić A. et al. (2020) [30] | Serbia | 3404 participants from Vojvodina Province aged 0–84 | May 2015– December 2017 | Retrospective | Rubella | At the beginning of 2016, the National Assembly adopted a Law on Protection of the Population from Infectious Diseases, mandating vaccination. | Incidence, seroprevalence, VC | From 2008 to 2017, only three cases of rubella were reported (in 2009, in 2012, and in 2015). The highest number of seronegatives was in the youngest (1 year) age group (44.7%), followed by the group aged 24–49 (6.4%) and 2–11 years (6.2%). In the group of children aged 2–11 years, the level of anti-rubella IgG antibodies was higher since any of them have received both doses of the MMR vaccine. VC in Vojvodina was lower than 95% in 2012 (91%), 2014 (86%), 2015 (90%), 2016 (89%), and 2017 (78%). Coverage with the second dose of MMR increased significantly since 2015: 2015 (83,7%), 2016 (90,9%), 2017 (93,2%). | |||||
| Ristić M et al.(2019) [31] | Serbia | 3199 residents of Vojvodina province aged 12 months and older | April 2015–June 2017 | Retrospective | Measles | At the beginning of 2016, the National Assembly adopted a Law on Protection of the Population from Infectious Diseases, mandating vaccination. | Incidence, seroprevalence, VC | Declining trend of measles incidence in Vojvodina in 1948–2017 was observed with wide variation in annual notification rates from 768.8/100,000 in 1970 to 0 during 12 different periods/years (2001–2006, 2008–2011, 2012, and 2016). VC for both MMR1 and MMR2 vaccines in Vojvodina increased from 78% and 93% (at the end of 2017) to 90% and 94% (during the first two months of 2018), respectively. Findings showed that the main susceptible age group for measles transmission in the province are the subjects aged 20–39 years. | |||||
| World Health Organization (2020) [27] | Serbia | The population of Serbia | 1980–2019 | Registry analysis | Diphtheria Tetanus Pertussis HepB Hib Measles Mumps Rubella Polio | At the beginning of 2016, the National Assembly adopted a Law on Protection of the Population from Infectious Diseases, mandating vaccination. | VC, incidence | VC | 2019 | 2018 | 2017 | 2016 | 2015 |
| DTP3 | 97 | 97 | 95 | 93 | 95 | ||||||||
| HepB3 | 94 | 91 | 93 | 91 | 94 | ||||||||
| Hib3 | 97 | 97 | 95 | 92 | 95 | ||||||||
| MCV1 | 87 | 93 | 86 | 82 | 87 | ||||||||
| MVC2 | 91 | 90 | 91 | 90 | 87 | ||||||||
| Pol3 | 97 | 97 | 95 | 93 | 95 | ||||||||
| Cases n | |||||||||||||
| Measles | 22 | 5076 | 721 | 11 | 383 | ||||||||
| Mumps | - | 13 | 37 | 40 | 41 | ||||||||
| Pertussis | - | 351 | 285 | 148 | 89 | ||||||||
| Rubella | - | 5 | 5 | 5 | 10 | ||||||||
| Tetanus | - | 0 | 2 | 4 | 4 | ||||||||
| Public Health Center of the Ministry of Health of Ukraine (2021) [32] | Ukraine | The population of Ukraine | 2017–2020 | Registry analysis | Polio DTP HepB Hib MMR | From 2019, unvaccinated children are prohibited from attending educational institutions. | VC | VC | 2020 | 2019 | 2018 | ||
| DTP | 80.1 | 80.5 | 69 | ||||||||||
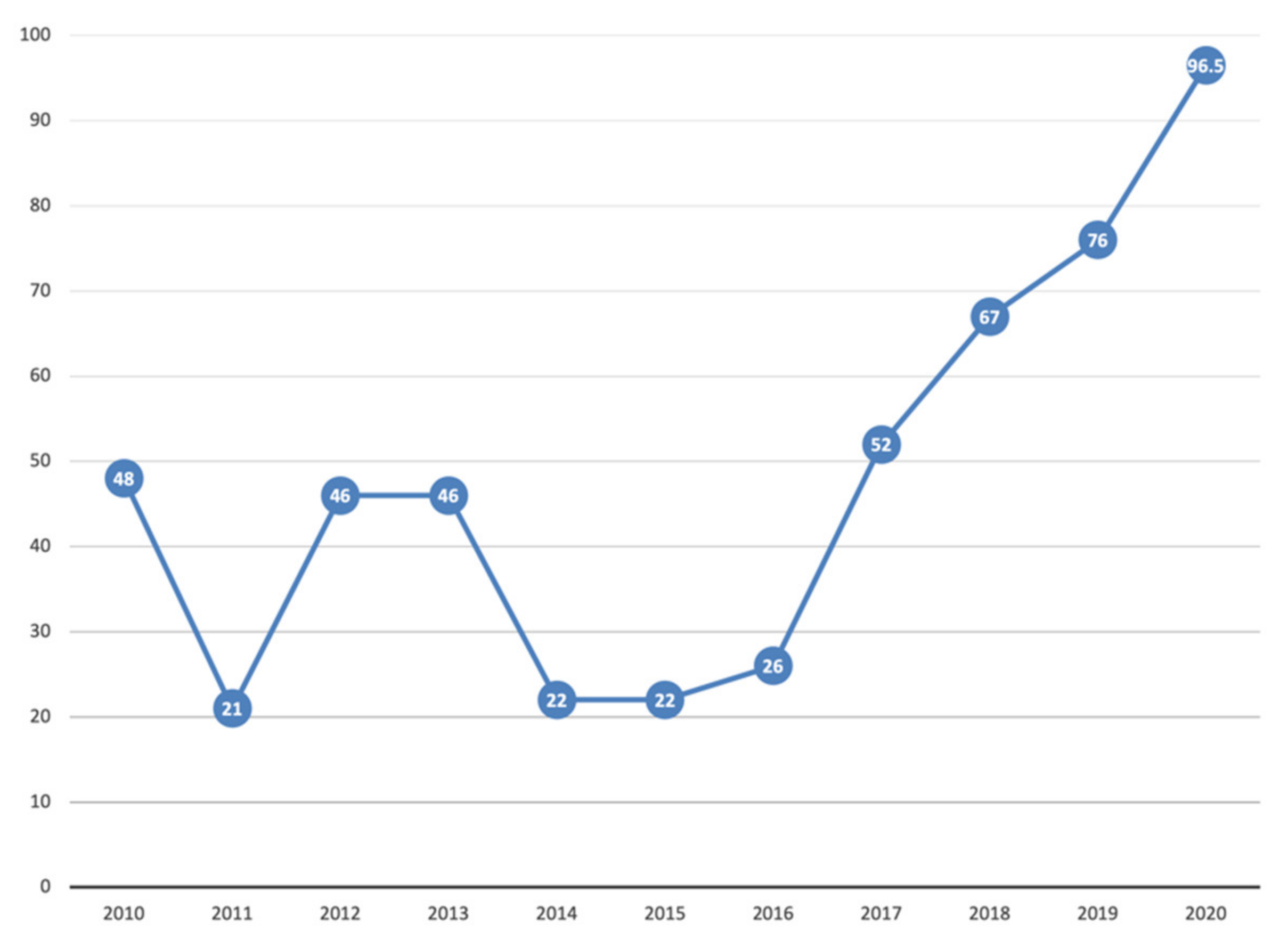
| HepB | 96.5 | 76 | 67 | ||||||||||
| Hib | 83.6 | 80 | 58 | ||||||||||
| MMR1 | 83.3 | 93.2 | 91 | ||||||||||
| Polio | 83 | 78.4 | 71 | ||||||||||
| Public Health Center of the Ministry of Health of Ukraine (2021) [8] | Ukraine | The population of Ukraine | 2018–2021 | Registry analysis | Tetanus Diphtheria Pertussis Hepatitis B Hib Measles Mumps Rubella | From 2019, unvaccinated children are prohibited from attending educational institutions. | Incidence | Cases/100,000 | 2020 | 2019 | 2018 | ||
| Measles | 0.63 | 135 | 125 | ||||||||||
| Mumps | 0.39 | 0.90 | 0.92 | ||||||||||
| Pertussis | 2.48 | 5.48 | 5.22 | ||||||||||
| Rubella | 0.09 | 0.33 | 0.55 | ||||||||||
| HepB | 1.74 | 3.11 | 3.42 | ||||||||||
| Cases n | |||||||||||||
| Tetanus | 12 | 15 | 18 | ||||||||||
| Diphtheria | 0 | 21 | 10 | ||||||||||
| Hib | 10 | 25 | 75 | ||||||||||
| Vaccine | 2018 | 2019 | 2020 |
|---|---|---|---|
| Hexavalent, 3 doses at 21 months | 84.1% | 90.3% | 90.5% |
| Hexavalent, including HepB among children vaccinated against diphtheria, tetanus, and polio, 1 dose at 8 months | 96.4% | 99.1% | 99.4% |
| MMR, 1 dose at 12 months | 90.8% | 92.5% | 92.2% |
| MMR, 2 doses at 33 months | 81.6% | 83.1% | 84% |
| Disease | January–May 2019 | January–May 2020 | January–May 2021 |
|---|---|---|---|
| Measles N cases | 422 | 75 | 4 |
| Mumps N cases | 210 | 265 | 38 |
| Rubella N cases | 10 | 4 | 2 |
| Vaccine/Disease | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|
| Measles VC, 1 dose at 24 months | 87.3% | 91.7% | 93% | 94.5% |
| Polio VC, 3 doses at 24 months | 93.3% | 94.5% | 95.1% | 95% |
| Measles N cases | 862 | 5404 | 2682 | 1622 |
| Mumps N cases | 782 | 829 | 777 | 587 |
| Rubella N cases | 30 | 68 | 21 | 23 |
| Vaccine | 1998 | 1999 | 2000 | 2001 | 2002 |
|---|---|---|---|---|---|
| DTP1 | 99% | 93% | 100% | 100% | 99% |
| DTP, 3 doses at 12 months | 94% | 95% | 96% | 97% | 97% |
| HepB, 3 doses at 12 months | 9% | 94% | 95% | 96% | 98% |
| Hib, 3 doses at 12 months | 47% | 76% | 79% | 84% | 87% |
| Measles, 1 dose at 12 months | 97% | 97% | 97% | 98% | 98% |
| Polio, 3 doses at 12 months | 94% | 95% | 96% | 97% | 98% |
| Disease, N cases | |||||
| Diphtheria | 67 | 81 | 264 | 91 | 45 |
| Measles | 3 | 0 | 0 | 1 | - |
| Mumps | - | 41 | 1949 | 6834 | 231 |
| Pertussis | 149 | 55 | 135 | 160 | 159 |
| Rubella | - | 91 | 62 | 358 | 2578 |
| Tetanus | 1 | 3 | 2 | 1 |
| Vaccine | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|
| DTP1 | 95 | 96 | 95 | 93 | 96 |
| DTP, 3 doses at 12 months | 92 | 90 | 94 | 90 | 93 |
| HepB, 3 doses at 12 months | 95 | 97 | 95 | 98 | 96 |
| Hib, 3 doses at 12 months | - | - | 94 | 63 | 78 |
| Measles, 1 dose at 12 months | 96 | 95 | 91 | 97 | 91 |
| Measles, 2 doses at 7 years of age | 95 | 97 | 98 | 98 | 97 |
| Polio, 3 doses at 12 months | 93 | 96 | 95 | 97 | 96 |
| Disease, N cases | |||||
| Diphtheria | 0 | 0 | 1 | 0 | 0 |
| Measles | 10 | 0 | 0 | 0 | 0 |
| Mumps | 1757 | 29,783 | 292 | 144 | 143 |
| Pertussis | 36 | 30 | 47 | 31 | 102 |
| Rubella | 3 | 1 | 1 | 0 | 0 |
| Tetanus | 0 | 0 | 0 | 2 | 0 |
| Vaccine | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|
| DTP, 3 doses at 12 months | 95 | 93 | 95 | 97 | 97 |
| HepB, 3 doses at 12 months | 94 | 91 | 93 | 91 | 94 |
| Hib, 3 doses at 12 months | 95 | 92 | 95 | 97 | 97 |
| Measles, 1 dose at 12 months | 87 | 82 | 86 | 93 | 87 |
| Measles, 2 doses at 7 years of age | 87 | 90 | 91 | 90 | 91 |
| Polio, 3 doses at 12 months | 95 | 93 | 95 | 97 | 97 |
| Disease, N cases | |||||
| Measles | 383 | 11 | 721 | 5076 | 22 |
| Mumps | 41 | 40 | 37 | 13 | - |
| Pertussis | 89 | 148 | 285 | 351 | - |
| Rubella | 10 | 5 | 5 | 5 | - |
| Tetanus | 4 | 4 | 2 | 0 | - |
| Vaccine | 2018 | 2019 | 2020 |
|---|---|---|---|
| DTP, 3 doses at 12 months | 69 | 80.5 | 80.1 |
| HepB, 3 doses at 12 months | 67 | 76 | 96.5 |
| Hib, 3 doses at 12 months | 58 | 80 | 83.6 |
| Measles, 1 dose at 12 months | 91 | 93.2 | 83.3 |
| Polio, 3 doses at 12 months | 71 | 78.4 | 83 |
| Disease, N cases | |||
| Diphtheria | 10 | 21 | 0 |
| Measles | 53,219 | 57,282 | 264 |
| Mumps | 392 | 382 | 163 |
| Pertussis | 2214 | 2314 | 1041 |
| Rubella | 235 | 138 | 36 |
| HepB | 1449 | 1312 | 731 |
| Tetanus | 18 | 15 | 12 |
| Hib | 75 | 25 | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuznetsova, L.; Cortassa, G.; Trilla, A. Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunization Programs in Europe: A Systematic Review of the Literature. Vaccines 2021, 9, 1173. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101173
Kuznetsova L, Cortassa G, Trilla A. Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunization Programs in Europe: A Systematic Review of the Literature. Vaccines. 2021; 9(10):1173. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101173
Chicago/Turabian StyleKuznetsova, Lidia, Giorgio Cortassa, and Antoni Trilla. 2021. "Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunization Programs in Europe: A Systematic Review of the Literature" Vaccines 9, no. 10: 1173. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9101173