1. Introduction
COVID-19 vaccines, which became available at the very end of 2020, have brought new hope to the fight against the pandemic [
1]. The vaccines have been shown to have a good safety profile and efficacy against symptomatic SARS-CoV-2 infection [
2,
3,
4,
5]. The production of specific antibodies starts a few weeks after the first dose, but a second dose is required for optimal protection against COVID-19 [
6,
7,
8]. As recently shown among those hospitalized due to COVID-19 in the first half of 2021, infections among vaccinated people are sporadic [
9]. Recent studies suggest that humoral immunity against SARS-CoV-2, associated with natural infection or vaccination, may persist for more than six months, but specific antibody levels decline over time [
7]. However, we must bear in mind that a large proportion of those vaccinated had previously experienced COVID-19 even before vaccination, gaining an additional immunogenic stimulus that could imitate the third dose of the vaccine. Unfortunately, the level of antibodies providing an effective barrier against SARS-CoV-2 infection has not yet been established. Despite the attempts to standardize the quantification of the level of antibodies, the tests of individual manufacturers present their concentration in various reference ranges and units. This makes it difficult to compare test results and conduct retrospective multicenter, real-world analyses, which do not use a central laboratory.
The current study aimed to determine to what extent prior COVID-19 infection affects the response of specific antibodies following vaccination.
2. Materials and Methods
The retrospective study involved 173 health workers (30 men and 143 women) aged 50.1 ± 10.3 years from six hospitals who completed an entire two-dose vaccination course (21 days apart) with BNT162b2 (BioNTech, Mainz, Germany and Pfizer, New York, USA) between January 18 and March 18, 2021. Of these, 40 had previously experienced symptomatic COVID-19 (C+) (mean: 102 ± 90 days), which was not the case for the remaining 133 participants (C−). The level of anti-spike (anti-SARS-CoV-2 S1S2 IgG; anti-S) antibodies was determined six months (+/−1 month) after the second vaccination dose. In addition, in some cases, anti-spike receptor binding domain antibodies (anti-SARS-CoV-S-RBD IgG; anti-S-RBD) were additionally measured. The study included consecutive anonymous samples obtained from volunteer hospital workers available six months (+/−1 month) after the end of the vaccination course. Due to the retrospective and anonymous nature of the study, it did not require authorization. The antibody level was measured using different methods and different normal ranges. The antibody levels are shown as multiple cut-off values determined for a positive result for a given diagnostic method. This was due to the fact that the tests were carried out in different hospitals whose laboratories used reagents from various manufacturers. Unfortunately, to date, the producers have not standardized the units and the way of interpreting the results. However, for each test, the manufacturers provide a cut-off value above which the result is considered positive. In an attempt to ensure comparability of the results obtained using different methods, we considered this cut-off value as a kind of universal unit and the multiple of its excess as the level of antibodies observed in a given person. Statistical analysis was performed using the chi-square test.
3. Results
A level exceeding the cut-off values for both anti-S and anti-S-RBD antibodies was observed in 100% of subjects, and almost the same result was obtained when doubling the cut-off level (
Figure 1). However, after setting the analysis to 5- and 10-fold cut-off levels, the percentage of subjects meeting this criterion was significantly higher for the anti-S-RBD measurement and exceeded 90%. This difference disappeared at the 100-fold cut-off level, with anti-S and anti-S-RBD achieving only 21% and 16%, respectively (
Figure 1).
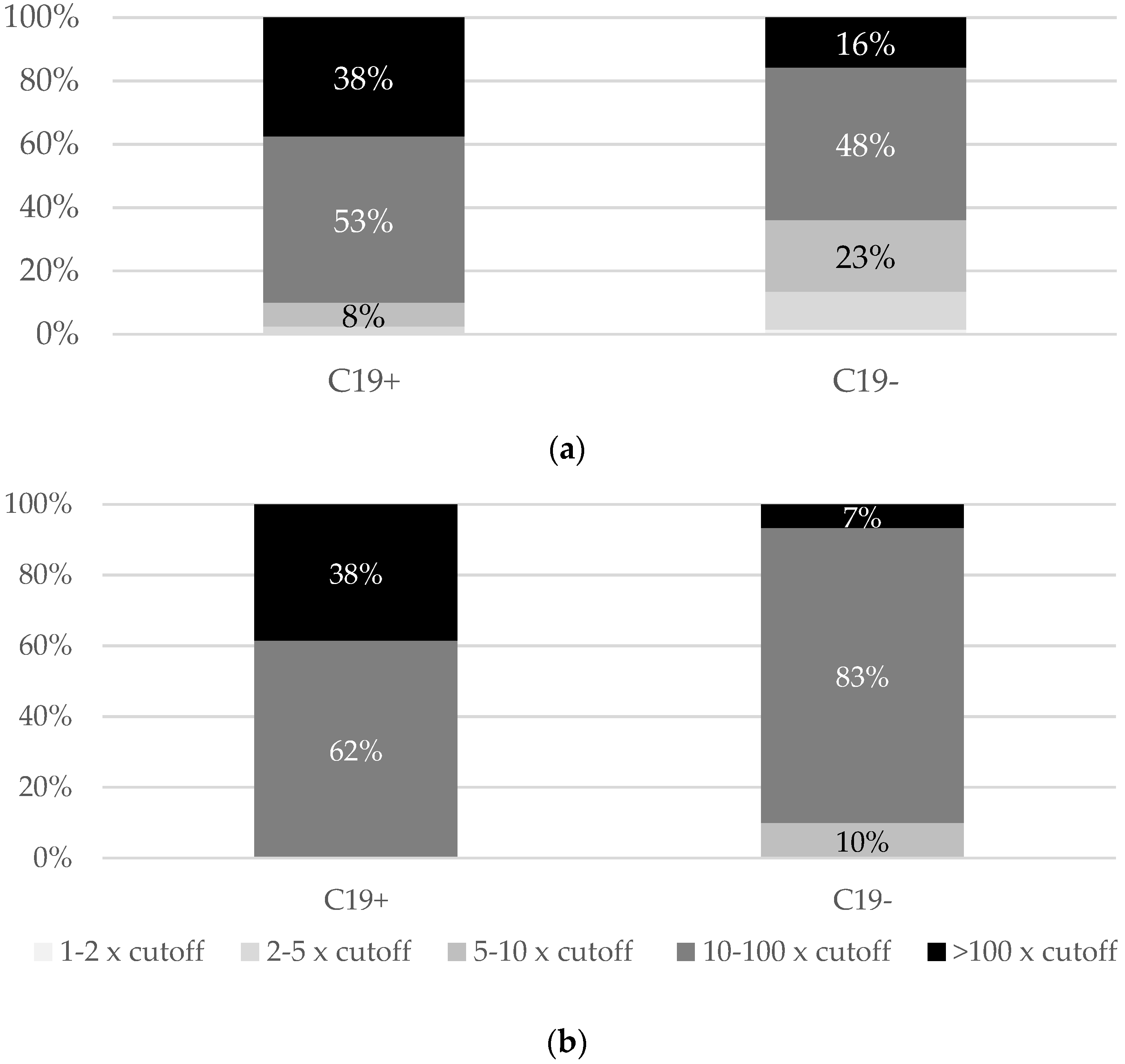
Most people with a history of COVID-19 had levels of both anti-S (91%) and anti-S-RBD (100%) above ten times the positive cut-off, while among those without a history of COVID-19, the percentages of such the values were lower (64% and 90%, respectively) (
Figure 2).
A comparison of data between subjects with a clinical history of COVID-19 and those without it did not show a statistical difference in the frequency of anti-S values above the cut-off and double the positive cut-off (
Table 1). However, as shown in
Table 1, a significantly higher incidence among people with a history of COVID-19 became apparent for anti-S values set above 5, 10, and 100 times the cut-off value. A similar tendency was demonstrated for anti-S-RBD but only for 10 and 100 times the cut-off value (
Table 2).
4. Discussion
In a placebo-controlled study evaluating the long-term efficacy of the BNT162b2 vaccine, carried out after the publication of the registration study results, the effectiveness of the vaccine against COVID-19 at six months of follow-up was 91%, while that against severe disease was 97% [
2,
3]. In turn, in studies carried out in clinical practice, vaccination protected 20%–47% of the subjects against infection within six months and 90%–96% of the subjects against a severe course of the disease requiring hospitalization and posing a threat to life [
6,
8]. On the other hand, we know that neutralizing antibodies persisted in 89% of the subjects and anti-spike antibodies in 97% of the subjects for at least 13 months after infection, but this figure decreased to 36% for anti-nucleoprotein antibodies [
10]. These studies also showed that there are more neutralizing antibodies after a severe course of the disease [
10].
According to data provided by Dimeglio et al. [
11], sufficient protection of 89% can be obtained with a neutralizing antibody level of 141 BAU/mL, which is approximately ten times the level considered in this study as the limit for positive results. In our study, only 64% of vaccinated people with no history of COVID-19 exceeded this anti-S antibody level, in contrast to 90% of those with a history of the disease. Therefore, it can be considered that COVID-19 enhances the humoral response and can be equivalent to a booster dose of the vaccine. This hypothesis is supported by the six-month observations in the registration study of BNT162b2. The clinically evident COVID-19 was less common among the placebo recipients with positive N-binding antibodies at trial (1.3%) than placebo recipients among those without infection at trial entry (4.7%). Based on these data, it can be concluded that the protective effect of the previous symptomatic infection is approximately 73% [
3].
Long-term follow-up would be needed to confirm the possible thesis that a booster dose of the vaccine is not required in previously infected individuals. However, we must bear in mind that we do not know the actual protective level of antibodies, so even higher concentrations of antibodies in this group of people do not guarantee safety. As the health of healthcare professionals is particularly important, until the results of long-term observation are obtained, the booster dose should be recommended in this group, regardless of the condition of previous infection, even if we assume that it may be equivalent to a booster dose.
The limitations of the current study are the relatively small number of samples, the inability to compare the absolute values of antibody concentrations due to the use of different methods of determination, and the lack of standardization. It should also be borne in mind that the study covers only specific humoral immunity, which may be significantly influenced by cellular immunity and the associated immune memory. Another limitation is the sole reliance on interviews when assessing the history of COVID-19. Further observation of the behavior of antibody levels is advisable to analyze the possibility of their disappearance. However, this may not be feasible due to the highly likely uptake of a booster dose by study participants.
5. Conclusions
Vaccination against COVID-19 in people who have previously experienced the disease provides higher levels of specific antibodies, especially against the spike receptor binding domain, six months after vaccination than those in those who have not experienced clinical COVID-19. The lower level of antibodies in people who have not had SARS-CoV-2 infection supports the use of a booster dose imitating the COVID-19 disease.
Author Contributions
Conceptualization, R.F. and M.P.; methodology, R.F.; validation, R.F. and D.Z.-M.; formal analysis, R.F.; investigation, M.P., M.R.-P., M.B.-J., K.K., A.P. and D.Z.-M.; resources, R.F.; data curation, R.F.; writing—original draft preparation, R.F.; writing—review and editing, M.P., M.R.-P., M.B.-J., K.K., A.P. and D.Z.-M.; visualization, R.F.; supervision, R.F.; project administration, R.F.; funding acquisition, R.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Medical Research Agency in Poland, grant number 2020/ABM/COVID19/PTEILCHZ.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the study design not meeting the requirements of the medical experiment according to the national law.
Informed Consent Statement
Patient consent was not required due to the retrospective nature of the study and the research not meeting the requirements of the medical experiment according to national law.
Data Availability Statement
The data presented in this study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The Strategies to support the COVID-19 vaccination with evidence-based communication and tackling misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Polack, F.P.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine through 6 months. N. Engl. J. Med. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody persistence through 6 months after the second dose of mRNA- 1273 vaccine for COVID-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Rzymski, P.; Pazgan-Simon, M.; Simon, K.; Łapiński, T.; Zarębska-Michaluk, D.; Szczepańska, B.; Chojnicki, M.; Mozer-Lisewska, I.; Flisiak, R. Clinical characteristics of hospitalized COVID-19 patients who received at least one dose of COVID-19 Vaccine. Vaccines 2021, 9, 781. [Google Scholar] [CrossRef] [PubMed]
- Haveri, A.; Ekström, N.; Solastie, A.; Virta, C.; Österlund, P.; Isosaari, E.; Nohynek, H.; Palmu, A.A.; Melin, M. Persistence of neutralizing antibodies a year after SARS-CoV-2 infection in humans. Eur. J. Immunol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Dimeglio, C.; Herin, F.; Martin-Blondel, G.; Miedougé, M.; Izopet, J. Antibody titers and protection against a SARS-CoV-2 infection. J. Infect. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}