
The Mediating Roles of Medical Mistrust, Knowledge, Confidence and Complacency of Vaccines in the Pathways from Conspiracy Beliefs to Vaccine Hesitancy


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Respondents
2.2. Sociodemographic Characteristics
3. Questionnaires
3.1. Conspiracy Beliefs
3.2. Medical Mistrust
3.3. Knowledge of Vaccines
3.4. Vaccine Confidence and Complacency
3.5. Vaccine Hesitancy
3.6. Statistical Analysis
3.7. Ethical Approval
4. Results
4.1. Sociodemographic Characteristics and the Distribution of Vaccine Hesitancy
4.2. Correlations of Conspiracy Beliefs, Medical Mistrust, Knowledge of Vaccines, Vaccine Confidence and Complacency, and Vaccine Hesitancy
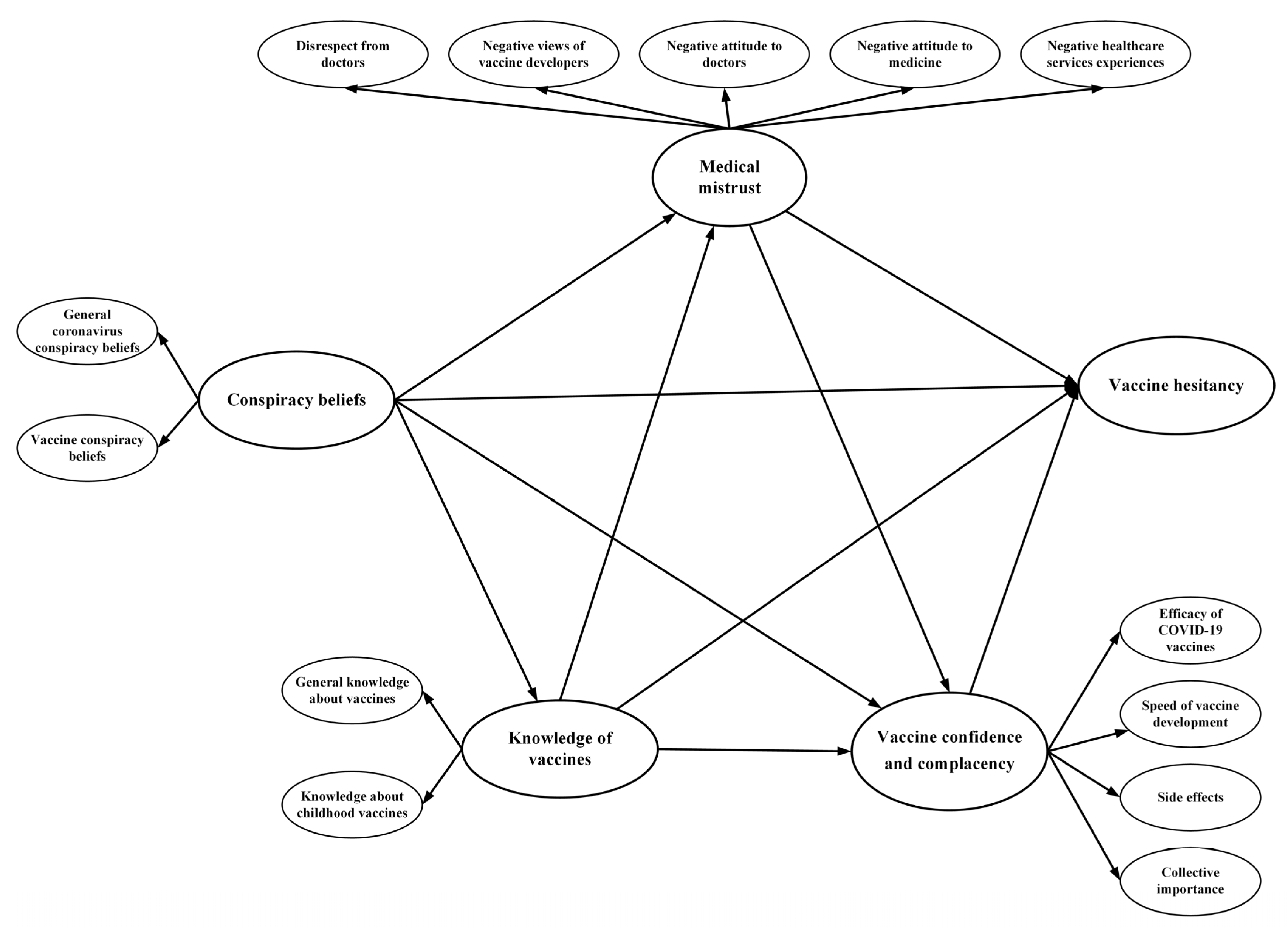
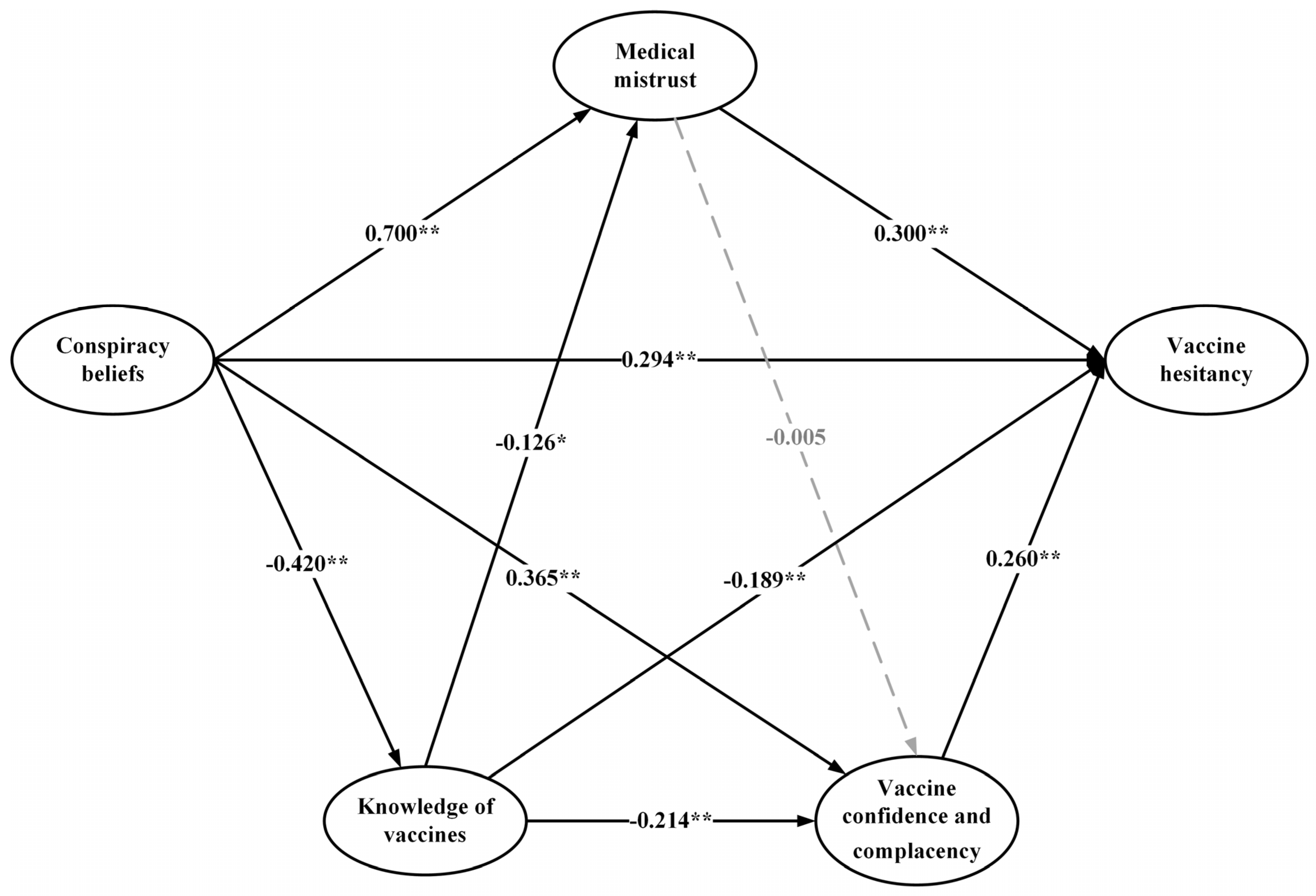
4.3. The Pathways from Conspiracy Beliefs to Vaccine Hesitancy
5. Discussion
6. Strength and Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Domek, G.J.; O’Leary, S.T.; Bull, S.; Bronsert, M.; Contreras-Roldan, I.L.; Ventura, G.A.B.; Kempe, A.; Asturias, E.J. Measuring vaccine hesitancy: Field testing the WHO SAGE Working Group on Vaccine Hesitancy survey tool in Guatemala. Vaccine 2018, 36, 5273–5281. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 11, 1–15. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Yu, L.-M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021, 6, e416–e427. [Google Scholar] [CrossRef]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of intention to vaccinate against COVID-19. Soc. Sci. Med. 2021, 272, 113638. [Google Scholar] [CrossRef]
- Jacobson, R.M.; St Sauver, J.L.; Finney Rutten, L.J. Vaccine Hesitancy. Mayo Clin. Proc. 2015, 90, 1562–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, Y.; Young, R.; Wu, X.; Zhu, G. Effects of Vaccine-Related Conspiracy Theories on Chinese Young Adults’ Perceptions of the HPV Vaccine: An Experimental Study. Health Commun. 2021, 36, 1343–1353. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Bentall, R.P. The concomitants of conspiracy concerns. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 595–604. [Google Scholar] [CrossRef] [Green Version]
- Bertin, P.; Nera, K.; Delouvée, S. Conspiracy Beliefs, Rejection of Vaccination, and Support for hydroxychloroquine: A Conceptual Replication-Extension in the COVID-19 Pandemic Context. Front. Psychol. 2020, 11, 565128. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Lobera, J.; Díaz-Catalán, C. Vaccine hesitancy is strongly associated with distrust of conventional medicine, and only weakly associated with trust in alternative medicine. Soc. Sci. Med. 2020, 255, 113019. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 1–12. [Google Scholar] [CrossRef]
- Arce, J.S.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.L.; Zuccarelli, E.; Zerhouni, E.G.A.; Lee, J.; Muller, J.; Scott, K.M.; Lujan, A.M.; Levi, R. Predicting Coronavirus Disease 2019 Infection Risk and Related Risk Drivers in Nursing Homes: A Machine Learning Approach. J. Am. Med. Dir. Assoc. 2020, 21, 1533–1538. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 16, e0255382. [Google Scholar] [CrossRef]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorini, C.; Santomauro, F.; Donzellini, M.; Capecchi, L.; Bechini, A.; Boccalini, S.; Bonanni, P.; Bonaccorsi, G. Health literacy and vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 478–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.-L.; Carr, L.; Mulhall, S.; et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol. Med. 2020, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Lledo, V.; Alvarez-Galvez, J. Prevalence of Health Misinformation on Social Media: Systematic Review. J. Med. Internet Res. 2021, 23, e17187. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. eLife 2021, 10, e68038. [Google Scholar] [CrossRef]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J.; Understanding Drivers of COVID-19 Vaccine Hesitancy Among Blacks. Clinical Infectious Diseases. 2021. Available online: https://www.scienceopen.com/document_file/de5530a1-1f70-4fd2-8f51-9a2f13552470/PubMedCentral/de5530a1-1f70-4fd2-8f51-9a2f13552470.pdf (accessed on 11 November 2021).
- Ong, S.W.X.; Young, B.E.; Lye, D.C. Lack of detail in population-level data impedes analysis of SARS-CoV-2 variants of concern and clinical outcomes. Lancet Infect. Dis. 2021, 1, 1195–1197. [Google Scholar] [CrossRef]
- Shapiro, G.K.; Holding, A.; Perez, S.; Amsel, R.; Rosberger, Z. Validation of the vaccine conspiracy beliefs scale. Papillomavirus Res. 2016, 2, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marteau, T.M. Attitudes to doctors and medicine: The preliminary development of a new scale. Psychol. Health 1990, 4, 351–356. [Google Scholar] [CrossRef]
- Zingg, A.; Siegrist, M. Measuring people’s knowledge about vaccination: Developing a one-dimensional scale. Vaccine 2012, 30, 3771–3777. [Google Scholar] [CrossRef]
- Akaike, H. Factor analysis and AIC. Psychometrika 1987, 52, 317–332. [Google Scholar] [CrossRef]
- Kline, R.B. Methodology in the Social Sciences. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- VanderWeele, T.J. Mediation Analysis: A Practitioner’s Guide. Annu. Rev. Public Health 2016, 37, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokemper, S.E.; Huber, G.A.; Gerber, A.S.; James, E.K.; Omer, S.B. Timing of COVID-19 vaccine approval and endorsement by public figures. Vaccine 2021, 39, 825–829. [Google Scholar] [CrossRef]
- Ratzan, S.; Ratzan, S.; Schneider, E.C.; Hatch, H.; Cacchione, J. Missing the Point—How Primary Care Can Overcome Covid-19 Vaccine “Hesitancy”. N. Engl. J. Med. 2021, 384, e100. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. Russia’s fast-track coronavirus vaccine draws outrage over safety. Nat. Cell Biol. 2020, 584, 334–335. [Google Scholar] [CrossRef] [PubMed]
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 94, 41–50. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health 2021, 1, 100012. [Google Scholar] [CrossRef]
- Jalloh, M.F.; Wilhelm, E.; Abad, N.; Prybylski, D. Mobilize to vaccinate: Lessons learned from social mobilization for immunization in low and middle-income countries. Hum. Vaccines Immunother. 2019, 16, 1208–1214. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, V.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Rutten, L.J.F.; Zhu, X.; Leppin, A.L.; Ridgeway, J.L.; Swift, M.D.; Griffin, J.M.; Sauver, J.L.S.; Virk, A.; Jacobson, R.M. Evidence-Based Strategies for Clinical Organizations to Address COVID-19 Vaccine Hesitancy. Mayo Clin. Proc. 2021, 96, 699–707. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Verger, P.; Dubé, E. Restoring confidence in vaccines in the COVID-19 era. Expert Rev. Vaccines 2020, 19, 991–993. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, C.; Hacquin, A.-S.; Mercier, H. COVID-19 Vaccine Hesitancy: Shortening the Last Mile. Trends Cogn. Sci. 2021, 25, 331–333. [Google Scholar] [CrossRef]
- Razai, M.S.; Osama, T.; McKechnie, D.G.J.; Majeed, A. COVID-19 vaccine hesitancy among ethnic minority groups. BMJ 2021, 372, n513. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Vaccine Hesitancy | |||||
|---|---|---|---|---|---|---|
| n (%) | Willing (n = 894) | Doubtful (n = 82) | Strongly Hesitancy (n = 39) | χ2 | p | |
| Sex | 7.407 | 0.023 | ||||
| Male | 463 (45.6) | 419 (90.5) | 34 (7.3) | 10 (2.2) | ||
| Female | 552 (54.4) | 475 (86.1) | 48 (8.7) | 29 (5.3) | ||
| Age | 13.097 | 0.041 | ||||
| 18–29 years | 275 (27.1) | 254 (92.4) | 14 (5.1) | 7 (2.5) | ||
| 30–39 years | 313 (30.8) | 260 (83.1) | 36 (11.5) | 17 (5.4) | ||
| 40–49 years | 290 (28.6) | 256 (88.3) | 23 (7.9) | 11 (3.8) | ||
| ≥50 years | 137 (13.5) | 124 (90.5) | 9 (6.6) | 4 (2.9) | ||
| Area of residence | 0.354 | 0.838 | ||||
| Rural | 381 (37.5) | 338 (88.7) | 30 (7.9) | 13 (3.4) | ||
| Urban | 634 (62.5) | 556 (87.7) | 52 (8.2) | 26 (4.1) | ||
| Marital status | 3.288 | 0.463 | ||||
| Single | 333 (32.8) | 289 (86.8) | 31 (9.3) | 13 (3.9) | ||
| Married | 659 (64.9) | 586 (88.9) | 49 (7.4) | 24 (3.6) | ||
| Others | 23 (2.3) | 19 (82.6) | 2 (8.7) | 2 (8.7) | ||
| Educational level | 13.319 | 0.031 | ||||
| Middle school and below | 55 (5.4) | 52 (94.5) | 2 (3.6) | 1 (1.8) | ||
| Senior high school | 92 (9.1) | 87 (94.6) | 3 (3.3) | 2 (2.2) | ||
| Bachelor’s degree | 638 (62.9) | 565 (88.6) | 53 (8.3) | 20 (3.1) | ||
| Master’s degree and above | 230 (22.7) | 190 (82.6) | 24 (10.4) | 16 (7.0) | ||
| Religious beliefs | 1.193 | 0.522 | ||||
| Yes | 61 (6.0) | 52 (85.2) | 7 (11.5) | 2 (3.3) | ||
| No | 954 (94.0) | 842 (88.3) | 75 (7.9) | 37 (3.9) | ||
| Family monthly income (RMB) | 29.703 | < 0.001 | ||||
| <5000 | 96 (9.5) | 68 (70.8) | 23 (24.0) | 5 (5.2) | ||
| 5000–10,000 | 400 (39.4) | 364 (91.0) | 25 (6.3) | 11 (2.8) | ||
| >10,000 | 519 (51.1) | 462 (89.0) | 34 (6.6) | 23 (4.4) | ||
| Employment status | 0.778 | 0.943 | ||||
| Unemployed | 168 (16.6) | 146 (86.9) | 15 (8.9) | 7 (4.2) | ||
| Employed | 520 (51.2) | 456 (87.7) | 43 (8.3) | 21 (4.0) | ||
| Student | 327 (32.2) | 292 (89.3) | 24 (7.3) | 11 (3.4) | ||
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | (16) | (17) | (18) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Observed variables | ||||||||||||||||||
| General coronavirus conspiracy beliefs (1) | 1 | |||||||||||||||||
| Vaccine conspiracy beliefs (2) | 0.59 * | 1 | ||||||||||||||||
| Disrespect from doctors (3) | 0.43 * | 0.60 * | 1 | |||||||||||||||
| Negative views of vaccine developers (4) | 0.44 * | 0.61 * | 0.80 * | 1 | ||||||||||||||
| Negative attitude to doctors (5) | 0.45 * | 0.62 * | 0.82 * | 0.83 * | 1 | |||||||||||||
| Negative attitude to medicine (6) | 0.37 * | 0.51 * | 0.67 * | 0.68 * | 0.70 * | 1 | ||||||||||||
| Negative health care service experiences (7) | 0.34 * | 0.47 * | 0.61 * | 0.62 * | 0.64 * | 0.52 * | 1 | |||||||||||
| Collective importance (8) | 0.29 * | 0.40 * | 0.32 * | 0.32 * | 0.33 * | 0.27 * | 0.25 * | 1 | ||||||||||
| Speed of vaccine development (9) | 0.23 * | 0.32 * | 0.25 * | 0.25 * | 0.26 * | 0.21 * | 0.19 * | 0.77 * | 1 | |||||||||
| Efficacy of COVID-19 vaccines (10) | 0.28 * | 0.38 * | 0.30 * | 0.30 * | 0.31 * | 0.26 * | 0.23 * | 0.93 * | 0.73 * | 1 | ||||||||
| Side effects (11) | 0.25 * | 0.35 * | 0.27 * | 0.28 * | 0.28 * | 0.23 * | 0.21 * | 0.85 * | 0.67 * | 0.80 * | 1 | |||||||
| General knowledge about vaccines (12) | −0.28 * | −0.39 * | −0.38 * | −0.39 * | −0.40 * | −0.33 * | −0.30 * | −0.37 * | −0.29 * | −0.35 * | −0.32 * | 1 | ||||||
| Knowledge about childhood vaccines (13) | −0.29 * | −0.40 * | −0.39 * | −0.40 * | −0.41 * | −0.33 * | −0.30 * | −0.38 * | −0.30 * | −0.36 * | −0.33 * | 0.96 * | 1 | |||||
| Latent variables | ||||||||||||||||||
| Conspiracy beliefs (14) | 0.65 * | 0.90 * | 0.67 * | 0.68 * | 0.69 * | 0.57 * | 0.52 * | 0.45 * | 0.35 * | 0.42 * | 0.39 * | −0.43 * | −0.44 * | 1 | ||||
| Knowledge of vaccines (15) | −0.27 * | −0.38 * | −0.37 * | −0.38 * | −0.39 * | −0.32 * | −0.29 * | −0.36 * | −0.29 * | −0.34 * | −0.31 * | 0.99 * | 0.97 * | −0.42 * | 1 | |||
| Medical mistrust (16) | 0.49 * | 0.68 * | 0.88 * | 0.90 * | 0.92 * | 0.76 * | 0.69 * | 0.36 * | 0.28 * | 0.34 * | 0.31 * | −0.43 * | −0.44 * | 0.75 * | −0.42 * | 1 | ||
| Vaccine confidence and complacency (17) | 0.29 * | 0.41 * | 0.32 * | 0.32 * | 0.33 * | 0.27 * | 0.25 * | 0.99 * | 0.78 * | 0.94 * | 0.85 * | −0.37 * | −0.38 * | 0.45 * | −0.37 * | 0.36 * | 1 | |
| Vaccine hesitancy (18) | 0.47 * | 0.64 * | 0.61 * | 0.63 * | 0.64 * | 0.53 * | 0.48 * | 0.57 * | 0.45 * | 0.53 * | 0.49 * | −0.55 * | −0.56 * | 0.72 * | −0.53 * | 0.70 * | 0.57 * | 1 |
| Pathways | Effect | S.E. | p | BC 95% CI |
|---|---|---|---|---|
| Conspiracy beliefs → Medical mistrust → Vaccine hesitancy | 0.210 | 0.048 | 0.001 | 0.106 to 0.301 |
| Conspiracy beliefs → Vaccine confidence and complacency → Vaccine hesitancy | 0.095 | 0.034 | 0.001 | 0.027 to 0.100 |
| Conspiracy beliefs → Knowledge of vaccines → Vaccine hesitancy | 0.079 | 0.022 | 0.001 | 0.029 to 0.163 |
| Conspiracy beliefs → Mistrust → Vaccine confidence and complacency → Vaccine hesitancy | −0.001 | 0.020 | 0.987 | 0.038 to 0.987 |
| Conspiracy beliefs → Knowledge of vaccines → Medical mistrust → Vaccine hesitancy | 0.016 | 0.008 | 0.015 | 0.032 to 0.015 |
| Conspiracy beliefs → Knowledge of vaccines → Vaccine confidence and complacency → Vaccine hesitancy | 0.023 | 0.010 | 0.003 | 0.045 to 0.003 |
| Conspiracy beliefs → Knowledge of vaccines → Medical mistrust → Vaccine confidence and complacency → Vaccine hesitancy | <0.001 | 0.002 | 0.994 | −0.003 to 0.003 |
| Variables | Standardized Direct Effects | Standardized Indirect Effects | Standardized Total Effects |
|---|---|---|---|
| Conspiracy beliefs | 0.294 * | 0.423 * | 0.717 * |
| Medical mistrust | 0.300 * | −0.001 | 0.299 * |
| Knowledge of vaccines | −0.189 * | −0.093 * | −0.282 * |
| Vaccine confidence and complacency | 0.260 * | - | 0.260 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Guo, Y.; Zhou, Q.; Tan, Z.; Cao, J. The Mediating Roles of Medical Mistrust, Knowledge, Confidence and Complacency of Vaccines in the Pathways from Conspiracy Beliefs to Vaccine Hesitancy. Vaccines 2021, 9, 1342. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111342
Zhang X, Guo Y, Zhou Q, Tan Z, Cao J. The Mediating Roles of Medical Mistrust, Knowledge, Confidence and Complacency of Vaccines in the Pathways from Conspiracy Beliefs to Vaccine Hesitancy. Vaccines. 2021; 9(11):1342. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111342
Chicago/Turabian StyleZhang, Xiaoning, Yuqing Guo, Qiong Zhou, Zaixiang Tan, and Junli Cao. 2021. "The Mediating Roles of Medical Mistrust, Knowledge, Confidence and Complacency of Vaccines in the Pathways from Conspiracy Beliefs to Vaccine Hesitancy" Vaccines 9, no. 11: 1342. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9111342