
Gender Differences in the Level of Antibodies to Measles Virus in Adults

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Historical Information
2.2. Contingent
- 1.
- known vaccination history;
- 2.
- presence of medical documents on vaccination and revaccination against measles;
- 3.
- only employees of the medical organization participated in the study.
- 4.
- immunosuppressive therapy, systemic use or inhalation of corticosteroids in high doses (over 800 µg of beclomethasone or equivalent per day), radiotherapy, cytotoxic drugs or nonsteroid anti-inflammatory drugs;
- 5.
- HIV infection (positive serological test), hepatitis B (acute form) and hepatitis C (acute form);
- 6.
- therapy containing immunoglobulins and other donor blood products within 90 days prior to the study participation;
- 7.
- any vaccine administration within 30 days prior to inclusion in the study;
- 8.
- contraindications to introduction of the measles vaccine (according to the instruction);
- 9.
- the accession of acute respiratory infections during the first days after vaccination.
2.3. Vaccines
2.4. Laboratory Methods
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- CDC. Evidence of Immunity. Available online: https://www.cdc.gov/measles/hcp/index.html (accessed on 5 November 2020).
- Timchenko, V.N.; Kaplina, T.A.; Leonicheva, O.A.; Bulina, O.V.; Hakizimana, J.K.; Timofeeva, E.V. Actual problems of measles. Pediatrician 2017, 8, 120–129. [Google Scholar] [CrossRef] [Green Version]
- Robesyn, E. Complications after measles. What can EU surveillance data tell us? European Centre for Disease Prevention and Control (ECDC) 36th Annual Meeting of the ESPID 2018, Malmo, Sweden, 1 June 2018. Available online: http://ecdc.europa.eu/en/home (accessed on 1 June 2018).
- Muscat, M. Measles elimination in Europe—how to close are we and what are the challenges? WHO, Europe, Association Centralized information system for infectious diseases (CISID) 36th Annual Meeting of the ESPID 2018, Malmo, Sweden, 1 June 2018. Available online: http://data.euro.who.int/cisid (accessed on 1 June 2018).
- Infectious Morbidity in the Russian Federation for January–July 2017 (According to the form № 1 «Information on Infectious and Parasitic Diseases»). Available online: http://rospotrebnadzor.ru/activities/statistical-materials/statictic_details.php?ELEMENT_ID=10158 (accessed on 5 June 2018).
- Kostinov, M.P.; Shmitko, A.D.; Solovieva, I.L.; Savisko, A.A.; Cherdantsev, A.P. Are children with allergic diseases and sickly children resistant to measles after revaccination? Pediatria 2017, 4, 140–145. [Google Scholar] [CrossRef]
- Kostinov, M.P.; Shmitko, A.D.; Solovieva, I.L.; Savisko, A.A.; Polishchuk, V.B.; Ryzhov, A.A.; Cherdantsev, A.P. Is a third dose of the measles vaccine necessary—an immunologist’s view. J. Microbiol. Epidemiol. Immunol. 2016, 5, 88–94. [Google Scholar]
- Mazankova, L.N.; Gorbunov, S.G.; Nesterina, L.F.; Tebenkov, A.V. Clinical features of measles course at the present stage. Pediatria 2013, 92, 18–22. [Google Scholar]
- Leonova, G.N.; Balabanov, I.V. Tick-Borne Encephalitis: Topical Aspects; Karolinska Institutet: Moscow, Russia, 2009; p. 168. [Google Scholar]
- Prokofiev, V.I.; Chernitsyna, L.O.; Jerusalimskiy, A.P.; Konenkov, V.I. Immunogenetic markers in the tick-borne encephalitis in Western Siberia. Bull. Sib. Branch Acad. Med Sci. USSR 1988, 5–6, 49–53. [Google Scholar]
- Balabolkin, I.I.; Kostinov, M.P.; Ignatieva, G.V.; Sadykova, D.K.; Gervazieva, V.B. Vaccination with Live Measles Vaccine in Children with Allergic Diseases; Information letter: Moscow, Russia, 1988; p. 8. [Google Scholar]
- Kostinov, M.P.; Gervazieva, V.B.; Balabolkin, I.I. Immunological reactivity of children with allergic diseases in the measles vaccination process. J. Microbiol. Epidemiol. Immunobiol. 1990, 3, 81–84. [Google Scholar]
- Solovyeva, I.L.; Kostinov, M.P.; Kuselman, A.I. Features of Vaccination of Children with Changed Premorbid Background Against Hepatitis B, Measles, Mump; Ulyanovsk State Technical University (UlSTU): Ulyanovsk, Russia, 2006; p. 296. [Google Scholar]
- Polishchuk, V.B.; Ryzhov, A.A.; Kostinov, M.P.; Magarshak, O.O.; Shmitko, A.D.; Lukachev, I.V.; Vasilieva, G.V.; Blagovidov, D.A.; Chuchalin, A.G.; Avdeev, S.N.; et al. Condition of anti-measles immunity in patients on waiting-list for lung transplantation. J. Microbiol. Epidemiol. Immunobiol. 2016, 4, 55–60. [Google Scholar] [CrossRef]
- Solovyeva, I.L.; Lezen, E.M.; Kuselman, A.I.; Kostinov, M.P.; Mukanova, D.S.; Krasheninnikova, E.Y. Vaccination of ailing children with home-made measles and parotitis vaccine. Ulyanovsk Med. Biol. J. 2013, 2, 20–25. [Google Scholar]
- About Incidence of Measles and Additional Prevention Measures; The Letter of 8 February 2018 N 01/1730-2018-32; Federal Service for Supervision of Consumer Rights Protection and Human Well-Being: Moscow, Russia, 2018.
- Chuchalin, A.G.; Khokhlova, A.L. Federal Guidance on the Application of Drugs (Formulary System); Issue XVIII: Moscow, Russia, 2017; p. 848. [Google Scholar]
- Ibragimova, E.M.; Yuminova, N.V.; Kostinov, M.P.; Alexander, S.K.; Kolyshkin, V.M.; Markelova, E.V. Some aspects of population immunity study to measles, mumps and rubella in the Primorsky Territory. Epidemiol. Vaccinal Prev. 2005, 3, 21–23. [Google Scholar]
- Kostinov, M.P.; Zverev, V.V. Vaccination Against Hepatitis B, Influenza and Rubella Adult Patients with Chronic Diseases; MDV: Moscow, Russia, 2009; p. 196. [Google Scholar]
- Kostinov, M.P. Ways to Improve Effectiveness of Immunization Against Measles in Children with Allergic Diseases. Ph.D. Thesis, Federal State Budgetary Scientific Institution, Moscow, Russia, 1988; p. 23. [Google Scholar]
- Kostinov, M.P.; Balabolkin, I.I.; Gervazieva, V.B.; Ovsyannikova, I.G. Significance of the study of total immunoglobulin E concentration in immunization with live measles vaccine in children with allergic diseases. Immunology 1990, 1, 41–44. [Google Scholar]
- Khaitov, R.M.; Ilina, N.I. Allergology and Immunology: National Guige; GEOTAR-Media: Moscow, Russia, 2014; p. 656. [Google Scholar]
- Kostinov, M.P. Immunotherapy in Pediatrics: A Practical Guide for Physicians; Medicine for Everyone: Moscow, Russia, 1997; p. 111. [Google Scholar]
- Solovyeva, I.L.; Kuselman, I.A.; Kostinov, M.P.; Anokhina, E.V. Use of immunomodulators in preparing children to vaccination. Allergol. Immunol. 2007, 2, 206–208. [Google Scholar]
- Afinogenova, V.P.; Lukachev, I.V.; Kostinov, M.P. Immunotherapy: Mechanism of action and clinical use of immunocorrecting drugs. Treat. Dr. 2010, 4, 9. [Google Scholar]
- Tarasova, A.A.; Kostinov, M.P.; Yushkova, I.V. Modern view on vaccine prevention of diseases in immunocompromised patients. Med. Dep. 2005, 1, 45–53. [Google Scholar]
- Ovsyannikova, I.G.; Jacobson, R.M.; Vierkant, R.A.; Pankratz, V.S.; Poland, G.A. HLA supertypes and immune responses to measles–mumps–rubella viral vaccine: Findings and implications for vaccine design. Vaccine 2007, 25, 3090–3100. [Google Scholar] [CrossRef]
- Khalil, M.K.; Al-Mazrou, Y.Y.; Al-Ghamdi, Y.S.; Tumsah, S.; Al-Jeffri, M.; Meshkhas, A. Effect of gender on reporting of MMR adverse events in Saudi Arabia. East. Mediterr. Health J. 2003, 9, 152–158. [Google Scholar]
- France, E.K.; Glanz, J.; Xu, S.; Hambidge, S.; Yamasaki, K.; Black, S.B.; Marcy, M.; Mullooly, J.P.; Jackson, L.A.; Nordin, J.; et al. Risk of Immune Thrombocytopenic Purpura After Measles-Mumps-Rubella Immunization in Children. Pediatrics 2008, 121, e687–e692. [Google Scholar] [CrossRef] [PubMed]
- Kostinov, M.P.; Filatov, N.N.; Zhuravlev, P.I.; Gladkova, L.S.; Polishchuk, V.B.; Shmitko, A.D.; Pahomov, D.V.; Kostinova, A.M.; Vasilieva, G.V.; Tihonova, I.A.; et al. Age-related immune response to measles virus in staff of a large city hospital. Pulmonology 2018, 28, 701–707. [Google Scholar] [CrossRef]
- Mossong, J.; O’Callaghan, C.; Ratnam, S. Modelling antibody response to measles vaccine and subsequent waning of immunity in a low exposure population. Vaccine 2000, 19, 523–529. [Google Scholar] [CrossRef]
- Domínguez, A.; Plans, P.; Costa, J.; Torner, N.; Cardenosa, N.; Batalla, J.; Plasencia, A.; Salleras, L. Seroprevalence of measles, rubella, and mumps antibodies in Catalonia, Spain: Results of a cross-sectional study. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 310–317. [Google Scholar] [CrossRef]
- Poethko-Müller, C.; Mankertz, A. Seroprevalence of Measles-, Mumps- and Rubella-Specific IgG Antibodies in German Children and Adolescents and Predictors for Seronegativity. PLoS ONE 2012, 7, e42867. [Google Scholar] [CrossRef]
- Fink, A.L.; Engle, K.; Ursin, R.L.; Tang, W.-Y.; Klein, S.L. Biological sex affects vaccine efficacy and protection against influenza in mice. Proc. Natl. Acad. Sci. USA 2018, 115, 12477–12482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, S.; Klein, R.S. Sex Drives Dimorphic Immune Responses to Viral Infections. J. Immunol. 2017, 198, 1782–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Zverev, V.V.; Haitov, R.M. Vaccines and Vaccination: National Guide; GEOTAR-Media: Moscow, Russia, 2014; p. 640. [Google Scholar]
- Boulton, M.L.; Wang, X.; Zhang, Y.; Montgomery, J.P.; Wagner, A.L.; Carlson, B.F.; Ding, Y.; Li, X.; Gillespie, B.; Su, X. A population profile of measles susceptibility in Tianjin, China. Vaccine 2016, 34, 3037–3043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemmons, N.S.; Wallace, G.S.; Patel, M.; Gastañaduy, P.A. Incidence of Measles in the United States, 2001–2015. JAMA 2017, 318, 1279–1281. [Google Scholar] [CrossRef]
- Brown, T. Measles Cases Continue to Rise, Highest Since 1992. Medscape Medical News. Available online: https://www.medscape.com/viewarticle/913916 (accessed on 6 June 2019).
- Measles (Rubeola): Measles Cases and Outbreaks. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/measles/cases-outbreaks.html (accessed on 6 June 2019).




{kind=link}
{kind=link}
{kind=link}
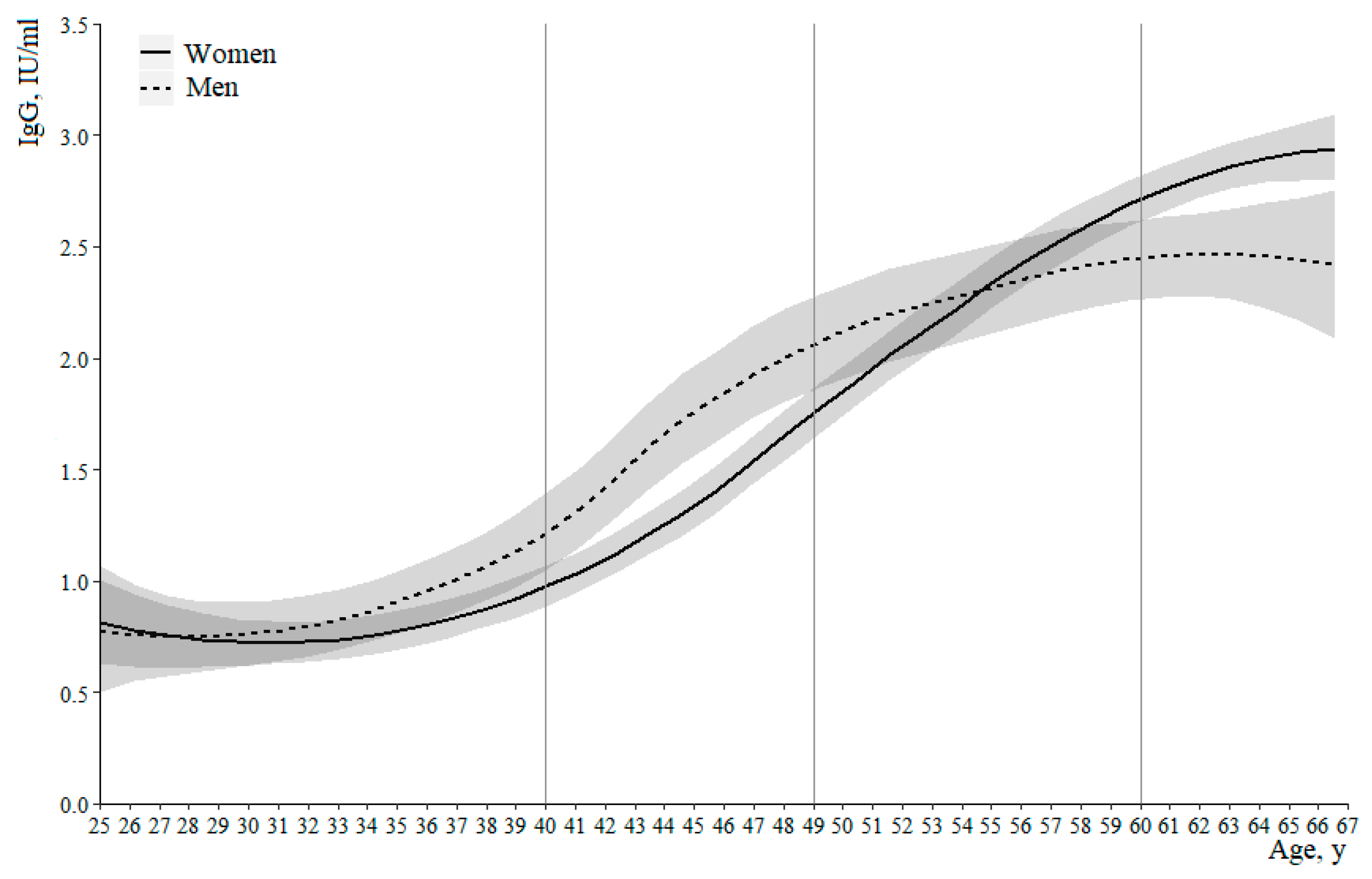
| Age | Regression Assessment of IgG Levels and 95% Confidence Interval | Age | Regression Assessment of IgG Levels and 95% Confidence Interval | ||
|---|---|---|---|---|---|
| Women | Men | Women | Men | ||
| 25 | 0.81 [1.00–0.63] | 0.78 [108–0.51] | 47 | 1.61 [1.72–1.50] | 2.00 [2.19–1.79] |
| 26 | 0.78 [0.95–0.62] | 0.76 [1.00–0.56] | 48 | 1.71 [1.,82–1.60] | 2.06 [2.26–1.86] |
| 27 | 0.76 [0.90–0.62] | 0.75 [0.95–0.57] | 49 | 1.81 [1.92–1.70] | 2.11 [2.31–1.92] |
| 28 | 0.74 [0.86–0.62] | 0.75 [0.92–0.59] | 50 | 1.91 [2.02–1.80] | 2.16 [2.35–1.95] |
| 29 | 0.73 [0.84–0.63] | 0.75 [0.91–0.61] | 51 | 2.01 [2.13–1.90] | 2.19 [2.39–1.98] |
| 30 | 0.72 [0.82–0.63] | 0.76 [0.91–0.63] | 52 | 2.11 [2.23–2.00] | 2.22 [2.43–2.01] |
| 31 | 0.72 [0.81–0.64] | 0.78 [0.92–0.65] | 53 | 2.20 [2.33–2.10] | 2.26 [2.47–2.05] |
| 32 | 0.73 [0.82–0.65] | 0.80 [0.94–0.67] | 54 | 2.30 [2.42–2.20] | 2.30 [2.51–2.10] |
| 33 | 0.74 [0.83–0.66] | 0.83 [0.97–0.71] | 55 | 2.39 [2.50–2.29] | 2.34 [2.54–2.14] |
| 34 | 0.76 [0.85–0.67] | 0.87 [1.01–0.74] | 56 | 2.48 [2.59–2.37] | 2.37 [2.57–2.17] |
| 35 | 0.78 [0.87–0.70] | 0.91 [1.05–0.78] | 57 | 2.56 [2.67–2.46] | 2.40 [2.59–2.21] |
| 36 | 0.81 [0.90–0.72] | 0.96 [1.11–0.82] | 58 | 2.64 [2.75–2.54] | 2.42 [2.60–2.22] |
| 37 | 0.85 [0.94–0.76] | 1.01 [1.17–0.87] | 59 | 2.72 [2.82–2.58] | 2.43 [2.61–2.25] |
| 38 | 0.89 [0.98–0.80] | 1.07 [1.24–0.93] | 60 | 2.80 [2.90–2.65] | 2.44 [2.62–2.28] |
| 39 | 0.94 [1.03–0.84] | 1.15 [1.32–1.00] | 61 | 2.80 [2.91–2.69] | 2.46 [2.63–2.29] |
| 40 | 0.99 [1.08–0.90] | 1.25 [1.42–1.08] | 62 | 2.81 [2.92–2.72] | 2.47 [2.64–2.29] |
| 41 | 1.06 [1.14–0.96] | 1.37 [1.55–1.19] | 63 | 2.86 [2.97–2.76] | 2.46 [2.66–2.27] |
| 42 | 1.13 [1.22–1.03] | 1.50 [1.68–1.29] | 64 | 2.90 [3.01–2.79] | 2.46 [2.69–2.24] |
| 43 | 1.20 [1.31–1.10] | 1.62 [1.80–1.40] | 65 | 2.92 [3.05–2.80] | 2.44 [2.73–2.18] |
| 44 | 1.29 [1.39–1.18] | 1.72 [1.92–1.51] | 66 | 2.94 [3.09–2.79] | 2.42 [2.74–2.11] |
| 45 | 1.39 [1.49–1.28] | 1.82 [2.01–1.61] | 67 | 2.95 [3.14–2,.77] | 2.41 [2.76–2.02] |
| 46 | 1.50 [1.61–1.39] | 1.91 [2.11–1.71] | |||
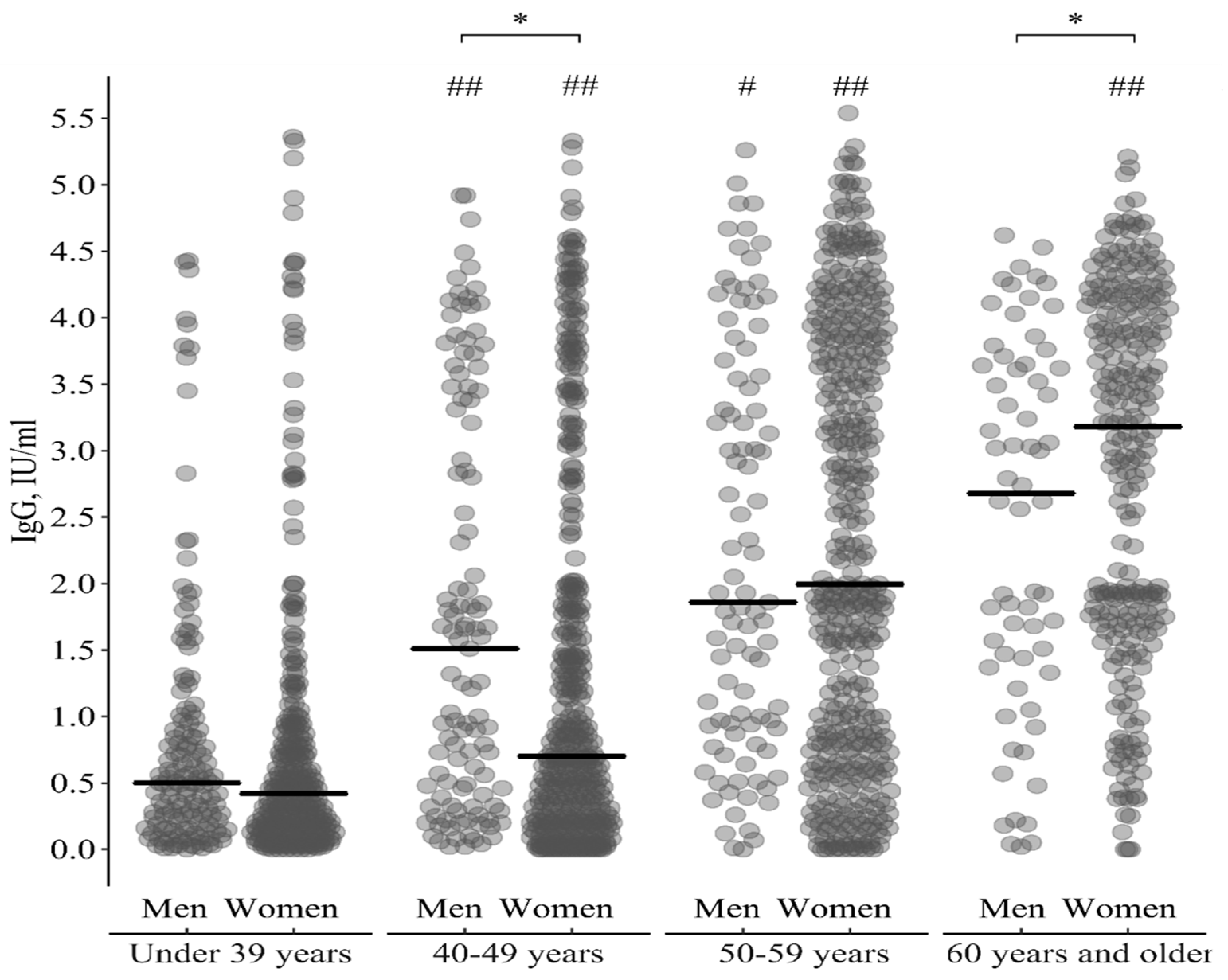
| Age Groups | IgG, IU/Ml—Me(IQR) | Comparison by Sex | |
|---|---|---|---|
| Men | Women | ||
| Under 39 y | 0.50(0.19; 0.97) | 0.42(0.16; 0.91) | U = 1.11, p = 0.27 |
| 40–49 y | 1.51(0.41; 3.38) | 0.70(0.22; 1.98) | U = 3.2, p = 0.001 |
| 50–59 y | 1.86(0.93; 3.54) | 2.00(0.79; 3.83) | U = 0.29, p = 0.77 |
| 60 y and older | 2.68(1.46; 3.53) | 3.29(1.72; 4.07) | U = 2.2, p = 0.03 |
| Comparison of age groups in dynamics: | |||
| 40–49 y/under 39 y | U = 5.2, ph < 0.001 | U = 4.7, ph < 0.001 | - |
| 50–59 y/40–49 y | U = 2.3, ph = 0.04 | U = 9.0, ph < 0.001 | |
| 60 y and older/50–59 y | U = 1.3, ph = 0.19 | U = 4.4, ph < 0.001 | |
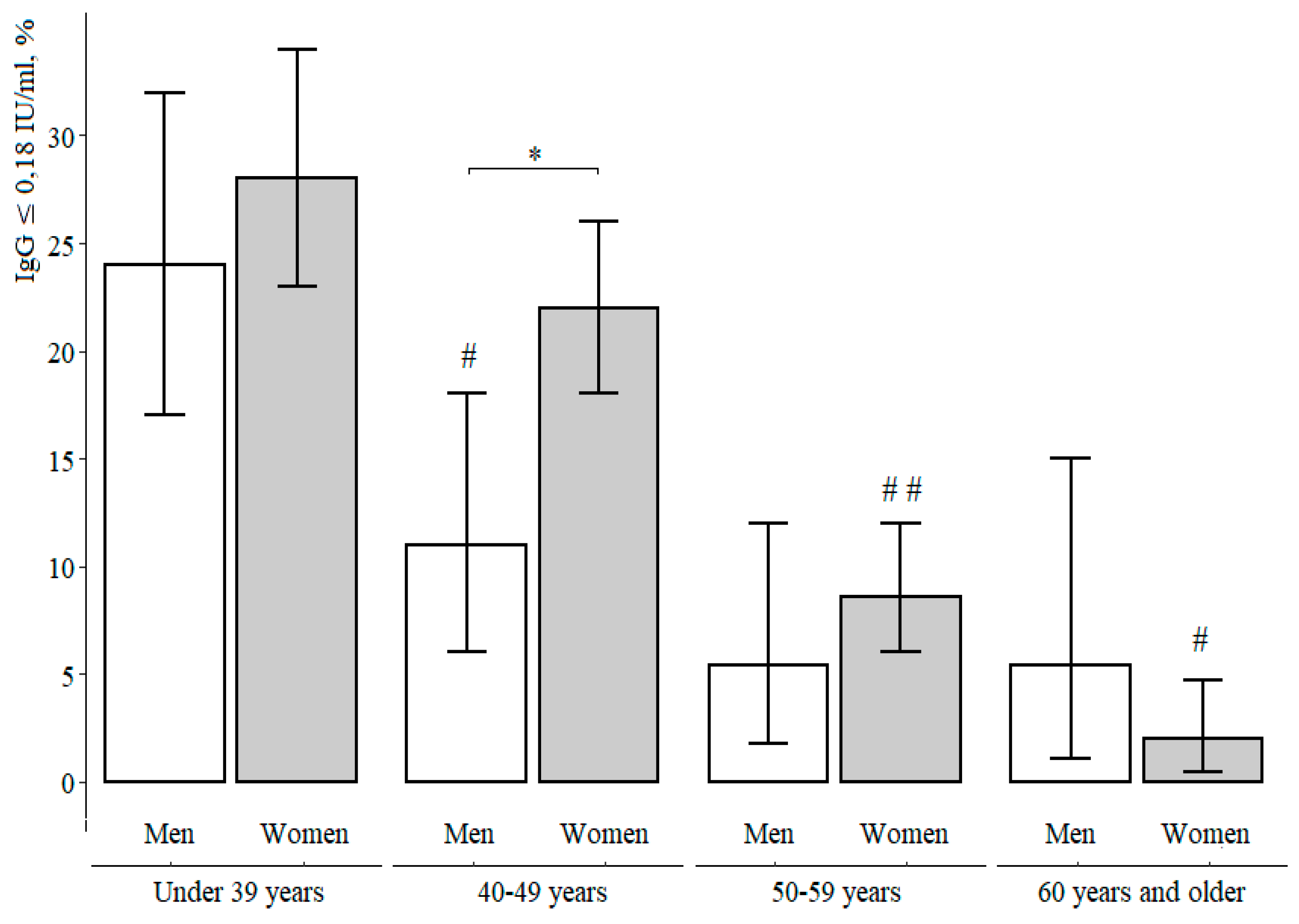
| Age Groups | IgG < 0.18 IU/mL | Comparison by Sex | ||
|---|---|---|---|---|
| Men | Women | |||
| Under 39 y | % [CI] | 24 [17–32]% | 28 [23–34]% | χ2 = 0.87, p = 0.27 |
| n/N | 34/141 | 85/300 | ||
| 40–49 y | % [CI] | 11 [6–18]% | 22 [18–26]% | χ2 = 7.0, p = 0.001 |
| n/N | 12/113 | 90/415 | ||
| 50–59 y | % [CI] | 5.4 [1.8–12]% | 8.6 [6.0–12]% | χ2 = 1.1, p = 0.77 |
| n/N | 5/93 | 35/408 | ||
| 60 y and older | % [CI] | 5.4 [1.1–15]% | 2.0 [0.5–4.7]% | p = 0.16 according to Fisher |
| n/N | 3/56 | 4/216 | ||
| Comparison of age groups in dynamics | ||||
| 40–49 y/under 39 y | χ2 = 7.7, ph = 0.02 | χ2 = 3.8, ph = 0.06 | - | |
| 50–59 y/40–49 y | χ2 = 1.9, ph = 0.35 | χ2 = 24.4, ph < 0.001 | ||
| 60 y and older/50–59 y | χ2 = 0.01, ph = 0.99 | χ2 = 10.9, ph = 0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostinov, P.M.; Zhuravlev, I.P.; Filatov, N.N.; Kostinova, M.А.; Polishchuk, B.V.; Shmitko, D.A.; Mashilov, V.C.; Vlasenko, E.A.; Ryzhov, A.A.; Kostinov, M.А. Gender Differences in the Level of Antibodies to Measles Virus in Adults. Vaccines 2021, 9, 494. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9050494
Kostinov PM, Zhuravlev IP, Filatov NN, Kostinova MА, Polishchuk BV, Shmitko DA, Mashilov VC, Vlasenko EA, Ryzhov AA, Kostinov MА. Gender Differences in the Level of Antibodies to Measles Virus in Adults. Vaccines. 2021; 9(5):494. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9050494
Chicago/Turabian StyleKostinov, P. Mikhail, I. Pavel Zhuravlev, N. Nikolay Filatov, M. Аristitsa Kostinova, B. Valentina Polishchuk, D. Anna Shmitko, V. Cyrill Mashilov, E. Anna Vlasenko, A. Alexey Ryzhov, and M. Аnton Kostinov. 2021. "Gender Differences in the Level of Antibodies to Measles Virus in Adults" Vaccines 9, no. 5: 494. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9050494