
Attitudes toward the SARS-CoV-2 Vaccine: Results from the Saudi Residents’ Intention to Get Vaccinated against COVID-19 (SRIGVAC) Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Survey Administration
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Clinical Characteristics and the Perceived Risk of COVID-19
3.3. Vaccination Intention and Associated Factors
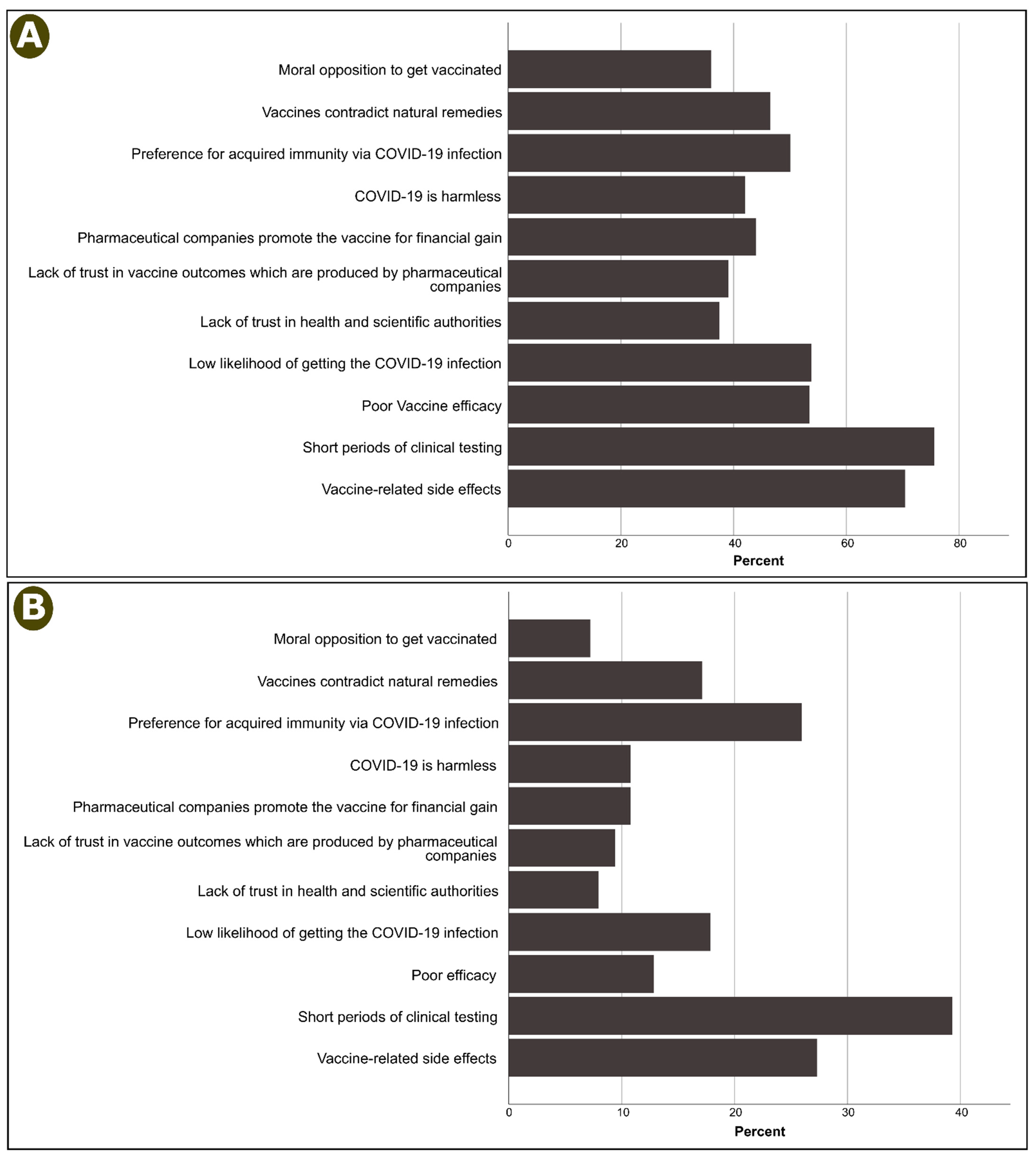
3.4. Reasons for No or Not Sure Responses Regarding Participant’s Intention to Get Vaccinated
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update—2 March 2021. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20210302_weekly_epi_update_29.pdf?sfvrsn=91306c8c_5&download=true (accessed on 7 March 2021).
- World Health Organization. Saudi Arabia: WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/region/emro/country/sa (accessed on 7 March 2021).
- Baig, M.; Jameel, T.; Alzahrani, S.H.; Mirza, A.A.; Gazzaz, Z.J.; Ahmad, T.; Baig, F.; Almurashi, S.H. Predictors of misconceptions, knowledge, attitudes, and practices of COVID-19 pandemic among a sample of Saudi population and its impact: A cross-sectional study. PLoS ONE 2020, 15, e0243526. [Google Scholar] [CrossRef]
- Ahmad, T.; Haroon; Baig, M.; Hui, J. Coronavirus disease 2019 (COVID-19) pandemic and economic impact. Pak. J. Med. Sci. 2020, 36, S73–S78. [Google Scholar] [CrossRef]
- Algaissi, A.A.; Alharbi, N.K.; Hassanain, M.; Hashem, A.M. Preparedness and response to COVID-19 in Saudi Arabia: Building on MERS experience. J. Infect. Public. Health 2020, 13, 834–838. [Google Scholar] [CrossRef]
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.; Murad, M.A.; Baig, M.; Hui, J. Research trends in COVID-19 vaccine: A bibliometric analysis. Hum. Vaccines Immunother. 2021, 9, 1–6. [Google Scholar] [CrossRef]
- Thunstrom, L.; Ashworth, M.; Finnoff, D.; Newbold, S. Hesitancy towards a COVID-19 Vaccine and Prospects for Herd Immunity. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3593098 (accessed on 24 May 2021). [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Faasse, K.; Newby, J. Public perceptions of COVID-19 in Australia: Perceived risk, knowledge, health-protective behaviors, and vaccine intentions. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.-A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, e110. [Google Scholar] [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: A web-based national survey. J. Multidiscip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.A.; Xu, X.; Dam, L. Information source dependence, presumed media influence, risk knowledge, and vaccination intention. Atl. J. Commun. 2021, 2, 53–64. [Google Scholar] [CrossRef]
- Sarathchandra, D.; Navin, M.C.; Largent, M.A.; McCright, A.M. A survey instrument for measuring vaccine acceptance. Prev. Med. 2018, 109, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Grech, V.; Gauci, C.; Agius, S. Vaccine hesitancy among Maltese healthcare workers toward influenza and novel COVID-19 vaccination. Early Hum. Dev. 2020, 105213. [Google Scholar] [CrossRef]
- Benecke, O.; DeYoung, S.E. Anti-vaccine decision-making and measles resurgence in the United States. Glob. Pediatr. Health 2019, 6, 2333794x19862949. [Google Scholar] [CrossRef] [Green Version]
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association between vaccine refusal and vaccine-preventable diseases in the United States: A review of measles and pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piltch-Loeb, R.; DiClemente, R. The vaccine uptake continuum: Applying social science theory to shift vaccine hesitancy. Vaccines 2020, 8, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 vaccination during the COVID-19 pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, P318–P319. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Willingness to vaccinate against COVID-19 in the US: Longitudinal evidence from a nationally representative sample of adults from April–October 2020. medRxiv 2020, 60, 766–773. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 1–12. [Google Scholar] [CrossRef]
- Burki, T. The online anti-vaccine movement in the age of COVID-19. Lancet Digit. Health 2020, 2, e504–e505. [Google Scholar] [CrossRef]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing COVID-19 vaccines at pandemic speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- Sun, C.; Pleyer, C.; Wiestner, A. COVID-19 vaccines for patients with haematological conditions. Lancet Haematol. 2021, 8, e312–e314. [Google Scholar] [CrossRef]
- Combe, C.; Kirsch, A.H.; Alfano, G.; Luyckx, V.A.; Shroff, R.; Kanbay, M.; van der Sande, F.; Basile, C.; The EUDIAL Working Group of the ERA-EDTA. At least 156 reasons to prioritize COVID-19 vaccination in patients receiving in-centre haemodialysis. Nephrol Dial. Transpl. 2021, 36, 571–574. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.M.; Afghani, B.; Byington, C.L.; Cunningham, C.K.; Golub, S.; Lu, K.D.; Radom-Aizik, S.; Ross, L.F.; Singh, J.; Smoyer, W.E. SARS-CoV-2 vaccine testing and trials in the pediatric population: Biologic, ethical, research, and implementation challenges. Pediatr. Res. 2021, 1, 1–5. [Google Scholar] [CrossRef]
- McAndrew, S.; Allington, D. Mode and frequency of COVID-19 information updates, political values, and future COVID-19 vaccine attitudes. PsyArXiv 2020. Available online: https://psyarxiv.com/j7srx/ (accessed on 17 July 2021).
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.J.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of intention to vaccinate against COVID-19. Soc. Sci. Med. 2021, 272, 113638. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.J.; Hagger, M.S.; Hamilton, K. The mediating role of constructs representing reasoned-action and automatic processes on the past behavior-future behavior relationship. Soc. Sci. Med. 2020, 258, 113085. [Google Scholar] [CrossRef] [PubMed]
- Ouellette, J.A.; Wood, W. Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior. Psychol. Bull. 1998, 124, 54–74. [Google Scholar] [CrossRef]
- Sheeran, P.; Conner, M. Degree of reasoned action predicts increased intentional control and reduced habitual control over health behaviors. Soc. Sci. Med. 2019, 228, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Chapman, G.B.; Coups, E.J. Emotions and preventive health behavior: Worry, regret, and influenza vaccination. Health Psychol. 2006, 25, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, N.D.; Kwitel, A.; McCaul, K.D.; Magnan, R.E.; Gerrard, M.; Gibbons, F.X. Risk perceptions: Assessment and relationship to influenza vaccination. Health Psychol. 2007, 26, 146. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Category | N (%) | Intention to Be Vaccinated, n (%) | p | ||
|---|---|---|---|---|---|---|
| Yes (n = 1612) | Unsure (n = 817) | No (n = 619) | ||||
| Age | 18–29 y | 1331 (43.7) | 713 (53.6) | 361 (27.1) | 257 (19.3) | 0.079 |
| 30–44 y | 1261 (41.4) | 638 (50.6) | 348 (27.6) | 275 (21.8) | ||
| 45–59 y | 409 (13.4) | 228 (55.7) | 99 (24.2) | 82 (20) | ||
| ≥60 y | 47 (1.5) | 33 (70.2) | 9 (19.1) | 5 (10.6) | ||
| Gender | Male | 1217 (39.9) | 779 (64) | 284 (23.3) | 154 (12.7) | <0.0001 |
| Female | 1831 (60.1) | 833 (45.5) | 533 (29.1) | 465 (25.4) | ||
| Education level | <Secondary education | 42 (1.4) | 34 (81) | 5 (11.9) | 3 (7.1) | 0.010 |
| Secondary | 302 (9.9) | 149 (49.3) | 80 (26.5) | 73 (24.2) | ||
| University | 2104 (69) | 1118 (53.1) | 567 (26.9) | 419 (19.9) | ||
| Post-graduate | 600 (19.7) | 311 (51.8) | 165 (27.5) | 124 (20.7) | ||
| Nationality | Saudi | 2729 (89.5) | 1468 (53.8) | 738 (27) | 523 (19.2) | <0.0001 |
| Non-Saudi | 319 (10.5) | 144 (45.1) | 79 (24.8) | 96 (30.1) | ||
| Current employment status | Employed—Government | 1157 (38) | 622 (53.8) | 311 (26.9) | 224 (19.4) | 0.320 |
| Employed—Private/self-employed | 530 (17.4) | 285 (53.8) | 127 (24.0) | 118 (22.3) | ||
| Student | 581 (19.1) | 314 (54) | 149 (25.6) | 118 (20.3) | ||
| Not working | 780 (25.6) | 391 (50.1) | 230 (29.5) | 159 (20.4) | ||
| Monthly income (SAR) | <3000 | 1220 (40) | 641 (52.5) | 332 (27.2) | 247 (20.2) | 0.067 |
| 3000–10,000 | 851 (27.9) | 426 (50.1) | 228 (26.8) | 197 (23.1) | ||
| >10,000–25,000 | 856 (28.1) | 470 (54.9) | 227 (26.5) | 159 (18.6) | ||
| >25,000 | 121 (4) | 75 (62) | 30 (24.8) | 16 (13.2) | ||
| Household size | 1–3 | 495 (16.2) | 260 (52.5) | 122 (24.6) | 113 (22.8) | 0.243 |
| 4–6 | 1402 (46) | 728 (51.9) | 392 (28) | 282 (20.1) | ||
| 7–9 | 818 (26.8) | 430 (52.6) | 227 (27.8) | 161 (19.7) | ||
| ≥10 | 333 (10.9) | 194 (58.3) | 76 (22.8) | 63 (18.9) | ||
| Geographic region of residency | Western | 1738 (57) | 916 (52.7) | 482 (27.7) | 340 (19.6) | <0.0001 |
| Eastern | 294 (9.6) | 154 (52.4) | 76 (25.9) | 64 (21.8) | ||
| Northern | 193 (6.3) | 93 (48.2) | 54 (28) | 46 (23.8) | ||
| Southern | 329 (10.8) | 217 (66) | 71 (21.6) | 41 (12.5) | ||
| Central | 494 (16.2) | 232 (47) | 134 (27.1) | 128 (25.9) | ||
| Parameter | Category | N (%) | Intention to Be Vaccinated, n (%) | p | ||
|---|---|---|---|---|---|---|
| Yes (n = 1612) | Not Sure (n = 817) | No (n = 619) | ||||
| History of a chronic disease | No | 2468 (81) | 1303 (52.8) | 673 (27.3) | 492 (19.9) | 0.367 |
| Yes | 580 (19) | 309 (53.3) | 144 (24.8) | 127 (21.9) | ||
| History of COVID-19 | No | 2699 (88.5) | 1430 (53) | 736 (27.3) | 533 (19.7) | 0.061 |
| Yes | 349 (11.5) | 182 (52.1) | 81 (23.2) | 86 (24.6) | ||
| History of COVID-19 among family members | No | 2064 (67.7) | 1092 (52.9) | 561 (27.2) | 411 (19.9) | 0.66 |
| Yes | 984 (32.3) | 520 (52.8) | 256 (26) | 208 (21.1) | ||
| History of COVID-19 among friends | No | 1035 (34) | 543 (52.5) | 271 (26.2) | 221 (21.4) | 0.571 |
| Yes | 2013 (66) | 1069 (53.1) | 546 (27.1) | 398 (19.8) | ||
| Recently received an influenza vaccine | No | 1794 (58.9) | 798 (44.5) | 535 (29.8) | 461 (25.7) | <0.0001 |
| Yes | 1254 (41.1) | 814 (64.9) | 282 (22.5) | 158 (12.6) | ||
| Perception of risk of COVID-19 to the individual | No | 376 (12.3) | 37 (38.9) | 9 (9.5) | 49 (51.6) | <0.0001 |
| Low to Moderate | 1931 (63.4) | 967 (50.9) | 551 (29) | 381 (20.1) | ||
| High to very high | 741 (24.3) | 608 (57.7) | 257 (24.4) | 189 (17.9) | ||
| Perception of risk of COVID-19 to others | No | 95 (3.1) | 164 (43.6) | 75 (19.9) | 137 (36.4) | <0.0001 |
| Low to Moderate | 1899 (62.3) | 1034 (53.5) | 556 (28.8) | 341 (17.7) | ||
| High to very high | 1054 (34.6) | 414 (55.9) | 186 (25.1) | 141 (19) | ||
| Parameter | Category | Intent to Be Vaccinated | |||
|---|---|---|---|---|---|
| No vs. Yes | Not Sure vs. Yes | ||||
| RRR (95% CI) | p | RRR (95% CI) | p | ||
| Gender | Female | 2.70 (2.18–3.36) | <0.0001 | 1.69 (1.41–2.02) | <0.0001 |
| Male | Ref | Ref | |||
| Nationality | Saudi | 0.49 (0.36–0.66) | <0.0001 | 0.85 (0.63–1.15) | 0.304 |
| Non-Saudi | Ref | Ref | |||
| Educational level | <Secondary education | 0.16 (0.05–0.57) | 0.005 | 0.26 (0.1–0.68) | 0.006 |
| Secondary | 0.92 (0.63–1.34) | 0.658 | 0.92 (0.66–1.29) | 0.632 | |
| University | 0.84 (0.65–1.09) | 0.183 | 0.88 (0.7–1.1) | 0.256 | |
| Post-graduate | Ref | Ref | |||
| Geographic location | Western | 0.78 (0.6–1.01) | 0.061 | 0.93 (0.73–1.19) | 0.576 |
| Eastern | 0.83 (0.57–1.23) | 0.356 | 0.87 (0.61–1.24) | 0.445 | |
| Northern | 0.99 (0.64–1.53) | 0.966 | 1.00 (0.66–1.49) | 0.982 | |
| Southern | 0.46 (0.30–0.69) | <0.0001 | 0.61 (0.43–0.87) | 0.006 | |
| Central | Ref | Ref | |||
| Received the influenza vaccine recently | No | 2.63 (2.12–3.25) | <0.0001 | 1.88 (1.57–2.24) | <0.0001 |
| Yes | Ref | Ref | |||
| Personal risk of COVID-19 | High to very high | 0.59 (0.35–0.99) | 0.046 | 1.05 (0.79–3.09) | 0.060 |
| Low to Moderate | 0.45 (0.26–0.79) | 0.006 | 1.68 (0.76–3.7) | 0.200 | |
| No | Ref | Ref | |||
| Risk of COVID-19 to others | High to very high | 0.52 (0.38–0.7) | <0.0001 | 1.16 (0.85–1.58) | 0.356 |
| Low to Moderate | 0.63 (0.43–0.91) | 0.014 | 1.16 (0.8–1.67) | 0.441 | |
| No | Ref | Ref | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, S.H.; Baig, M.; Alrabia, M.W.; Algethami, M.R.; Alhamdan, M.M.; Alhakamy, N.A.; Asfour, H.Z.; Ahmad, T. Attitudes toward the SARS-CoV-2 Vaccine: Results from the Saudi Residents’ Intention to Get Vaccinated against COVID-19 (SRIGVAC) Study. Vaccines 2021, 9, 798. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070798
Alzahrani SH, Baig M, Alrabia MW, Algethami MR, Alhamdan MM, Alhakamy NA, Asfour HZ, Ahmad T. Attitudes toward the SARS-CoV-2 Vaccine: Results from the Saudi Residents’ Intention to Get Vaccinated against COVID-19 (SRIGVAC) Study. Vaccines. 2021; 9(7):798. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070798
Chicago/Turabian StyleAlzahrani, Sami H., Mukhtiar Baig, Mohammed W. Alrabia, Mohammed R. Algethami, Meshari M. Alhamdan, Nabil A. Alhakamy, Hani Z. Asfour, and Tauseef Ahmad. 2021. "Attitudes toward the SARS-CoV-2 Vaccine: Results from the Saudi Residents’ Intention to Get Vaccinated against COVID-19 (SRIGVAC) Study" Vaccines 9, no. 7: 798. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9070798