
Association of Polymorphisms in the Glutathione S-Transferase Theta-1 Gene with Cirrhosis and Hepatocellular Carcinoma in Brazilian Patients with Chronic Hepatitis C

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
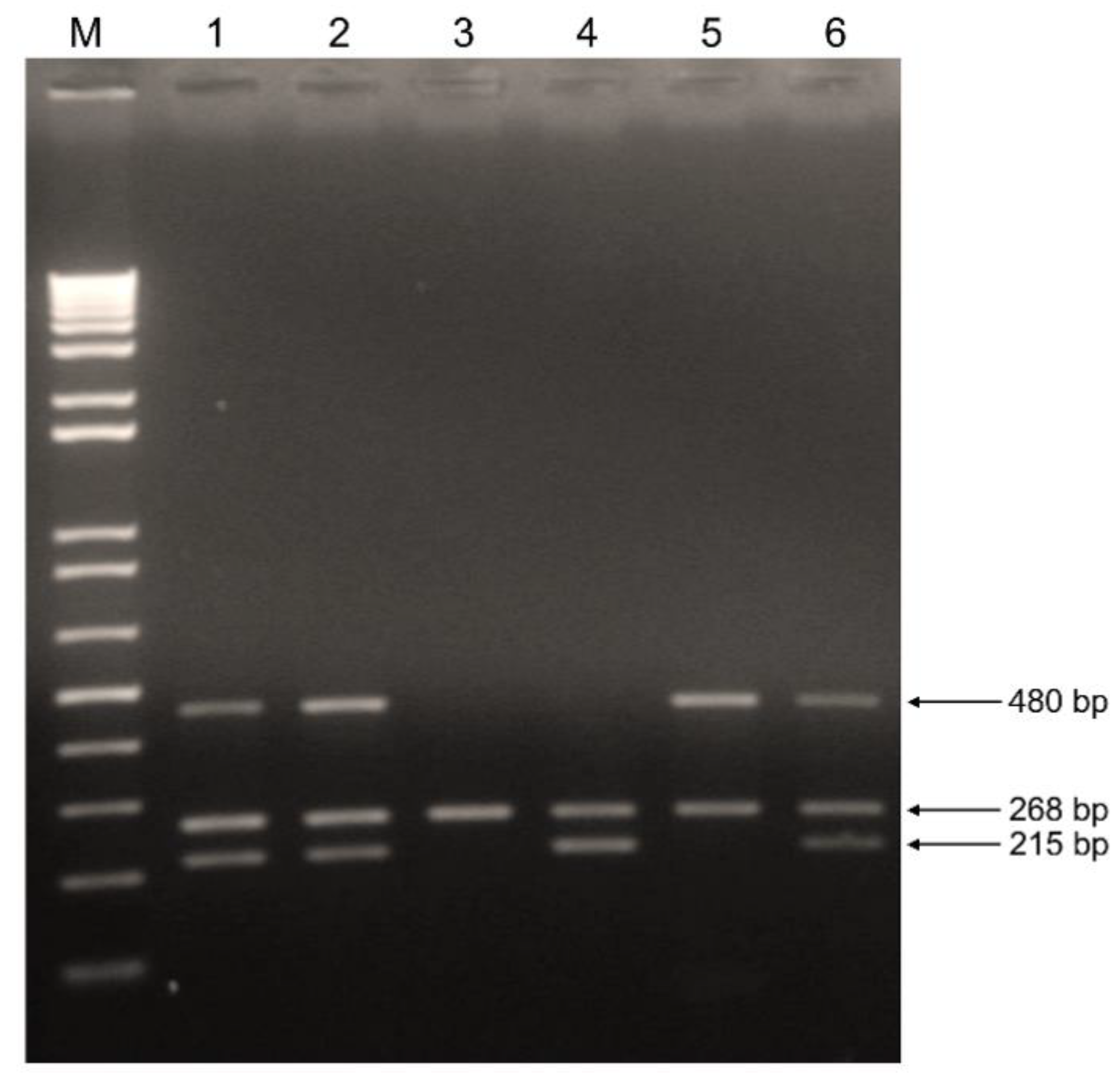
2.2. Genotyping of GSTM1 and GSTT1 Polymorphisms
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. GSTM1 and GSTT1 Polymorphisms and Risk for Cirrhosis and HCC
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- IARC. International Agency for Research on Cancer. Globocan 2020. 11-Liver-Fact-Sheet.pdf. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf (accessed on 13 May 2021).
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127, S35–S50. [Google Scholar] [CrossRef]
- INCA. Tipos de Câncer- =Câncer de Fígado. Instituto Nacional do Câncer, Ministério da Saúde. Available online: https://www.inca.gov.br/tipos-de-cancer/cancer-de-figado (accessed on 8 March 2021).
- Paranagua-Vezozzo, D.C.; Ono, S.K.; Alvarado-Mora, M.V.; Farias, A.Q.; Cunha-Silva, M.; Franca, J.I.; Alves, V.A.; Sherman, M.; Carrilho, F.J. Epidemiology of HCC in Brazil: Incidence and risk factors in a ten-year cohort. Ann. Hepatol. 2014, 13, 386–393. [Google Scholar] [CrossRef]
- WHO. The World Health Organization. Fact Sheets. Hepatitis C. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 13 May 2021).
- Ravi, S.; Axley, P.; Jones, D.; Kodali, S.; Simpson, H.; McGuire, B.M.; Singal, A.K. Unusually High Rates of Hepatocellular Carcinoma after Treatment With Direct-Acting Antiviral Therapy for Hepatitis C Related Cirrhosis. Gastroenterology 2017, 152, 911–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roche, B.; Coilly, A.; Duclos-Vallee, J.C.; Samuel, D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. Off. J. Int. Assoc. Study Liver 2018, 38 (Suppl. 1), 139–145. [Google Scholar] [CrossRef] [Green Version]
- Kanda, T.; Goto, T.; Hirotsu, Y.; Moriyama, M.; Omata, M. Molecular Mechanisms Driving Progression of Liver Cirrhosis towards Hepatocellular Carcinoma in Chronic Hepatitis B and C Infections: A Review. Int. J. Mol. Sci. 2019, 20, 1358. [Google Scholar] [CrossRef] [Green Version]
- Caruso, S.; O’Brien, D.R.; Cleary, S.P.; Roberts, L.R.; Zucman-Rossi, J. Genetics of Hepatocellular Carcinoma: Approaches to Explore Molecular Diversity. Hepatology 2021, 73 (Suppl. 1), 14–26. [Google Scholar] [CrossRef]
- Kumar, V.; Kato, N.; Urabe, Y.; Takahashi, A.; Muroyama, R.; Hosono, N.; Otsuka, M.; Tateishi, R.; Omata, M.; Nakagawa, H.; et al. Genome-wide association study identifies a susceptibility locus for HCV-induced hepatocellular carcinoma. Nat. Genet. 2011, 43, 455–458. [Google Scholar] [CrossRef]
- Miki, D.; Ochi, H.; Hayes, C.N.; Abe, H.; Yoshima, T.; Aikata, H.; Ikeda, K.; Kumada, H.; Toyota, J.; Morizono, T.; et al. Variation in the DEPDC5 locus is associated with progression to hepatocellular carcinoma in chronic hepatitis C virus carriers. Nat. Genet. 2011, 43, 797–800. [Google Scholar] [CrossRef]
- Nahon, P.; Zucman-Rossi, J. Single nucleotide polymorphisms and risk of hepatocellular carcinoma in cirrhosis. J. Hepatol. 2012, 57, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Ye, Z.; Zhang, Z.; Zheng, J.; Tang, Y.; Hou, E.; Huang, Z.; Meng, L. A comprehensive evaluation of single nucleotide polymorphisms associated with hepatocellular carcinoma risk in Asian populations: A systematic review and network meta-analysis. Gene 2020, 735, 144365. [Google Scholar] [CrossRef] [PubMed]
- Koike, K.; Miyoshi, H. Oxidative stress and hepatitis C viral infection. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2006, 34, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Awasthi, Y.C.; Sharma, R.; Singhal, S.S. Human glutathione S-transferases. Int. J. Biochem. 1994, 26, 295–308. [Google Scholar] [CrossRef]
- Hayes, J.D.; Flanagan, J.U.; Jowsey, I.R. Glutathione transferases. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 51–88. [Google Scholar] [CrossRef] [PubMed]
- McIlwain, C.C.; Townsend, D.M.; Tew, K.D. Glutathione S-transferase polymorphisms: Cancer incidence and therapy. Oncogene 2006, 25, 1639–1648. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Xue, F.; Zheng, Y.; Yang, P.; Lin, S.; Deng, Y.; Xu, P.; Zhou, L.; Hao, Q.; Zhai, Z.; et al. GSTM1 and GSTT1 null genotype increase the risk of hepatocellular carcinoma: Evidence based on 46 studies. Cancer Cell Int. 2019, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Zhang, L.; Lin, X.; Chen, L.; Shi, H.; Magaye, R.; Zou, B.; Zhao, J. Association of GST genetic polymorphisms with the susceptibility to hepatocellular carcinoma (HCC) in Chinese population evaluated by an updated systematic meta-analysis. PLoS ONE 2013, 8, e57043. [Google Scholar] [CrossRef]
- Shen, Y.H.; Chen, S.; Peng, Y.F.; Shi, Y.H.; Huang, X.W.; Yang, G.H.; Ding, Z.B.; Yi, Y.; Zhou, J.; Qiu, S.J.; et al. Quantitative assessment of the effect of glutathione S-transferase genes GSTM1 and GSTT1 on hepatocellular carcinoma risk. Tumour Biol. J. Int. Soc. Oncodevelopmental Biol. Med. 2014, 35, 4007–4015. [Google Scholar] [CrossRef]
- Ibrahim, A.M.; Ahmed, H.S.; Alazizi, N.M.; Mansour, M.A.; Mansour, S.A. Glutathione S-Transferase M1 and T1 Gene Polymorphisms and the Outcome of Chronic Hepatitis C Virus Infection in Egyptian Patients. Ann. Hum. Genet. 2016, 80, 32–37. [Google Scholar] [CrossRef]
- Martinez, C.; Garcia-Martin, E.; Ladero, J.M.; Herraez, O.; Ortega, L.; Taxonera, C.; Suarez, A.; Diaz-Rubio, M.; Agundez, J.A. GSTT1 and GSTM1 null genotypes may facilitate hepatitis C virus infection becoming chronic. J. Infect. Dis. 2007, 195, 1320–1323. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.C.; Jeng, Y.C.; Lee, M.S.; Wen, C.F.; Chen, T.M.; Lee, M.S. Glutathione-S-Transferase M1 and T1 Gene Polymorphisms and Susceptibility to the Progression of Liver Fibrosis in HCV-Infected Patients in Taiwan. J. Med. Biochem. 2014, 33, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Unal, M.; Guven, M.; Devranoglu, K.; Ozaydin, A.; Batar, B.; Tamcelik, N.; Gorgun, E.E.; Ucar, D.; Sarici, A. Glutathione S transferase M1 and T1 genetic polymorphisms are related to the risk of primary open-angle glaucoma: A study in a Turkish population. Br. J. Ophthalmol. 2007, 91, 527–530. [Google Scholar] [CrossRef] [Green Version]
- Bell, D.A.; Taylor, J.A.; Paulson, D.F.; Robertson, C.N.; Mohler, J.L.; Lucier, G.W. Genetic risk and carcinogen exposure: A common inherited defect of the carcinogen-metabolism gene glutathione S-transferase M1 (GSTM1) that increases susceptibility to bladder cancer. J. Natl. Cancer Inst. 1993, 85, 1159–1164. [Google Scholar] [CrossRef]
- Pena, S.D.J.; Santos, F.R.; Tarazona-Santos, E. Genetic admixture in Brazil. Am. J. Med. Genet. C Semin. Med. Genet. 2020, 184, 928–938. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, G.D.; Fernandes, G.M.M.; Penteado, C.; Coria, V.R.; Galbiatti-Dias, A.; Russo, A.; Castanhole-Nunes, M.M.U.; Silva, R.F.D.; Silva, R.; Pavarino, E.C.; et al. Polymorphisms in xenobiotic metabolism-related genes in patients with hepatocellular carcinoma: A case-control study. Xenobiotica 2021, 51, 737–744. [Google Scholar] [CrossRef]
- Sherratt, P.J.; Pulford, D.J.; Harrison, D.J.; Green, T.; Hayes, J.D. Evidence that human class Theta glutathione S-transferase T1-1 can catalyse the activation of dichloromethane, a liver and lung carcinogen in the mouse. Comparison of the tissue distribution of GST T1-1 with that of classes Alpha, Mu and Pi GST in human. Biochem. J. 1997, 326 Pt 3, 837–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| p-Value | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Chronic Hepatitis | Cirrhosis | HCC | HCC | HCC | Cirrhosis |
| (n = 47) | (n = 83) | (n = 60) | vs. | vs. | vs. | |
| Chronic Hepatitis | Cirrhosis | Chronic Hepatitis | ||||
| Age (years, mean ± SD) a | 57 ± 11 | 59 ± 9 | 64 ± 9 | <0.001 | 0.006 | 0.48 |
| Male (%) | 14 (30) | 42 (51) | 32 (53) | 0.015 | 0.74 | 0.99 |
| ALT (U/L, median (IQR)) | 59 (41) | 74 (75) | 82 (30) | 0.029 | 0.88 | 0.067 |
| AST (U/L, median (IQR)) | 43 (40) | 70 (77) | 91 (62) | 0.001 | 0.30 | 0.008 |
| ALP (U/L, median (IQR)) | 80 (35) | 110 (58) | 123 (134) | <0.01 | 0.18 | <0.01 |
| GGT (U/L, median (IQR)) | 68 (46) | 101 (146) | 113 (155) | 0.002 | 0.32 | 0.012 |
| ALB (g/dL, median (IQR)) | 3.8 (0.4) | 3.6 (1.0) | 3.6 (1.0) | 0.70 | 0.74 | 0.018 |
| T.BIL (mg/dL, median (IQR)) | 0.7 (0.3) | 0.8 (0.8) | 0.9 (0.6) | 0.005 | 0.40 | 0.016 |
| AFP (ng/mL, median (IQR)) | 6.9 ± (7.4) | 6.0 (15) | 31 (248) | <0.01 | <0.01 | 0.52 |
| HCV genotype (%) | ||||||
| 1a | 10 (21) | 31 (37) | 18 (30) | 0.378 | 0.378 | 0.076 |
| 1b | 15 (32) | 20 (24) | 19 (32) | 1.000 | 0.345 | 0.411 |
| 3a | 4 (9) | 5 (6) | 9 (15) | 0.380 | 0.091 | 0.722 |
| ND | 18 (38) | 27 (33) | 14 (23) | - | - | - |
| Genotype | Chronic Hepatitis (n = 47) | Cirrhosis (n = 83) | p-Value | OR | 95% CI |
|---|---|---|---|---|---|
| GSTM1-null (%) | 22 (46.8%) | 34 (41%) | 0.518 | 1.268 | 0.617–2.618 |
| GSTT1-null (%) | 3 (6.4%) | 17 (20.5%) | 0.043 | 3.778 | 1.045–13.659 |
| GSTM1-null/GSTT1-null (%) | 1 (2.1%) | 3 (3.6%) | 0.567 | 1.522 | 0.193–20.131 |
| Genotype | Chronic Hepatitis (n = 47) | HCC (n = 60) | p-Value | OR | 95% CI |
|---|---|---|---|---|---|
| GSTM1-null (%) | 22 (46.8%) | 28 (46.7%) | 0.98 | 1.006 | 0.468–2.162 |
| GSTT1-null (%) | 3 (6.4%) | 13 (21.7%) | 0.038 | 4.057 | 1.083–15.201 |
| GSTM1-null/GSTT1-null (%) | 1 (2.1%) | 6 (10%) | 0.127 | 5.520 | 0.617–49.393 |
| Variables | GSTM1 Null | GSTM1 Positive | GSTT1 Null | GSTT1 Positive | p-Value | |
|---|---|---|---|---|---|---|
| GSTM1 Null vs. GSTM1 Positive | GSTT1 Null vs. GSTT1 Positive | |||||
| ALT (U/L, median (IQR)) | 78 (67) | 71 (45) | 77 (42) | 71 (59) | 0.283 | 0.907 |
| AST (U/L, median (IQR)) | 70 (93) | 69 (73) | 85 (69) | 68 (78) | 0.279 | 0.748 |
| ALP (U/L, median (IQR)) | 97 (54) | 107 (79) | 116 (72) | 103 (76) | 0.074 | 0.206 |
| GGT (U/L, median (IQR)) | 85 (181) | 102 (130) | 89 (113) | 94 (141) | 0.692 | 0.937 |
| ALB (g/dL, median (IQR)) | 4.0 (1.0) | 4.0 (1.0) | 3.0 (1.2) | 4.0 (0.8) | 0.913 | 0.173 |
| T.BIL (mg/dL, median (IQR)) | 1.0 (0.9) | 1.0 (0.5) | 1.0 (0.9) | 1.0 (0.7) | 0.420 | 0.839 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Araujo, O.C.; de Paula, V.S.; do Ó, K.M.; Villela-Nogueira, C.A.; Araujo, N.M. Association of Polymorphisms in the Glutathione S-Transferase Theta-1 Gene with Cirrhosis and Hepatocellular Carcinoma in Brazilian Patients with Chronic Hepatitis C. Vaccines 2021, 9, 831. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9080831
Araujo OC, de Paula VS, do Ó KM, Villela-Nogueira CA, Araujo NM. Association of Polymorphisms in the Glutathione S-Transferase Theta-1 Gene with Cirrhosis and Hepatocellular Carcinoma in Brazilian Patients with Chronic Hepatitis C. Vaccines. 2021; 9(8):831. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9080831
Chicago/Turabian StyleAraujo, Oscar C., Vanessa S. de Paula, Kycia M. do Ó, Cristiane A. Villela-Nogueira, and Natalia M. Araujo. 2021. "Association of Polymorphisms in the Glutathione S-Transferase Theta-1 Gene with Cirrhosis and Hepatocellular Carcinoma in Brazilian Patients with Chronic Hepatitis C" Vaccines 9, no. 8: 831. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9080831