
Prevalence of Depression among Healthcare Workers during the COVID-19 Outbreak: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
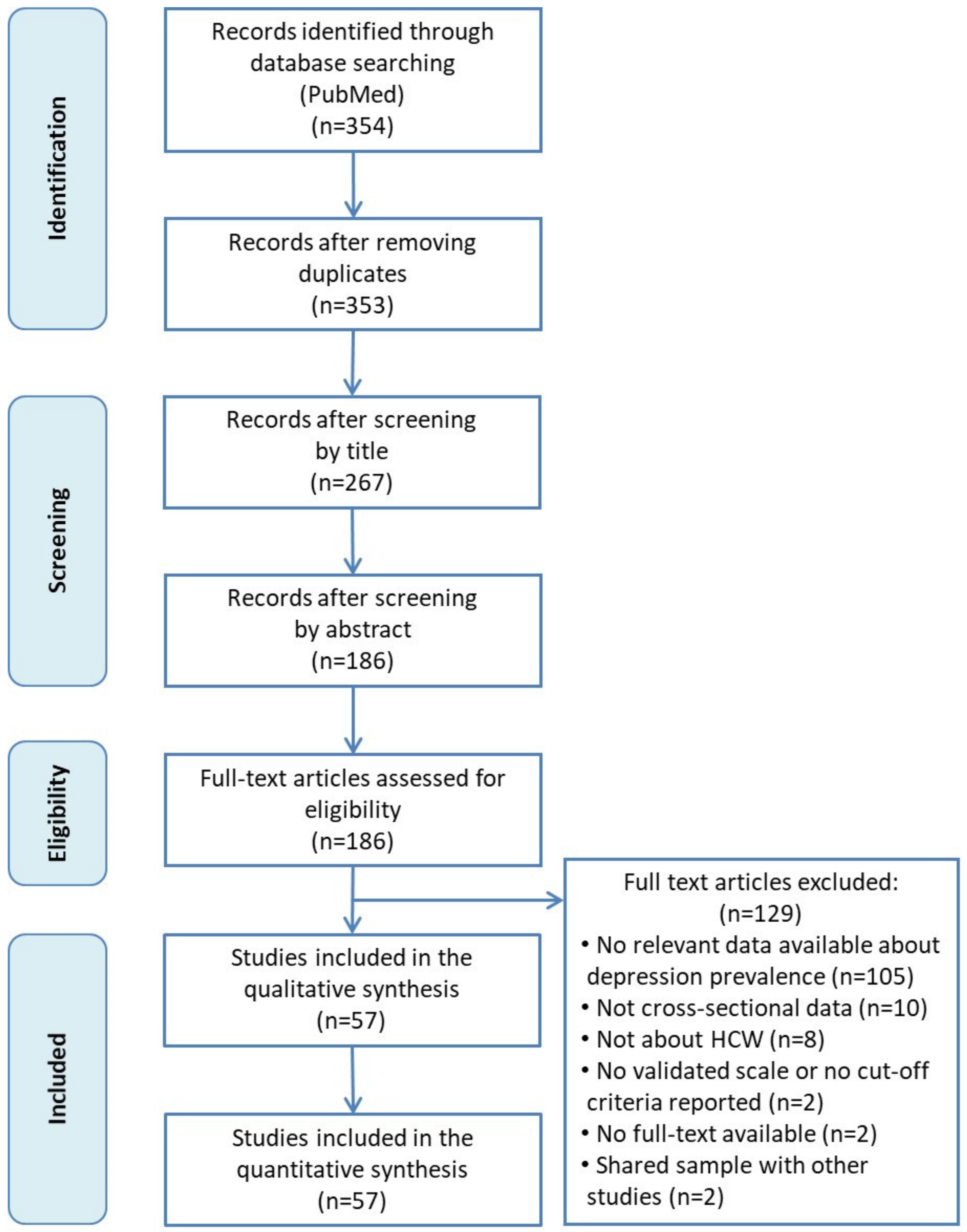
2.1. Search Strategy
2.2. Selection Criteria
2.3. Assessment of Methodological Quality
2.4. Statistical Analysis
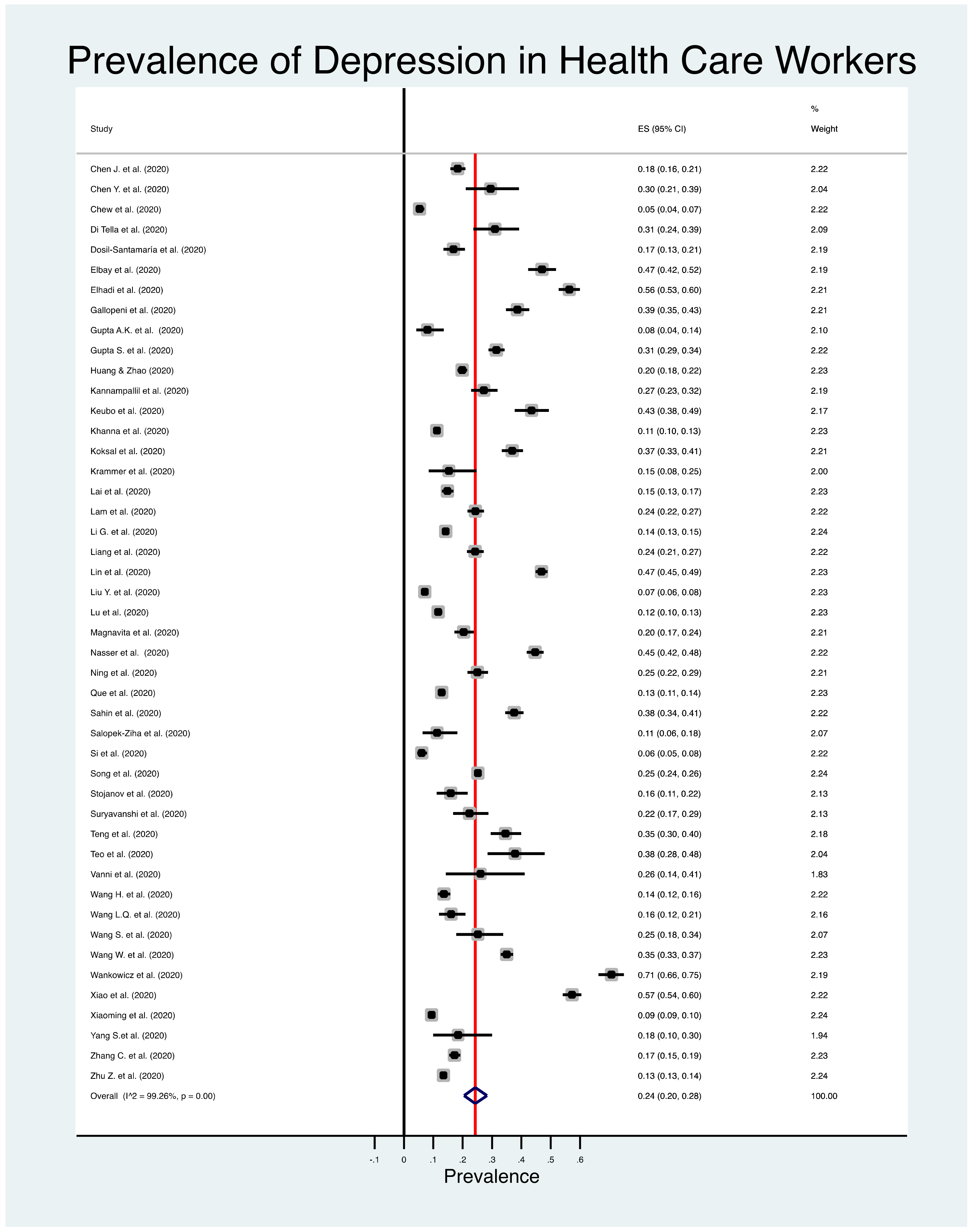
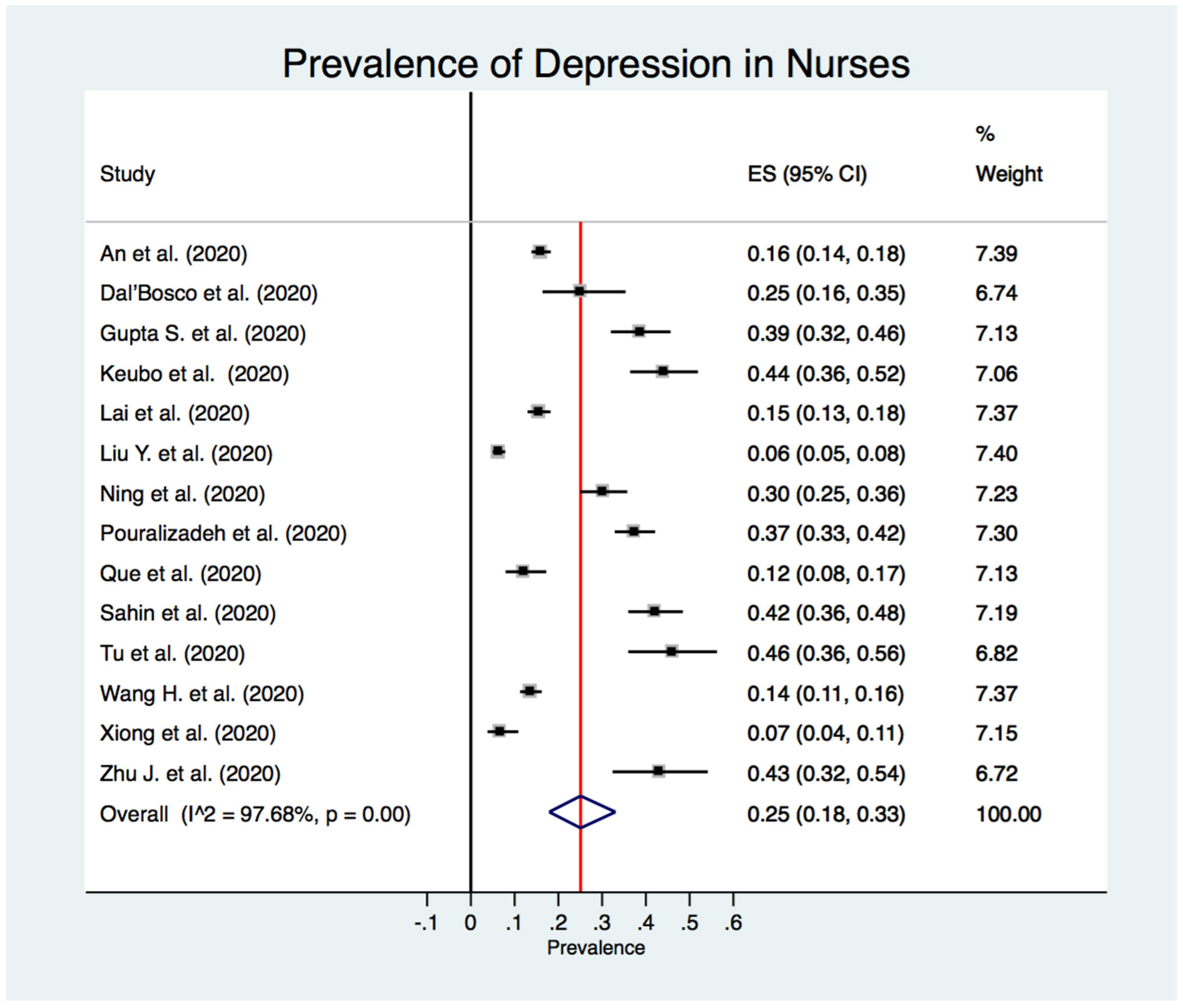
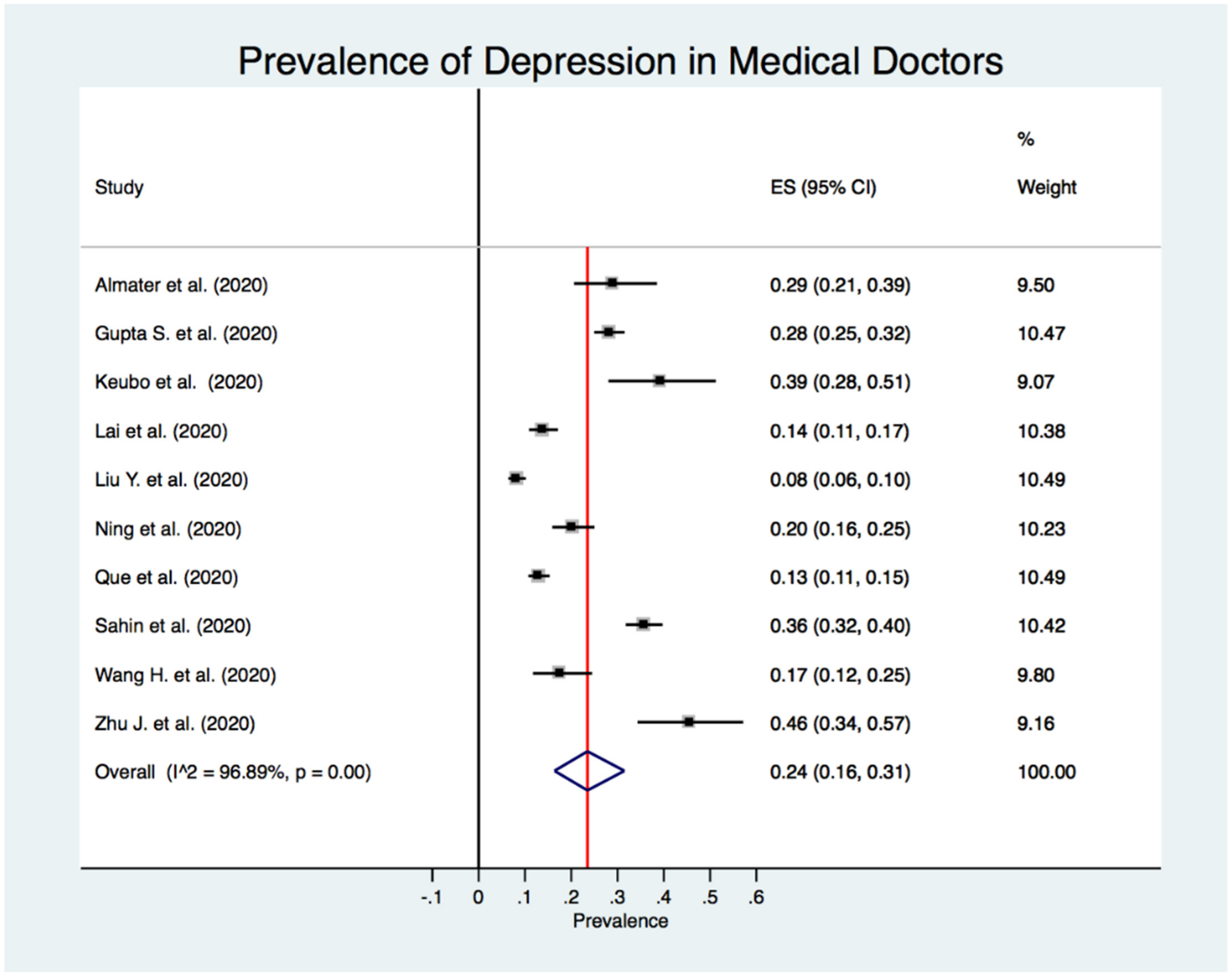
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020#.XqySGbWV4O4.mailto (accessed on 12 December 2020).
- World Health Organization (WHO). COVID-19 Weekly Epidemiological Update; World Health Organization (WHO): Geneva, Switzerland, 2020. [Google Scholar]
- Campion, J.; Javed, A.; Sartorius, N.; Marmot, M. Addressing the public mental health challenge of COVID-19. Lancet Psychiatry 2020, 7, 657–659. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; et al. Survey of Insomnia and Related Social Psychological Factors Among Medical Staff Involved in the 2019 Novel Coronavirus Disease Outbreak. Front. Psychiatry 2020, 11, 306. [Google Scholar] [CrossRef]
- Rana, W.; Mukhtar, S.; Mukhtar, S. Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102080. [Google Scholar] [CrossRef]
- Spoorthy, M.S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic—A review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef]
- Grover, S.; Sahoo, S.; Mehra, A.; Avasthi, A.; Tripathi, A.; Subramanyan, A.; Pattojoshi, A.; Rao, G.; Saha, G.; Mishra, K.; et al. Psychological impact of COVID-19 lockdown: An online survey from India. Indian J. Psychiatry 2020, 62, 354. [Google Scholar] [CrossRef]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.Q.; Tian, Q.; Leng, H.X.; Du, J.L.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosomat. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, L.; Chen, L.; Zhang, X.; Bao, L.; Shi, Y. Mental Health Status of Paediatric Medical Workers in China During the COVID-19 Outbreak. Front. Psychiatry 2020, 11, 702. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Da Silva, F.C.T.; Neto, M.L.R. Psychological effects caused by the COVID-19 pandemic in health professionals: A systematic review with meta-analysis. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2021, 104, 110062. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017; pp. 219–226. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Von Hippel, P.T. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.G.; Higgins, J.P.T. How should meta-regression analyses be undertaken and interpreted? Stat. Med. 2002, 21, 1559–1573. [Google Scholar] [CrossRef]
- Egger, M.; Schneider, M.; Smith, G.D. Meta-analysis Spurious precision? Meta-analysis of observational studies. BMJ 1998, 316, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.P.; Saratzis, A.; Sutton, A.J.; Boucher, R.H.; Sayers, R.D.; Bown, M.J. In meta-analyses of proportion studies, funnel plots were found to be an inaccurate method of assessing publication bias. J. Clin. Epidemiol. 2014, 67, 897–903. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Di Tella, M.; Romeo, A.; Benfante, A.; Castelli, L. Mental health of healthcare workers during the COVID-19 pandemic in Italy. J. Eval. Clin. Pract. 2020, 26, 1583–1587. [Google Scholar] [CrossRef]
- Dosil Santamaría, M.; Ozamiz-Etxebarria, N.; Redondo Rodríguez, I.; Jaureguizar Alboniga-Mayor, J.; Picaza Gorrotxategi, M. Psychological impact of COVID-19 on a sample of Spanish health professionals. Rev. Psiquiatr. Salud Ment. 2020. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Psychological status of healthcare workers during the civil war and COVID-19 pandemic: A cross-sectional study. J. Psychosomat. Res. 2020, 137, 110221. [Google Scholar] [CrossRef]
- Gallopeni, F.; Bajraktari, I.; Selmani, E.; Tahirbegolli, I.A.; Sahiti, G.; Muastafa, A.; Bojaj, G.; Muharremi, V.B.; Tahirbegolli, B. Anxiety and depressive symptoms among healthcare professionals during the Covid-19 pandemic in Kosovo: A cross sectional study. J. Psychosomat. Res. 2020, 137, 110212. [Google Scholar] [CrossRef]
- Gupta, A.K.; Mehra, A.; Niraula, A.; Kafle, K.; Deo, S.P.; Singh, B.; Sahoo, S.; Grover, S. Prevalence of anxiety and depression among the healthcare workers in Nepal during the COVID-19 pandemic. Asian J. Psychiatry 2020, 54, 102260. [Google Scholar] [CrossRef]
- Gupta, S.; Prasad, A.S.; Dixit, P.K.; Padmakumari, P.; Gupta, S.; Abhisheka, K. Survey of prevalence of anxiety and depressive symptoms among 1124 healthcare workers during the coronavirus disease 2019 pandemic across India. Med. J. Armed Forces India 2020, 77, S404–S412. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Kannampallil, T.G.; Goss, C.W.; Evanoff, B.A.; Strickland, J.R.; McAlister, R.P.; Duncan, J. Exposure to COVID-19 patients increases physician trainee stress and burnout. PLoS ONE 2020, 15, e0237301. [Google Scholar] [CrossRef]
- Keubo, F.R.N.; Mboua, P.C.; Tadongfack, T.D.; Tchoffo, E.F.; Tatang, C.T.; Zeuna, J.I.; Noupoue, E.M.; Tsoplifack, C.B.; Folefack, G.O. Psychological distress among health care professionals of the three COVID-19 most affected Regions in Cameroon: Prevalence and associated factors. In Annales Medico-Psychologiques, Revue Psychiatrique; Elsevier Masson: Hoboken, NJ, USA, 2020; Volume 179, pp. 141–146. [Google Scholar] [CrossRef]
- Khanna, R.C.; Honavar, S.G.; Metla, A.L.; Bhattacharya, A.; Maulik, P.K. Psychological impact of COVID-19 on ophthalmologists-in-training and practising ophthalmologists in India. Indian J. Ophthalmol. 2020, 68, 994–998. [Google Scholar] [CrossRef]
- Koksal, E.; Dost, B.; Terzi, Ö.; Ustun, Y.B.; Özdin, S.; Bilgin, S. Evaluation of Depression and Anxiety Levels and Related Factors Among Operating Theater Workers During the Novel Coronavirus (COVID-19) Pandemic. J. Perianesth. Nurs. Off. J. Am. Soc. PeriAnesth. Nurses 2020, 35, 472–477. [Google Scholar] [CrossRef]
- Krammer, S.; Augstburger, R.; Haeck, M.; Maercker, A. Adjustment Disorder, Depression, Stress Symptoms, Corona Related Anxieties and Coping Strategies during the Corona Pandemic (COVID-19) in Swiss Medical Staff. Psychother. Psychosomat. Med. Psychol. 2020, 70, 272–282. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.C.; Arora, T.; Grey, I.; Suen, L.K.P.; Huang, E.Y.-Z.; Li, D.; Lam, K.B.H. Perceived Risk and Protection From Infection and Depressive Symptoms Among Healthcare Workers in Mainland China and Hong Kong During COVID-19. Front. Psychiatry 2020, 11, 686. [Google Scholar] [CrossRef]
- Li, G.; Miao, J.; Wang, H.; Xu, S.; Sun, W.; Fan, Y.; Zhang, C.; Zhu, S.; Zhu, Z.; Wang, W. Psychological impact on women health workers involved in COVID-19 outbreak in Wuhan: A cross-sectional study. J. Neurol. Neurosurg. Psychiatry 2020, 91, 895–897. [Google Scholar] [CrossRef]
- Liang, Y.; Wu, K.; Zhou, Y.; Huang, X.; Zhou, Y.; Liu, Z. Mental Health in Frontline Medical Workers during the 2019 Novel Coronavirus Disease Epidemic in China: A Comparison with the General Population. Int. J. Environ. Res. Public Health 2020, 17, 6550. [Google Scholar] [CrossRef]
- Lin, K.; Yang, B.X.; Luo, D.; Liu, Q.; Ma, S.; Huang, R.; Lu, W.; Majeed, A.; Lee, Y.; Lui, L.M.W.; et al. The Mental Health Effects of COVID-19 on Health Care Providers in China. Am. J. Psychiatry 2020, 177, 635–636. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of Posttraumatic Stress, Anxiety, Depression, Levels of Resilience and Burnout in Spanish Health Personnel during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in Health Care Workers during the COVID-19 Epidemic. A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef] [PubMed]
- Almater, A.; Tobaigy, M.; Younis, A.; Alaqeel, M.; Abouammoh, M. Effect of 2019 coronavirus pandemic on ophthalmologists practicing in Saudi Arabia: A psychological health assessment. Middle East Afr. J. Ophthalmol. 2020, 27, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Naser, A.Y.; Dahmash, E.Z.; Al-Rousan, R.; Alwafi, H.; Alrawashdeh, H.M.; Ghoul, I.; Abidine, A.; Bokhary, M.A.; Al-Hadithi, H.T.; Ali, D.; et al. Mental health status of the general population, healthcare professionals, and university students during 2019 coronavirus disease outbreak in Jordan: A cross-sectional study. Brain Behav. 2020, 10, e01730. [Google Scholar] [CrossRef] [PubMed]
- Ning, X.; Yu, F.; Huang, Q.; Li, X.; Luo, Y.; Huang, Q.; Chen, C. The mental health of neurological doctors and nurses in Hunan Province, China during the initial stages of the COVID-19 outbreak. BMC Psychiatry 2020, 20, 436. [Google Scholar] [CrossRef]
- Pouralizadeh, M.; Bostani, Z.; Maroufizadeh, S.; Ghanbari, A.; Khoshbakht, M.; Alavi, S.A.; Ashrafi, S. Anxiety and depression and the related factors in nurses of Guilan University of Medical Sciences hospitals during COVID-19: A web-based cross-sectional study. Int. J. Afr. Nurs. Sci. 2020, 13, 100233. [Google Scholar] [CrossRef] [PubMed]
- Que, J.; Shi, L.; Deng, J.; Liu, J.; Zhang, L.; Wu, S.; Gong, Y.; Huang, W.; Yuan, K.; Yan, W.; et al. Psychological impact of the COVID-19 pandemic on healthcare workers: A cross-sectional study in China. Gen. Psychiatry 2020, 33, e100259. [Google Scholar] [CrossRef] [PubMed]
- Şahin, M.K.; Aker, S.; Şahin, G.; Karabekiroğlu, A. Prevalence of Depression, Anxiety, Distress and Insomnia and Related Factors in Healthcare Workers During COVID-19 Pandemic in Turkey. J. Community Health 2020, 45, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Salopek-Žiha, D.; Hlavati, M.; Gvozdanović, Z.; Gašić, M.; Placento, H.; Jakić, H.; Klapan, D.; Šimić, H. Differences in Distress and Coping with the COVID-19 Stressor in Nurses and Physicians. Psychiatr. Danub 2020, 32, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Sandesh, R.; Shahid, W.; Dev, K.; Mandhan, N.; Shankar, P.; Shaikh, A.; Rizwan, A. Impact of COVID-19 on the Mental Health of Healthcare Professionals in Pakistan. Cureus 2020, 12, e8974. [Google Scholar] [CrossRef] [PubMed]
- Si, M.Y.; Su, X.Y.; Jiang, Y.; Wang, W.J.; Gu, X.F.; Ma, L.; Li, J.; Zhang, S.K.; Ren, Z.F.; Ren, R.; et al. Psychological impact of COVID-19 on medical care workers in China. Infect. Dis. Poverty 2020, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Fu, W.; Liu, X.; Luo, Z.; Wang, R.; Zhou, N.; Yan, S.; Lv, C. Mental health status of medical staff in emergency departments during the Coronavirus disease 2019 epidemic in China. Brain Behav. Immun. 2020, 88, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Stojanov, J.; Malobabic, M.; Stanojevic, G.; Stevic, M.; Milosevic, V.; Stojanov, A. Quality of sleep and health-related quality of life among health care professionals treating patients with coronavirus disease-19. Int. J. Soc. Psychiatry 2020, 67, 175. [Google Scholar] [CrossRef]
- An, Y.; Yang, Y.; Wang, A.; Li, Y.; Zhang, Q.; Cheung, T.; Ungvari, G.S.; Qin, M.-Z.; An, F.-R.; Xiang, Y.-T. Prevalence of depression and its impact on quality of life among frontline nurses in emergency departments during the COVID-19 outbreak. J. Affect. Disord. 2020, 276, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Suryavanshi, N.; Kadam, A.; Dhumal, G.; Nimkar, S.; Mave, V.; Gupta, A.; Cox, S.R.; Gupte, N. Mental health and quality of life among healthcare professionals during the COVID-19 pandemic in India. Brain Behav. 2020, 10, e01837. [Google Scholar] [CrossRef]
- Teng, Z.; Huang, J.; Qiu, Y.; Tan, Y.; Zhong, Q.; Tang, H.; Wu, H.; Wu, Y.; Chen, J. Mental health of front-line staff in prevention of coronavirus disease 2019. Zhong Nan Da Xue Xue Bao Yi Xue Ban J. Cent. South Univ. Med. Sci. 2020, 45, 613–619. [Google Scholar] [CrossRef]
- Teo, W.Z.Y.; Soo, Y.E.; Yip, C.; Lizhen, O.; Chun-Tsu, L. The psychological impact of COVID-19 on “hidden” frontline healthcare workers. Int. J. Soc. Psychiatry 2020, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Tu, Z.H.; He, J.W.; Zhou, N. Sleep quality and mood symptoms in conscripted frontline nurse in Wuhan, China during COVID-19 outbreak: A cross-sectional study. Medicine 2020, 99, e20769. [Google Scholar] [CrossRef]
- Vanni, G.; Materazzo, M.; Santori, F.; Pellicciaro, M.; Costesta, M.; Orsaria, P.; Cattadori, F.; Pistolese, C.A.; Perretta, T.; Chiocchi, M.; et al. The Effect of Coronavirus (COVID-19) on Breast Cancer Teamwork: A Multicentric Survey. In Vivo 2020, 34, 1685–1694. [Google Scholar] [CrossRef]
- Wang, H.; Huang, D.; Huang, H.; Zhang, J.; Guo, L.; Liu, Y.; Ma, H.; Geng, Q. The psychological impact of COVID-19 pandemic on medical staff in Guangdong, China: A cross-sectional study. Psychol. Med. 2020, 1–9. [Google Scholar] [CrossRef]
- Wang, L.Q.; Zhang, M.; Liu, G.M.; Nan, S.Y.; Li, T.; Xu, L.; Xue, Y.; Wang, L.; Qu, Y.D.; Liu, F. Psychological impact of coronavirus disease (2019) (COVID-19) epidemic on medical staff in different posts in China: A multicenter study. J. Psychiatr. Res. 2020, 129, 198–205. [Google Scholar] [CrossRef]
- Wang, S.; Xie, L.; Xu, Y.; Yu, S.; Yao, B.; Xiang, D. Sleep disturbances among medical workers during the outbreak of COVID-2019. Occup. Med. 2020, 70, 364–369. [Google Scholar] [CrossRef]
- Wang, W.; Song, W.; Xia, Z.; He, Y.; Tang, L.; Hou, J.; Lei, S. Sleep Disturbance and Psychological Profiles of Medical Staff and Non-Medical Staff During the Early Outbreak of COVID-19 in Hubei Province, China. Front. Psychiatry 2020, 11, 733. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. Assessment of Mental Health Factors among Health Professionals Depending on Their Contact with COVID-19 Patients. Int. J. Environ. Res. Public Health 2020, 17, 5849. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Feng, H.; Huang, J.; Wang, M.; Wang, Q.; Lu, X.; Xie, Y.; Wang, X.; Liu, Z.; Hou, B.; et al. The mental health of frontline and non-frontline medical workers during the coronavirus disease 2019 (COVID-19) outbreak in China: A case-control study. J. Affect. Disord. 2020, 275, 210–215. [Google Scholar] [CrossRef]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Xiaoming, X.; Ming, A.; Su, H.; Wo, W.; Jianmei, C.; Qi, Z.; Hua, H.; Xuemei, L.; Lixia, W.; Jun, C.; et al. The psychological status of 8817 hospital workers during COVID-19 Epidemic: A cross-sectional study in Chongqing. J. Affect. Disord. 2020, 276, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Xiong, H.; Yi, S.; Lin, Y. The Psychological Status and Self-Efficacy of Nurses During COVID-19 Outbreak: A Cross-Sectional Survey. Inquiry 2020, 57, 46958020957114. [Google Scholar] [CrossRef]
- Yang, S.; Kwak, S.G.; Ko, E.J.; Chang, M.C. The Mental Health Burden of the COVID-19 Pandemic on Physical Therapists. Int. J. Environ. Res. Public Health 2020, 17, 3723. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, W.; Sun, Y.; Qian, W.; Liu, Z.; Wang, R.; Qi, L.; Yang, J.; Song, X.; Zhou, X.; et al. The prevalence and risk factors of psychological disturbances of frontline medical staff in china under the COVID-19 epidemic: Workload should be concerned. J. Affect. Disord. 2020, 277, 510–514. [Google Scholar] [CrossRef]
- Zhu, J.; Sun, L.; Zhang, L.; Wang, H.; Fan, A.; Yang, B.; Li, W.; Xiao, S. Prevalence and Influencing Factors of Anxiety and Depression Symptoms in the First-Line Medical Staff Fighting Against COVID-19 in Gansu. Front. Psychiatry 2020, 11, 386. [Google Scholar] [CrossRef]
- Zhu, Z.; Xu, S.; Wang, H.; Liu, Z.; Wu, J.; Li, G.; Miao, J.; Zhang, C.; Yang, Y.; Sun, W.; et al. COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. EClinicalMedicine 2020, 24, 100443. [Google Scholar] [CrossRef]
- Chen, J.; Liu, X.; Wang, D.; Jin, Y.; He, M.; Ma, Y.; Zhao, X.; Song, S.; Zhang, L.; Xiang, X.; et al. Risk factors for depression and anxiety in healthcare workers deployed during the COVID-19 outbreak in China. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 56, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhou, H.; Zhou, Y.; Zhou, F. Prevalence of self-reported depression and anxiety among pediatric medical staff members during the COVID-19 outbreak in Guiyang, China. Psychiatry Res. 2020, 288, 113005. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain. Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Dal’Bosco, E.B.; Messias Floriano, L.S.; Skupien, S.V.; Arcaro, G.; Martins, A.R.; Correa Anselmo, A.C. Mental health of nursing in coping with COVID-19 at a regional university hospital. Rev. Bras. Enferm. 2020, 73. [Google Scholar] [CrossRef]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2020, 21–100196. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. medRxiv 2020. [Google Scholar] [CrossRef]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Kang, W.S.; Cho, A.R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef] [PubMed]
- Tomlin, J.; Dalgleish-Warburton, B.; Lamph, G. Psychosocial Support for Healthcare Workers During the COVID-19 Pandemic. Front. Psychol. 2020, 11, 1960. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Publication Year) | Population | Country | Mean Age (SD) | % Females (n) | Sample Size (n) | Response Rate (%) | Sampling Method | Depression Assessment | Time Frame Assessment | Diagnostic Criteria | Prevalence | Quality Assessment * | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | n | ||||||||||||
| Chen J. et al. (2020) | HCW | China | 36.54 (8.57) | 68.63% (619) | 902 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 18.29% | 165 | 7 |
| Chen Y. et al. (2020) | Pediatric HCW | China | 32.6 (6.5) | 90.48% (95) | 105 | 84.68% | NR | SDS | Past several days | ≥53 | 29.52% | 31 | 7 |
| Chew et al. (2020) | HCW | India, Singapore | 29 (NR) | 64.3% (583) | 906 | 90.60% | NR | DASS-21 | Last week | ≥14 | 5.30% | 48 | 8 |
| Di Tella et al. (2020) | HCW | Italy | 42.9 (11.2) | 72.4% (105) | 145 | NR | Convenience sampling | BDI-II | Last 2 weeks | >13 | 31.03% | 45 | 6 |
| Dosil Santamaría et al. (2020) | HCW | Spain | 42.8 (10.2) | 80.29% (338) | 421 | NR | Snowball sampling | DASS-21 | Last week | ≥14 | 16.86% | 71 | 7 |
| Elbay et al.(2020) | HCW | Turkey | 36.05 (8.69) | 56.8% (251) | 442 | NR | Convenience sampling | DASS-21 | Last week | ≥14 | 47.06% | 208 | 7 |
| Elhadi et al. (2020) | HCW | Libya | 33.3 (7.4) | 51.94% (387) | 745 | 93.13% | Convenience sampling | HADS | Last week | >10 | 56.38% | 420 | 8 |
| Gallopeni et al. (2020) | HCW | Kosovo | 39 (10.37) | 61.32% (363) | 592 | NR | NR | HADS | Last week | >10 | 38.68% | 229 | 7 |
| Gupta A.K. et al. (2020) | HCW | Nepal | 29.5 (6.1) | 52.67% (79) | 150 | NR | Snowball sampling | PHQ-9 | Last 2 weeks | ≥10 | 8.00% | 12 | 6 |
| Gupta S. et al. (2020) | HCW | India | NR | 36.12% (406) | 1124 | 79.45% | Quota sampling | HADS | Last week | >7 | 31.49% | 354 | 8 |
| Huang & Zhao (2020) | HCW | China | NR | NR | 2250 | 85.30% | Convenience sampling | CES-D | Last 2 weeks | >28 | 19.82% | 446 | 7 |
| Kannampallil et al. (2020) | HCW | USA | NR | 54.96% (216) | 393 | 28.58% | NR | DASS-21 | Last week | ≥10 | 27.23% | 107 | 6 |
| Keubo et al. (2020) | HCW | Cameroon | NR | 54.45% (159) | 292 | NR | Snowball sampling | HADS | Last week | >10 | 43.49% | 127 | 6 |
| Khanna et al. (2020) | HCW | India | 42.5 (12.05) | 43.44% (1023) | 2355 | NR | NR | PHQ-9 | Last 2 weeks | ≥10 | 11.21% | 264 | 7 |
| Koksal et al. (2020) | HCW | Turkey | 35.6 (8.5) | 70.1% (492) | 702 | NR | NR | HADS | Last week | >7 | 36.89% | 259 | 7 |
| Krammer et al. (2020) | HCW | Switzerland | 42.6 (13.5) | 74.00% (74) | 85 | 76.92% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 15.29% | 13 | 7 |
| Lai et al. (2020) | HCW | China | NR | 76.69% (964) | 1257 | 68.69% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 14.80% | 186 | 8 |
| Lam et al. (2020) | HCW | China | NR | 75.21% (701) | 932 | 59.51% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥9 | 24.36% | 227 | 7 |
| Li et al. (2020) | HCW | China | NR | 100% (4369) | 4369 | 82.17% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 14.21% | 621 | 8 |
| Liang et al. (2020) | HCW | China | NR | 81.31% (731) | 899 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 24.25% | 218 | 7 |
| Lin et al. (2020) | HCW | China | NR | NR | 2316 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | >5 | 46.89% | 1086 | 6 |
| Liu et al. (2020) | Pediatric HCW | China | NR | 85.52% (1737) | 2031 | NR | Convenience sampling | DASS-21 | Last week | ≥14 | 7.09% | 144 | 7 |
| Lu et al. (2020) | HCW | China | NR | 77.64% (1785) | 2299 | 94.88% | NR | HAMD | Last week | ≥7 | 11.66% | 268 | 8 |
| Magnavita et al. (2020) | HCW | Italy | NR | 70.10% (417) | 595 | 73.46% | Convenience sampling | GADS | Last 2 weeks | ≥2 | 20.34% | 121 | 8 |
| Naser et al. (2020) | HCW | Jordan | NR | 56,1% (653) | 1163 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 44.71% | 520 | 7 |
| Ning et al. (2020) | HCW | China | NR | 72.88% (446) | 612 | NR | Snowball sampling | SDS | Past several days | ≥53 | 25.00% | 153 | 7 |
| Que et al. (2020) | HCW | China | 31.06 (6.99) | 69.06% (1578) | 2285 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 12.82% | 293 | 7 |
| Sahin et al. (2020) | HCW | Turkey | NR | 66.03% (620) | 939 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 37.59% | 353 | 7 |
| Salopek-Žiha et al. (2020) | HCW | Croatia | NR | NR | 124 | NR | Convenience sampling | DASS-21 | Last week | ≥14 | 11.29% | 14 | 5 |
| Si et al. (2020) | HCW | China | NR | 70.68% (610) | 863 | 76.00% | Convenience sampling | DASS-21 | Last week | ≥14 | 6.03% | 52 | 8 |
| Song et al. (2020) | HCW | China | 34 (8.2) | 64.3% (NR) | NR | Convenience sampling | CES-D | Last 2 weeks | ≥16 | 25.18% | 3733 | 7 | |
| Stojanov et al. (2020) | HCW | Serbia | 40.5 (8.37) | 66.17% (133) | 201 | NR | NR | SDS | Past several days | ≥60 | 15.92% | 32 | 6 |
| Suryavanshi et al. (2020) | HCW | India | NR | 51.27% (101) | 197 | 20.40% | Snowball sampling | PHQ-9 | Last 2 weeks | ≥10 | 22.34% | 44 | 6 |
| Teng et al. (2020) | HCW | China | NR | NR | 338 | NR | Snowball sampling | PHQ-9 | Last 2 weeks | ≥5 | 34.62% | 117 | 6 |
| Teo et al. (2020) | Laboratory HCW | Singapore | 34 (NR) | 73.77% (90/122) | 103 | 84.43% | NR | SDS | Past several days | ≥60 | 37.86% | 39 | 7 |
| Vanni et al. (2020) | HCW | Italy | 47 (10.37) | 65.22% (30) | 46 | 90.20% | Convenience sampling | DASS-21 | Last week | ≥14 | 26.09% | 12 | 7 |
| Wang H. et al. (2020) | HCW | China | NR | 85.84% (897) | 1045 | 73.18% | Convenience sampling | HADS | Last week | >10 | 13.59% | 142 | 7 |
| Wang L.Q. et al. (2020) | HCW | China | 37 (NR) | 77.37% (212) | 274 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 16.06% | 44 | 6 |
| Wang S. et al. (2020) | Pediatric HCW | China | 33.75 (8.41) | 90.24% (111) | 123 | 52.44% | Convenience sampling | SDS | Past several days | ≥50 | 25.20% | 31 | 7 |
| Wang W. et al. (2020) | HCW | China | 33.5 (8.89) | 64.52% (1291) | 2001 | 72.06% | Convenience sampling | HADS | Last week | >7 | 35.03% | 701 | 8 |
| Wankowicz et al. (2020) | HCW | Poland | 40.25 (5.25) | 52.15% (230) | 441 | NR | NR | PHQ-9 | Last 2 weeks | >5 | 70.75% | 312 | 7 |
| Xiao et al. (2020) | HCW | China | NR | 67.22% (644) | 958 | NR | Convenience sampling | HADS | Last week | >7 | 57.31% | 549 | 6 |
| Xiaoming et al. (2020) | HCW | China | 33.25 (8.26) | 77.93% (6874) | 8817 | 90.62% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 9.41% | 830 | 8 |
| Yang et al. (2020) | Physical therapists | South Korea | NR | 47.69% (31) | 65 | 89.04% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 18.46% | 12 | 7 |
| Zhang et al. (2020) | HCW | China | NR | 82.73% (1293) | 1563 | 80.32% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 17.21% | 269 | 8 |
| Zhu et al. (2020) | HCW | China | NR | 85.03% (4304) | 5062 | 77.07% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 13.45% | 681 | 8 |
| Author (Publication Year) | Population | Country | Mean Age (SD) | % Females (n) | Sample Size (n) | Response Rate (%) | Sampling Method | Depression Assessment | Time Frame Assessment | Diagnostic Criteria | Prevalence | Quality Assessment * | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | n | ||||||||||||
| An et al. (2020) | Nurses | China | 32.2 (7.61) | 90.75% (1001) | 1103 | NR | Snowball sampling | PHQ-9 | Last 2 weeks | ≥10 | 15.96% | 176 | 7 |
| Dal’Bosco et al. (2020) | Nurses | Brazil | NR | 79% (89.8) | 88 | 18.49% | Convenience sampling | HADS | Last week | >7 | 25.00% | 22 | 6 |
| Gupta S. et al. (2020) | Nurses | India | NR | NR | 207 | 79.45% | Quota sampling | HADS | Last week | >7 | 38.65% | 80 | 6 |
| Keubo et al. (2020) | Nurses | Cameroon | NR | NR | 168 | NR | Snowball sampling | HADS | Last week | >10 | 44.05% | 74 | 5 |
| Lai et al. (2020) | Nurses | China | NR | 90.84% (694) | 764 | 68.69% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 15.45% | 118 | 8 |
| Liu Y. et al. (2020) | Nurses | China | NR | NR | 1173 | NR | Convenience sampling | DASS-21 | Last week | ≥14 | 6.31% | 74 | 6 |
| Ning et al. (2020) | Nurses | China | NR | 97.97% (289) | 295 | NR | Snowball sampling | SDS | Past several days | ≥53 | 30.17% | 89 | 6 |
| Pouralizadeh et al. (2020) | Nurses | Iran | 36.34 (8.74) | 95.2% (420) | 441 | NR | NR | PHQ-9 | Last 2 weeks | ≥10 | 37.41% | 165 | 7 |
| Que et al. (2020) | Nurses | China | 35.94 (8.17) | 97.75% (195) | 208 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 12.02% | 25 | 6 |
| Sahin et al. (2020) | Nurses | Turkey | NR | NR | 254 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 42.13% | 107 | 5 |
| Tu et al. (2020) | Frontline Nurses | China | 34.44 (5.85) | 100% (100) | 100 | 100% | Cluster Sampling | PHQ-9 | Last 2 weeks | ≥5 | 46.00% | 46 | 8 |
| Wang H. et al. (2020) | Nurses | China | NR | NR | 773 | 73.18% | Convenience sampling | HADS | Last week | >10 | 13.58% | 105 | 7 |
| Xiong et al. (2020) | Nurses | China | NR | 97.31 (217) | 223 | 61.80% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 6.73% | 15 | 7 |
| Zhu J. et al. (2020) | Frontline Nurses | China | NR | NR | 86 | NR | Convenience sampling | SDS | Past several days | ≥50 | 43.02% | 37 | 5 |
| Author (Publication Year) | Population | Country | Mean Age (SD) | % Females (n) | Sample Size (n) | Response Rate (%) | Sampling Method | Depression Assessment | Time Frame Assessment | Diagnostic Criteria | Prevalence | Quality Assessment * | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | n | ||||||||||||
| Almater et al. (2020) | MD | Saudi Arabia | 32.9 (9.6) | 43.9% (47) | 107 | 30.60% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 28.97% | 31 | 6 |
| Gupta S. et al. (2020) | MD | India | NR | NR | 749 | 79.45% | Quota sampling | HADS | Last week | >7 | 28.17% | 211 | 7 |
| Keubo et al. (2020) | MD | Cameroon | NR | NR | 74 | NR | Snowball sampling | HADS | Last week | >10 | 39.19% | 29 | 5 |
| Lai et al. (2020) | MD | China | NR | 54.77% (270) | 493 | 68.69% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 13.79% | 68 | 8 |
| Liu Y. et al. (2020) | MD | China | NR | NR | 858 | NR | Convenience sampling | DASS-21 | Last week | ≥14 | 8.16% | 70 | 6 |
| Ning et al. (2020) | MD | China | NR | 49.53% (157) | 317 | NR | Snowball sampling | SDS | Past several days | ≥53 | 20.19% | 64 | 6 |
| Que et al. (2020) | MD | China | 33.69 (7.44) | 63.49% (546) | 860 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 12.91% | 111 | 7 |
| Sahin et al. (2020) | MD | Turkey | NR | NR | 580 | NR | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 35.69% | 207 | 6 |
| Wang H. et al. (2020) | MD | China | NR | NR | 149 | 73.18% | Convenience sampling | HADS | Last week | >10 | 17.45% | 26 | 6 |
| Zhu J. et al. (2020) | Frontline MD | China | NR | 64.56% (51) | 79 | NR | Convenience sampling | SDS | Past several days | ≥50 | 45.57% | 36 | 6 |
| Author (Publication Year) | Population | Country | Mean Age (SD) | % Females (n) | Sample Size (n) | Response Rate (%) | Sampling Method | Depression Assessment | Time Frame Assessment | Diagnostic Criteria | Prevalence | Quality Assessment * | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | n | ||||||||||||
| Cai et al. (2020) | Frontline HCW | China | 30.6 (8.8) | 68.82% (819) | 1173 | NR | Non-probabilistic sampling | PHQ-9 | Last 2 weeks | ≥10 | 14.32% | 168 | 7 |
| Kannampallil et al. (2020) | Frontline HCW | USA | NR | 51.38% (112) | 218 | 15.85% | NR | DASS-21 | Last week | ≥10 | 27.98% | 61 | 5 |
| Lai et al. (2020) | Frontline HCW | China | NR | NR | 522 | 68.69% | Convenience sampling | PHQ-9 | Last 2 weeks | ≥10 | 18.01% | 94 | 7 |
| Luceño-Moreno et al. (2020) | Frontline HCW | Spain | 43.88 (10.82) | 86.40% (1228) | 1422 | 92.40% | Non probabilistic sampling | HADS | Last week | ≥7 | 51.34% | 730 | 8 |
| Sandesh et al. (2020) | Frontline HCW | Pakistan | NR | 42.86% (48) | 112 | NR | Convenience sampling | DASS-21 | Last week | ≥14 | 72.32% | 81 | 5 |
| Stojanov et al. (2020) | Frontline HCW | Serbia | 39.1 (7.3) | 65.25% (77) | 118 | NR | NR | SDS | Past several days | ≥60 | 17.80% | 21 | 6 |
| Tu et al. (2020) | Frontline Nurses | China | 34.44 (5.85) | 100% (100) | 100 | 100% | Cluster Sampling | PHQ-9 | Last 2 weeks | ≥5 | 46.00% | 46 | 8 |
| Wang H. et al. (2020) | Frontline HCW | China | NR | NR | 401 | 73.18% | Convenience sampling | HADS | Last week | >10 | 16.46% | 66 | 7 |
| Wang W. et al. (2020) | Frontline HCW | China | NR | 59.46% (393) | 661 | 72.06% | Convenience sampling | HADS | Last week | >7 | 45.99% | 304 | 8 |
| Wankowicz et al. (2020) | Frontline HCW | Poland | 40.47 (4.93) | 56.31% (116) | 206 | NR | NR | PHQ-9 | Last 2 weeks | >5 | 99.51% | 205 | 6 |
| Zhou et al. (2020) | Frontline HCW | China | 35.77 (8.13) | 81.19% (492) | 606 | NR | NR | PHQ-9 | Last 2 weeks | >5 | 57.59% | 349 | 7 |
| Zhu J. et al. (2020) | Frontline HCW | China | 34.16 (8.06) | 83.03% (137) | 165 | NR | Convenience sampling | SDS | Past several days | ≥50 | 44.24% | 73 | 6 |
| Healthcare Workers | Nurses | Medical Doctors | Frontline Healthcare Workers | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. Studies | Prevalence (%) (95% CI) | p * | No. Studies | Prevalence (%) (95% CI) | p * | No. Studies | Prevalence (%) (95% CI) | p * | No. Studies | Prevalence (%) (95% CI) | p * | |
| Depression assessment | 0.531 | 0.636 | 0.964 | 0.600 | ||||||||
| PHQ-9 | 20 | 23 (17–29) | 7 | 23 (14–34) | 4 | 22 (11–35) | 5 | 50 (18–81) | ||||
| HADS | 43 | 43 (35–51) | 4 | 29 (14–48) | 3 | 27 (18–38) | 2 | 51 (44–58) | ||||
| DASS-21 | 9 | 16 (9–24) | 1 | 6 (5–8) | 1 | 8 (6–10) | 3 | 37 (19–57) | ||||
| SDS | 5 | 26 (20–32) | 2 | 33 (28–38) | 2 | 25 (21–29) | 2 | 32 (27–38) | ||||
| CES-D | 2 | 24 (24–25) | - | - | - | - | - | - | ||||
| Other (BDI-II/HAMD/GADS) | 3 | 20 (11–31) | - | - | - | - | - | - | ||||
| Country | 0.087 | 0.031 | 0.067 | 0.235 | ||||||||
| China | 23 | 21 (16–25) | 8 | 21 (15–27) | 6 | 18 (12–24) | 7 | 33 (19–49) | ||||
| Other | 23 | 28 (21–36) | 6 | 38 (33–43) | 4 | 32 (27–38) | 5 | 57 (25–86) | ||||
| Sampling method | 0.803 | 0.058 | 0.508 | 0.900 | ||||||||
| Convenience | 29 | 23 (19–28) | 8 | 19 (11–27) | 7 | 22 (13–32) | 5 | 38 (21–57) | ||||
| Other | 7 | 25 (18–33) | 5 | 34 (21–48) | 3 | 28 (20–36) | 3 | 36 (10–63) | ||||
| Quality rating | 0.440 | 0.356 | 0.314 | 0.307 | ||||||||
| Medium (< 7) | 11 | 28 (19–37) | 8 | 29 (15–44) | 7 | 27 (15–40) | 5 | 55 (18–90) | ||||
| High (≥ 7) | 35 | 23 (19–27) | 6 | 21 (13–30) | 3 | 18 (12–24) | 7 | 34 (20–50) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olaya, B.; Pérez-Moreno, M.; Bueno-Notivol, J.; Gracia-García, P.; Lasheras, I.; Santabárbara, J. Prevalence of Depression among Healthcare Workers during the COVID-19 Outbreak: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3406. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153406
Olaya B, Pérez-Moreno M, Bueno-Notivol J, Gracia-García P, Lasheras I, Santabárbara J. Prevalence of Depression among Healthcare Workers during the COVID-19 Outbreak: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(15):3406. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153406
Chicago/Turabian StyleOlaya, Beatriz, María Pérez-Moreno, Juan Bueno-Notivol, Patricia Gracia-García, Isabel Lasheras, and Javier Santabárbara. 2021. "Prevalence of Depression among Healthcare Workers during the COVID-19 Outbreak: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 15: 3406. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153406