
How to Predict the Suitability for Corneal Donorship?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Donor Exclusion Criteria
2.2. Donor Cornea Retrieval and Culture
2.3. Investigated Factors
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Donors
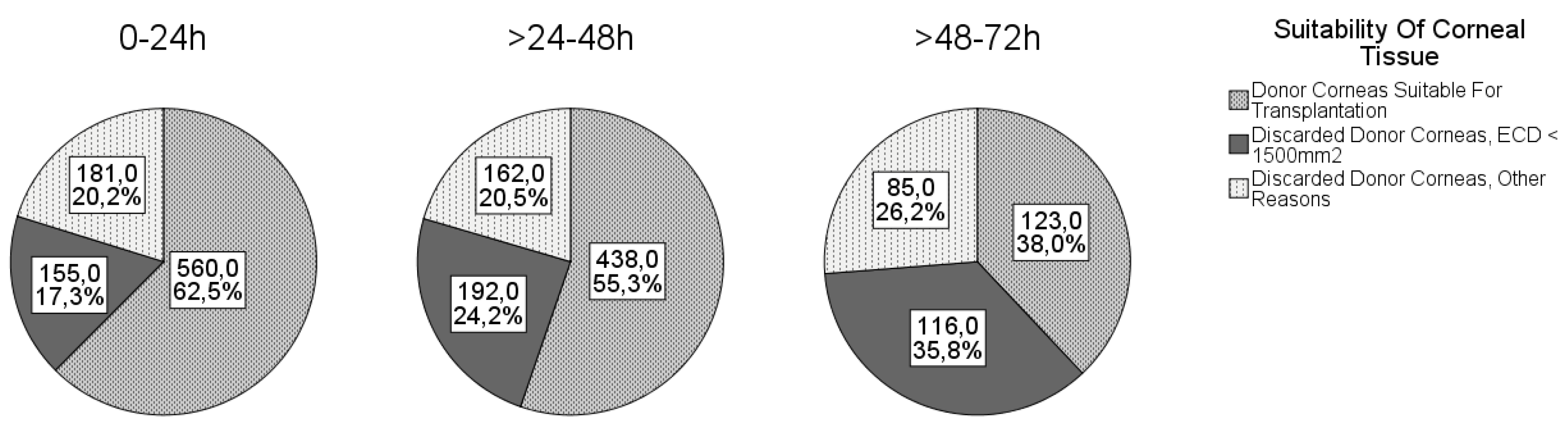
3.2. Causes of Disqualification
3.3. Associations
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seitz, B. Präsentation zum Deutschen Keratoplastikregister 2018 DOG-Sektion Kornea. Available online: https://www.dog.org/?cat=121#6; https://www.dog.org/wp-content/uploads/2010/02/KPL-Register-2018-f%C3%BCr-DOG-WEBSITE.pdf (accessed on 1 December 2019).
- De Sanctis, U.; Alovisi, C.; Bauchiero, L.; Caramello, G.; Girotto, G.; Panico, C.; Vinai, L.; Genzano, F.; Amoroso, A.; Grignolo, F. Changing trends in corneal graft surgery: a ten-year review. Int. J. Ophthalmol. 2016, 9, 48–52. [Google Scholar] [CrossRef]
- Eye Bank Association of America. Eye Banking Statistical Report; Eye Bank Association of America: Washington, DC, USA, 2016. [Google Scholar]
- Dritter Bericht der Bundesregierung über die Situation der Versorgung der Bevölkerung mit Gewebe und Gewebezubereitungen 2018; Deutscher Bundestag: Berlin Germany, 2018.
- Gain, P.; Jullienne, R.; He, Z.; Aldossary, M.; Acquart, S.; Cognasse, F.; Thuret, G. Global Survey of Corneal Transplantation and Eye Banking. JAMA Ophthalmol. 2016, 134, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Siegmund-Schultze, N. Gewinnung von Spenderhornhäuten und Führen einer Gewebebank: Neue Richtlinie verabschiedet. Dtsch Arztebl Int. 2014, 111, 1356. [Google Scholar]
- Gavrilov, J.-C.; Borderie, V.M.; Laroche, L.; Delbosc, B. Influencing factors on the suitability of organ-cultured corneas. Eye 2010, 24, 1227–1233. [Google Scholar] [CrossRef] [Green Version]
- Gain, P.; Thuret, G.; Chiquet, C.; Rizzi, P.; Pugniet, J.L.; Acquart, S.; Colpart, J.J.; Le Petit, J.C.; Maugery, J. Cornea procurement from very old donors: post organ culture cornea outcome and re-cipient graft outcome. Br. J. Ophthalmol. 2002, 86, 404–411. [Google Scholar] [CrossRef] [Green Version]
- Krohn, J.; Høvding, G. The influence of donor age and cause of death on corneal endothelial cell density. Acta Ophthalmol. Scand. 2005, 83, 746–750. [Google Scholar] [CrossRef]
- Galgauskas, S.; Norvydaite, D.; Krasauskaite, D.; Stech, S.; Ašoklis, R.S. Age-related changes in corneal thickness and endothelial characteristics. Clin. Interv. Aging 2013, 8, 1445–1450. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, M.J.; Armitage, W.J.; A Jones, M.N.; Kaye, S.B.; Larkin, D.F.P.; Tole, D.; Prydal, J. The impact of donor age and endothelial cell density on graft survival following penetrating keratoplasty: Table 1. Br. J. Ophthalmol. 2015, 100, 986–989. [Google Scholar] [CrossRef]
- Gipson, I.K. Age-Related Changes and Diseases of the Ocular Surface and Cornea. Investig. Opthalmology Vis. Sci. 2013, 54, ORSF48–ORSF53. [Google Scholar] [CrossRef] [Green Version]
- Schaub, F.; Pohl, L.; Enders, P.; Adler, W.; Bachmann, B.O.; Cursiefen, C.; Heindl, L.M. Impact of corneal donor lens status on two-year course and outcome of Descemet membrane endothelial keratoplasty (DMEK). Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 2407–2414. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.W.; Cho, K.J.; Kim, H.K.; Lee, J.K.; Gore, P.K.; McCartney, M.D.; Chuck, R.S. Analyses of Factors Affecting Endothelial Cell Density in an Eye Bank Corneal Donor Database. Cornea 2016, 35, 1206–1210. [Google Scholar] [CrossRef]
- Snellingen, T.; Rao, G.N.; Shrestha, J.K.; Huq, F.; Cheng, H. Quantitative and Morphological Characteristics of the Human Corneal Endothelium in Relation to Age, Gender, and Ethnicity in Cataract Populations of South Asia. Cornea 2001, 20, 55–58. [Google Scholar] [CrossRef]
- Lass, J.H.; Beck, R.W.; Benetz, B.A.; Dontchev, M.; Gal, R.L.; Holland, E.J.; Kollman, C.; Mannis, M.J.; Price, F.; Raber, I.; et al. Baseline factors related to endothelial cell loss following penetrating keratoplasty. Arch. Ophthalmol. 2011, 129, 1149–1154. [Google Scholar] [CrossRef] [Green Version]
- McGlumphy, E.J.; Margo, J.A.; Haidara, M.; Brown, C.H.; Hoover, C.K.; Munir, W.M. Predictive Value of Corneal Donor Demographics on Endothelial Cell Density. Cornea 2018, 37, 1159–1162. [Google Scholar] [CrossRef]
- Inoue, K.; Tokuda, Y.; Inoue, Y.; Amano, S.; Oshika, T.; Inoue, J. Corneal endothelial cell morphology in patients undergoing cata-ract surgery. Cornea 2002, 21, 360–363. [Google Scholar] [CrossRef]
- Scherer, W.J. Corneal endothelial cell density and cardiovascular mortality. Clin. Anat. 2018, 31, 927–936. [Google Scholar] [CrossRef]
- Spelsberg, H.; Reinhard, T.; Sengler, U.; Daeubener, W.; Sundmacher, R. Organ-cultured corneal grafts from septic donors: a retrospective study. Eye 2002, 16, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Armitage, W.J.; Jones, M.N.A.; Zambrano, I.; Carley, F.; Tole, D.M. The Suitability of Corneas Stored by Organ Culture for Penetrating Keratoplasty and Influence of Donor and Recipient Factors on 5-Year Graft Survival. Investig. Opthalmology Vis. Sci. 2014, 55, 784–791. [Google Scholar] [CrossRef]
- Redbrake, C.; Sieben, P.; Salla, S.; Reim, M. Einfluß der Grunderkrankung des Spenders auf die Endothelzellzahl bei humanen Hornhäuten. Klinische Monatsblätter für Augenheilkunde 1995, 206, 46–48. [Google Scholar] [CrossRef] [PubMed]
- Böhringer, D.; Reinhard, T.; Spelsberg, H.; Sundmacher, R. Influencing factors on chronic endothelial cell loss characterised in a homogeneous group of patients. Br. J. Ophthalmol. 2002, 86, 35–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parekh, M.; Salvalaio, G.; Ferrari, S.; Frigo, A.C.; Griffoni, C.; Grassetto, A.; Ruzza, A.; Camposampiero, D.; Ponzin, D. Effect of postmortem interval on the Graft Endothelium During Preservation and After Transplantation for Keratoconus. Cornea 2013, 32, 842–846. [Google Scholar] [CrossRef]
- Richtlinie zur Gewinnung von Spenderhornhäuten und zum Führen einer Augenhornhautbank; Deutsches Aerzteblatt; Bundesaerztekammer Deutschland: Berlin, Germany, 2014.
- ChandraSekar, A. Post mortem retrieval time limits and time from retrieval to processing for ocular tissue. In Proceedings of the Meeting of the Joint United Kingdom (UK) Blood Transfusion and Tissue Transplantation Ser-vices Professional Advisory Committee, 4 March 2016. [Google Scholar]
- Medicine USNLo. Study Record Detail: Cornea Donor Study (CDS). Available online: https://clinicaltrials.gov/ct2/show/study/NCT00006411?show_desc=Y#desc (accessed on 8 July 2019).
- Committee JUKUBTaTTSPA. Guidelines for the Blood Transfusion Services: 21.12: Ocular Tissue Retrieval, Processing and Storage. Available online: https://www.transfusionguidelines.org/red-book/chapter-21-tissue-banking-tissue-retrieval-and-processing/21-12-ocular-tissue-retrieval-and-storage (accessed on 8 July 2019).
- Linke, S.J.; Eddy, M.-T.; Bednarz, J.; Fricke, O.H.; Wulff, B.; Schröder, A.-S.; Hassenstein, A.; Klemm, M.; Püschel, K.; Richard, G.; et al. Thirty years of cornea cultivation: long-term experience in a single eye bank. Acta Ophthalmol. 2012, 91, 571–578. [Google Scholar] [CrossRef]
- Chen, Y.; Tsao, S.W.; Heo, M.; Gore, P.K.; McCarthy, M.D.; Chuck, R.S.; Channa, P. Age-Stratified Analysis of Diabetes and Pseudophakia Effects on Corneal Endothelial Cell Density: A Retrospective Eye Bank Study. Cornea 2017, 36, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Sugar, J.; Mitchelson, J.; Kraff, M. Endothelial Trauma and Cell Loss From Intraocular Lens Insertion. Arch. Ophthalmol. 1978, 96, 449–450. [Google Scholar] [CrossRef]
- Higa, A.; Sakai, H.; Sawaguchi, S.; Iwase, A.; Tomidokoro, A.; Amano, S.; Araie, M. Corneal Endothelial Cell Density and Associated Factors in a Population-Based Study in Japan: The Kumejima Study. Am. J. Ophthalmol. 2010, 149, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Nioi, M.; Napoli, P.E.; Demontis, R.; Locci, E.; Fossarello, M.; D’Aloja, E. Morphological analysis of corneal findings modifications after death: A preliminary OCT study on an animal model. Exp. Eye Res. 2018, 169, 20–27. [Google Scholar] [CrossRef]
- Napoli, P.E.; Nioi, M.; Gabiati, L.; Laurenzo, M.; De-Giorgio, F.; Scorcia, V.; Grassi, S.; D’Aloja, E.; Fossarello, M. Repeatability and reproducibility of post-mortem central corneal thickness measurements using a portable optical coherence tomography system in humans: a prospective multicenter study. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Napoli, P.E.; Nioi, M.; D’Aloja, E.; Fossarello, M. The Bull’s Eye Pattern of the Tear Film in Humans during Visual Fixation on En-Face Optical Coherence Tomography. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]


{kind=link}
| Postmortem interval >72 h. Diseases affecting the central nervous system:
Active systemical infections (bacterial sepsis is no absolute contraindication, as bacterial contamination can be detected during tissue culture). Donors who had one of the following infections:
Donors who possibly had one of the following diseases:
Corneal/local infection from:
Malignant tumors of the ocular fundus (e.g., retinoblastoma, uveal melanoma). High risk for infection due to travel record. Exposure to cyanide, lead, mercury, gold. Shortly received vaccination with live vaccine with risk for transmission (e.g., rabies). Recipients of heterografts or xenografts. Hematological neoplasia (e.g., leukemia, lymphoma, MDS, MPN). Relative contraindication:
|
| ECD < 1500 mm2; ECD < 2000 mm2 (as optic grafts) and/or corneal culture overdue (storage over 34 days); Positive serology in the last blood sample; Microbial contamination; Corneal morphology e.g., scars, opacities; Damage of the DSAEK preparation. |
| Cause of Death/CPR | Male | Female | Total |
|---|---|---|---|
| Cardiovascular/cerebrovascular disease n (%) (n = 837) | 186 (38.2%) | 142 (40.6%) | 328 (39.2%) |
| Cancer n (%) (n = 836) | 181 (37.2%) | 113 (32.3%) | 294 (35.2%) |
| Sepsis n (%) (n = 848) | 71 (14.4%) | 64 (18.1%) | 135 (15.9%) |
| CPR n (%) (n = 928) | 24 (4.4%) | 9 (2.3%) | 33 (3.6%) |
| Male | Female | |
|---|---|---|
| Mean ECD ± SD (cells/mm2) | 1944 ± 622 | 2018 ± 581 |
| Minimum (cells/mm2) | 32 | 118 |
| Maximum (cells/mm2) | 3272 | 3142 |
| Phakic eyes | 799 (68.9%) | 473 (55.6%) |
| Pseudophakic eyes | 352 (30.3%) | 369 (43.4%) |
| Aphakic eyes | 9 (0.8%) | 8 (0.9%) |
| Suitable | Discarded | |
|---|---|---|
| No (%) (n = 2032) | 1127 (55.5%) | 905 (44.5%) |
| Gender (n = 2028) | ||
| Corneas from male donors (%) | 622 (53.3%) | 544 (46.7%) |
| Corneas from female donors (%) | 503 (58.4%) | 359 (41.6%) |
| Side (n = 2032) | ||
| Right corneas (%) | 573 (56.3%) | 445 (43.7%) |
| Left corneas (%) | 554 (54.6%) | 460 (45.4%) |
| Lens status (n = 2014) | ||
| Phakic (%) | 812 (63.6%) | 464 (36.4%) |
| Pseudophakic (%) | 302 (41.9%) | 419 (58.1%) |
| Aphakic (%) | 7 (41.2%) | 10 (58.8%) |
| Decade of Life | ECD ± SD (cells/mm2) | n |
|---|---|---|
| <50 years | 2316 ± 47 | 63 |
| 50–59 years | 2233 ± 49 | 166 |
| 60–69 years | 2137 ± 59 | 325 |
| 70–79 years | 1949 ± 58 | 541 |
| 80–89 years | 1846 ± 63 | 613 |
| ≥90 years | 1839 ± 59 | 147 |
| Parameter | Estimate ECD ± SD (cells/mm2) | 95% CI (cells/mm2) | p-Value |
|---|---|---|---|
| Intercept | 2919 ± 149 | (2626; 3212) | |
| Sex (ref: female) | |||
| Male | −189 ± 44 | (−275; −102) | <0.001 |
| Age (year) | −6 ± 2 | (−10; −2) | 0.001 |
| DEI (hour) | −7 ± 2 | (−10; −5) | <0.001 |
| Lens status (ref: phakic) | |||
| Aphakic | −87 ± 156 | (−393; 218) | 0.574 |
| Pseudophakic | −378 ± 42 | (−461; −295) | <0.001 |
| Odds Ratio | 95% CI for Odds Ratio | Regression Coefficient b | p-Value | |
|---|---|---|---|---|
| Age | 0.99 | (0.98; 0.99) | −0.01 (−0.02; −0.01) | p = 0.001 |
| DEI | 0.98 | (0.97; 0.98) | −0.02 (−0.03; −0.02) | p < 0.001 |
| Lens status (pseudophakic) | 0.48 | (0.39; 0.60) | −0.73 (−0.96; −0.52) | p < 0.001 |
| Sex (male) | 0.72 | (0.59; 0.89) | −0.32 (−0.52; −0.12) | p = 0.002 |
| CPR (no) | 0.45 | (0.25; 0.81) | −0.80 (−1.56; −0.25) | p = 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schön, F.; Gericke, A.; Bu, J.B.; Apel, M.; Poplawski, A.; Schuster, A.K.; Pfeiffer, N.; Wasielica-Poslednik, J. How to Predict the Suitability for Corneal Donorship? J. Clin. Med. 2021, 10, 3426. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153426
Schön F, Gericke A, Bu JB, Apel M, Poplawski A, Schuster AK, Pfeiffer N, Wasielica-Poslednik J. How to Predict the Suitability for Corneal Donorship? Journal of Clinical Medicine. 2021; 10(15):3426. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153426
Chicago/Turabian StyleSchön, Franziska, Adrian Gericke, Julia Bing Bu, Melissa Apel, Alicia Poplawski, Alexander K. Schuster, Norbert Pfeiffer, and Joanna Wasielica-Poslednik. 2021. "How to Predict the Suitability for Corneal Donorship?" Journal of Clinical Medicine 10, no. 15: 3426. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153426