
Serum Sclerostin Is Associated with Peripheral and Central Systolic Blood Pressure in Pediatric Patients with Primary Hypertension

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Ethical Issues
2.3. Clinical Parameters
2.4. Serum Sclerostin
2.5. Biochemical Parameters
2.6. Blood Pressure and Parameters of Arterial Damage
2.7. Statistical Analysis
3. Results
3.1. Clinical, Laboratory Parameters, Blood Pressure, and Arterial Damage
3.2. Sclerostin and Parameters of Calcium-Phosphate Metabolism
3.3. Correlations of Sclerostin with Clinical and Biochemical Parameters, Blood Pressure, and Parameters of Arterial Damage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J. Hypertens 2016, 34, 1887–1920. [Google Scholar] [CrossRef] [Green Version]
- Gupta-Malhotra, M.; Banker, A.; Shete, S.; Hashmi, S.S.; Tyson, J.E.; Barratt, M.S.; Hecht, J.T.; Milewicz, D.M.; Boerwinkle, E. Essential hypertension vs. secondary hypertension among children. Am. J. Hypertens 2015, 28, 73–80. [Google Scholar] [CrossRef]
- Litwin, M.; Feber, J.; Niemirska, A.; Michałkiewicz, J. Primary hypertension is a disease of premature vascular aging associated with neuro-immuno-metabolic abnormalities. Pediatr. Nephrol. 2016, 31, 185–194. [Google Scholar] [CrossRef] [Green Version]
- Skrzypczyk, P.; Stelmaszczyk-Emmel, A.; Szyszka, M.; Ofiara, A.; Pańczyk-Tomaszewska, M. Circulating calcification inhibitors are associated with arterial damage in pediatric patients with primary hypertension. Pediatr. Nephrol. 2021. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Winkler, D.G.; Sutherland, M.K.; Geoghegan, J.C.; Yu, C.; Hayes, T.; Skonier, J.E.; Shpektor, D.; Jonas, M.; Kovacevich, B.R.; Staehling-Hampton, K.; et al. Osteocyte control of bone formation via sclerostin, a novel BMP antagonist. EMBO J. 2003, 22, 6267–6276. [Google Scholar] [CrossRef] [Green Version]
- Rao, T.P.; Kühl, M. An updated overview on Wnt signaling pathways: A prelude for more. Circ. Res. 2010, 106, 1798–1806. [Google Scholar] [CrossRef]
- Delgado-Calle, J.; Sato, A.Y.; Bellido, T. Role and mechanism of action of sclerostin in bone. Bone 2017, 96, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Matsumoto, T. Sclerostin: From bench to bedside. J. Bone Min. Metab. 2021, 39, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Liao, R.; Wang, L.; Li, J.; Sun, S.; Xiong, Y.; Li, Y.; Han, M.; Jiang, H.; Anil, M.; Su, B. Vascular calcification is associated with Wnt-signaling pathway and blood pressure variability in chronic kidney disease rats. Nephrology (Carlton) 2020, 25, 264–272. [Google Scholar] [CrossRef]
- Didangelos, A.; Yin, X.; Mandal, K.; Baumert, M.; Jahangiri, M.; Mayr, M. Proteomics characterization of extracellular space components in the human aorta. Mol. Cell Proteom. 2010, 9, 2048–2062. [Google Scholar] [CrossRef] [Green Version]
- Morales-Santana, S.; García-Fontana, B.; García-Martín, A.; Rozas-Moreno, P.; García-Salcedo, J.A.; Reyes-García, R.; Muñoz-Torres, M. Atherosclerotic disease in type 2 diabetes is associated with an increase in sclerostin levels. Diabetes Care 2013, 36, 1667–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hampson, G.; Edwards, S.; Conroy, S.; Blake, G.M.; Fogelman, I.; Frost, M.L. The relationship between inhibitors of the Wnt signalling pathway (Dickkopf-1(DKK1) and sclerostin), bone mineral density, vascular calcification and arterial stiffness in post-menopausal women. Bone 2013, 56, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, A.; Privitera, F.; Pulvirenti, I.; Canzonieri, E.; Rapisarda, R.; Fiore, C.E. The relationship between inhibitors of the Wnt signalling pathway (sclerostin and Dickkopf-1) and carotid intima-media thickness in postmenopausal women with type 2 diabetes mellitus. Diabetes Vasc. Dis. Res. 2014, 11, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, A.; Fiore, V.; Rapisarda, R.; Sidoti, M.H.; Xourafa, A.; Catalano, A.; Tringali, G.; Zanoli, L.; Signorelli, S.S.; Fiore, C.E. Sclerostin is a possible candidate marker of arterial stiffness: Results from a cohort study in Catania. Mol. Med. Rep. 2017, 15, 3420–3424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thambiah, S.; Roplekar, R.; Manghat, P.; Fogelman, I.; Fraser, W.D.; Goldsmith, D.; Hampson, G. Circulating sclerostin and Dickkopf-1 (DKK1) in predialysis chronic kidney disease (CKD): Relationship with bone density and arterial stiffness. Calcif. Tissue Int. 2012, 90, 473–480. [Google Scholar] [CrossRef]
- Gravani, F.; Papadaki, I.; Antypa, E.; Nezos, A.; Masselou, K.; Ioakeimidis, D.; Koutsilieris, M.; Moutsopoulos, H.M.; Mavragani, C.P. Subclinical atherosclerosis and impaired bone health in patients with primary Sjogren’s syndrome: Prevalence, clinical and laboratory associations. Arthritis Res. Ther. 2015, 17, 99. [Google Scholar] [CrossRef] [Green Version]
- Paccou, J.; Mentaverri, R.; Renard, C.; Liabeuf, S.; Fardellone, P.; Massy, Z.A.; Brazier, M.; Kamel, S. The relationships between serum sclerostin, bone mineral density, and vascular calcification in rheumatoid arthritis. J. Clin. Endocrinol. Metab. 2014, 99, 4740–4748. [Google Scholar] [CrossRef] [Green Version]
- Kirmani, S.; Amin, S.; McCready, L.K.; Atkinson, E.J.; Melton, L.J., 3rd; Müller, R.; Khosla, S. Sclerostin levels during growth in children. Osteoporos Int. 2012, 23, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.C.; Hsu, B.G.; Liou, H.H.; Lee, C.J.; Wang, J.H. Serum levels of sclerostin as a potential biomarker in central arterial stiffness among hypertensive patients. BMC Cardiovasc. Disord. 2018, 18, 214. [Google Scholar] [CrossRef] [Green Version]
- Kułaga, Z.; Litwin, M.; Tkaczyk, M.; Palczewska, I.; Zajączkowska, M.; Zwolińska, D.; Krynicki, T.; Wasilewska, A.; Moczulska, A.; Morawiec-Knysak, A.; et al. Polish 2010 growth references for school-aged children and adolescents. Eur. J. Pediatr. 2011, 170, 599–609. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Rusińska, A.; Płudowski, P.; Walczak, M.; Borszewska-Kornacka, M.K.; Bossowski, A.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dobrzańska, A.; Franek, E.; Helwich, E.; et al. Vitamin D Supplementation Guidelines for General Population and Groups at Risk of Vitamin D Deficiency in Poland-Recommendations of the Polish Society of Pediatric Endocrinology and Diabetes and the Expert Panel With Participation of National Specialist Consultants and Representatives of Scientific Societies-2018 Update. Front. Endocrinol. (Lausanne) 2018, 9, 246. [Google Scholar] [CrossRef]
- Kułaga, Z.; Litwin, M.; Grajda, A.; Kułaga, K.; Gurzkowska, B.; Góźdź, M.; Pan, H. Oscillometric blood pressure percentiles for Polish normal-weight school-aged children and adolescents. J. Hypertens 2012, 30, 1942–1954. [Google Scholar] [CrossRef]
- Flynn, J.T.; Daniels, S.R.; Hayman, L.L.; Maahs, D.M.; McCrindle, B.W.; Mitsnefes, M.; Zachariah, J.P.; Urbina, E.M. Update: Ambulatory blood pressure monitoring in children and adolescents: A scientific statement from the American Heart Association. Hypertension 2014, 63, 1116–1135. [Google Scholar] [CrossRef]
- Doyon, A.; Kracht, D.; Bayazit, A.K.; Deveci, M.; Duzova, A.; Krmar, R.T.; Litwin, M.; Niemirska, A.; Oguz, B.; Schmidt, B.M.; et al. Carotid artery intima-media thickness and distensibility in children and adolescents: Reference values and role of body dimensions. Hypertension 2013, 62, 550–556. [Google Scholar] [CrossRef] [Green Version]
- Reusz, G.S.; Cseprekal, O.; Temmar, M.; Kis, E.; Cherif, A.B.; Thaleb, A.; Fekete, A.; Szabó, A.J.; Benetos, A.; Salvi, P. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension 2010, 56, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Skrzypczyk, P.; Przychodzień, J.; Mizerska-Wasiak, M.; Kuźma-Mroczkowska, E.; Okarska-Napierała, M.; Górska, E.; Stelmaszczyk-Emmel, A.; Demkow, U.; Pańczyk-Tomaszewska, M. Renalase in Children with Glomerular Kidney Diseases. Adv. Exp. Med. Biol. 2017, 1021, 81–92. [Google Scholar] [CrossRef]
- Couffinhal, T.; Dufourcq, P.; Duplàa, C. Beta-catenin nuclear activation: Common pathway between Wnt and growth factor signaling in vascular smooth muscle cell proliferation? Circ. Res. 2006, 99, 1287–1289. [Google Scholar] [CrossRef] [Green Version]
- Quasnichka, H.; Slater, S.C.; Beeching, C.A.; Boehm, M.; Sala-Newby, G.B.; George, S.J. Regulation of smooth muscle cell proliferation by beta-catenin/T-cell factor signaling involves modulation of cyclin D1 and p21 expression. Circ. Res. 2006, 99, 1329–1337. [Google Scholar] [CrossRef] [Green Version]
- Arderiu, G.; Espinosa, S.; Peña, E.; Aledo, R.; Badimon, L. Monocyte-secreted Wnt5a interacts with FZD5 in microvascular endothelial cells and induces angiogenesis through tissue factor signaling. J. Mol. Cell Biol. 2014, 6, 380–393. [Google Scholar] [CrossRef] [Green Version]
- Ueland, T.; Otterdal, K.; Lekva, T.; Halvorsen, B.; Gabrielsen, A.; Sandberg, W.J.; Paulsson-Berne, G.; Pedersen, T.M.; Folkersen, L.; Gullestad, L.; et al. Dickkopf-1 enhances inflammatory interaction between platelets and endothelial cells and shows increased expression in atherosclerosis. Arter. Thromb. Vasc. Biol. 2009, 29, 1228–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, B.G.; Liou, H.H.; Lee, C.J.; Chen, Y.C.; Ho, G.J.; Lee, M.C. Serum Sclerostin as an Independent Marker of Peripheral Arterial Stiffness in Renal Transplantation Recipients: A Cross-Sectional Study. Medicine (Baltim.) 2016, 95, e3300. [Google Scholar] [CrossRef] [PubMed]
- Litwin, M.; Niemirska, A. Intima-media thickness measurements in children with cardiovascular risk factors. Pediatr. Nephrol. 2009, 24, 707–719. [Google Scholar] [CrossRef] [PubMed]
- Stavrinou, E.; Sarafidis, P.A.; Koumaras, C.; Loutradis, C.; Giamalis, P.; Tziomalos, K.; Karagiannis, A.; Papagianni, A. Increased Sclerostin, but Not Dickkopf-1 Protein, Is Associated with Elevated Pulse Wave Velocity in Hemodialysis Subjects. Kidney Blood Press Res. 2019, 44, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; Solak, Y.; Siriopol, D.; Aslan, G.; Afsar, B.; Yazici, D.; Covic, A. Sclerostin, cardiovascular disease and mortality: A systematic review and meta-analysis. Int. Urol. Nephrol. 2016, 48, 2029–2042. [Google Scholar] [CrossRef] [PubMed]
- Bovijn, J.; Krebs, K.; Chen, C.Y.; Boxall, R.; Censin, J.C.; Ferreira, T.; Pulit, S.L.; Glastonbury, C.A.; Laber, S.; Millwood, I.Y.; et al. Evaluating the cardiovascular safety of sclerostin inhibition using evidence from meta-analysis of clinical trials and human genetics. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef]
- Vestergaard Kvist, A.; Faruque, J.; Vallejo-Yagüe, E.; Weiler, S.; Winter, E.M.; Burden, A.M. Cardiovascular Safety Profile of Romosozumab: A Pharmacovigilance Analysis of the US Food and Drug Administration Adverse Event Reporting System (FAERS). J. Clin. Med. 2021, 10, 1660. [Google Scholar] [CrossRef]
- Krishna, S.M.; Seto, S.W.; Jose, R.J.; Li, J.; Morton, S.K.; Biros, E.; Wang, Y.; Nsengiyumva, V.; Lindeman, J.H.; Loots, G.G.; et al. Wnt Signaling Pathway Inhibitor Sclerostin Inhibits Angiotensin II-Induced Aortic Aneurysm and Atherosclerosis. Arter. Thromb. Vasc. Biol. 2017, 37, 553–566. [Google Scholar] [CrossRef] [Green Version]
- Mayer, O., Jr.; Seidlerová, J.; Kučera, R.; Kučerová, A.; Černá, V.; Gelžinský, J.; Mateřánková, M.; Mareš, Š.; Kordíková, V.; Pešta, M.; et al. Synergistic effect of sclerostin and angiotensin II receptor 1 polymorphism on arterial stiffening. Biomark Med. 2020, 14, 173–184. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Children with Primary Hypertension | Healthy Children | p |
|---|---|---|---|
| Number of patients (n) | 60 | 20 | - |
| Age (years) | 15.0 ± 2.9 (13.9–17.1) | 14.4 ± 2.5 (12.6–16.8) | 0.405 |
| Gender (boys/girls) | 37/23 (61.7%/38.3%) | 9/11 (45%/55%) | 0.205 |
| Height (cm) | 168.0 ± 16.2 (162–178) | 164.9 ± 12.0 (158–174) | 0.162 |
| Height Z-score | 0.50 ± 1.09 (−0.10–1.22) | 0.54 ± 1.51 (−0.13–1.35) | 0.689 |
| Weight (kg) | 71.4 ± 21.8 (60.5–82.7) | 57.5 ± 15.4 (47.2–66.5) | 0.010 |
| Weight Z-score | 1.20 ± 1.06 (0.39–1.95) | 0.49 ± 1.14 (−0.27–1.53) | 0.012 |
| BMI (kg/m2) | 24.7 ± 5.2 (20.92–28.36) | 20.8 ± 3.8 (18.1–23.3) | 0.003 |
| BMI Z-score | 1.15 ± 1.11 (0.39–2.13) | 0.32 ± 0.91 (−0.49–1.13) | 0.002 |
| Antihypertensive medications (n) | 25 (41.7%) | - | - |
| Calcium channel antagonists | 19 | ||
| Angiotensin convertase inhibitors | 8 | ||
| Beta-adrenolytics | 3 | ||
| Diuretics | 2 | ||
| Alfa-adrenolytics | 2 | ||
| eGFR ac. to Schwartz (mL/min/1.73 m2) | 101.9 ± 21.4 (88.8–113.1) | 108.4 ± 20.8 (94.2–124.4) | 0.192 |
| Uric acid (mg/dL) | 5.5 ± 1.4 (4.8–6.1) | 4.5 ± 1.1 (3.8–5.5) | 0.003 |
| Total cholesterol (mg/dL) | 159.9 ± 36.9 (136–171) | 152.8 ± 29.5 (133–176) | 0.509 |
| HDL-cholesterol (mg/dL) | 51.7 ± 14.4 (43–58) | 57.7 ± 12.3 (49–64) | 0.041 |
| LDL-cholesterol (mg/dL) | 88.6 ± 33.9 (66–98) | 81.3 ± 25 (64–104) | 0.505 |
| Triglyceride (mg/dL) | 98.4 ± 48.8 (63–121) | 69.2 ± 26.3 (50–82) | 0.010 |
| Parameter | Children with Primary Hypertension | Healthy Children | p |
|---|---|---|---|
| Office oscillometric blood pressure | |||
| SBP (mm Hg) | 130.5 ± 11.6 (121–138) | 119.0 ± 9.8 (109–126) | <0.001 |
| SBP Z-score | 1.43 ± 0.95 (0.93–2.12) | 0.52 ± 0.79 (−0.17–1.13) | <0.001 |
| DBP (mm Hg) | 77.3 ± 10.8 (71–82) | 67.7 ± 7.3 (65–74) | <0.001 |
| DBP Z-score | 1.65 ± 1.49 (0.88–2.28) | 0.30 ± 0.91 (−0.14–1.06) | <0.001 |
| Central blood pressure | |||
| AoSBP (mm Hg) | 109.6 ± 9.6 (102–117) | 98.1 ± 8.1 (91–105) | <0.001 |
| AoDBP (mm Hg) | 79.2 ± 10.9 (72–84) | 69.0 ± 7.2 (66–74) | <0.001 |
| 24 h ambulatory blood pressure | |||
| SBP 24 h (mm Hg) | 129.3 ± 9.6 (121–136) | 114.8 ± 4.9 (112–117) | <0.001 |
| DBP 24 h (mm Hg) | 70.8 ± 7.7 (66–76) | 64.4 ± 5.2 (62–68) | <0.001 |
| MAP 24 h (mm Hg) | 90.3 ± 7.7 (85–96) | 81.1 ± 4.7 (78–85) | <0.001 |
| SBPL 24 h (%) | 44.0 ± 26.7 (27–63) | 10.2 ± 6.8 (6–14) | <0.001 |
| DBPL 24 h (%) | 23.9 ± 21.0 (8–36) | 7.3 ± 5.8 (2–11) | <0.001 |
| SBP DIP (%) | 10.3 ± 5.2 (8–13) | 11.4 ± 3.4 (10–13) | 0.383 |
| DBP DIP (%) | 15.3 ± 7.6 (11–20) | 16.1 ± 3.7 (14–18) | 0.642 |
| Parameters of arterial damage | |||
| cIMT (mm) | 0.46 ± 0.07 (0.41–0.51) | 0.41 ± 0.06 (0.31–0.42) | 0.003 |
| cIMT Z-score | 1.47 ± 1.47 (0.45–2.41) | 0.45 ± 1.08 (−0.29–0.68) | 0.003 |
| aPWV (m/s) | 5.3 ± 1.0 (4.7–5.9) | 4.6 ± 0.6 (4.2–5.0) | 0.004 |
| aPWV Z-score | −0.05 ± 1.17 (−0.95–0.71) | −0.88 ± 0.79 (−1.53–−0.33) | 0.004 |
| AIx75HR (%) | −2.1 ± 13.0 (−10.0–4.8) | −3.4 ± 13.0 (−9.2–3.3) | 0.756 |
| SEVR (%) | 163.2 ± 41.2 (133–195) | 155.6 ± 27.3 (137–169) | 0.440 |
| E-tracking beta | 3.9 ± 3.3 (2.5–4.2) | 3.7 ± 1.0 (3.1–4.5) | 0.315 |
| E-tracking Ep (kPa) | 52.1 ± 42.3 (33–57) | 44.9 ± 13.0 (34–55) | 0.991 |
| E-tracking AC (mm2/kPa) | 1.3 ± 0.5 (0.9–1.6) | 1.0 ± 0.2 (0.8–1.1) | 0.016 |
| E-tracking AIx (%) | −5.5 ± 17.2 (−11.9–−0.7) | −2.7 ± 6.1 (−4.5–0.4) | 0.168 |
| E-tracking PWVbeta (m/s) | 4.1 ± 1.3 (3.4–4.4) | 3.9 ± 0.6 (3.5–4.5) | 0.934 |
| E-tracking D_max (mm) | 6.4 ± 0.7 (6.0–6.8) | 5.7 ± 0.7 (5.1–6.3) | <0.001 |
| E-tracking D_min (mm) | 5.5 ± 0.7 (4.9–5.9) | 4.9 ± 0.7 (4.3–5.4) | 0.003 |
| E-tracking DAT_max (ms) | 128.5 ± 39.9 (105–140) | 146.0 ± 41.8 (125–152) | 0.026 |
| Parameter | Primary Hypertension | Healthy Children | p |
|---|---|---|---|
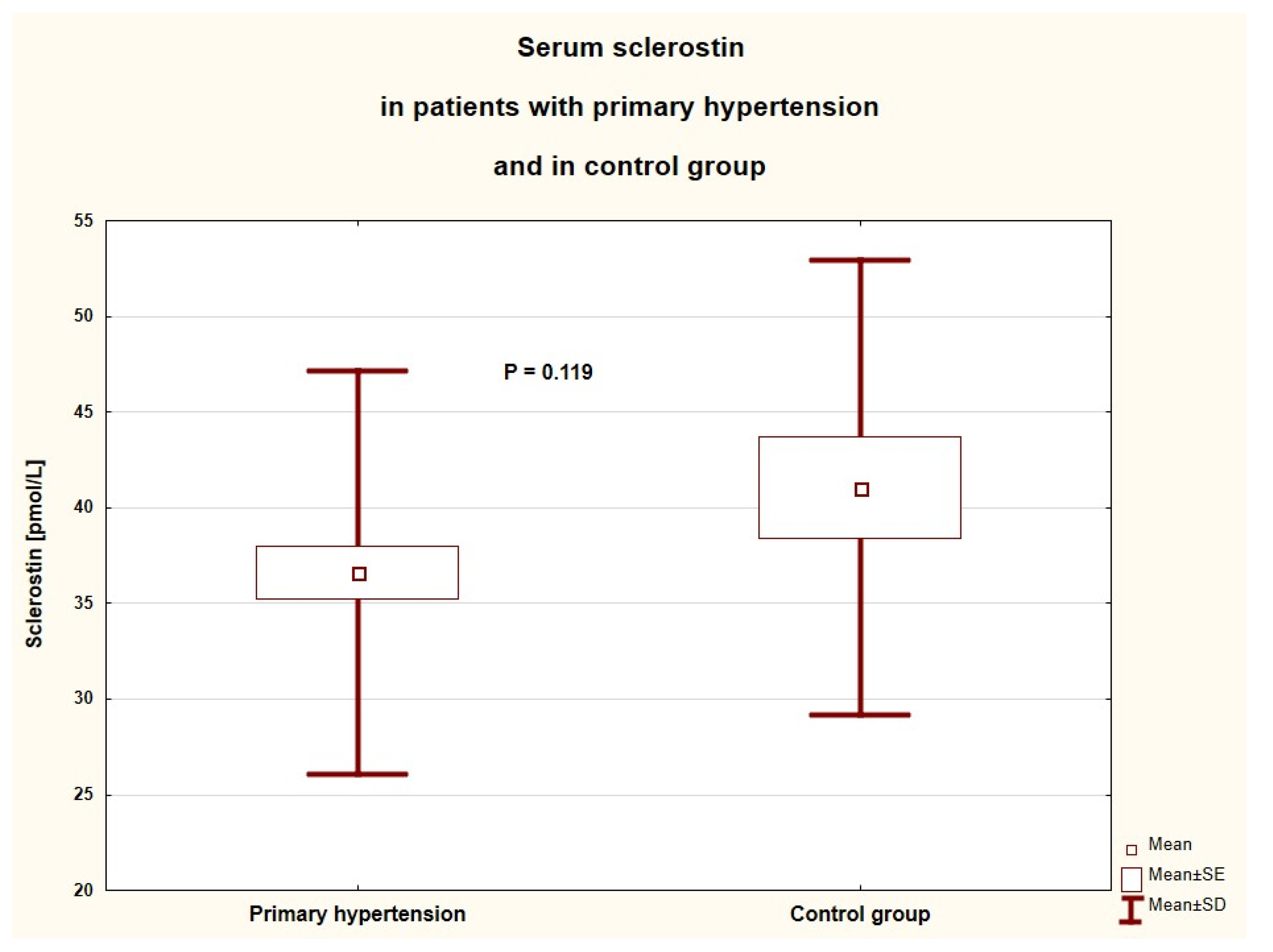
| Sclerostin (pmol/L) | 36.6 ± 10.6 (27.3–42.7) | 41.0 ± 11.9 (31.9–50.3) | 0.119 |
| Calcium (mg/dL) | 10.0 ± 0.3 (9.8–10.2) | 9.8 ± 0.3 (9.6–9.9) | 0.005 |
| Phosphate (mg/dL) | 4.4 ± 0.7 (3.9–4.9) | 4.4 ± 0.5 (4.0–4.7) | 0.922 |
| 25OHD (ng/mL) | 20.5 ± 7.8 (15.8–23.4) | 20.3 ± 7.8 (15.8–22.3) | 0.859 |
| Severe vitamin D deficiency | 3 (5.0%) | 0 (0.0%) | 0.580 |
| Vitamin D deficiency | 30 (50.0%) | 12 (60.0%) | |
| Suboptimal vitamin D level | 20 (33.3%) | 7 (35.0%) | |
| Optimal vitamin D level | 7 (11.7%) | 1 (5.0%) | |
| Parathyroid hormone (pg/mL) | 27.5 ± 12.7 (17–35) | 22.9 ± 11.4 (13–31) | 0.153 |
| Alkaline phosphate (IU/L) | 125.2 ± 67.8 (74–153) | 154.3 ± 80.6 (91–213) | 0.153 |
| Analyzed Parameter | r | p |
|---|---|---|
| age (years) | −0.329 | 0.003 |
| height Z-score | 0.320 | 0.004 |
| SBP (mm Hg) | −0.251 | 0.025 |
| SBP Z-score | −0.240 | 0.032 |
| MAP (mm Hg) | −0.226 | 0.044 |
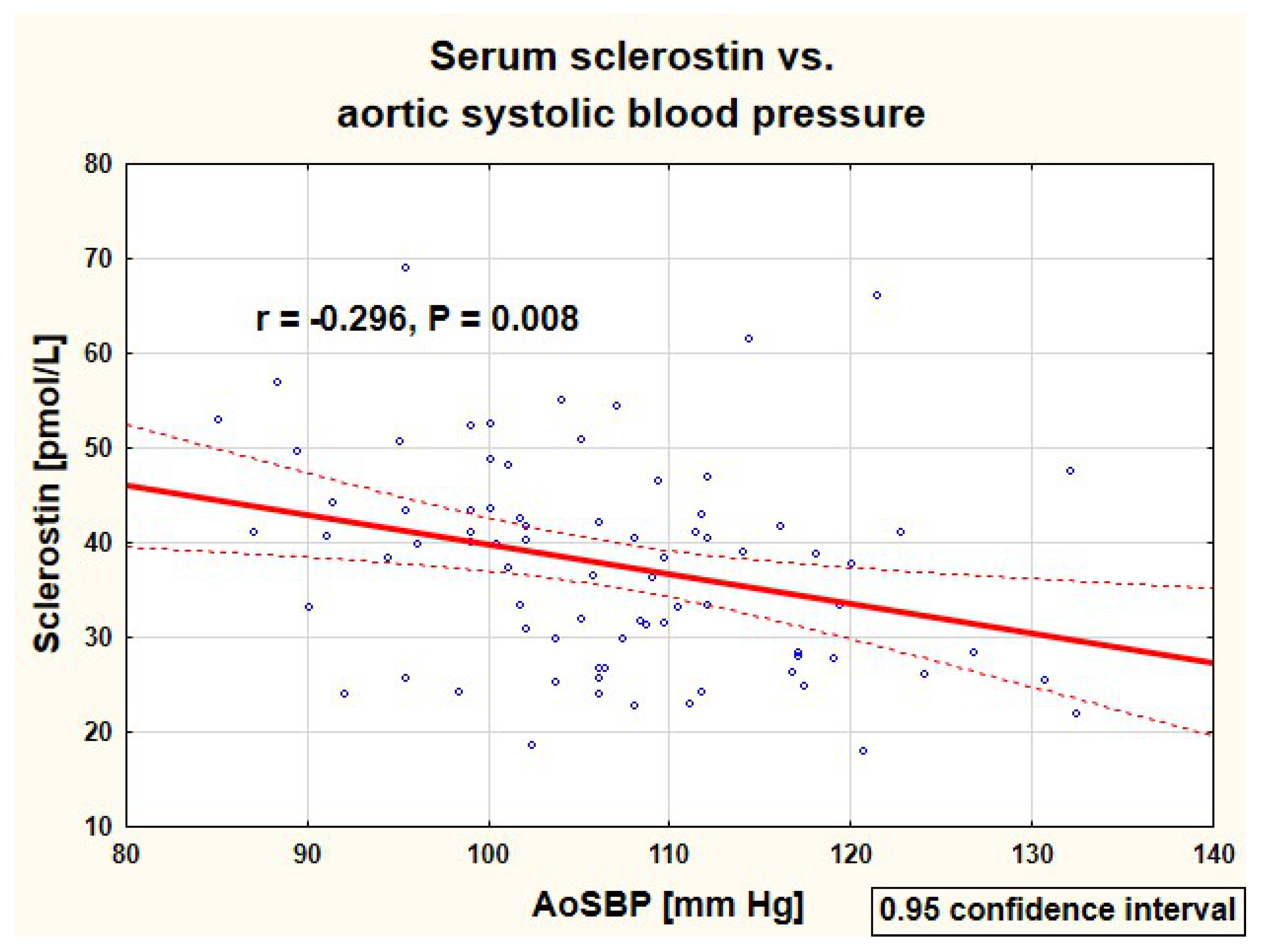
| AoSBP (mm Hg) | −0.296 | 0.008 |
| AoMAP (mm Hg) | −0.253 | 0.024 |
| phosphate (mg/dL) | 0.323 | 0.003 |
| alkaline phosphatase (IU/L) | 0.462 | <0.001 |
| Parameter | Beta | 95% Confidence Interval | p |
|---|---|---|---|
| Height Z-score | 0.224 | (0.017–0.430) | 0.034 |
| SBP Z-score | −0.216 | (−0.417–−0.016) | 0.035 |
| Phosphate (mg/dL) | 0.219 | (−0.002–0.441) | 0.053 |
| Age (years) | −0.170 | (−0.396–0.055) | 0.137 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skrzypczyk, P.; Ofiara, A.; Szyszka, M.; Stelmaszczyk-Emmel, A.; Górska, E.; Pańczyk-Tomaszewska, M. Serum Sclerostin Is Associated with Peripheral and Central Systolic Blood Pressure in Pediatric Patients with Primary Hypertension. J. Clin. Med. 2021, 10, 3574. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163574
Skrzypczyk P, Ofiara A, Szyszka M, Stelmaszczyk-Emmel A, Górska E, Pańczyk-Tomaszewska M. Serum Sclerostin Is Associated with Peripheral and Central Systolic Blood Pressure in Pediatric Patients with Primary Hypertension. Journal of Clinical Medicine. 2021; 10(16):3574. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163574
Chicago/Turabian StyleSkrzypczyk, Piotr, Anna Ofiara, Michał Szyszka, Anna Stelmaszczyk-Emmel, Elżbieta Górska, and Małgorzata Pańczyk-Tomaszewska. 2021. "Serum Sclerostin Is Associated with Peripheral and Central Systolic Blood Pressure in Pediatric Patients with Primary Hypertension" Journal of Clinical Medicine 10, no. 16: 3574. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163574