
Effect of Early Peripheral Parenteral Nutrition Support in an Enhanced Recovery Program for Colorectal Cancer Surgery: A Randomized Open Trial

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
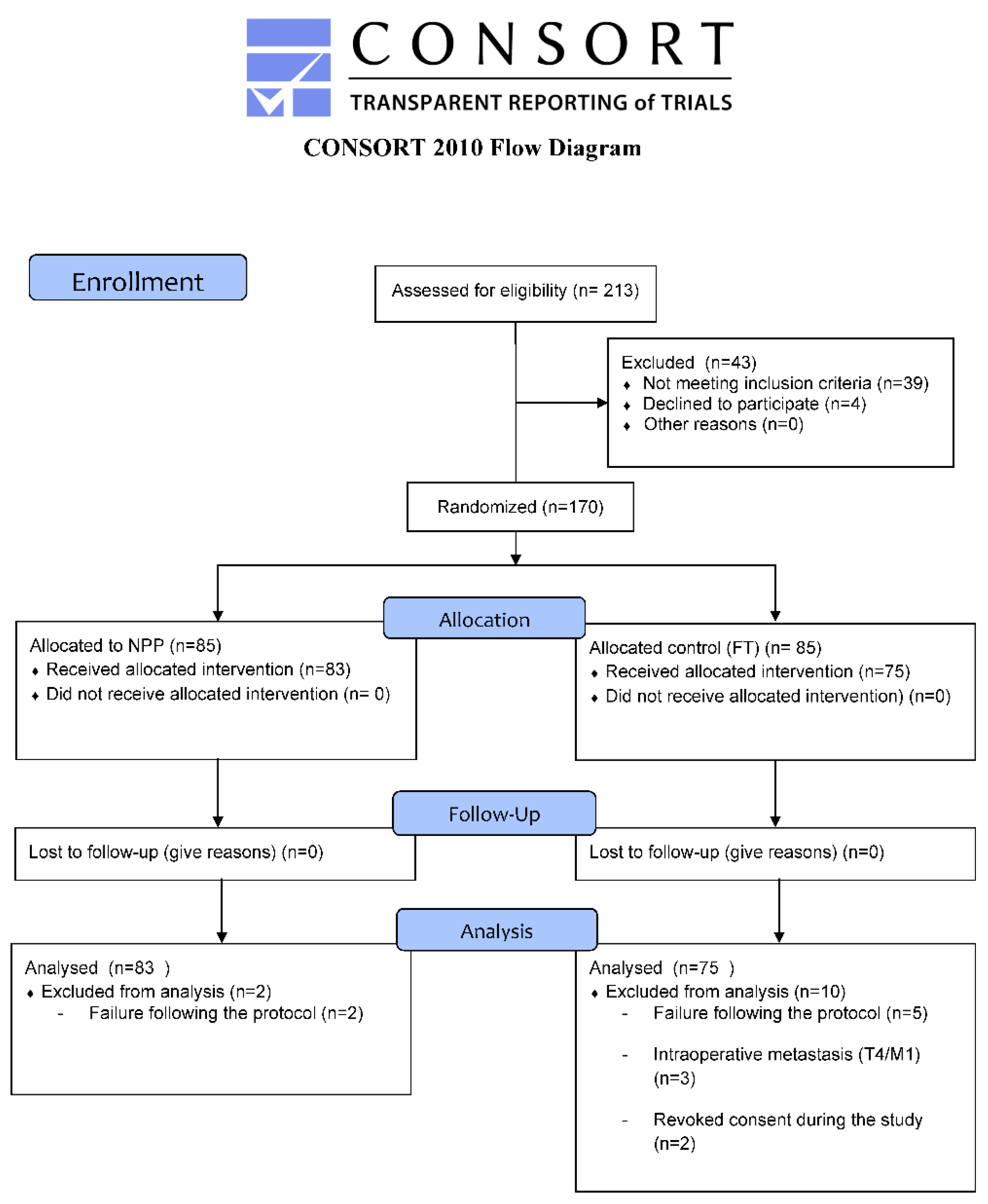
2.2. Randomization and Masking
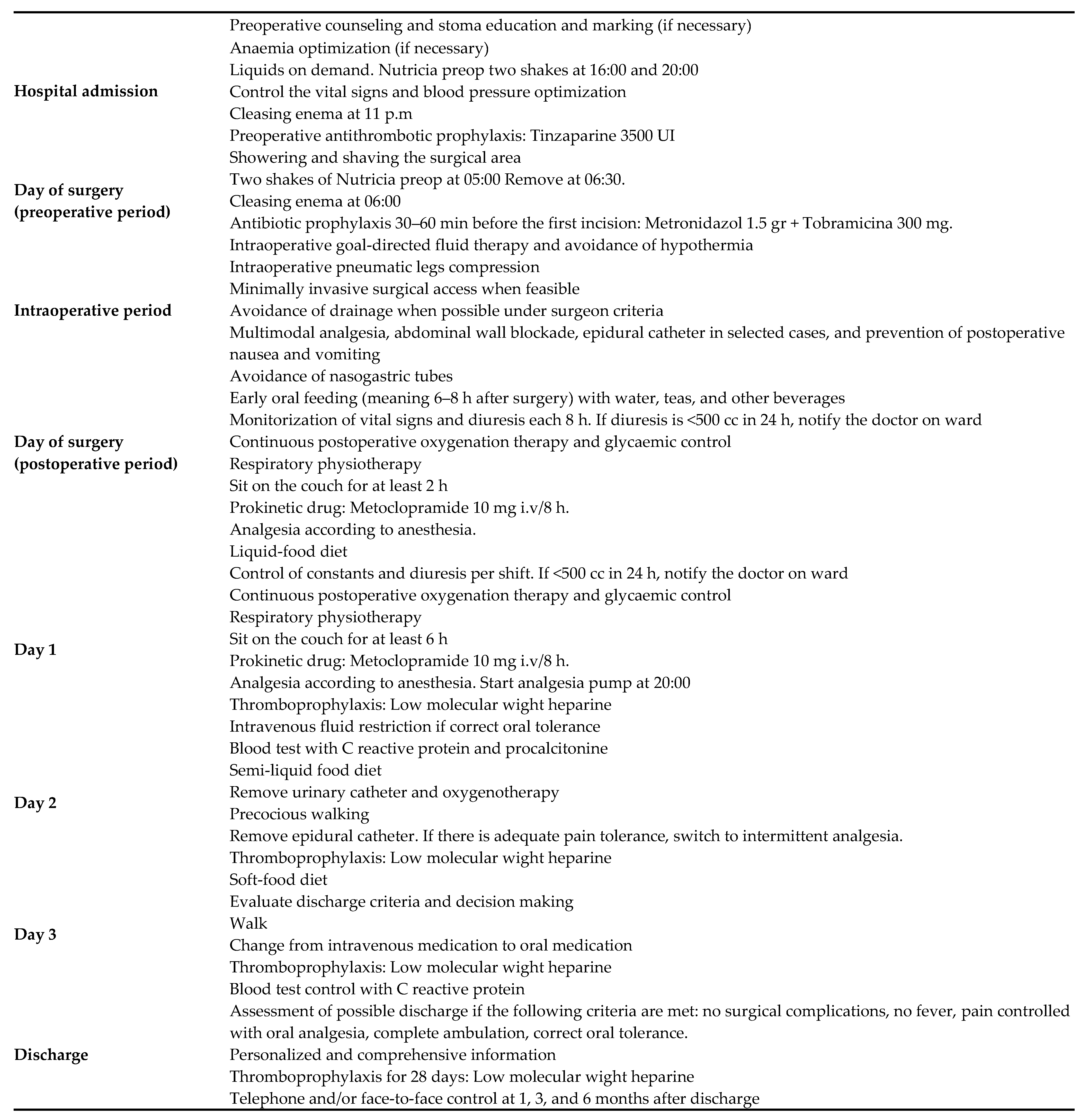
2.3. Procedures
2.3.1. Outcome Measures
2.3.2. Statistical Analysis
3. Results
3.1. Pre- and Perioperative Clinical and Laboratory Features
3.2. Postoperative Changes in Laboratory Parameters
3.3. Postoperative Complications and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Guillén, L.; Frasson, M.; Pellino, G.; Fornés-Ferrer, V.; Ramos, J.L.; Flor-Lorente, B.; García-Granero, Á.; Sierra, I.B.; Jiménez-Gómez, L.M.; Moya-Martínez, A.; et al. Nomograms for morbidity and mortality after oncologic colon resection in the enhanced recovery era: Results from a multicentric prospective national study. Int. J. Color. Dis. 2020, 35, 2227–2238. [Google Scholar] [CrossRef]
- Damle, R.N.; Alavi, K. Risk factors for 30-d readmission after colorectal surgery: A systematic review. J. Surg. Res. 2015, 200, 200–207. [Google Scholar] [CrossRef]
- Van der Kroft, G.; Bours, M.; Janssen-Heijnen, M.; van Berlo, C.; Konsten, J. Value of sarcopenia assessed by computed tomography for the prediction of postoperative morbidity following oncological colorectal resection: A comparison with the malnutrition screening tool. Clin. Nutr. ESPEN 2018, 24, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Kuppinger, D.; Hartl, W.H.; Bertok, M.; Hoffmann, J.M.; Cederbaum, J.; Küchenhoff, H.; Jauch, K.; Rittler, P. Nutritional screening for risk prediction in patients scheduled for abdominal operations. BJS 2012, 99, 728–737. [Google Scholar] [CrossRef]
- Herbert, G.; Perry, R.; Andersen, H.K.; Atkinson, C.; Penfold, C.; Lewis, S.J.; Ness, A.; Thomas, S. Early enteral nutrition within 24 hours of lower gastrointestinal surgery versus later commencement for length of hospital stay and postoperative complications. Cochrane Database Syst. Rev. 2019, 2019, CD004080. [Google Scholar] [CrossRef] [Green Version]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Willcutts, K.F.; Chung, M.C.; Erenberg, C.L.; Finn, K.L.; Schirmer, B.D.; Byham-Gray, L.D. Early Oral Feeding as Compared With Traditional Timing of Oral Feeding After Upper Gastrointestinal Surgery. Ann. Surg. 2016, 264, 54–63. [Google Scholar] [CrossRef]
- Bliss, L.A.; Maguire, L.H.; Chau, Z.; Yang, C.J.; Nagle, D.A.; Chan, A.T.; Tseng, J.F. Readmission after resections of the colon and rectum: Predictors of a costly and common outcome. Dis. Colon. Rectum. 2015, 58, 1164–1173. [Google Scholar] [CrossRef]
- Williams, D.G.A.; Ohnuma, T.; Krishnamoorthy, V.; Raghunathan, K.; Sulo, S.; Cassady, B.A.; Hegazi, R.; Wischmeyer, P.E. Impact of early postoperative oral nutritional supplement utilization on clinical outcomes in colorectal surgery. Perioper. Med. 2020, 9, 29. [Google Scholar] [CrossRef]
- Ooi, S.-E.; Chen, G.-W.; Chou, C.-T. Adequate nourishment through total parenteral nutrition treatment may augment immune function in patients with colon cancer. Arch. Med Res. 2004, 35, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Celaya Pérez, S.; Navarro, M.; Román, A.; Salinas, J.C.; Larrad, L.; Lasierra, M.P.; Lozano Mantecón, R. Efecto de la nutrición parenteral preoperatoria en la capacidad de respuesta inmune en pacientes desnutridos. (Nutrición parenteral preoperatoria e inmunidad) [The effect of preoperative parenteral nutrition on the capacity of the immune response in malnourished patients (preoperative parenteral nutrition and immunity)]. Nutr. Hosp. 1989, 4, 145–148. (In Spanish) [Google Scholar]
- Iresjö, B.-M.; Engström, C.; Lundholm, K. Preoperative overnight parenteral nutrition (TPN) improves skeletal muscle protein metabolism indicated by microarray algorithm analyses in a randomized trial. Physiol. Rep. 2016, 4, e12789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iresjö, B.; Engström, C.; Smedh, U.; Lundholm, K. Overnight Steady-State Infusions of Parenteral Nutrition on Myosin Heavy Chain Transcripts in Rectus Abdominis Muscle Related to Amino Acid Transporters, Insulin-like Growth Factor 1, and Blood Amino Acids in Patients Aimed at Major Surgery. J. Parenter. Enter. Nutr. 2019, 43, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.; Ljungqvist, O.; Soeters, P.; Fearon, K.; Weimann, A.; Bozzetti, F. ESPEN Guidelines on Parenteral Nutrition: Surgery. Clin. Nutr. 2009, 28, 378–386. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Therneau, T.; Atkinson, B. rpart: Recursive Partitioning and Regression Trees. R Package Version 4.1-15. Available online: https://cran.r-project.org/package=rpart (accessed on 12 February 2021).
- Dolan, R.D.; Almasaudi, A.S.; Dieu, L.B.; Horgan, P.G.; McSorley, S.T.; McMillan, D.C. The relationship between computed tomography-derived body composition, systemic inflammatory response, and survival in patients undergoing surgery for colorectal cancer. J. Cachex Sarcopenia Muscle 2019, 10, 111–122. [Google Scholar] [CrossRef]
- Ziętarska, M.; Krawczyk-Lipiec, J.; Kraj, L.; Zaucha, R.; Małgorzewicz, S. Nutritional status assessment in colorectal cancer patients qualified to systemic treatment. Współczesna Onkol. 2017, 2, 157–161. [Google Scholar] [CrossRef]
- Lakananurak, N.; Gramlich, L. The Role of Preoperative Parenteral Nutrition. Nutrients 2020, 12, 1320. [Google Scholar] [CrossRef]
- Zhou, J.; Hiki, N.; Mine, S.; Kumagai, K.; Ida, S.; Jiang, X.; Nunobe, S.; Ohashi, M.; Sano, T.; Yamaguchi, T. Role of Prealbumin as a Powerful and Simple Index for Predicting Postoperative Complications After Gastric Cancer Surgery. Ann. Surg. Oncol. 2016, 24, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Haskins, I.N.; Baginsky, M.; Amdur, R.L.; Agarwal, S. Preoperative hypoalbuminemia is associated with worse outcomes in colon cancer patients. Clin. Nutr. 2017, 36, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Junqueira, J.C.D.S.; Soares, E.C.; Filho, H.R.C.; Hoehr, N.F.; Magro, D.O.; Ueno, M. Nutritional risk factors for postoperative complications in Brazilian elderly patients undergoing major elective surgery. Nutrients 2003, 19, 321–326. [Google Scholar] [CrossRef]
- Critselis, E.; Panagiotakos, D.B.; Machairas, A.; Zampelas, A.; Critselis, A.N.; Polychronopoulos, E. Risk and predictive factors of hypoalbuminemia in cancer patients following extensive abdominal surgery despite total parenteral nutritional support. Int. J. Food Sci. Nutr. 2011, 63, 208–215. [Google Scholar] [CrossRef]
- Critselis, E.; Panagiotakos, D.B.; Machairas, A.; Zampelas, A.; Critselis, A.N.; Polychronopoulos, E. Postoperative Hypoproteinemia in Cancer Patients Following Extensive Abdominal Surgery Despite Parenteral Nutritional Support. Nutr. Cancer 2011, 63, 1021–1028. [Google Scholar] [CrossRef]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Pozzo, C.; Strippoli, A.; Bria, E.; Tortora, G.; Gasbarrini, A.; Mele, M.C. Effects of nutritional interventions on nutritional status in patients with gastric cancer: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. ESPEN 2020, 38, 28–42. [Google Scholar] [CrossRef]
- Lucia, P.E.O.; Liliana, V.V.M. Protocolo para el manejo de nutrición parenteral periférica lista para usar en paciente quirúrgico. Nutr. Hosp. 2015, 31, 1003–1011. [Google Scholar] [CrossRef]
- Cai, W.; Calder, P.C.; Cury-Boaventura, M.F.; De Waele, E.; Jakubowski, J.; Zaloga, G. Biological and Clinical Aspects of an Olive Oil-Based Lipid Emulsion—A Review. Nutrients 2018, 10, 776. [Google Scholar] [CrossRef] [Green Version]
- Dąbrowska, A.M.; Słotwiński, R. The immune response to surgery and infection. Cent. Eur. J. Immunol. 2014, 39, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.E.; Hilkewich, L.; Gillis, C.; Heine, J.A.; Fenton, T.R. Protein intakes are associated with reduced length of stay: A comparison between Enhanced Recovery After Surgery (ERAS) and conventional care after elective colorectal surgery. Am. J. Clin. Nutr. 2017, 106, 44–51. [Google Scholar] [CrossRef]
- IHI. What Is a Bundle? Disponibleen. Available online: http://www.ihi.org/resources/Pages/ImprovementStories/WhatIsaBundle.aspx (accessed on 30 March 2021).
- Dean, H.; King, E.; Gane, D.; Hocking, D.; Rogers, J.; Pullyblank, A. Introduction of a care bundle effectively and sustainably reduces patient-reported surgical site infection in patients undergoing colorectal surgery. J. Hosp. Infect. 2020, 105, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Tejedor, P.; Ayora, S.G.; López, M.O.; Arellano, M.L.; Guadalajara, H.; García-Olmo, D.; Pastor, C. Implementation barriers for Enhanced Recovery After Surgery (ERAS) in rectal cancer surgery: A comparative analysis of compliance with colon cancer surgeries. Updates Surg. 2021, 1–8. [Google Scholar] [CrossRef]
- Burden, S.; Billson, H.A.; Lal, S.; Owen, K.A.; Muneer, A. Perioperative nutrition for the treatment of bladder cancer by radical cystectomy. Cochrane Database Syst. Rev. 2019, 5, CD010127. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| FT (N = 75) (%) | PPN (N = 83) (%) | TOTAL (N = 158) | p-Value | ||
|---|---|---|---|---|---|
| Age (mean SD) | 67.8 (11.6) | 71.4 (11.0) | 69.7(11.4) | 0.049 | |
| Sex | Male | 46 (47.4) | 51 (52.6%) | 97 (61.4) | 1.000 |
| Female | 29 (47.5) | 32 (52.5%) | 61 (38.6) | ||
| ASA score | 1 | 10 (71.4) | 4 (28.6%) | 14 (8.9) | 0.139 |
| 2 | 38 (47.5) | 42 (52.5%) | 80 (50.6) | ||
| 3 | 27 (42.2) | 37 (57.8) | 64 (40.5) | ||
| Surgical approach | Open | 9 (52.9) | 8 (47.1) | 17 (10.8) | 0.845 |
| Laparoscopic | 66 (46.8) | 75 (53.2) | 141 (89.2) | ||
| Type of procedure | Abdominoperineal excision | 13 (72.3) | 5 (27.7) | 18 (11.4) | 0.551 |
| Left hemicolectomy | 4 (40) | 6 (60%) | 10 (6.3) | ||
| Subtotal colectomy | 2 (50) | 2 (50%) | 4 (2.5) | ||
| Total colectomy | 0 (0) | 1 (100) | 1 (0.6) | ||
| Hartmann | 1 (50) | 1 (50) | 2 (1.3) | ||
| Right hemicolectomy | 25 (46.3) | 29 (53.7) | 54 (34.2) | ||
| ULAR | 2 (50) | 2 (50) | 4 (2.5) | ||
| Anterior resection | 19 (43.18) | 25 (56.82) | 44 (27.8) | ||
| Sigmoidectomy | 9 (42.85) | 12 (57.15) | 21 (13.3) | ||
| Stoma | 0 | 53 (44.9) | 66 (55.1) | 119 (75.4) | 0.402 |
| 1 | 22 (56.5) | 17 (43.5) | 39 (24.6) | ||
| Type of stoma | Colostomy | 16 (64) | 9 (36) | 25 (15.8) | 0.307 |
| Ileostomy | 5 (35.7) | 9 (64.3) | 14 (8.9) | ||
| Baseline disease | Left colon cancer | 6 (42.8) | 8 (57.2) | 14 (8.9) | 0.651 |
| Right colon cancer | 19 (41) | 27 (59) | 46 (29.1) | ||
| Transverse colon cancer | 4 (66.7) | 2 (33.3) | 6 (3.8) | ||
| Rectal cancer | 35 (52.2) | 32 (47.8) | 67 (42.4) | ||
| Sigmoid colon cancer | 11 (44) | 14 (56) | 25 (15.8) | ||
| Anastomosis configuration | Side to side | 25 (48.1) | 27 (51.9) | 52 (32.9) | 0.280 |
| End to side | 0 (0) | 3 (100) | 3 (1.9) | ||
| End to end | 36 (43.4) | 47 (53.6) | 83 (52.5) | ||
| No anastomosis | 14 (70) | 6 (30) | 20 (12.7) |
| Day | FT (N = 75) | PPN (N = 83) | p-Value | |
|---|---|---|---|---|
| GLUCOSE, mean (SD) | Before surgery | 106.798 (28.075) | 108.406 (25.622) | 0.706 |
| First day after surgery | 118.422 (21.159) | 136.079 (36.321) | <0.001 | |
| Third day after surgery | 96.641 (18.586) | 116.073 (30.522) | <0.001 | |
| UREA, mean (SD) | Before surgery | 41.199 (17.823) | 44.319 (15.473) | 0.239 |
| First day after surgery | 31.678 (13.25) | 38.243 (15.492) | 0.005 | |
| Third day after surgery | 34.105 (18.152) | 37.944 (20.903) | 0.220 | |
| CREATININE, mean (SD) | Before surgery | 0.836 (0.272) | 0.846 (0.255) | 0.795 |
| First day after surgery | 0.74 (0.256) | 0.777 (0.296) | 0.404 | |
| Third day after surgery | 0.796 (0.336) | 0.774 (0.424) | 0.729 | |
| TOTAL PROTEINS, mean (SD) | Before surgery | 7.108 (0.603) | 6.944 (0.648) | 0.102 |
| First day after surgery | 5.644 (0.589) | 5.522 (0.609) | 0.203 | |
| Third day after surgery | 5.598 (0.694) | 5.528 (0.63) | 0.508 | |
| ALBUMINE, mean (SD) | Before surgery | 4.058 (0.404) | 3.956 (0.484) | 0.153 |
| First day after surgery | 3.145 (0.394) | 3.053 (0.433) | 0.168 | |
| Third day after surgery | 3.039 (0.493) | 2.996 (0.441) | 0.554 | |
| PREALBUMIN, mean (SD) | Before surgery | 22.128 (5.728) | 21.236 (5.052) | 0.298 |
| First day after surgery | 16.535 (3.669) | 16.807 (3.965) | 0.655 | |
| Third day after surgery | 13.998 (3.919) | 14.472 (3.606) | 0.429 | |
| HEMOGLOBIN, mean (SD) | Before surgery | 12.748 (1.639) | 12.82 (1.949) | 0.802 |
| First day after surgery | 11.221 (1.759) | 11.414 (1.819) | 0.497 | |
| Third day after surgery | 11.168 (1.859) | 11.203 (1.647) | 0.900 | |
| TRANSFERRINE, mean (SD) | Before surgery | 257.348 (54.15) | 271.33 (65.302) | 0.146 |
| First day after surgery | 201.16 (42.743) | 214.134 (46.386) | 0.069 | |
| Third day after surgery | 185.008 (43.717) | 192.315 (49.159) | 0.325 | |
| ZINC, mean (SD) | Before surgery | 63.94 (16.692) | 64.774 (14.079) | 0.733 |
| First day after surgery | 43.074 (10.037) | 35.422 (14.203) | <0.001 | |
| Third day after surgery | 59.705 (15.865) | 48.058 (16.313) | <0.001 | |
| WBC, mean (SD) | Before surgery | 6.039 (2.322) | 6.189 (2.125) | 0.673 |
| First day after surgery | 9.22 (2.94) | 10.964 (3.692) | 0.001 | |
| Third day after surgery | 7.152 (2.893) | 7.498 (2.567) | 0.426 | |
| % NEUTROPHILS, mean (SD) | Before surgery | 64.514 (8.692) | 63.887 (9.46) | 0.665 |
| First day after surgery | 80.241 (5.627) | 81.135 (6.161) | 0.342 | |
| Third day after surgery | 74.029 (9.402) | 72.927 (8.522) | 0.439 | |
| LYMPHOCYTES, mean (SD) | Before surgery | 22.91 (7.928) | 23.366 (8.923) | 0.734 |
| First day after surgery | 11.634 (4.513) | 10.876 (5.381) | 0.340 | |
| Third day after surgery | 14.857 (7.235) | 15.487 (7.135) | 0.581 | |
| PLATELETS, mean (SD) | Before surgery | 230.802 (117.353) | 230.108 (72.006) | 0.964 |
| First day after surgery | 215.17 (102.572) | 212.811 (66.995) | 0.863 | |
| Third day after surgery | 213.432 (97.272) | 203.345 (73.989) | 0.461 | |
| FIBRINOGEN, mean (SD) | Before surgery | 412.79 (120.087) | 379.33 (115.917) | 0.076 |
| First day after surgery | 445.295 (119.332) | 440.461 (114.263) | 0.794 | |
| Third day after surgery | 642.406 (181.08) | 654.873 (203.599) | 0.685 | |
| RCP, mean (SD) | Before surgery | 14.71 (29.005) | 11.017 (22.532) | 0.369 |
| First day after surgery | 60.982 (37.77) | 63.545 (45.955) | 0.703 | |
| Third day after surgery | 114.501 (95.885) | 95.086 (67.622) | 0.140 | |
| PROCALCITONINE, mean (SD) | Before surgery | 0.634 (3.664) | 0.164 (0.129) | 0.245 |
| First day after surgery | 0.545 (1.054) | 0.963 (1.687) | 0.066 | |
| Third day after surgery | 1.631 (3.636) | 1.751 (7.424) | 0.899 |
| FT N = 75 (%) | PPN N = 83 (%) | p-Value | |
|---|---|---|---|
| Postoperative complications | 33 (0.44) | 28 (33.7) | 0.186 |
| Major complications (C–D III–V) | 14 (18.7) | 10 (12) | 0.001 |
| Minor complications (C–D I–II) | 19 (25.3) | 18 (21.7) | 0.001 |
| Anastomotic leak | 15 (20) | 13(15.6) | 0.062 |
| Major leak | 12 (16) | 6 (7.2) | 0.001 |
| Minor leak | 3 (4) | 7 (8.4) | 0.001 |
| Postoperative ileus | 12 (16) | 13 (15.7) | 0.954 |
| Surgical site infections (SSI) | 11 (14.6) | 9 (10.8) | 0.47 |
| Other complications | 7 (9.3) | 5 (6) | 0.433 |
| Length of hospital stay (LOS) | 7 (5–9) | 6 (5–8) | 0.19 |
| Variables | Patients without Complications N = 97 (61.39) (%) | Patients with Any Complications N = 61 (38.61) (%) | p-Value 1 | Odds Ratio 2 | 95 % CI 2 | p-Value 2 | |
|---|---|---|---|---|---|---|---|
| Age | <65 | 36 (37.1) | 19 (31.1) | 0.7133 | 1 | 0.4262 | |
| 65–75 | 25 (25.8) | 16 (26.2) | 0.43 | (0.1, 1.64) | |||
| >75 | 36 (37.1) | 26 (42.6) | 0.77 | (0.19, 3.07) | |||
| Gender | Male | 62 (63.9) | 35 (57.4) | 0.5129 | 1 | 0.4441 | |
| Female | 35 (36.1) | 26 (42.6) | 1.49 | (0.53, 4.16) | |||
| ASA score | I-ii | 58 (59.8) | 36 (59) | 0.6188 | 1 | 0.736 | |
| Iii | 39 (40.2) | 25 (41) | 0.82 | (0.25, 2.58) | |||
| PPN | No | 42 (43.3) | 33 (54.1) | 0.2461 | 1 | 0.0031 | |
| Yes | 55 (56.7) | 28 (45.9) | 0.2 | (0.06, 0.59) | |||
| Surgical approach | Open | 7 (7.2) | 10 (16.4) | 0.1215 | 1 | 0.7451 | |
| Laparoscopy | 90 (92.8) | 51 (83.6) | 0.76 | (0.15, 3.9) | |||
| Stoma | No | 79 (81.5) | 40 (65.6) | 0.016 | 1.47 | (0.57, 5.26) | 0.5412 |
| Yes | 18 (18.5) | 21 (34.4) | 1 | ||||
| 1st day movilization | No | 16 (16.5) | 25 (41) | <0.001 | 1.39 | (0.3, 7.37) | 0.678 |
| Yes | 81 (83.5) | 36 (59) | 1 | ||||
| 1st day tolerance | No | 7 (7.2) | 20 (32.8) | <0.001 | 1 | 0.0950 | |
| Yes | 90 (92.8) | 41 (67.2) | 0.24 | (0.04, 1.28) | |||
| 2nd day diet | Clear liquid/ Full liquid diet | 72 (74.2) | 42 (68.9) | 0.5813 | 1.7 | (0.57, 5.1) | |
| Pureed food/ soft food diet | 25 (25.8) | 19 (31.1) | 1 | 0.34044 | |||
| 3rd day diet | Clear liquid/ full liquid diet | 24 (24.7) | 25 (41) | 0.0486 | 1 | 0.8575 | |
| Pureed food/ soft food diet | 73 (75.3) | 36 (59) | 0.9 | (0.3, 2.83) | |||
| Variables | OR (95% CI) | |
|---|---|---|
| Age | <65 | |
| 65–75 | 0.51 (0.13–1.8) | |
| >75 | 1.15 (0.32–4.11) | |
| Gender | Male | 1 |
| Female | 1.92 (0.75–4.92 | |
| ASA score | I-II | 1 |
| III | 0.63 (0.20–1.86) | |
| PPN | No | 1 |
| YES | 0.27 (0.09–0.72) | |
| Surgical approach | Open | 1 |
| Laparoscopy | 0.66 (0.17–2.57) | |
| 1st day mobilization | No | 1 |
| Yes | 1.14 (0.29–4.82) | |
| 1st day tolerance | No | 1 |
| Yes | 0.22 (0.05–0.98) | |
| 3rd day diet | Clear liquid/ Full liquid diet | 1 |
| Pureed food/ Soft food diet | 1.17 (0.43–3.38) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Guillén, L.; Soriano-Irigaray, L.; López-Rodríguez-Arias, F.; Barber, X.; Murcia, A.; Alcaide, M.J.; Aranaz-Ostáriz, V.; Soler-Silva, Á.; Navarro-Ruiz, A.; Arroyo, A. Effect of Early Peripheral Parenteral Nutrition Support in an Enhanced Recovery Program for Colorectal Cancer Surgery: A Randomized Open Trial. J. Clin. Med. 2021, 10, 3647. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163647
Sánchez-Guillén L, Soriano-Irigaray L, López-Rodríguez-Arias F, Barber X, Murcia A, Alcaide MJ, Aranaz-Ostáriz V, Soler-Silva Á, Navarro-Ruiz A, Arroyo A. Effect of Early Peripheral Parenteral Nutrition Support in an Enhanced Recovery Program for Colorectal Cancer Surgery: A Randomized Open Trial. Journal of Clinical Medicine. 2021; 10(16):3647. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163647
Chicago/Turabian StyleSánchez-Guillén, Luis, Leticia Soriano-Irigaray, Francisco López-Rodríguez-Arias, Xavier Barber, Ana Murcia, M José Alcaide, Verónica Aranaz-Ostáriz, Álvaro Soler-Silva, Andrés Navarro-Ruiz, and Antonio Arroyo. 2021. "Effect of Early Peripheral Parenteral Nutrition Support in an Enhanced Recovery Program for Colorectal Cancer Surgery: A Randomized Open Trial" Journal of Clinical Medicine 10, no. 16: 3647. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163647