
SARS-CoV-2 in Urine May Predict a Severe Evolution of COVID-19

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
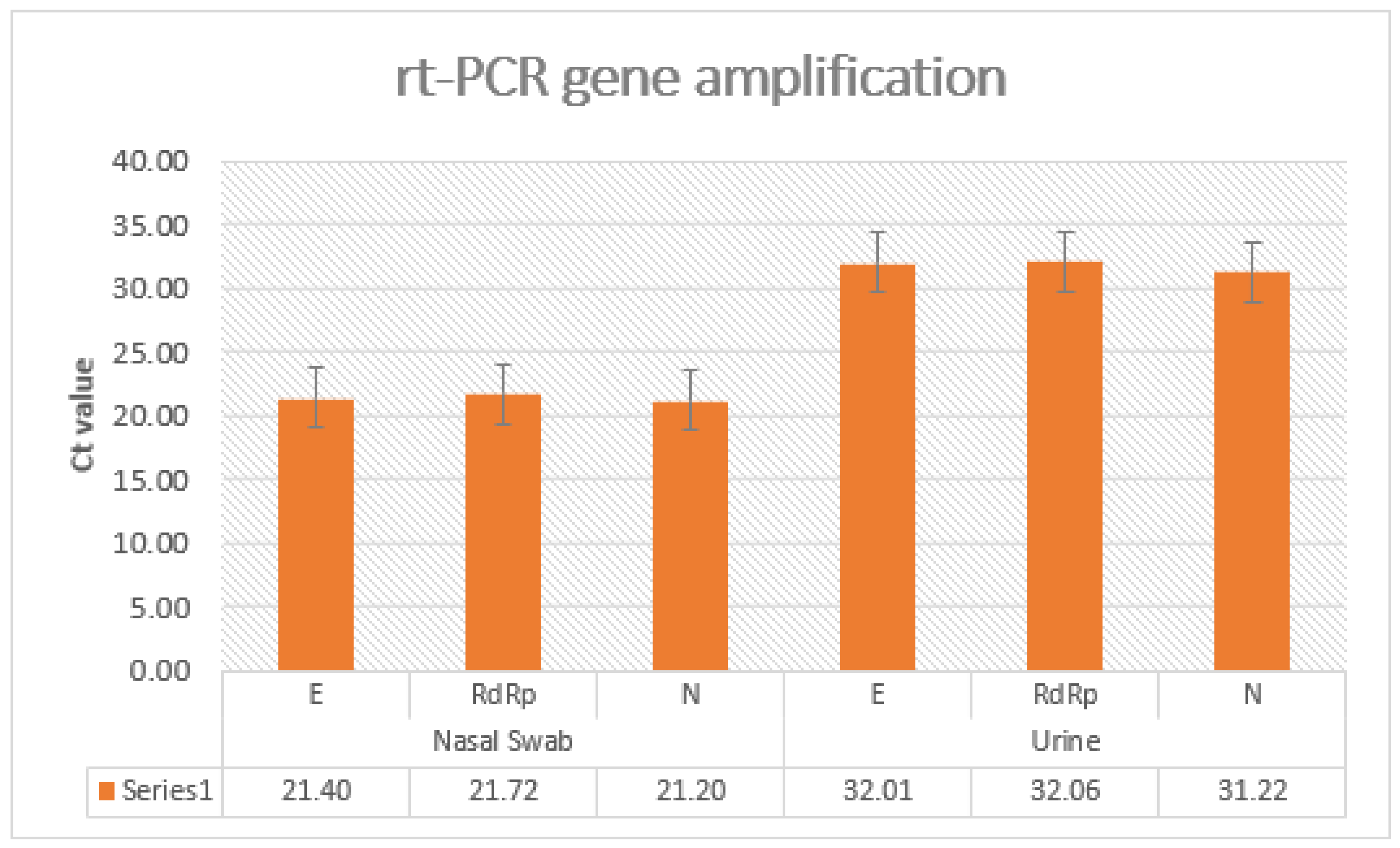
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perrella, A.; Carannante, N.; Berretta, M.; Rinaldi, M.; Maturo, N.; Rinaldi, L. Novel Coronavirus 2019 (SARS-CoV2): A global emer-gency that needs new approaches? Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2162–2164. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Scully, E.P.; Gupta, A.; Klein, S.L. Sex-biased clinical presentation and outcomes from COVID-19. Clin. Microbiol. Infect. 2021, 27, 1072–1073. [Google Scholar] [CrossRef] [PubMed]
- Yassin, A.; Nawaiseh, M.; Shaban, A.; Alsherbini, K.; El-Salem, K.; Soudah, O.; Abu-Rub, M. Neurological manifestations and com-plications of coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. BMC Neurol. 2021, 21, 138. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Wang, S.F. SARS-CoV-2 entry related viral and host genetic variations: Implications on COVID-19 severity, immune escape, and infectivity. Int. J. Mol. Sci. 2021, 22, 3060. [Google Scholar] [CrossRef] [PubMed]
- Shirato, K.; Nao, N.; Katano, H.; Takayama, I.; Saito, S.; Kato, F.; Katoh, H.; Sakata, M.; Nakatsu, Y.; Mori, Y.; et al. Development of henetic diagnostic methods for novel corona virus 2019(nCoV-2019) in Japan. Jpn. J. Infect. Dis. 2020, 73, 304e7. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.-W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. Laboratory diagnosis of COVID-19: Current issues and challenges. J. Clin. Microbiol. 2020, 58, e00512–e00520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quiroga, S.A.; Hernández, C.; Castañeda, S.; Jimenez, P.; Vega, L.; Gomez, M.; Martinez, D.; Ballesteros, N.; Muñoz, M.; Cifuentes, C.; et al. Contrasting SARS-CoV-2 RNA copies and clinical symptoms in a large cohort of Colombian patients during the first wave of the COVID-19 pandemic. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 39. [Google Scholar] [CrossRef]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January–March 2020: A retrospective cohort study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.N.; Manissero, D.; Steele, V.R.; Pareja, J. A narrative systematic review of the clinical utility of cycle threshold values in the context of COVID-19. Infect. Dis. 2020, 9, 573–586. [Google Scholar] [CrossRef]
- Hossain, M.E.; Lister, D.; Bartolo, C.; Kinsella, P.M.; Knox, J.; Aldrich, R.; Cowan, R.; Commons, R.J. Prolonged viral shedding in patients with mild to moderate COVID-19 disease: A regional perspective. Infect. Dis. Res. Treat. 2021, 14, 11786337211010428. [Google Scholar] [CrossRef]
- Váncsa, S.; Dembrovszky, F.; Farkas, N.; Szakó, L.; Teutsch, B.; Bunduc, S.; Nagy, R.; Párniczky, A.; Erőss, B.; Péterfi, Z.; et al. Repeated SARS-CoV-2 positivity: Analysis of 123 cases. Viruses 2021, 13, 512. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef]
- The World Medical Association. Declaration of Helsinki [Web Page]. 2004. Available online: http://www.wma.net/e/policy/b3.htm (accessed on 28 December 2020).
- Lascarrou, J.-B.; Gaultier, A.; Soumagne, T.; Serck, N.; Sauneuf, B.; Piagnerelli, M.; Ly, A.; Lejeune, F.; Lefebvre, L.; Hraiech, S.; et al. Identifying clinical phenotypes in moderate to severe acute respiratory distress syndrome related to COVID-19: The COVADIS study. Front. Med. 2021, 8, 632933. [Google Scholar] [CrossRef]
- Castro, R.A.; Frishman, W.H. Thrombotic complications of COVID-19 infection: A review. Cardiol Rev. 2021, 29, 43–47. [Google Scholar] [CrossRef]
- Stringer, D.; Braude, P.; Myint, P.K.; Evans, L.; Collins, J.T.; Verduri, A.; Quinn, T.J.; Vilches-Moraga, A.; Stechman, M.J.; Pearce, L.; et al. COPE Study Collaborators. The role of C-reactive protein as a prognostic marker in COVID-19. Int. J. Epidemiol. 2021, 50, 420–429. [Google Scholar] [CrossRef]
- Wu, J.; Liu, J.; Li, S.; Peng, Z.; Xiao, Z.; Wang, X.; Yan, R.; Luo, J. Detection and analysis of nucleic acid in various biological samples of COVID-19 patients. Travel Med. Infect. Dis. 2020, 37, 101673. [Google Scholar] [CrossRef]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal changes of CT findings in 90 patients with COVID-19 pneumonia: A longitudinal study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Casals, M.; Brito-Zerón, P.; Mariette, X. Systemic and organ-specific immune-related manifestations of COVID-19. Nat. Rev. Rheumatol. 2021, 17, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; van der Poll, T. Coagulation and sepsis. Thromb. Res. 2017, 149, 38–44. [Google Scholar] [CrossRef]
- Frithiof, R.; Bergqvist, A.; Järhult, J.D.; Lipcsey, M.; Hultström, M. Presence of SARS-CoV-2 in urine is rare and not associated with acute kidney injury in critically ill COVID-19 patients. Crit. Care 2020, 24, 587. [Google Scholar] [CrossRef] [PubMed]
- Phanthanawiboon, S.; Limkittikul, K.; Sakai, Y.; Takakura, N.; Saijo, M.; Kurosu, T. Acute systemic infection with dengue virus leads to vascular leakage and death through tumor necrosis factor-α and Tie2/Angiopoietin signaling in mice lacking type I and II interferon receptors. PLoS ONE 2016, 11, e0148564. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Scoring System | |||
|---|---|---|---|
| Score 1 | Score 2 | Score 3 | |
| Lymphocytes (>1000 cell/mmc) | 601–1000 | 401–600 | <400 |
| CRP (<5 mg) | >10 x n.v. | >20 x n.v. | <25 x n.v. |
| P/F ratio | ≥250 | 250–150 | <150 |
| CT Scan Score * | <10/25 | 11–18/25 | >18/25 |
| Fever for more than 3 days | <38 °C | 38–39 °C | >39 °C |
| Dyspnea | mild | moderate | severe |
| Variables | Total | Urine Negative (Acute Infection) | Urine Positive (Acute Infection) |
|---|---|---|---|
| (n = 60) | (n = 53) | (n = 7) | |
| Demographic data | |||
| Age (years) Sex | 68 ± 5 | 65 ± 6 | 67 ± 3 |
| Male | 16 (84%) | 9 (75%) | 7 (100%) |
| Female | 3 (16%) | 3 (25%) | 0 (0%) |
| Smoking history | |||
| Yes | 13 (68%) | 7 (58%) | 6 (86%) |
| No | 6 (32%) | 5 (42%) | 1 (14%) |
| Comorbidities | |||
| Hypertension | 12 | 4 | 2 |
| Diabetes | 6 | 3 | 1 |
| Cardiovascular disease | 8 | 4 | 3 |
| Chronic liver disease | 2 | 0 | 0 |
| Chronic lung disease | 4 | 2 | 0 |
| Chronic kidney | 3 | 0 | 0 |
| disease Cancer | 5 | 2 | 1 |
| Immunocompromising conditions | 3 | 1 | 0 |
| Signs and symptoms | |||
| Fever | 12 | 8 | 4 |
| Cough | 9 | 6 | 3 |
| Fatigue | 8 | 3 | 5 |
| Diarrhea | 3 | 2 | 1 |
| Shortness of breath | 13 | 9 | 4 |
| Laboratory findings | 5.753 (±204) | 6.355 (±159) | 4.673 (±109) |
| WBC (cells/mmc) | 1530 (±71) | 996 (±52) | 628 (±64) |
| Lymphocyte (cells/mmc) | 4.0 (5.2) | 4.3 (4.2) | 3.2 (14.2) |
| NLR (Neutropylete/lymphocyte ratio) | 88.1 | 72.1 | 85 |
| CRP (mg/L) | 25 (±15) | 24 (±11) | 35 (±12) |
| AST (U/L < 50) | 267 (±43) | 312 (±15) | 318 (±29) |
| ALT (U/L < 40) | 273 (±159) | 300 (±192) | 234 (±711) |
| LDH (U/L < 250) | 602 (±117) | 425 (±231) | 835 (±194) |
| Fibrinogen (ng/mL) | 2.6 (4.9) | 3.2 (7.6) | 1.8 (3.4) |
| D-dimer (ng/mL) | 257 (12.1) | 28.4 (9.4) | 22.2 (5.4) |
| Creatinine Clearance (MDRD 6 variable) | 62 ± 2 mL/min | 61 ± 2 mL/min | 58 ± 3 mL/min |
| Ct 4 gens mean value of RT-PCR | 20.8 | 18.2 | 21.3 |
| Respiratory Function | 25 (±15) | 24 (±11) | 35 (±12) |
| P/F Ratio | 172 ± 14 | 170 ± 12 | 145 ± 22 |
| NIV (Non-Invasive ventilation) (as %) | 44% | 45% | 43% |
| Venturi Mask (as %) | 32% | 40% | 0% |
| Intubation (as %) | 24% | 15% | 57% |
| CT scan findings | |||
| T Score Wang (x/24) | 19/24 (±1) | 18/254 (±1) | 21/24 (±2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrella, A.; Brita, M.; Coletta, F.; Cotena, S.; De Marco, G.; Longobardi, A.; Sala, C.; Sannino, D.; Tomasello, A.; Perrella, M.; et al. SARS-CoV-2 in Urine May Predict a Severe Evolution of COVID-19. J. Clin. Med. 2021, 10, 4061. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184061
Perrella A, Brita M, Coletta F, Cotena S, De Marco G, Longobardi A, Sala C, Sannino D, Tomasello A, Perrella M, et al. SARS-CoV-2 in Urine May Predict a Severe Evolution of COVID-19. Journal of Clinical Medicine. 2021; 10(18):4061. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184061
Chicago/Turabian StylePerrella, Alessandro, Mario Brita, Francesco Coletta, Simona Cotena, GiamPaola De Marco, Adele Longobardi, Crescenzo Sala, Dania Sannino, Antonio Tomasello, Marco Perrella, and et al. 2021. "SARS-CoV-2 in Urine May Predict a Severe Evolution of COVID-19" Journal of Clinical Medicine 10, no. 18: 4061. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184061