
Elevated Epidermal Growth Factor (EGF) as Candidate Biomarker of Mood Disorders—Longitudinal Study in Adolescent and Young Adult Patients

 , and
, and
Abstract
:1. Introduction
Hypotheses
2. Materials and Methods
2.1. Participants
2.2. BDNF, proBDNF, EGF, MIF, SCF Serum Levels ELISA Determination
2.3. Mature BDNF (mBDNF) and mBDNF/proBDNF Ratio Estimation
2.4. Statistical Analyses
3. Results
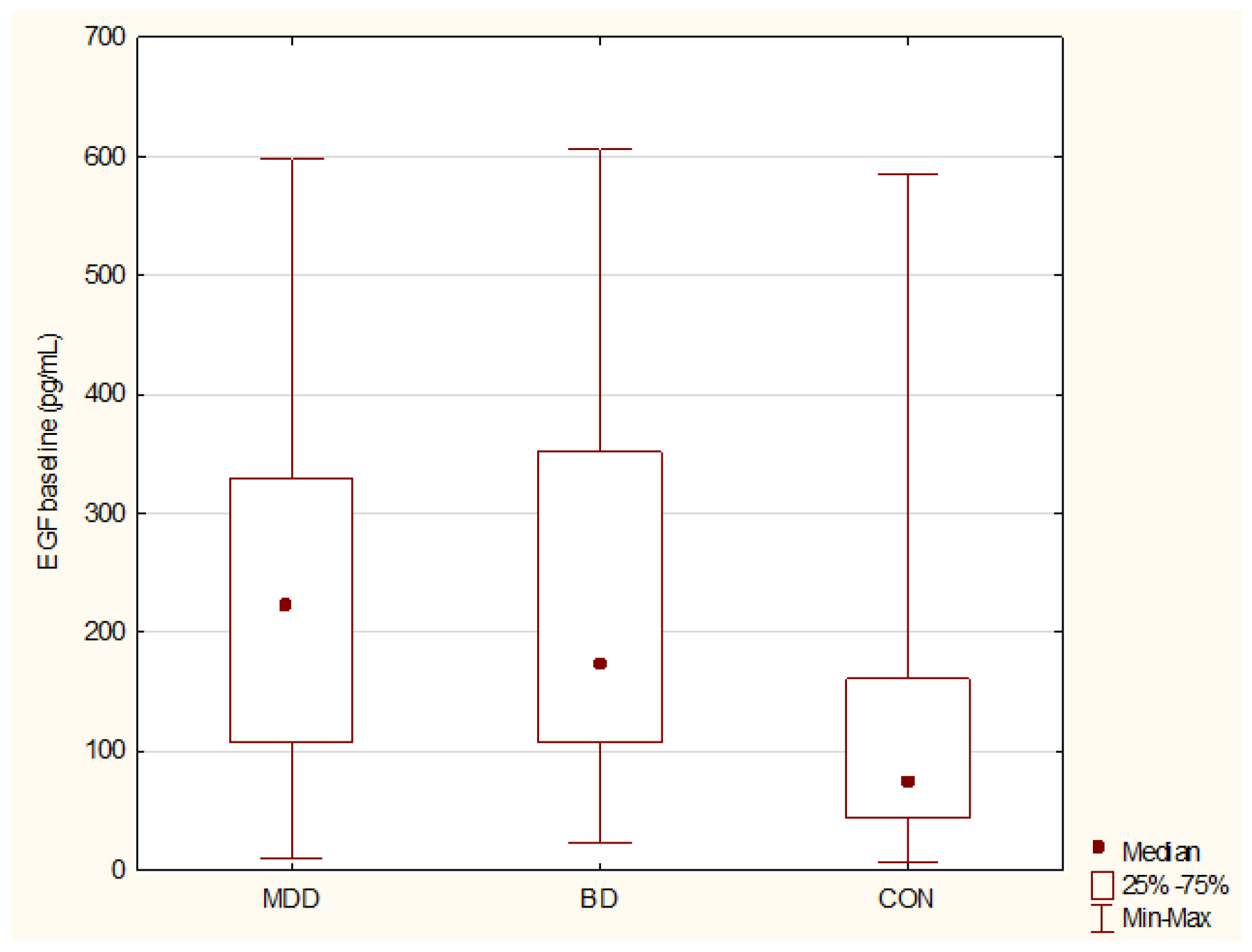
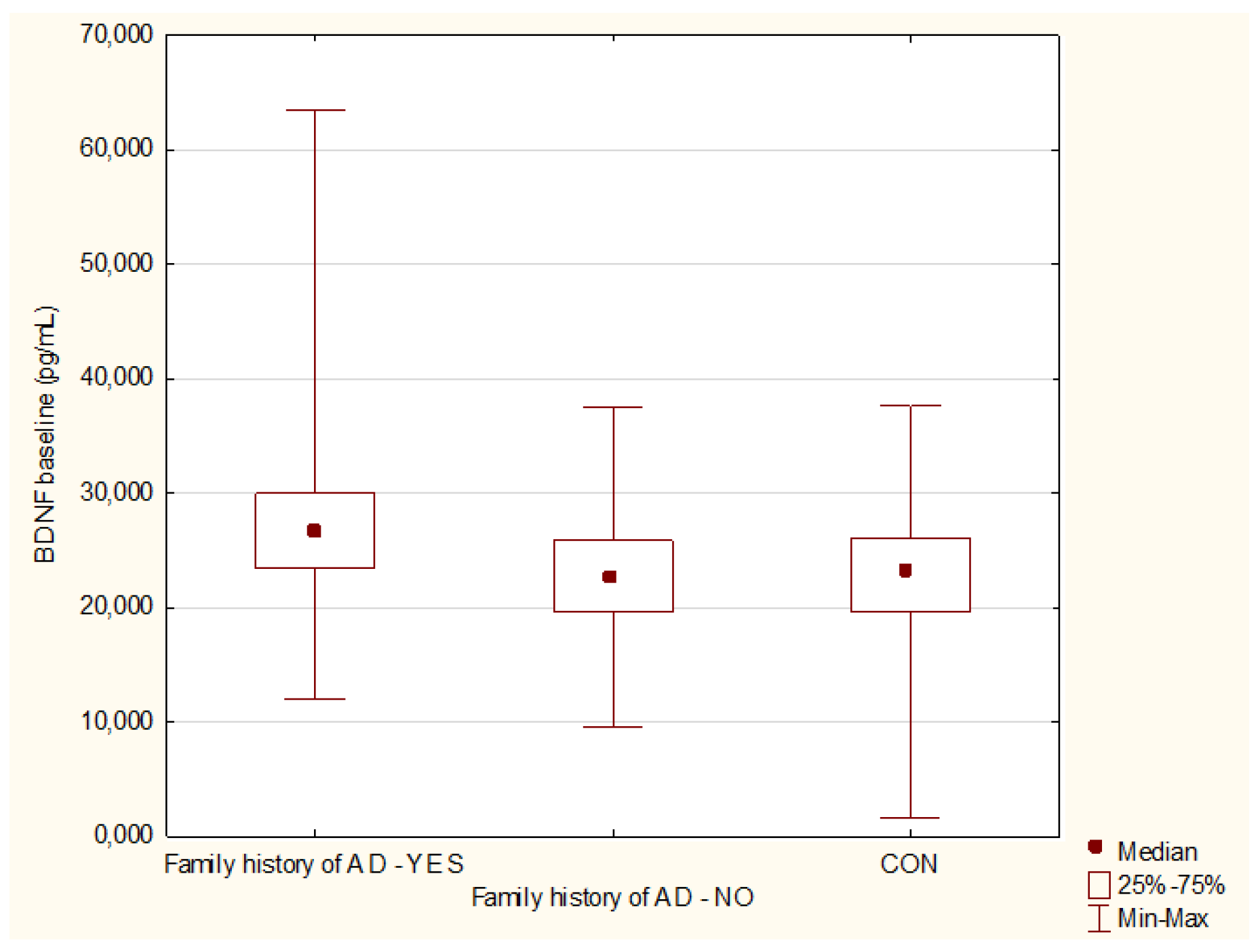
3.1. Baseline Comparisons of BDNF, proBDNF, mBDNF, rBDNF, EGF, SCF, and MIF Levels
3.2. Longitudinal Comparisons of BDNF, proBDNF, mBDNF, rBDNF, EGF, SCF, and MIF Levels
3.3. Comparisons of BDNF, proBDNF, mBDNF, rBDNF, EGF, SCF, and MIF Levels—Euthymic State vs. Controls
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waraich, P.; Goldner, E.M.; Somers, J.M.; Hsu, L. Prevalence and Incidence Studies of Mood Disorders: A Systematic Review of the Literature. Can. J. Psychiatry 2004, 49, 124–138. [Google Scholar] [CrossRef] [Green Version]
- Dudek, D.; Siwek, M.; Zielińska, D.; Jaeschke, R.; Rybakowski, J. Diagnostic conversions from major depressive disorder into bipolar disorder in an outpatient setting: Results of a retrospective chart review. J. Affect. Disord. 2013, 144, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Salagre, E.; Grande, I.; Carvalho, A.F.; Fernandes, B.S.; Berk, M.; Birmaher, B.; Tohen, M.; Suppes, T. Early Intervention in Bipolar Disorder. Am. J. Psychiatry 2018, 175, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Miyahara, S.; Marangell, L.B.; Wisniewski, S.; Ostacher, M.; DelBello, M.P.; Bowden, C.L.; Sachs, G.S.; Nierenberg, A.; STEP-BD Investigators. Long-Term implications of early onset in bipolar disorder: Data from the first 1000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD). Biol. Psychiatry 2004, 55, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Cahill, C.M.; Walter, G.; Malhi, G.S. Neurocognition in Bipolar Disorder and Juvenile Bipolar Disorder. J. Can. Acad. Child. Adolesc. Psychiatry 2009, 18, 221–230. [Google Scholar] [PubMed]
- Reddy, Y.C.J.; Srinath, S. Juvenile bipolar disorder. Acta Psychiatr. Scand. 2000, 102, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Gill, M.K.; Axelson, D.A.; Goldstein, B.I.; Goldstein, T.R.; Yu, H.; Liao, F.; Iyengar, S.; Diler, R.S.; Strober, M.; et al. Longitudinal Trajectories and Associated Baseline Predictors in Youths with Bipolar Spectrum Disorders. Am. J. Psychiatry 2014, 171, 990–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birmaher, B.; Axelson, D.; Goldstein, B.; Strober, M.; Gill, M.M.K.; Hunt, J.; Houck, P.; Ha, W.; Iyengar, S.; Kim, E.; et al. Four-Year Longitudinal Course of Children and Adolescents with Bipolar Spectrum Disorders: The Course and Outcome of Bipolar Youth (COBY) Study. Am. J. Psychiatry 2009, 166, 795–804. [Google Scholar] [CrossRef] [Green Version]
- Van Meter, A.R.; Henry, D.B.; West, A.E. What goes up must come down: The burden of bipolar depression in youth. J. Affect. Disord. 2013, 150, 1048–1054. [Google Scholar] [CrossRef] [Green Version]
- Kloiber, S.; Rosenblat, J.D.; Husain, M.I.; Ortiz, A.; Berk, M.; Quevedo, J.; Vieta, E.; Maes, M.; Birmaher, B.; Soares, J.C.; et al. Neurodevelopmental pathways in bipolar disorder. Neurosci. Biobehav. Rev. 2020, 112, 213–226. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, F.; Aggio, V.; Pratesi, M.L.; Greco, G.; Furlan, R. Neuroinflammation in Bipolar Depression. Front. Psychiatry 2020, 11, 71. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, A.L.; Felsky, D.; Viviano, J.D.; Stojanovski, S.; Ameis, S.H.; Szatmari, P.; Lerch, J.P.; Chakravarty, M.M.; Voineskos, A.N. BDNF-Dependent Effects on Amygdala–Cortical Circuitry and Depression Risk in Children and Youth. Cereb. Cortex 2017, 28, 1760–1770. [Google Scholar] [CrossRef]
- Brambilla, P.; Glahn, D.C.; Balestrieri, M.; Soares, J.C. Magnetic Resonance Findings in Bipolar Disorder. Psychiatr. Clin. N. Am. 2005, 28, 443–467. [Google Scholar] [CrossRef] [PubMed]
- Numakawa, T.; Suzuki, S.; Kumamaru, E.; Adachi, N.; Richards, M.; Kunugi, H. BDNF function and intracellular signaling in neurons. Histol. Histopathol. 2010, 25, 237–258. [Google Scholar] [CrossRef] [PubMed]
- Gibon, J.; Barker, P.A. Neurotrophins and Proneurotrophins: Focus on Synaptic Activity and Plasticity in the Brain. Neurosci. 2017, 23, 587–604. [Google Scholar] [CrossRef] [PubMed]
- Bond, D.; Torres, I.J.; Lam, R.W.; Yatham, L.N. Serum epidermal growth factor, clinical illness course, and limbic brain volumes in early-stage bipolar disorder. J. Affect. Disord. 2020, 270, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Romano, R.; Bucci, C. Role of EGFR in the Nervous System. Cells 2020, 9, 1887. [Google Scholar] [CrossRef] [PubMed]
- Petralia, M.C.; Mazzon, E.; Fagone, P.; Basile, M.S.; Lenzo, V.; Quattropani, M.C.; Bendtzen, K.; Nicoletti, F. Pathogenic contribution of the Macrophage migration inhibitory factor family to major depressive disorder and emerging tailored therapeutic approaches. J. Affect. Disord. 2019, 263, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Günther, S.; Fagone, P.; Jalce, G.; Atanasov, A.G.; Guignabert, C.; Nicoletti, F. Role of MIF and D-DT in immune-inflammatory, autoimmune, and chronic respiratory diseases: From pathogenic factors to therapeutic targets. Drug Discov. Today 2018, 24, 428–439. [Google Scholar] [CrossRef]
- Benedetti, F.; Poletti, S.; Hoogenboezem, T.A.; Locatelli, C.; Ambrée, O.; De Wit, H.; Wijkhuijs, A.J.M.; Mazza, E.; Bulgarelli, C.; Vai, B.; et al. Stem Cell Factor (SCF) is a putative biomarker of antidepressant response. J. Neuroimmune Pharmacol. 2016, 11, 248–258. [Google Scholar] [CrossRef]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial Reliability and Validity Data. J. Am. Acad. Child. Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J. Structured Clinical Interview for DSM IV Axis I Disorders, Clinician Version (SCID-CV); American Psychiatric Press, Inc.: Washington, DC, USA, 1996. [Google Scholar]
- Hamilton, M. A Rating Scale for Depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Domenici, E.; Willé, D.R.; Tozzi, F.; Prokopenko, I.; Miller, S.; McKeown, A.; Brittain, C.; Rujescu, D.; Giegling, I.; Turck, C.W.; et al. Plasma Protein Biomarkers for Depression and Schizophrenia by Multi Analyte Profiling of Case-Control Collections. PLoS ONE 2010, 5, e9166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, W.; Zhang, J.; Zhang, K.; Yang, H.; Sun, Y.; Shen, Y.; Xu, Q. A study of the functional significance of epidermal growth factor in major depressive disorder. Psychiatr. Genet. 2012, 22, 161–167. [Google Scholar] [CrossRef]
- Grosse, L.; Hoogenboezem, T.; Ambrée, O.; Bellingrath, S.; Jörgens, S.; De Wit, H.J.; Wijkhuijs, A.M.; Arolt, V.; Drexhage, H.A. Deficiencies of the T and natural killer cell system in major depressive disorder: T regulatory cell defects are associated with inflammatory monocyte activation. Brain Behav. Immun. 2016, 54, 38–44. [Google Scholar] [CrossRef]
- Yamamori, H.; Ishima, T.; Yasuda, Y.; Fujimoto, M.; Kudo, N.; Ohi, K.; Hashimoto, K.; Takeda, M.; Hashimoto, R. Assessment of a multi-assay biological diagnostic test for mood disorders in a Japanese population. Neurosci. Lett. 2016, 612, 167–171. [Google Scholar] [CrossRef]
- Snijders, G.; Mesman, E.; de Wit, H.; Wijkhuijs, A.; Nolen, W.; Drexhage, H.; Hillegers, M. Immune dysregulation in offspring of a bipolar parent. Altered serum levels of immune growth factors at adolescent age. Brain Behav. Immun. 2017, 64, 116–123. [Google Scholar] [CrossRef]
- Wu, H.E.; Teixeira, A.L.; Barroso, L.; Silva, A.P.M.; de Souza Nicolau, M.; Ferreira, J.D.R.; Bertola, L.; Vieira, E.M.; Diniz, B.S. Epidermal growth factor and fibroblast growth factor-2 circulating levels in elderly with major depressive disorder. Psychiatry Res. 2018, 272, 141–143. [Google Scholar] [CrossRef]
- Woo, H.I.; Lim, S.-W.; Myung, W.; Kim, D.K.; Lee, S.-Y. Differentially expressed genes related to major depressive disorder and antidepressant response: Genome-wide gene expression analysis. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Weissleder, C.; Webster, M.J.; Barry, G.; Weickert, C.S. Reduced Insulin-Like Growth Factor Family Member Expression Predicts Neurogenesis Marker Expression in the Subependymal Zone in Schizophrenia and Bipolar Disorder. Schizophr. Bull. 2020, 47, 1168–1178. [Google Scholar] [CrossRef]
- Knorr, U.; Søndergaard, M.H.G.; Koefoed, P.; Jørgensen, A.; Faurholt-Jepsen, M.; Vinberg, M.; Kessing, L. Increased blood BDNF in healthy individuals with a family history of depression. Psychiatry Res. 2017, 256, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Duffy, A.; Horrocks, J.; Doucette, S.; Keown-Stoneman, C.; Grof, P.; Andreazza, A.; Young, L.T. Immunological and neurotrophic markers of risk status and illness development in high-risk youth: Understanding the neurobiological underpinnings of bipolar disorder. Int. J. Bipolar Disord. 2014, 2, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binici, N.C.; Emiroglu, F.N.I.; Resmi, H.; Ellidokuz, H. Serum Brain-derived Neurotrophic Factor Levels among Euthymic Adolescents with Bipolar Disorder Type I. Noro Psikiyatr. Ars. 2016, 53, 267–271. [Google Scholar] [CrossRef]
- Inal-Emiroglu, F.N.; Karabay, N.; Resmi, H.; Güleryüz, H.; Baykara, B.; Alşen, S.; Senturk-Pilan, B.; Akay, A.; Kose, S. Correlations between amygdala volumes and serum levels of BDNF and NGF as a neurobiological markerin adolescents with bipolar disorder. J. Affect. Disord. 2015, 182, 50–56. [Google Scholar] [CrossRef]
- Hatch, J.K.; Scola, G.; Olowoyeye, O.; Collins, J.E.; Andreazza, A.C.; Moody, A.; Levitt, A.J.; Strauss, B.H.; Lanctot, K.L.; Goldstein, B.I. Inflammatory Markers and Brain-Derived Neurotrophic Factor as Potential Bridges Linking Bipolar Disorder and Cardiovascular Risk Among Adolescents. J. Clin. Psychiatry 2017, 78, e286–e293. [Google Scholar] [CrossRef]
- Tsuchimine, S.; Saito, M.; Kaneko, S.; Yasui-Furukori, N. Decreased serum levels of polyunsaturated fatty acids and folate, but not brain-derived neurotrophic factor, in childhood and adolescent females with depression. Psychiatry Res. 2014, 225, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Newton, D.F.; Naiberg, M.R.; Andreazza, A.C.; Scola, G.; Dickstein, D.P.; Goldstein, B.I. Association of Lipid Peroxidation and Brain-Derived Neurotrophic Factor with Executive Function in Adolescent Bipolar Disorder. Psychopharmacology 2016, 234, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Inal-Emiroglu, F.N.; Resmi, H.; Karabay, N.; Güleryüz, H.; Baykara, B.; Cevher, N.; Akay, A. Decreased Right Hippocampal Volumes and Neuroprogression Markers in Adolescents with Bipolar Disorder. Neuropsychobiology 2015, 71, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Peruzzolo, T.L.; Anes, M.; de Moura Kohmann, A.; Souza, A.C.M.L.; Rodrigues, R.B.; Brun, J.B.; Peters, R.; De Aguiar, B.W.; Kapczinski, F.; Tramontina, S.; et al. Correlation between Peripheral Levels of Brain-Derived Neurotrophic Factor and Hippocampal Volume in Children and Adolescents with Bipolar Disorder. Neural Plast. 2015, 2015, 324825. [Google Scholar] [CrossRef]
- Pallavi, P.; Sagar, R.; Mehta, M.; Sharma, S.; Subramanium, A.; Shamshi, F.; Sengupta, U.; Qadri, R.; Pandey, R.M.; Mukhopadhyay, A.K. Serum neurotrophic factors in adolescent depression: Gender difference and correlation with clinical severity. J. Affect. Disord. 2013, 150, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Pandey, G.N.; Dwivedi, Y.; Rizavi, H.S.; Ren, X.; Zhang, H.; Pavuluri, M.N. Brain-derived neurotrophic factor gene and protein expression in pediatric and adult depressed subjects. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2010, 34, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, K.H.; Kim, S.H.; Han, J.Y.; Hong, S.-B.; Cho, S.-C.; Kim, J.-W.; Brent, D. Early changes of serum BDNF and SSRI response in adolescents with major depressive disorder. J. Affect. Disord. 2020, 265, 325–332. [Google Scholar] [CrossRef]
- Shi, Y.; Luan, D.; Song, R.; Zhang, Z. Value of peripheral neurotrophin levels for the diagnosis of depression and response to treatment: A systematic review and meta-analysis. Eur. Neuropsychopharmacol. 2020, 41, 40–51. [Google Scholar] [CrossRef]
- Fernandes, B.S.; Molendijk, M.L.; Kohler, C.A.; Soares, J.C.; Leite, C.M.G.S.; Machado-Vieira, R.; Ribeiro, T.L.; Silva, J.C.; Sales, P.M.G.; Quevedo, J.; et al. Peripheral brain-derived neurotrophic factor (BDNF) as a biomarker in bipolar disorder: A meta-analysis of 52 studies. BMC Med. 2015, 13, 289. [Google Scholar] [CrossRef] [Green Version]
- Herberth, M.; Koethe, D.; Levin, Y.; Schwarz, E.; Krzyszton, N.D.; Schoeffmann, S.; Ruh, H.; Rahmoune, H.; Kranaster, L.; Schoenborn, T.; et al. Peripheral profiling analysis for bipolar disorder reveals markers associated with reduced cell survival. Proteomics 2010, 11, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Stelzhammer, V.; Haenisch, F.; Chan, M.; Cooper, J.D.; Steiner, J.; Steeb, H.; Martins-De-Souza, D.; Rahmoune, H.; Guest, P.; Bahn, S. Proteomic changes in serum of first onset, antidepressant drug-naïve major depression patients. Int. J. Neuropsychopharmacol. 2014, 17, 1599–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bot, M.; Chan, M.; Jansen, R.; Lamers, F.; Vogelzangs, N.; Steiner, J.; Leweke, F.; Rothermundt, M.; Cooper, J.D.; Bahn, S.; et al. Serum proteomic profiling of major depressive disorder. Transl. Psychiatry 2015, 5, e599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musil, R.; Schwarz, M.; Riedel, M.; Dehning, S.; Cerovecki, A.; Spellmann, I.; Arolt, V.; Müller, N. Elevated macrophage migration inhibitory factor and decreased transforming growth factor-beta levels in major depression—No influence of celecoxib treatment. J. Affect. Disord. 2011, 134, 217–225. [Google Scholar] [CrossRef]
- Shi, S.; Li, L.; Song, L.; Wang, X. Effect of lamotrigine on cognitive function and serum inflammatory factors in patients with depression of recurrent bipolar disorder. Pak. J. Pharm. Sci. 2018, 31, 2775–2778. [Google Scholar]
- Cattaneo, A.; Ferrari, C.; Uher, R.; Bocchio-Chiavetto, L.; Riva, M.A.; Pariante, C.M.; The MRC ImmunoPsychiatry Consortium. Absolute Measurements of Macrophage Migration Inhibitory Factor and Interleukin-1-β mRNA Levels Accurately Predict Treatment Response in Depressed Patients. Int. J. Neuropsychopharmacol. 2016, 19, 31–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuellar-Barboza, A.; Sánchez-Ruiz, J.A.; Rodriguez-Sanchez, I.P.; González, S.; Calvo, G.; Lugo, J.; Costilla-Esquivel, A.; Martínez, L.E.; Ibarra-Ramirez, M. Gene expression in peripheral blood in treatment-free major depression. Acta Neuropsychiatr. 2020, 32, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Lipschutz, R.; Bick, J.; Nguyen, V.; Lee, M.; Leng, L.; Grigorenko, E.; Bucala, R.; Mayes, L.C.; Crowley, M.J. Macrophage migration inhibitory factor (MIF) gene is associated with adolescents’ cortisol reactivity and anxiety. Psychoneuroendocrinology 2018, 95, 170–178. [Google Scholar] [CrossRef]
- Wang, X.; Sundquist, K.; Palmér, K.; Hedelius, A.; Memon, A.; Sundquist, J. Macrophage Migration Inhibitory Factor and microRNA-451a in Response to Mindfulness-based Therapy or Treatment as Usual in Patients with Depression, Anxiety, or Stress and Adjustment Disorders. Int. J. Neuropsychopharmacol. 2018, 21, 513–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, K.M.; Bosch, J.A.; Engeland, C.G.; Cacioppo, J.T.; Marucha, P.T. Elevated Macrophage Migration Inhibitory Factor (MIF) is associated with depressive symptoms, blunted cortisol reactivity to acute stress, and lowered morning cortisol. Brain Behav. Immun. 2010, 24, 1202–1208. [Google Scholar] [CrossRef]
- He, Y.; Vinkers, C.H.; Houtepen, L.; De Witte, L.D.; Boks, M.P. Childhood Adversity Is Associated With Increased KITLG Methylation in Healthy Individuals but Not in Bipolar Disorder Patients. Front. Psychiatry 2019, 9, 743. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All Patients | MDD | BD | Control | |
|---|---|---|---|---|
| n | 79 | 52 | 27 | 31 |
| Female/Male | 56/23 | 39/13 | 17/10 | 26/5 |
| Mean age | 18.59 (±3.28) | 18.67 (±3.54) | 18.44 (±2.79) | 21.1 (±2.68) |
| Mean age at illness onset | 16.77 (±2.76) | 16.82 (±2.96) | 16.6 (±2.31) | NA |
| Drug free yes/no | 25/54 | 21/31 | 4/23 | |
| Inpatient/outpatient | 60/19 | 36/16 | 24/3 | |
| Mean number of hospitalization | 1.27 (±0.74) | 1.25 (±0.80) | 1.29 (±0.62) | |
| Family history of bipolar disorder = yes/no | 38/41 | 29/23 | 9/18 | |
| Change of diagnosis to BD | 19 | 15 | 4 | |
| HDRS-17 | 14.62 (±8.27) | 19.37 (±5.30) | 5.48 (±4.27) | |
| YMRS | 6.71 (±9.10) | 1.04 (±1.55) | 17.6 (±7.47) | |
| BDNF (pg/mL) (mean ± SD) | 25,154.48 (±7937.7) | 24,118.76 (±6318.7) | 27,149.21 (±10219.1) | 22,349.56 (±7078.5) |
| proBDNF (pg/mL) (mean ± SD) | 2202.25 (±2187) | 2379.82 (±2282.2) | 1860.26 (±1987) | 3224.38 (±3336.3) |
| mBDNF (pg/mL) (mean ± SD) | 22,952.23 (±8201.1) | 21,738.93 (±6474.5) | 25,288.95 (±10532.5) | 19,125.18 (±7879.6) |
| rBDNF (mean ± SD) | 23.97 (±24.4) | 23.57 (±25.8) | 24.79 (±21.52) | 19.09 (±18.4) |
| EGF (pg/mL) (mean ± SD) | 229.95 (±154.1) | 230.77 (±154.9) | 228.37 (±155.3) | 156.05 (±165.1) |
| MIF (pg/mL) (mean ± SD) | 1871.55 (±1035.4) | 1927.63 (±1136.4) | 1763.55 (±815.28) | 2295.74 (±1471.7) |
| SCF (pg/mL) (mean ± SD) | 155.02 (±100.1) | 161.49 (±116.2) | 142.86 (±59.31) | 168.58 (±150.8) |
| Mean Rank | ||||||
|---|---|---|---|---|---|---|
| MDD | BD | CON | H | Χ2 | p | |
| BDNF | 56.06 | 62.22 | 48.71 | 2.62 | 1.22 | 0.2699 |
| proBDNF | 58.14 | 49.15 | 56.61 | 1.46 | 1.65 | 0.4812 |
| mBDNF | 55.33 | 63.56 | 48.77 | 3.10 | 1.73 | 0.2121 |
| rBDNF | 52.98 | 60.28 | 52.39 | 1.12 | 3.22 | 0.5727 |
| EGF | 63.67 | 63.74 | 37.00 | 15.67 | 10.84 | 0.0004 |
| MIF | 56.02 | 54.59 | 57.16 | 0.09 | 0.61 | 0.9546 |
| SCF | 52.85 | 49.02 | 49.71 | 0.36 | 0.58 | 0.836 |
| Baseline vs. Euthymia | Baseline vs. 24 Month | |||||
|---|---|---|---|---|---|---|
| MDD | BD | MDD + BD | ||||
| Z | p | Z | p | Z | p | |
| BDNF | 1.91 | 0.06 | 1.57 | 0.12 | 0.96 | 0.34 |
| proBDNF | 1.02 | 0.31 | 1.15 | 0.25 | 0.05 | 0.96 |
| mBDNF | 1.33 | 0.18 | 1.08 | 0.28 | 0.795 | 0.43 |
| rBDNF | 0.33 | 0.74 | 0.31 | 0.75 | 0.435 | 0.66 |
| EGF | 1.04 | 0.30 | 2.41 | 0.02 | 0.665 | 0.51 |
| MIF | 0.51 | 0.61 | 0.10 | 0.92 | 0.185 | 0.85 |
| SCF | 0.28 | 0.78 | 0.18 | 0.86 | 1.495 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skibinska, M.; Kapelski, P.; Dmitrzak-Weglarz, M.; Lepczynska, N.; Pawlak, J.; Twarowska-Hauser, J.; Szczepankiewicz, A.; Rajewska-Rager, A. Elevated Epidermal Growth Factor (EGF) as Candidate Biomarker of Mood Disorders—Longitudinal Study in Adolescent and Young Adult Patients. J. Clin. Med. 2021, 10, 4064. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184064
Skibinska M, Kapelski P, Dmitrzak-Weglarz M, Lepczynska N, Pawlak J, Twarowska-Hauser J, Szczepankiewicz A, Rajewska-Rager A. Elevated Epidermal Growth Factor (EGF) as Candidate Biomarker of Mood Disorders—Longitudinal Study in Adolescent and Young Adult Patients. Journal of Clinical Medicine. 2021; 10(18):4064. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184064
Chicago/Turabian StyleSkibinska, Maria, Pawel Kapelski, Monika Dmitrzak-Weglarz, Natalia Lepczynska, Joanna Pawlak, Joanna Twarowska-Hauser, Aleksandra Szczepankiewicz, and Aleksandra Rajewska-Rager. 2021. "Elevated Epidermal Growth Factor (EGF) as Candidate Biomarker of Mood Disorders—Longitudinal Study in Adolescent and Young Adult Patients" Journal of Clinical Medicine 10, no. 18: 4064. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184064