
Impact of COVID-19 Pandemic on Remote Monitoring of Cardiac Implantable Electronic Devices in Italy: Results of a Survey Promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing)

 , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
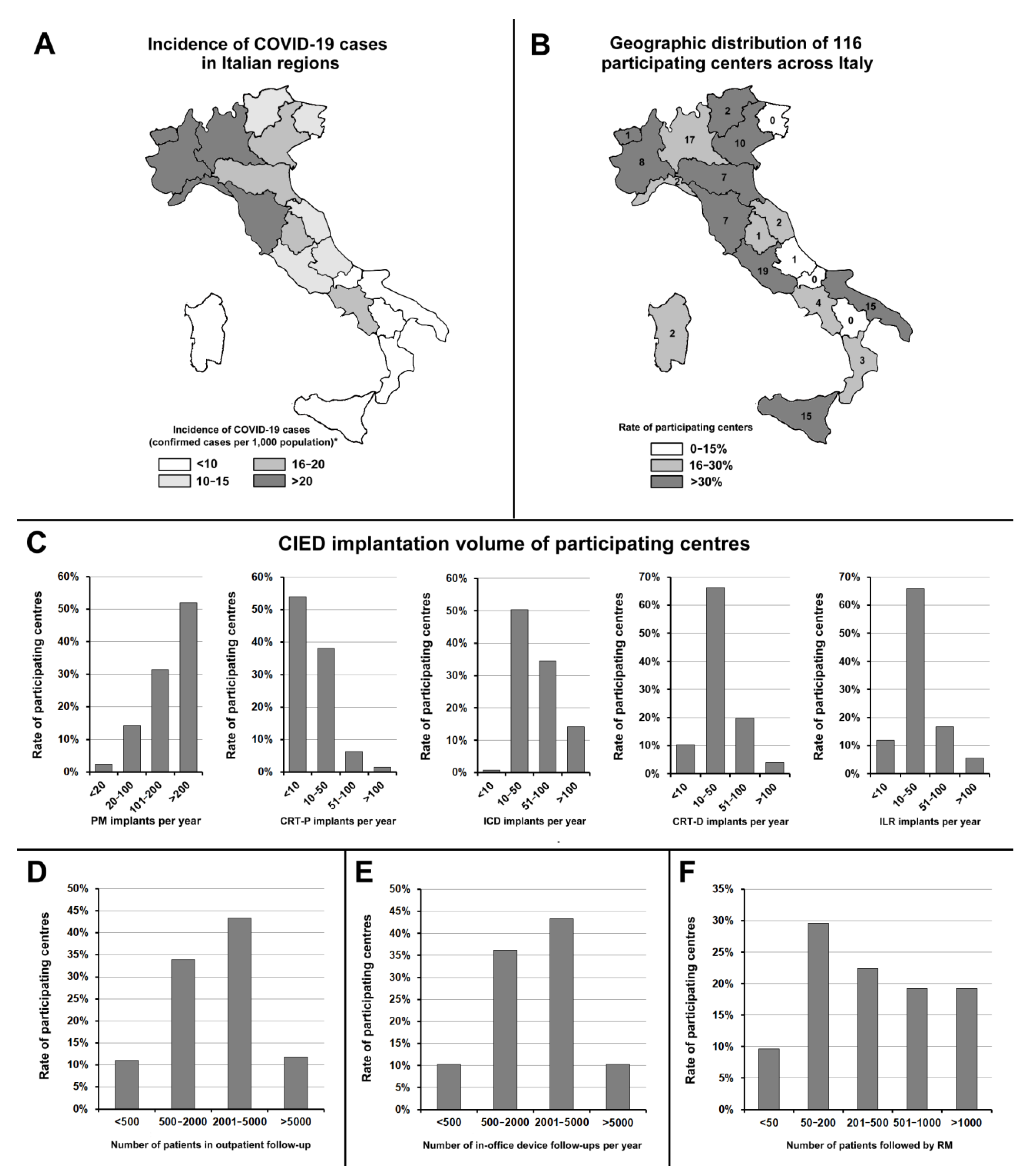
3.1. Participating Centres
3.2. Use of Remote Monitoring
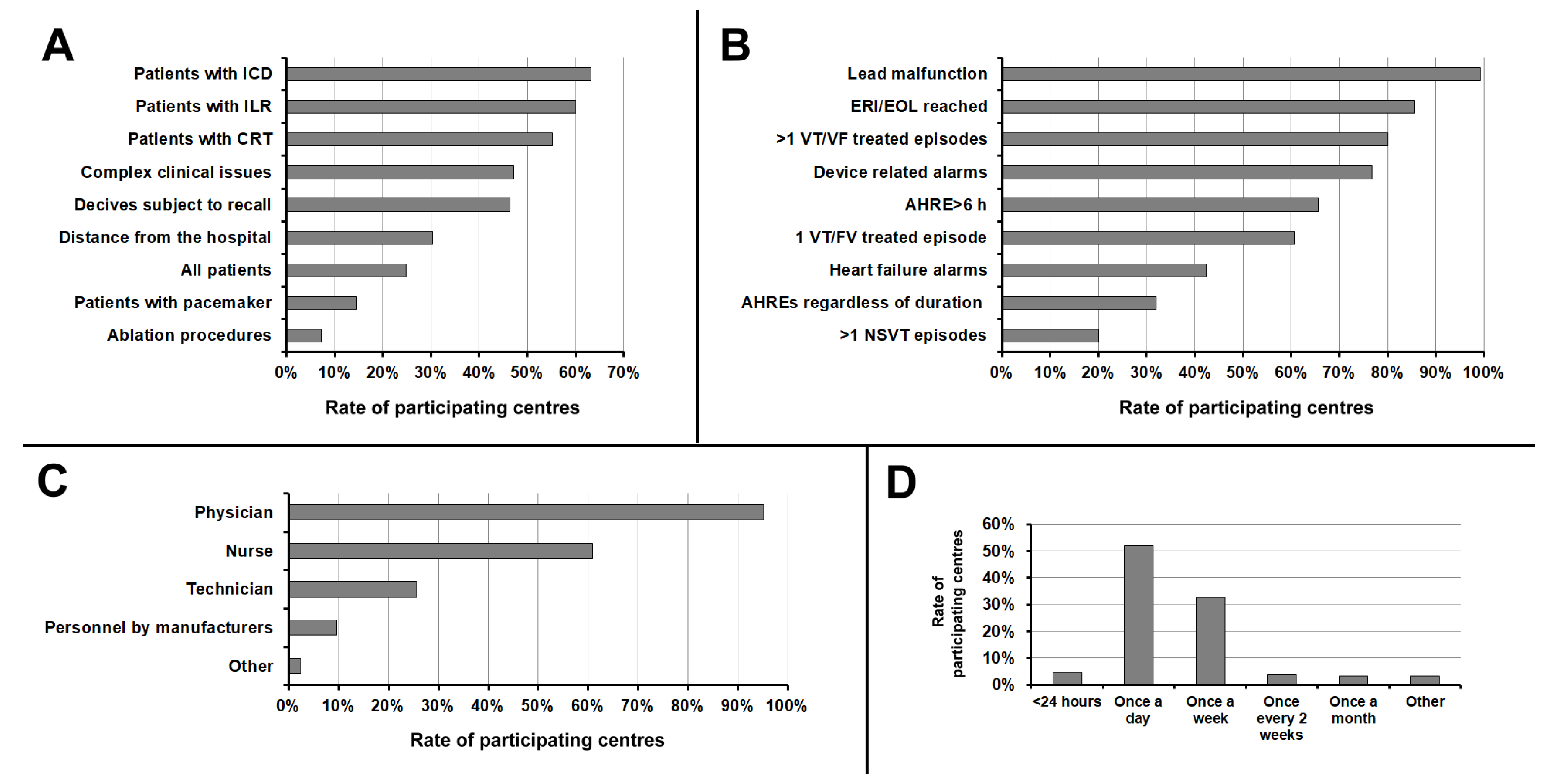
3.3. Organisation of Remote Monitoring
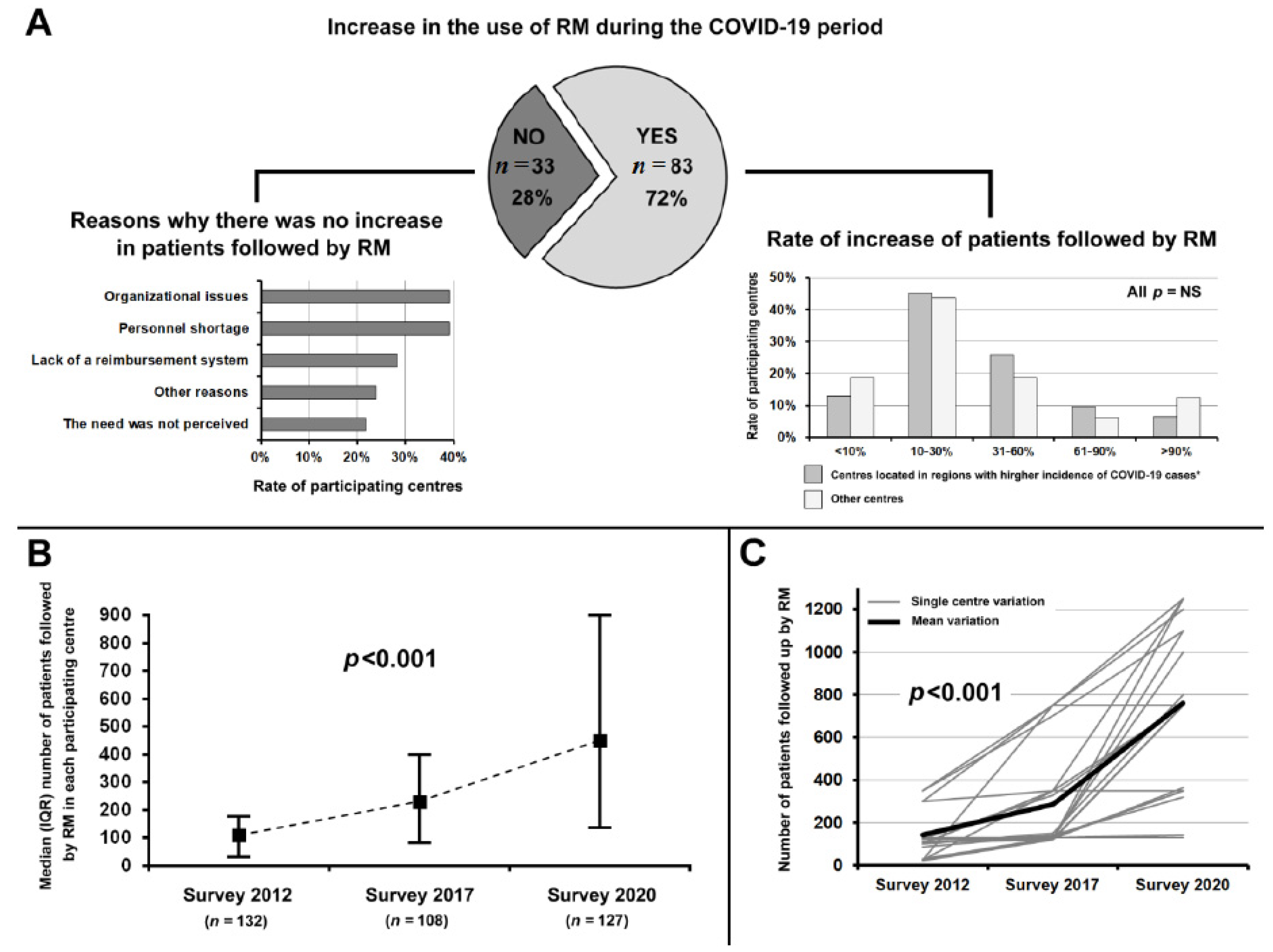
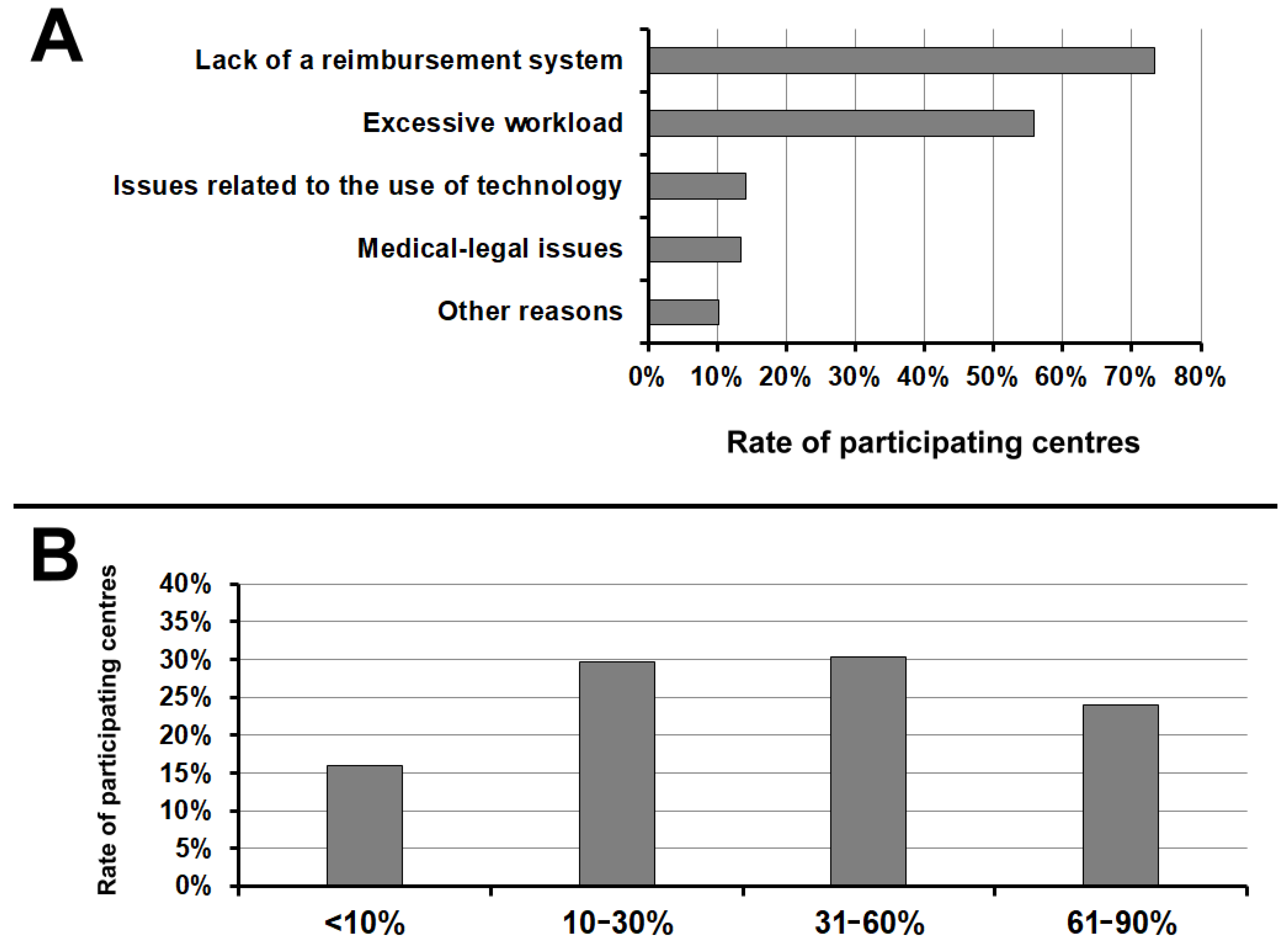
3.4. Impact of COVID-19 Pandemic on the Use of Remote Monitoring
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boriani, G.; Palmisano, P.; Guerra, F.; Bertini, M.; Zanotto, G.; Lavalle, C.; Notarstefano, P.; Accogli, M.; Bisignani, G.; Forleo, G.B.; et al. Impact of COVID-19 pandemic on the clinical activities related to arrhythmias and electrophysiology in Italy: Results of a survey promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing). Intern. Emerg. Med. 2020, 15, 1445–1456. [Google Scholar] [CrossRef]
- Maines, M.; Zorzi, A.; Benetollo, P.P.; Guarrera, G.M.; Moz, M.; Manica, A.; Demattè, C.; Del Greco, M. Short-term outcome associated with remote evaluation (telecardiology) of patients with cardiovascular diseases during the COVID-19 pandemic. Int. J. Cardiol. Heart Vasc. 2020, 30, 100625. [Google Scholar] [CrossRef] [PubMed]
- Censimento Delle Strutture Aritmologiche Italiane AIAC. 2019. Available online: https://aiac.it/attivita/censimenti/ (accessed on 4 January 2021).
- COVID-19 ITALIA. Data from Italian Civil Protection Department. 2020. Available online: http://opendatadpc.maps.arcgis.com/apps/opsdashboard/index.html#/b0c68bce2cce478eaac82fe38d4138b1 (accessed on 13 November 2020).
- Palmisano, P.; Melissano, D.; Zanotto, G.; Perego, G.B.; Toselli, T.; Landolina, M.; Ricci, R.P. Italian Association of Arrhythmology, Cardiac Pacing (AIAC). Change in the use of remote monitoring of cardiac implantable electronic devices in Italian clinical practice over a 5-year period: Results of two surveys promoted by the AIAC (Italian Association of Arrhythmology and Cardiac Pacing). J. Cardiovasc. Med. 2020, 21, 305–314. [Google Scholar]
- Slotwiner, D.; Varma, N.; Akar, J.G.; Annas, G.; Beardsall, M.; Fogel, R.I.; Galizio, N.O.; Glotzer, T.V.; Leahy, R.A.; Love, C.J.; et al. HRS Expert Consensus Statement on remote interrogation and monitoring for cardiovascular implantable electronic devices. Heart Rhythm 2015, 12, e69–e100. [Google Scholar] [CrossRef]
- Maines, M.; Zorzi, A.; Tomasi, G.; Angheben, C.; Catanzariti, D.; Piffer, L.; Del Greco, M. Clinical impact, safety, and accuracy of the remotely monitored implantable loop recorder Medtronic Reveal LINQTM. Europace 2018, 20, 1050–1057. [Google Scholar] [CrossRef]
- Landolina, M.; Perego, G.B.; Lunati, M.; Curnis, A.; Guenzati, G.; Vicentini, A.; Parati, G.; Borghi, G.; Zanaboni, P.; Valsecchi, S.; et al. Remote monitoring reduces healthcare use and improves quality of care in heart failure patients with implantable defibrillators: The evolution of management strategies of heart failure patients with implantable defibrillators (EVOLVO) study. Circulation 2012, 125, 2985–2992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guédon-Moreau, L.; Lacroix, D.; Sadoul, N.; Clémenty, J.; Kouakam, C.; Hermida, J.S.; Aliot, E.; Boursier, M.; Bizeau, O.; Kacet, S.; et al. A randomized study of remote follow-up of implantable cardioverter defibrillators: Safety and efficacy report of the ECOST trial. Eur. Heart J. 2013, 34, 605–614. [Google Scholar] [CrossRef] [Green Version]
- Ricci, R.P.; Morichelli, L.; Quarta, L.; Porfili, A.; Magris, B.; Giovene, L.; Torcinaro, S.; Gargaro, A. Effect of daily remote monitoring on pacemaker longevity: A retrospective analysis. Heart Rhythm 2015, 12, 330–337. [Google Scholar] [CrossRef]
- Campana, A.; Giofrè, F.; Stabile, G.; Iori, M.; La Rosa, C.; Tomasi, C.; Calzolari, V.; Miracapillo, G.; Notarstefano, P.; Carinci, V.; et al. Use of remote monitoring in the management of ICD end-of-life: Data from the DECODE registry. Int. J. Cardiol. 2016, 221, 430–432. [Google Scholar] [CrossRef]
- Zanotto, G.; Melissano, D.; Baccillieri, S.; Campana, A.; Caravati, F.; Maines, M.; Platania, F.; Zuccaro, L.; Landolina, M.; Berisso, M.Z.; et al. Intrahospital organizational model of remote monitoring data sharing, for a global management of patients with cardiac implantable electronic devices: A document of the Italian Association of Arrhythmology and Cardiac Pacing. J. Cardiovasc. Med. 2020, 21, 171–181. [Google Scholar] [CrossRef]
- Maines, M.; Tomasi, G.; Moggio, P.; Peruzza, F.; Catanzariti, D.; Angheben, C.; Simoncelli, M.; Degiampietro, M.; Piffer, L.; Valsecchi, S.; et al. Implementation of remote follow-up of cardiac implantable electronic devices in clinical practice: Organizational implications and resource consumption. J. Cardiovasc. Med. 2020, 21, 648–653. [Google Scholar] [CrossRef]
- Maines, M.; Tomasi, G.; Moggio, P.; Poian, L.; Peruzza, F.; Catanzariti, D.; Angheben, C.; Cont, N.; Valsecchi, S.; Del Greco, M. Scheduled versus alert transmissions for remote follow-up of cardiac implantable electronic devices: Clinical relevance and resource consumption. Int. J. Cardiol. 2021, 334, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Crossley, G.H.; Chen, J.; Choucair, W.; Cohen, T.J.; Gohn, D.C.; Johnson, W.B.; Kennedy, E.E.; Mongeon, L.R.; Serwer, G.A.; Qiao, H.; et al. Clinical benefits of remote versus transtelephonic monitoring of implanted pacemakers. J. Am. Coll. Cardiol. 2009, 54, 2012–2019. [Google Scholar] [CrossRef] [Green Version]
- Crossley, G.H.; Boyle, A.; Vitense, H.; Chang, Y.; Mead, R.H.; CONNECT Investigators. The CONNECT (Clinical Evaluation of Remote Notification to Reduce Time to Clinical Decision) trial: The value of wireless remote monitoring with automatic clinician alerts. J. Am. Coll. Cardiol. 2011, 57, 1181–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boriani, G.; Glotzer, T.V.; Santini, M.; West, T.M.; De Melis, M.; Sepsi, M.; Gasparini, M.; Lewalter, T.; Camm, J.A.; Singer, D.E. Device-detected atrial fibrillation and risk for stroke: An analysis of >10,000 patients from the SOS AF project (Stroke preventiOn Strategies based on Atrial Fibrillation information from implanted devices). Eur. Heart J. 2014, 35, 508–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Boriani, G.; Healey, J.S.; Schnabel, R.B.; Lopes, R.D.; Calkins, H.; Camm, J.A.; Freedman, B. Oral anticoagulation for subclinical atrial tachyarrhythmias detected by implantable cardiac devices: An international survey of the AF-SCREEN Group. Int. J. Cardiol. 2019, 296, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.; Camm, J.; Calkins, H.; Healey, J.S.; Rosenqvist, M.; Wang, J.; Albert, C.M.; Anderson, C.S.; Antoniou, S.; Benjamin, E.J.; et al. AF-Screen Collaborators. Screening for Atrial Fibrillation: A Report of the AF-SCREEN International Collaboration. Circulation 2017, 135, 1851–1867. [Google Scholar] [CrossRef]
- Boriani, G. Remote monitoring of cardiac implantable electrical devices in Europe: Quo vadis? Europace 2015, 17, 674–676. [Google Scholar] [CrossRef]
- Mairesse, G.H.; Braunschweig, F.; Klersy, K.; Cowie, M.R.; Leyva, F. Implementation and reimbursement of remote monitoring for cardiac implantable electronic devices in Europe: A survey from the health economics committee of the European Heart Rhythm Association. Europace 2015, 17, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Caballero, S.; Selles, M.A.; Peydro, M.A.; Perez-Bernabeu, E. An Efficient COVID-19 Prediction Model Validated with the Cases of China, Italy and Spain: Total or Partial Lockdowns? J. Clin. Med. 2020, 9, 1547. [Google Scholar] [CrossRef]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. The Enemy Which Sealed the World: Effects of COVID-19 Diffusion on the Psychological State of the Italian Population. J. Clin. Med. 2020, 9, 1802. [Google Scholar] [CrossRef]
- Varma, N.; Marrouche, N.F.; Aguinaga, L.; Albert, C.M.; Arbelo, E.; Choi, J.I.; Chung, M.K.; Conte, G.; Dagher, L.; Epstein, L.M.; et al. HRS/EHRA/APHRS/LAHRS/ACC/AHA Worldwide Practice Update for Telehealth and Arrhythmia Monitoring During and After a Pandemic. J. Am. Coll. Cardiol. 2020, 76, 1363–1374. [Google Scholar] [CrossRef]
- De Rosa, S.; Spaccarotella, C.; Basso, C.; Calabrò, M.P.; Curcio, A.; Filardi, P.P.; Mancone, M.; Mercuro, G.; Muscoli, S.; Nodari, S.; et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur. Heart J. 2020, 41, 2083–2088. [Google Scholar] [CrossRef]
- Fileti, L.; Vecchio, S.; Moretti, C.; Reggi, A.; Aquilina, M.; Balducelli, M.; Santarelli, A.; Grosseto, D.; Piovaccari, G.; Rubboli, A. Impact of the COVID-19 pandemic on coronary invasive procedures at two Italian high-volume referral centers. J. Cardiovasc. Med. 2020, 21, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Tomasoni, D.; Adamo, M.; Italia, L.; Branca, L.; Chizzola, G.; Fiorina, C.; Lupi, L.; Inciardi, R.M.; Cani, D.S.; Lombardi, C.M.; et al. Impact of COVID-2019 outbreak on prevalence, clinical presentation and outcomes of ST-elevation myocardial infarction. J. Cardiovasc. Med. 2020, 21, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Toniolo, M.; Negri, F.; Antonutti, M.; Masè, M.; Facchin, D. Unpredictable Fall of Severe Emergent Cardiovascular Diseases Hospital Admissions During the COVID-19 Pandemic: Experience of a Single Large Center in Northern Italy. J. Am. Heart Assoc. 2020, 9, e017122. [Google Scholar] [CrossRef]
- Migliore, F.; Zorzi, A.; Gregori, D.; Del Monte, A.; Falzone, P.V.; Verlato, R.; Siciliano, M.; Themistoclakis, S.; China, P.; Marchese, D.; et al. Padua School of Cardiology Network. Urgent Pacemaker Implantation Rates in the Veneto Region of Italy After the COVID-19 Outbreak. Circ. Arrhythm. Electrophysiol. 2020, 13, e008722. [Google Scholar] [CrossRef] [PubMed]
- Baldi, E.; Sechi, G.M.; Mare, C.; Canevari, F.; Brancaglione, A.; Primi, R.; Klersy, C.; Palo, A.; Contri, E.; Ronchi, V.; et al. Lombardia CARe researchers. COVID-19 kills at home: The close relationship between the epidemic and the increase of out-of-hospital cardiac arrests. Eur. Heart J. 2020, 41, 3045–3054. [Google Scholar] [CrossRef]
- O’Shea, C.J.; Thomas, G.; Middeldorp, M.E.; Harper, C.; Elliott, A.D.; Ray, N.; Lau, D.H.; Campbell, K.; Sanders, P. Ventricular arrhythmia burden during the coronavirus disease 2019 (COVID-19) pandemic. Eur. Heart J. 2021, 42, 520–528. [Google Scholar] [CrossRef]
- Varma, N. Remote monitoring for advisories: Automatic early detection of silent lead failure. Pacing Clin. Electrophysiol. 2009, 32, 525–527. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, P.; Pisanò, E.C.L.; La Rosa, C.; Ammendola, E.; Zaccaria, M.; Milanese, G.; Lauretti, M.; Rillo, M.; Aloisio, A.; Rago, A.; et al. Effectiveness of Implantable DEfibrillators Alert Systems: Comparison between audible and vibratory alert: IDEAS study. J. Cardiovasc. Med. 2019, 20, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Varma, N.; Michalski, J.; Epstein, A.E.; Schweikert, R. Automatic remote monitoring of implantable cardioverter-defibrillator lead and generator performance: The Lumos-T Safely RedUceS RouTine Office Device Follow-Up (TRUST) trial. Circ. Arrhythm. Electrophysiol. 2010, 3, 428–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mabo, P.; Victor, F.; Bazin, P.; Ahres, S.; Babuty, D.; Da Costa, A.; Binet, D.; Daubert, J.C.; COMPAS Trial Investigators. A randomized trial of long-term remote monitoring of pacemaker recipients (the COMPAS trial). Eur. Heart J. 2012, 33, 1105–1111. [Google Scholar] [CrossRef] [Green Version]
- Ricci, R.P.; Morichelli, L.; D’Onofrio, A.; Calò, L.; Vaccari, D.; Zanotto, G.; Curnis, A.; Buja, G.; Rovai, N.; Gargaro, A. Effectiveness of remote monitoring of CIEDs in detection and treatment of clinical and device-related cardiovascular events in daily practice: The HomeGuide Registry. Europace 2013, 15, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Whellan, D.J.; Ousdigian, K.T.; Al-Khatib, S.M.; Pu, W.; Sarkar, S.; Porter, C.B.; Pavri, B.B.; O’Connor, C.M.; PARTNERS Study Investigators. Combined heart failure device diagnostics identify patients at higher risk of subsequent heart failure hospitalizations: Results from PARTNERS HF (Program to Access and Review Trending Information and Evaluate Correlation to Symptoms in Patients With Heart Failure) study. J. Am. Coll. Cardiol. 2010, 55, 1803–1810. [Google Scholar] [PubMed] [Green Version]
- Boehmer, J.P.; Hariharan, R.; Devecchi, F.G.; Smith, A.L.; Molon, G.; Capucci, A.; An, Q.; Averina, V.; Stolen, C.M.; Thakur, P.H.; et al. A Multisensor Algorithm Predicts Heart Failure Events in Patients With Implanted Devices: Results From the MultiSENSE Study. JACC Heart Fail. 2017, 5, 216–225. [Google Scholar] [CrossRef]
- Palmisano, P.; Guerra, F.; Ammendola, E.; Ziacchi, M.; Luigi Pisanò, E.C.; Dell’Era, G.; Aspromonte, V.; Zaccaria, M.; Di Ubaldo, F.; Capucci, A.; et al. Physical Activity Measured by Implanted Devices Predicts Atrial Arrhythmias and Patient Outcome: Results of IMPLANTED (Italian Multicentre Observational Registry on Patients With Implantable Devices Remotely Monitored). J. Am. Heart Assoc. 2018, 7, e008146. [Google Scholar] [CrossRef]
- Morgan, J.M.; Kitt, S.; Gill, J.; McComb, J.M.; Ng, G.A.; Raftery, J.; Roderick, P.; Seed, A.; Williams, S.G.; Witte, K.K.; et al. Remote management of heart failure using implantable electronic devices. Eur. Heart J. 2017, 38, 2352–2360. [Google Scholar] [CrossRef] [Green Version]
- Klersy, C.; De Silvestri, A.; Gabutti, G.; Regoli, F.; Auricchio, A. A meta-analysis of remote monitoring of heart failure patients. J. Am. Coll. Cardiol. 2009, 54, 1683–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maines, M.; Palmisano, P.; Del Greco, M.; Melissano, D.; De Bonis, S.; Baccillieri, S.; Zanotto, G.; D’Onofrio, A.; Ricci, R.P.; De Ponti, R.; et al. Impact of COVID-19 Pandemic on Remote Monitoring of Cardiac Implantable Electronic Devices in Italy: Results of a Survey Promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing). J. Clin. Med. 2021, 10, 4086. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184086
Maines M, Palmisano P, Del Greco M, Melissano D, De Bonis S, Baccillieri S, Zanotto G, D’Onofrio A, Ricci RP, De Ponti R, et al. Impact of COVID-19 Pandemic on Remote Monitoring of Cardiac Implantable Electronic Devices in Italy: Results of a Survey Promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing). Journal of Clinical Medicine. 2021; 10(18):4086. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184086
Chicago/Turabian StyleMaines, Massimiliano, Pietro Palmisano, Maurizio Del Greco, Donato Melissano, Silvana De Bonis, Stella Baccillieri, Gabriele Zanotto, Antonio D’Onofrio, Renato Pietro Ricci, Roberto De Ponti, and et al. 2021. "Impact of COVID-19 Pandemic on Remote Monitoring of Cardiac Implantable Electronic Devices in Italy: Results of a Survey Promoted by AIAC (Italian Association of Arrhythmology and Cardiac Pacing)" Journal of Clinical Medicine 10, no. 18: 4086. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10184086