Drug-Induced Acute Kidney Injury: A Study from the French Medical Administrative and the French National Pharmacovigilance Databases Using Capture-Recapture Method

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Case Definition
2.3. Collection of Drug-Induced Acute Kidney Injury (DIAKIs) Cases
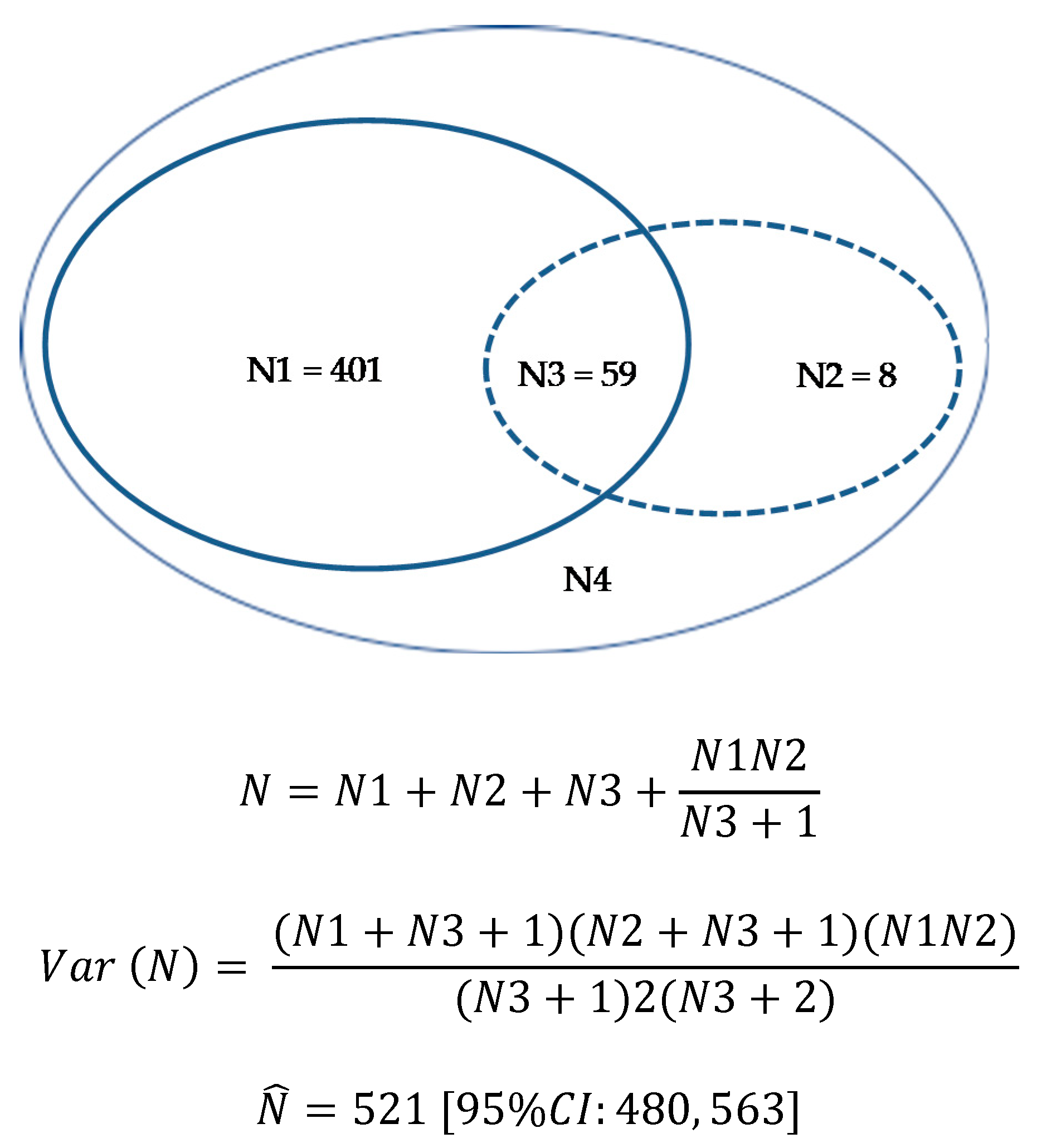
2.4. Estimation of the Prevalence of DIAKI Cases in Hospital Stays Using Capture-Recapture Method
2.5. Description and Analysis of DIAKI Cases
3. Results
3.1. Hospital Stays Selection
3.2. Pharmacovigilance Cases Selection
3.3. Estimation of the Prevalence of DIAKIs in Hospital Stays Using Capture-Recapture Method
3.4. Description of the DIAKI Cases
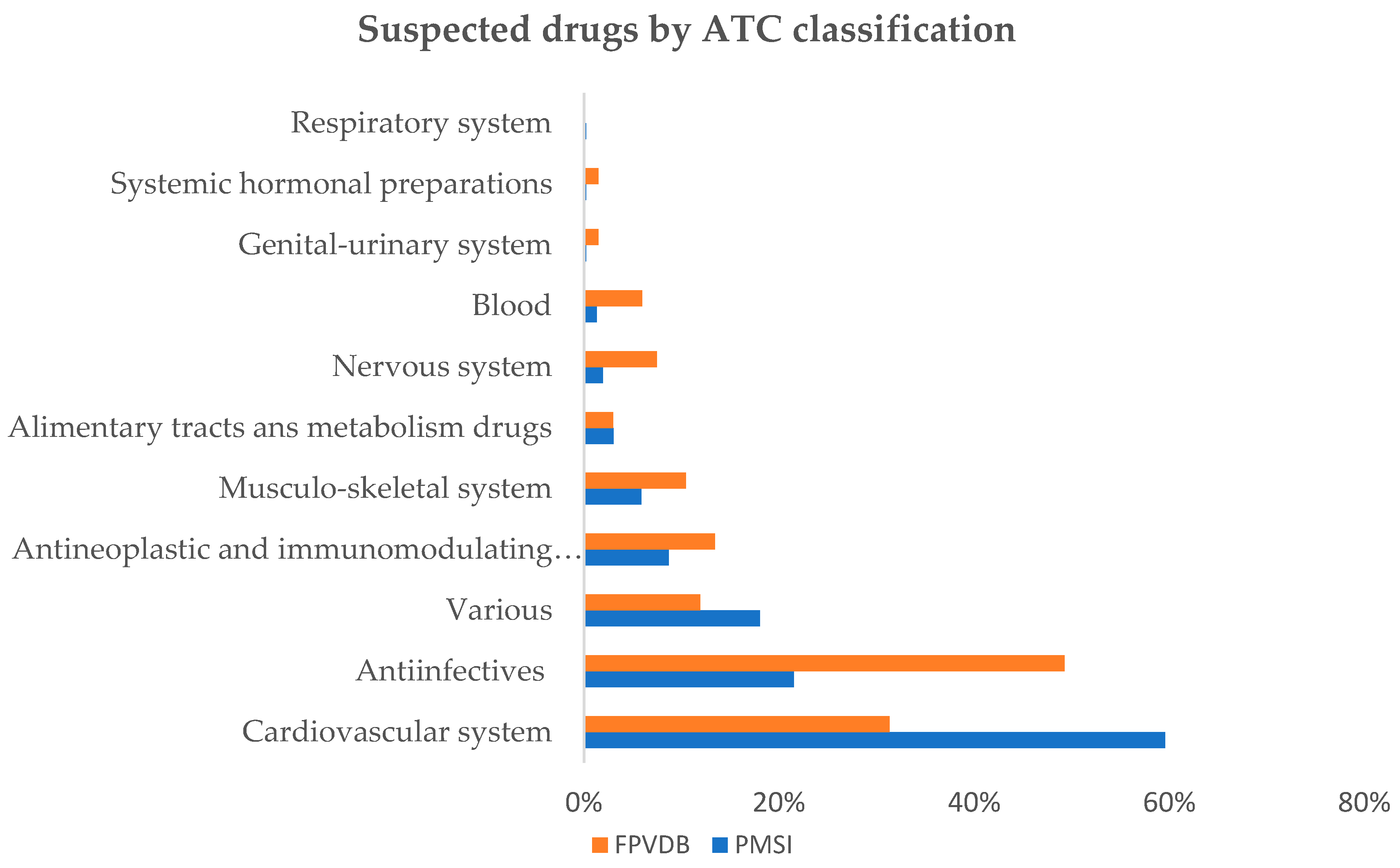
3.5. Description of the Drug Involved in DIAKIs
4. Discussion
4.1. DIAKIs Prevalence and Notification Rate
4.2. DIAKI Cases Characteristics
4.3. Drugs Involved in DIAKI Cases
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Susantitaphong, P.; Cruz, D.N.; Cerda, J.; Abulfaraj, M.; Alqahtani, F.; Koulouridis, I.; Jaber, B.L. World Incidence of AKI: A meta-analysis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1482–1493. [Google Scholar] [CrossRef] [Green Version]
- Kurzhagen, J.T.; Dellepiane, S.; Cantaluppi, V.; Rabb, H. AKI: An increasingly recognized risk factor for CKD development and progression. J. Nephrol. 2020, 33, 1171–1187. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.; Bagga, A.; Cruz, D.; De Maeseneer, J.; Endre, Z.; Kellum, J.A.; Liu, K.D.; Mehta, R.L.; Pannu, N.; Van Biesen, W.; et al. Acute kidney injury: An increasing global concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Taber, S.S.; Pasko, D.A. The epidemiology of drug-induced disorders: The kidney. Expert Opin. Drug Saf. 2008, 7, 679–690. [Google Scholar] [CrossRef]
- Perazella, M.A. Pharmacology behind common drug nephrotoxicities. Clin. J. Am. Soc. Nephrol. 2018, 13, 1897–1908. [Google Scholar] [CrossRef]
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef]
- Osmont, M.-N.; Degremont, A.; Jantzem, H.; Audouard-Marzin, Y.; Lalanne, S.; Carlhant-Kowalski, D.; Bellissant, E.; Oger, E.; Polard, E. Hospital databases for the identification of adverse drug reactions: A 2-year multicentre study in 9 French general hospitals. Br. J. Clin. Pharmacol. 2020. [Google Scholar] [CrossRef]
- Durrieu, G.; Batz, A.; Rousseau, V.; Bondon-Guitton, E.; Petiot, D.; Montastruc, J.L. Use of administrative hospital database to identify adverse drug reactions in a Pediatric University Hospital. Eur. J. Clin. Pharmacol. 2014, 70, 1519–1526. [Google Scholar] [CrossRef]
- Lugardon, S.; Desboeuf, K.; Fernet, P.; Montastruc, J.-L.; Lapeyre-Mestre, M. Using a capture–recapture method to assess the frequency of adverse drug reactions in a French university hospital. Br. J. Clin. Pharmacol. 2006, 62, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- ICD-10 Version: 2019. Available online: https://icd.who.int/browse10/2019/en#/ (accessed on 5 November 2020).
- CCAM en Ligne-Plan de la CCAM. Available online: https://www.ameli.fr/accueil-de-la-ccam/plan-de-la-ccam.php (accessed on 5 November 2020).
- MedDRA. MedDRA Hierarchy. Available online: https://www.meddra.org/how-to-use/basics/hierarchy (accessed on 5 November 2020).
- Hook, E.B.; Regal, R.R. Capture-recapture methods in epidemiology: Methods and limitations. Epidemiol. Rev. 1995, 17, 243–264. [Google Scholar] [CrossRef] [PubMed]
- Chapman, D.G. Some Properties of the Hypergeometric Distribution with Applications to Zoological Sample Censuses; University of California Press: Berkeley, CA, USA, 1951. [Google Scholar]
- Wittes, J.T. 331. Note: On the bias and estimated variance of Chapman’s two-sample capture-recapture population estimate. Biometrics 1972, 28, 592. [Google Scholar] [CrossRef]
- Mehta, R.L.; Pascual, M.T.; Soroko, S.; Savage, B.R.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Chertow, G.M. Spectrum of acute renal failure in the intensive care unit: The PICARD experience. Kidney Int. 2004, 66, 1613–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA 2005, 294, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, K.; Hafeez, A.; Hou, S. Hospital-acquired renal insufficiency. Am. J. Kidney Dis. 2002, 39, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Bonnie, R.J.; Graham, G.K. Tobacco advertising and freedom of speech. JAMA 2002, 288, 1586. [Google Scholar] [CrossRef]
- Lopez-Gonzalez, E.; Herdeiro, M.T.; Figueiras, A. Determinants of under-reporting of adverse drug reactions. Drug Saf. 2009, 32, 19–31. [Google Scholar] [CrossRef]
- Pushkin, R.; Frassetto, L.; Tsourounis, C.; Segal, E.S.; Kim, S. Improving the reporting of adverse drug reactions in the hospital setting. Postgrad. Med. 2010, 122, 154–164. [Google Scholar] [CrossRef]
- Hamzic-Mehmedbasic, A.; Rebic, D.; Balavac, M.; Muslimovic, A.; Dzemidzić, J. Clinical analysis of etiology, risk factors and outcome in patients with acute kidney injury. Mater. Socio Med. 2015, 27, 70–74. [Google Scholar] [CrossRef] [Green Version]
- Pierson-Marchandise, M.; Gras, V.; Moragny, J.; Micallef, J.; Gaboriau, L.; Picard, S.; Choukroun, G.; Masmoudi, K.; Liabeuf, S.; French National Network of Pharmacovigilance Centres. The drugs that mostly frequently induce acute kidney injury: A case-noncase study of a pharmacovigilance database. Br. J. Clin. Pharmacol. 2017, 83, 1341–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diurétiques De l’anse. Available online: https://pharmacomedicale.org/medicaments/par-specialites/item/diuretiques-de-l-anse (accessed on 8 August 2020).
- Pannu, N.; Nadim, M.K. An overview of drug-induced acute kidney injury. Crit. Care Med. 2008, 36, S216–S223. [Google Scholar] [CrossRef] [PubMed]
- Navis, G.; Faber, H.J.; De Zeeuw, D.; De Jong, P.E. ACE inhibitors and the kidney. Drug Saf. 1996, 15, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Perazella, M.A.; Markowitz, G.S. Drug-induced acute interstitial nephritis. Nat. Rev. Nephrol. 2010, 6, 461–470. [Google Scholar] [CrossRef]
- Praga, M.; González, E. Acute interstitial nephritis. Kidney Int. 2010, 77, 956–961. [Google Scholar] [CrossRef] [Green Version]
- Baker, R.J.; Pusey, C.D. The changing profile of acute tubulointerstitial nephritis. Nephrol. Dial. Transplant. 2004, 19, 8–11. [Google Scholar] [CrossRef] [Green Version]
- Garnier, A.-S.; Dellamaggiore, J.; Brilland, B.; Lagarce, L.; Abgueguen, P.; Furber, A.; Legrand, E.; Subra, J.-F.; Drablier, G.; Augusto, J.-F. High incidence of amoxicillin-induced crystal nephropathy in patients receiving high dose of intravenous amoxicillin. J. Clin. Med. 2020, 9, 2022. [Google Scholar] [CrossRef]
- Verdesca, S.; Cucchiari, D.; Monari, M.; Podestà, M.A.; Badalamenti, S. Sulfamethoxazole crystalluria. G. Ital. Nefrol. Organo Uff. Soc. Ital. Nefrol. 2015, 32, gin/32.3.5. [Google Scholar]
- Vora, S. Acute Renal Failure due to Vancomycin Toxicity in the Setting of Unmonitored Vancomycin Infusion. In Baylor University Medical Center Proceedings; Informa UK Limited: London, UK, 2016; Volume 29, pp. 412–413. [Google Scholar]
- Mahi-Birjand, M.; Yaghoubi, S.; Abdollahpour-Alitappeh, M.; Keshtkaran, Z.; Bagheri, N.; Pirouzi, A.; Khatami, M.; Sepehr, K.S.; Peymani, P.; Karimzadeh, I. Protective effects of pharmacological agents against aminoglycoside-induced nephrotoxicity: A systematic review. Expert Opin. Drug Saf. 2020, 19, 167–186. [Google Scholar] [CrossRef]
- López-Novoa, J.M.; Quiros, Y.; Vicente, L.; Morales, A.I.; López-Hernández, F.J. New insights into the mechanism of aminoglycoside nephrotoxicity: An integrative point of view. Kidney Int. 2011, 79, 33–45. [Google Scholar] [CrossRef] [Green Version]
- McCullough, P.A. Radiocontrast-induced acute kidney injury. Nephron 2008, 109, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Geenen, R.W.F.; Kingma, H.J.; Van Der Molen, A.J. Contrast-induced nephropathy: Pharmacology, pathophysiology and prevention. Insights Imaging 2013, 4, 811–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khadzhynov, D.; Schmidt, D.; Hardt, J.; Rauch, G.; Gocke, P.; Eckardt, K.-U.; Schmidt-Ott, K.M. The incidence of acute kidney injury and associated hospital mortality. Dtsch. Aerzteblatt Online 2019, 116, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Gallay, A.; Nardone, A.; Vaillant, V.; Desenclos, J.-C. The capture-recapture applied to epidemiology: Principles, limits and application. Rev. Épidémiol. Santé Publique 2002, 50, 219–232. [Google Scholar]



{kind=link}
{kind=link}
| All DIAKIs | DIAKIs Recorded in FPVDB | DIAKIs Not Recorded in FPVDB | ||
|---|---|---|---|---|
| n = 468 | n = 67 | n = 401 | p Value | |
| Age, years [mean ± SD] | 75.4 ± 13.9 | 68.9 ± 13.8 | 76.5 ± 13.6 | <0.001 a |
| Length of stay, days [median (IQR)] | 13 (8–22) | 21 (10.5–29.0) | 12 (7–20) | <0.001 b |
| Male [n (%)] | 288 (61.5) | 48 (68.7) | 240 (59.9) | 0.066 c |
| Chronic kidney disease [n (%)] | 106 (22.6) | 17 (25.4) | 89 (22.2) | 0.565 c |
| Acute heart failure [n (%)] | 142 (30.3) | 12 (17.9) | 130 (32.4) | 0.017 c |
| Diabetes mellitus [n (%)] | 127 (27.1) | 17 (25.4) | 110 (27.4) | 0.726 c |
| Sepsis [n (%)] | 98 (20.9) | 21 (31.3) | 77 (19.2) | 0.024 c |
| Number of drug(s) involved [n (%)] | 0.037 c | |||
| 1 drug | 291 (62.2) | 34 (50.7) | 257 (64.1) | |
| 2 drugs or more | 177 (37.8) | 33 (49.3) | 144 (35.9) | |
| KDIGO stage [n (%)] | <0.001 c | |||
| Stage 1 | 235 (50.2) | 15 (22.4) | 220 (54.9) | |
| Stage 2 | 95 (20.3) | 11 (16.4) | 84 (20.9) | |
| Stage 3 | 138 (29.5) | 41 (61.2) | 97 (24.2) | |
| Death during stay [n (%)] | 52 (11.1) | 6 (9.0) | 46 (11.5) | 0.544 c |
| Intensive care unit hospitalization [n (%)] | 107 (22.9) | 27 (40.3) | 80 (20.0) | <0.001 c |
| Extra-renal replacement therapy [n (%)] | 45 (9.6) | 21 (31.3) | 24 (6.0) | <0.001 c |
| ATC Classes | Active Substances | DIAKIs in PSMSI Database n = 460 | DIAKIs in FPVDB n = 67 | Total DIAKIs n = 468 a | Notification Rate b | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | % | ||
| C03 | Diuretic drugs | 190 | 41.3 | 11 | 16.4 | 192 | 41.0 | 5.7 |
| C03CA01 | furosemide | 167 | 36.3 | 6 | 9.0 | 168 | 35.9 | 3.6 |
| C03AA03 | hydrochlorothiazide | 17 | 3.7 | 3 | 4.5 | 18 | 3.8 | 16.7 |
| C03DA01 | spironolactone | 15 | 3.3 | 2 | 3.0 | 16 | 3.4 | 12.5 |
| C09 | Agents acting on the renin-angiotensin system | 145 | 31.5 | 15 | 22.4 | 146 | 31.2 | 10.3 |
| C09AA05 | ramipril | 37 | 8.0 | 5 | 7.5 | 37 | 7.9 | 13.5 |
| C09AA04 | perindopril | 23 | 5.0 | 1 | 1.5 | 23 | 4.9 | 4.3 |
| C09CA04 | irbesartan | 16 | 3.5 | 3 | 4.5 | 17 | 3.6 | 17.6 |
| C09CA03 | valsartan | 14 | 3.0 | 1 | 1.5 | 14 | 3.0 | 7.1 |
| C09CA06 | candesartan | 9 | 2.0 | 2 | 3.0 | 9 | 1.9 | - |
| J01 | Antibacterial drugs | 81 | 17.6 | 25 | 37.3 | 84 | 17.9 | 29.8 |
| J01CA04 | amoxicillin | 21 | 4.6 | 8 | 11.9 | 21 | 4.5 | 38.1 |
| J01GB03 | gentamicin | 18 | 3.9 | 2 | 3.0 | 18 | 3.8 | 11.1 |
| J01XA01 | vancomycin | 18 | 3.9 | 2 | 3.0 | 18 | 3.8 | 11.1 |
| J01EE01 | sulfamethoxazole/trimethoprim | 14 | 3.0 | 7 | 10.4 | 14 | 3.0 | 50.0 |
| J01GB06 | amikacin | 8 | 1.7 | 1 | 1.5 | 8 | 1.7 | - |
| V08 | Contrast media | 79 | 17.2 | 8 | 11.9 | 79 | 16.9 | 10.1 |
| V08AB11 | iobitridol | 52 | 11.3 | 6 | 9.0 | 52 | 11.1 | 11.5 |
| V08AB09 | iodixanol | 27 | 5.9 | 1 | 1.5 | 27 | 5.8 | 3.7 |
| L01 | Antineoplastic drugs | 21 | 4.6 | 7 | 10.4 | 23 | 4.9 | 30.4 |
| L01XA02 | carboplatin | 6 | 1.3 | 1 | 1.5 | 6 | 1.3 | - |
| L01CB01 | etoposide | 5 | 1.1 | 1 | 1.5 | 6 | 1.3 | - |
| L01AA01 | cyclophosphamide | 4 | 0.9 | 1 | 1.5 | 5 | 0.9 | - |
| L01XA01 | cisplatin | 4 | 0.9 | 1 | 1.5 | 4 | 0.9 | - |
| L01BA01 | methotrexate | 4 | 0.9 | 0 | 0.0 | 4 | 0.9 | - |
| M01 | Anti-inflammatory and antirheumatic drugs | 19 | 4.1 | 4 | 6.0 | 19 | 4.1 | 21.1 |
| M01AE03 | ketoprofen | 7 | 1.5 | 1 | 1.5 | 7 | 1.5 | - |
| M01AE13 | ibuprofen | 3 | 0.7 | 1 | 1.5 | 3 | 0.6 | - |
| L04 | Immunosuppressant drugs | 16 | 3.5 | 2 | 3.0 | 17 | 3.6 | 11.7 |
| L04AD02 | tacrolimus | 9 | 2.0 | 0 | 0.0 | 9 | 1.9 | - |
| L04AD01 | cyclosporine | 5 | 1.0 | 0 | 0 | 5 | 1.1 | - |
| L04AX04 | lenalidomide | 1 | 0.2 | 0 | 0.0 | 1 | 0.2 | - |
| J05 | Antiviral drugs | 14 | 3.0 | 7 | 10.4 | 15 | 3.2 | 46.7 |
| J05AB01 | acyclovir | 8 | 1.7 | 4 | 6.0 | 8 | 1.7 | - |
| J05AB11 | valaciclovir | 3 | 0.7 | 1 | 1.5 | 3 | 0.6 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rolland, A.-L.; Garnier, A.-S.; Meunier, K.; Drablier, G.; Briet, M. Drug-Induced Acute Kidney Injury: A Study from the French Medical Administrative and the French National Pharmacovigilance Databases Using Capture-Recapture Method. J. Clin. Med. 2021, 10, 168. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020168
Rolland A-L, Garnier A-S, Meunier K, Drablier G, Briet M. Drug-Induced Acute Kidney Injury: A Study from the French Medical Administrative and the French National Pharmacovigilance Databases Using Capture-Recapture Method. Journal of Clinical Medicine. 2021; 10(2):168. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020168
Chicago/Turabian StyleRolland, Anne-Lise, Anne-Sophie Garnier, Katy Meunier, Guillaume Drablier, and Marie Briet. 2021. "Drug-Induced Acute Kidney Injury: A Study from the French Medical Administrative and the French National Pharmacovigilance Databases Using Capture-Recapture Method" Journal of Clinical Medicine 10, no. 2: 168. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020168