
Operative and Clinical Outcomes of Minimally Invasive Living-Donor Surgery on Uterus Transplantation: A Literature Review


Abstract
:1. Introduction
2. Materials and Methods
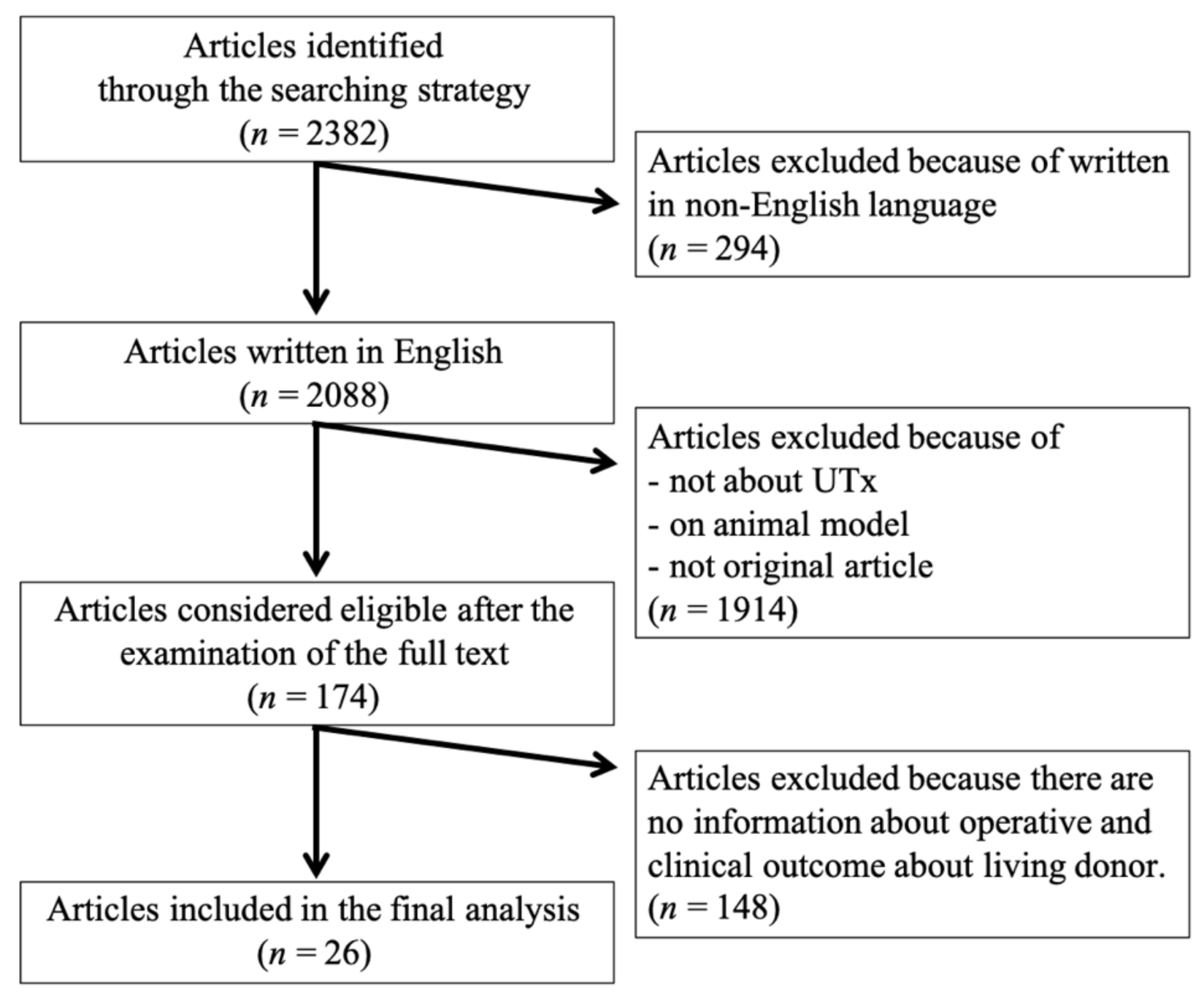
2.1. Search Strategy
2.2. Eligibility Assessment
2.3. Data Extraction and Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Herlin, M.; Petersen, M.B.; Brännström, M. Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome: A comprehensive update. Orphanet J. Rare Dis. 2020, 15, 1–16. [Google Scholar] [CrossRef]
- Hur, C.; Rehmer, J.; Flyckt, R.; Falcone, T. Uterine Factor Infertility: A Clinical Review. Clin. Obstet. Gynecol. 2019, 62, 257–270. [Google Scholar] [CrossRef]
- Fageeh, W.; Raffa, H.; Jabbad, H.; Marzouki, A. Transplantation of the human uterus. Int. J. Gynecol. Obstet. 2002, 76, 245–251. [Google Scholar] [CrossRef]
- Brannstrom, M.; Johannesson, L.; Bokstrom, H.; Kvarnstrom, N.; Molne, J.; Dahm-Kahler, P.; Enskog, A.; Milenkovic, M.; Ekberg, J.; Diaz-Garcia, C.; et al. Livebirth after uterus transplantation. Lancet 2015, 385, 607–616. [Google Scholar] [CrossRef] [Green Version]
- Daolio, J.; Palomba, S.; Paganelli, S.; Falbo, A.; Aguzzoli, L. Uterine transplantation and IVF for congenital or acquired uterine factor infertility: A systematic review of safety and efficacy outcomes in the first 52 recipients. PLoS ONE 2020, 15, e0232323. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M.; Johannesson, L.; Dahm-Kähler, P.; Enskog, A.; Mölne, J.; Kvarnström, N.; Diaz-Garcia, C.; Hanafy, A.; Lundmark, C.; Marcickiewicz, J.; et al. First clinical uterus transplantation trial: A six-month report. Fertil. Steril. 2014, 101, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Chmel, R.; Novackova, M.; Janousek, L.; Matecha, J.; Pastor, Z.; Maluskova, J.; Cekal, M.; Kristek, J.; Olausson, M.; Fronek, J. Revaluation and lessons learned from the first 9 cases of a Czech uterus transplantation trial: Four deceased donor and 5 living donor uterus transplantations. Am. J. Transplant. 2019, 19, 855–864. [Google Scholar] [CrossRef] [PubMed]
- Testa, G.; McKenna, G.J.; Gunby, R.T.; Anthony, T.; Koon, E.C.; Warren, A.M.; Putman, J.M.; Zhang, L.; DePrisco, G.; Mitchell, J.M.; et al. First live birth after uterus transplantation in the United States. Am. J. Transplant. 2018, 18, 1270–1274. [Google Scholar] [CrossRef] [Green Version]
- Puntambekar, S.; Telang, M.; Kulkarni, P.; Puntambekar, S.; Jadhav, S.; Panse, M.; Sathe, R.; Agarkhedkar, N.; Warty, N.; Kade, S.; et al. Laparoscopic-Assisted Uterus Retrieval from Live Organ Donors for Uterine Transplant: Our Experience of Two Patients. J. Minim. Invasive Gynecol. 2018, 25, 622–631. [Google Scholar] [CrossRef]
- Wei, L.; Xue, T.; Tao, K.-S.; Zhang, G.; Zhao, G.-Y.; Guang-Yue, Z.; Cheng, L.; Yang, Z.-X.; Zheng, M.-J.; Bi-Liang, C.; et al. Modified human uterus transplantation using ovarian veins for venous drainage: The first report of surgically successful robotic-assisted uterus procurement and follow-up for 12 months. Fertil. Steril. 2017, 108, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Järvholm, S.; Johannesson, L.; Clarke, A.; Brännström, M. Uterus transplantation trial: Psychological evaluation of recipients and partners during the post-transplantation year. Fertil. Steril. 2015, 104, 1010–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brännström, M.; Bokström, H.; Dahm-Kähler, P.; Díaz-García, C.; Ekberg, J.; Enskog, A.; Hagberg, H.; Johannesson, L.; Kvarnström, N.; Mölne, J.; et al. One uterus bridging three generations: First live birth after mother-to-daughter uterus transplantation. Fertil. Steril. 2016, 106, 261–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mölne, J.; Broecker, V.; Ekberg, J.; Nilsson, O.; Dahm-Kähler, P.; Brännström, M. Monitoring of Human Uterus Transplantation with Cervical Biopsies: A Provisional Scoring System for Rejection. Am. J. Transplant. 2017, 17, 1628–1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvarnstrom, N.; Jarvholm, S.; Johannesson, L.; Dahm-Kahler, P.; Olausson, M.; Brannstrom, M. Live Donors of the Initial Obser-vational Study of Uterus Transplantation-Psychological and Medical Follow-Up Until 1 Year After Surgery in the 9 Cases. Transplantation 2017, 101, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Brännström, M.; Dahm-Kähler, P.; Kvarnström, N.; Akouri, R.; Rova, K.; Olausson, M.; Groth, K.; Ekberg, J.; Enskog, A.; Sheikhi, M.; et al. Live birth after robotic-assisted live donor uterus transplantation. Acta Obstet. Gynecol. Scand. 2020, 99, 1222–1229. [Google Scholar] [CrossRef] [Green Version]
- Brännström, M.; Dahm-Kähler, P.; Ekberg, J.; Akouri, R.; Groth, K.; Enskog, A.; Broecker, V.; Mölne, J.; Ayoubi, J.M.; Kvarnström, N. Outcome of Recipient Surgery and 6-Month Follow-Up of the Swedish Live Donor Robotic Uterus Transplantation Trial. J. Clin. Med. 2020, 9, 2338. [Google Scholar] [CrossRef]
- Järvholm, S.; Dahm-Kähler, P.; Kvarnström, N.; Brännström, M. Psychosocial outcomes of uterine transplant recipients and partners up to 3 years after transplantation: Results from the Swedish trial. Fertil. Steril. 2020, 114, 407–415. [Google Scholar] [CrossRef]
- Brännström, M.; Kvarnström, N.; Groth, K.; Akouri, R.; Wiman, L.; Enskog, A.; Dahm-Kähler, P. Evolution of surgical steps in robotics-assisted donor surgery for uterus transplantation: Results of the eight cases in the Swedish trial. Fertil. Steril. 2020, 114, 1097–1107. [Google Scholar] [CrossRef]
- Broecker, V.; Brännström, M.; Ekberg, J.; Dahm-Kähler, P.; Mölne, J. Uterus transplantation: Histological findings in explants at elective hysterectomy. Am. J. Transplant. 2020. [Google Scholar] [CrossRef]
- Huang, Y.; Ding, X.; Chen, B.; Zhang, G.; Li, A.; Hua, W.; Zhou, D.; Wang, X.; Liu, D.; Yan, G.; et al. Report of the first live birth after uterus transplantation in People’s Republic of China. Fertil. Steril. 2020, 114, 1108–1115. [Google Scholar] [CrossRef]
- Testa, G.; Koon, E.C.; Johannesson, L.; McKenna, G.J.; Anthony, T.; Klintmalm, G.B.; Gunby, R.T.; Warren, A.M.; Putman, J.M.; DePrisco, G.; et al. Living Donor Uterus Transplantation: A Single Center’s Observations and Lessons Learned from Early Setbacks to Technical Success. Am. J. Transplant. 2017, 17, 2901–2910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramani, A.; Testa, G.; Ghouri, Y.; Koon, E.C.; Di Salvo, M.; McKenna, G.J.; Bayer, J.; Warren, A.M.; Wall, A.; Johannesson, L. DUETS (Dallas UtErus Transplant Study): Complete report of 6-month and initial 2-year outcomes following open donor hysterectomy. Clin. Transplant. 2020, 34, e13757. [Google Scholar] [CrossRef] [PubMed]
- Johannesson, L.; Koon, E.C.; Bayer, J.; McKenna, G.J.; Wall, A.; Fernandez, H.; Martinez, E.J.; Gupta, A.; Ruiz, R.; Onaca, N.; et al. DUETS (Dallas UtErus Transplant Study): Early Outcomes and Complications of Robot-Assisted Hysterectomy for Living Uterus Donors. Transplantation 2021, 105, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Testa, G.; McKenna, G.J.; Bayer, J.; Wall, A.; Fernandez, H.; Martinez, E.; Gupta, A.; Ruiz, R.; Onaca, N.; Gunby, R.T.; et al. The Evolution of Transplantation from Saving Lives to Fertility Treatment: DUETS (Dallas UtErus Transplant Study). Ann. Surg. 2020, 272, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Chmel, R.; Cekal, M.; Pastor, Z.; Chmel, R., Jr.; Paulasova, P.; Havlovicova, M.; Macek, M., Jr.; Novackova, M. Assisted Reproductive Techniques and Preg-nancy Results in Women with Mayer-Rokitansky-Kuster-Hauser Syndrome Undergoing Uterus Transplantation: The Czech Experience. J. Pediatr. Adolesc. Gynecol. 2020, 33, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Chmel, R.; Novackova, M.; Pastor, Z. Lessons learned from the Czech uterus transplant trial related to surgical technique that may affect reproductive success. Aust. New Zealand J. Obstet. Gynaecol. 2020, 60, 625–627. [Google Scholar] [CrossRef] [PubMed]
- Brucker, S.Y.; Brannstrom, M.; Taran, F.A.; Nadalin, S.; Konigsrainer, A.; Rall, K.; Schöller, D.; Henes, M.; Bösmüller, H.; Fend, F.; et al. Selecting living donors for uterus trans-plantation: Lessons learned from two transplantations resulting in menstrual functionality and another attempt, aborted after organ retrieval. Arch Gynecol Obstet. 2018, 297, 675–684. [Google Scholar] [CrossRef]
- Brucker, S.Y.; Strowitzki, T.; Taran, F.-A.; Rall, K.; Schöller, D.; Hoopmann, M.; Henes, M.; Guthoff, M.; Heyne, N.; Zipfel, S.; et al. Living-Donor Uterus Transplantation: Pre-, Intra-, and Postoperative Parameters Relevant to Surgical Success, Pregnancy, and Obstetrics with Live Births. J. Clin. Med. 2020, 9, 2485. [Google Scholar] [CrossRef]
- Puntambekar, S.; Puntambekar, S.; Telang, M.; Kulkarni, P.; Date, S.; Panse, M.; Sathe, R.; Agarkhedkar, N.; Warty, N.; Kade, S.; et al. Novel Anastomotic Technique for Uterine Transplant Using Utero-ovarian Veins for Venous Drainage and Internal Iliac Arteries for Perfusion in Two Laparoscopically Harvested Uteri. J. Minim. Invasive Gynecol. 2019, 26, 628–635. [Google Scholar] [CrossRef]
- Tamauchi, S.; Kajiyama, H.; Sakata, J.; Sekiya, R.; Suzuki, S.; Mizuno, M.; Utsumi, F.; Niimi, K.; Kotani, T.; Shibata, K.; et al. Oncologic and obstetric outcomes of early stage cervical cancer with abdominal radical trachelectomy: Single-institution experience. J. Obstet. Gynaecol. Res. 2016, 42, 1796–1801. [Google Scholar] [CrossRef] [Green Version]
- Allyse, M.; Amer, H.; Coutifaris, C.; Falcone, T.; Famuyide, A.; Flyckt, R.; Gargiulo, A.; Heimbach, J.; Johannesson, L.; Jowsey-Gregoire, S.; et al. American Society for Reproductive Medicine position statement on uterus transplantation: A committee opinion. Fertil Steril. 2018, 110, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantitamit, T.; Huang, K.G.; Lee, C.L. Laparoscopic versus open radical hysterectomy in women with early stage cervical cancer: A systematic review and meta-analysis. Taiwan J. Obstet. Gynecol. 2020, 59, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Giacomoni, A.; Di Sandro, S.; Lauterio, A.; Concone, G.; Buscemi, V.; Rossetti, O.; De Carlis, L. Robotic nephrectomy for living donation: Surgical technique and literature systematic review. Am. J. Surg. 2016, 211, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Ejzenberg, D.; Andraus, W.; Baratelli Carelli Mendes, L.R.; Ducatti, L.; Song, A.; Tanigawa, R.; Rocha-Santos, V.; Macedo Arantes, R.; Soares, J.M., Jr.; Serafini, P.C.; et al. Livebirth after uterus trans-plantation from a deceased donor in a recipient with uterine infertility. Lancet 2019, 392, 2697–2704. [Google Scholar] [CrossRef]
- Flyckt, R.; Falcone, T.; Quintini, C.; Perni, U.; Eghtesad, B.; Richards, E.G.; Farrell, R.M.; Hashimoto, K.; Miller, C.; Ricci, S.; et al. First birth from a deceased donor uterus in the United States: From severe graft rejection to successful cesarean delivery. Am. J. Obstet. Gynecol. 2020, 223, 143–151. [Google Scholar] [CrossRef]
- Kisu, I.; Umene, K.; Adachi, M.; Emoto, K.; Nogami, Y.; Banno, K.; Itagaki, I.; Kawamoto, I.; Nakagawa, T.; Narita, H.; et al. Allowable warm ischemic time and morphological and bi-ochemical changes in uterine ischemia/reperfusion injury in cynomolgus macaque: A basic study for uterus transplantation. Hum. Reprod. 2017, 32, 2026–2035. [Google Scholar] [CrossRef] [Green Version]
- Zaami, S.; Di Luca, A.; Marinelli, E. Advancements in uterus transplant: New scenarios and future implications. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 892–902. [Google Scholar]
- Kisu, I.; Liu, Y.; Chen, G.; Song, M.J.; Chang, C.Y.-Y.; Koon, T.H.; Banno, K.; Aoki, D. Current Progress in Uterus Transplantation Research in Asia. J. Clin. Med. 2019, 8, 245. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Country | Operation | No. | Surgical Time (h:min) | Blood Loss (mL) | Preserved Vein | Graft Failure | Operative Complications (Grade *) | Discharge | Live Birth | Remarks |
|---|---|---|---|---|---|---|---|---|---|---|
| Saudi Arabia [3] | OPEN | 1 | N/R | N/R | 2 × UV | Yes | Intraoperative ureteric injury (N/R) | N/R | N/A | |
| Sweden [4,6,11,12,13,14,15,16,17,18,19] | OPEN | 1 | 10:54 | 300 | 2 × UV, 1 × UOV | No | Nocturia (1) | 6POD | Yes × 2 | |
| OPEN | 2 | 12:37 | 2400 | 2 × UV, 1 × UOV | Yes | Wound infection (2) Uterovaginal fistula (3b) | 6POD | N/A | ||
| OPEN | 3 | 12:53 | 800 | 2 × UV, 1 × UOV | No | None | 6POD | no | ||
| OPEN | 4 | 10:34 | 600 | 2 × UV, 1 × UOV | No | Unilateral sensibility impairment of the thigh (1) | 6POD | Yes × 2 | ||
| OPEN | 5 | 10:17 | 600 | 2 × UV | No | None | 6POD | Yes × 1 | ||
| OPEN | 6 | 10:52 | 700 | 2 × UV, 1 × UOV | No | None | 6POD | Yes × 2 | ||
| OPEN | 7 | 10:17 | 400 | 2 × UV, 1 × UOV | No | None | 6POD | Yes × 1 | ||
| OPEN | 8 | 11:23 | 400 | 2 × UV | No | None | 6POD | Yes × 1 | ||
| OPEN | 9 | 13:08 | 2100 | 2 × UV | Yes | None | 6POD | N/A | ||
| ROBOT | 1 | 13:00 | 600 | 2 × UV, 1 × UOV | No | None | N/R | N/R | ||
| ROBOT | 2 | 12:30 | 400 | 2 × UV, 1 × UOV | No | Gluteal light pain when walking (N/R) | 5POD | Yes | ||
| ROBOT | 3 | 11:30 | N/R | 2 × UV, 2 × UOV | Yes | N/R | N/R | N/A | ||
| ROBOT | 4 | 12:30 | N/R | 2 × UV, 1 × UOV | No | Pressure alopecia (2) | N/R | N/R | ||
| ROBOT | 5 | 11:30 | N/R | 2 × UV, 2 × UOV | No | N/R | N/R | N/R | ||
| ROBOT | 6 | 11:30 | N/R | 2 × UV, 2 × UOV | No | N/R | N/R | N/R | ||
| ROBOT | 7 | 11:30 | N/R | 2 × UV, 2 × UOV | No | N/R | N/R | N/R | ||
| ROBOT | 8 | 10:00 | N/R | 2 × UV, 1 × UOV | Yes | Pyelonephritis (3b) | N/R | N/A | ||
| China [10,20] | ROBOT | 1 | 6:00 | 100 | 2 × OV | No | None | 5POD | Yes | |
| US (Dallas) [8,21,22,23,24] | OPEN | 1 | 5:45 | 400 | 1 × UV, 1 × UOV | Yes | Leg/buttocks pain (1) | 6POD | N/A | |
| OPEN | 2 | 7:21 | 1000 | 1 × UV, 1 × UOV | Yes | UTI (2) | 6POD | N/A | ||
| OPEN | 3 | 6:41 | 1300 | 1 × UV, 1 × UOV | Yes | Vaginal cuff dehiscence (3b) Depression (2), UTI (2) | 6POD | N/A | ||
| OPEN | 4 | 6:40 | 1700 | 2 × UOV | No | UTI (2) | 5POD | Yes | ||
| OPEN | 5 | 6:34 | 250 | 2 × UOV | No | Faecal impaction (3b) | 7POD | Yes | ||
| OPEN | 6 | 7:07 | 1100 | 1 × UV, 1 × UOV | No | Acute blood loss anaemia (2) | 5POD | Yes | ||
| OPEN | 7 | 6:38 | 600 | 2 × UV | No | UTI (2) | 5POD | Yes | ||
| OPEN | 8 | 6:12 | 400 | 2 × UOV | Yes | None | 6POD | N/A | ||
| OPEN | 9 | 7:34 | 750 | 1 × UV, 1 × UOV | No | Symptomatic anaemia (2), UTI (2) | 5POD | Yes | ||
| OPEN | 10 | 6:27 | 1500 | 2 × UV | No | Acute blood loss anaemia (4a) Prolonged intubation (4a), UTI (2) | 8POD | N/R | ||
| OPEN | 11 | 5:33 | 600 | 2 × UOV | No | None | 5POD | Yes | ||
| OPEN | 12 | 5:13 | 950 | 1 × UV, 2 × UOV | Yes | Haemorrhage (N/R) | 4POD | N/A | ||
| OPEN | 13 | 6:10 | 800 | 1 × UV, 1 × UOV | No | UTI (2) | 6POD | Yes | Not anastomosed UV | |
| ROBOT | 1 | 9:25 | 150 | 1 × UV, 2 × UOV | No | Temporary alopecia (1) | 4POD | N/R | Not anastomosed UV | |
| ROBOT | 2 | 10:48 | 100 | 1 × UV, 2 × UOV | N/R | Ureteral blood clot (3b) | 6POD | N/R | ||
| ROBOT | 3 | 12:10 | 200 | 1 × UV, 2 × UOV | N/R | Bilateral ureteral injury (3b) | 3POD | N/R | Not anastomosed UV | |
| ROBOT | 4 | 9:27 | 20 | 2 × UV, 2 × UOV | N/R | None | 4POD | N/R | There were 2 left UOV | |
| ROBOT | 5 | 12:03 | 100 | 3 × UOV | N/R | None | 3POD | N/R | ||
| Czech [7,25,26] | OPEN | 1 | 5:20 | 100 | 2 × UV, 2 × OV | No | None | 7POD | N/R | Not anastomosed UV |
| OPEN | 2 | 6:10 | 800 | 2 × UV, 2 × OV | No | None | 7POD | N/R | Not anastomosed UV | |
| OPEN | 3 | 7:10 | 100 | 2 × UV, 2 × OV | No | Climacteric symptoms (N/R) | 6POD | N/R | Not anastomosed UV | |
| OPEN | 4 | 5:30 | 100 | 2 × UV, 2 × OV | Yes | Bladder hypotonia (3a) | 11POD | N/A | Not anastomosed OV | |
| OPEN | 5 | 5:30 | 1000 | 2×UV, 2×OV | No | Ureter laceration (3a) Climacteric symptoms (N/R) | 9POD | Yes | ||
| Germany [27,28] | OPEN | 1 | 12:07 | 100 | 2 × UV | No | None | 11 days † | Yes | |
| OPEN | 2 | 13:06 | N/R | UV ‡ | N/A | Hydronephrosis (3b) | N/R | N/A | No transplantation performed | |
| OPEN | 3 | 9:03 | 100 | 1 × UV, 1 × OV | No | None | 12 days† | Yes | ||
| OPEN | 4 | 10:24 | 100 | 2 × UV, 1 × UOV | No | None | 14 days † | N/A | ||
| OPEN | 5 | 9:11 | 100 | 2 × UV, 2 × UOV | No | None | 14 days † | N/A | ||
| India [9,29] | LAP | 1 | 4:00 | 100 | 1 × or 2 × UV, 2 × OV § | No | None | 7POD | N/R | |
| LAP | 2 | 4:00 | 100 | 1 × or 2 × UV, 2 × OV § | No | None | 7POD | N/R | ||
| LAP | 3 | 2:40 | 100 | 2 × OV | No | None | 6POD | N/R | ||
| LAP | 4 | 3:20 | 100 | 2 × OV | No | None | 6POD | N/R |
| OPEN | LAP | ROBOT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| UV (+) | UV (−) | Total | UV (+) | UV (−) | Total | UV (+) | UV (−) | Total | |
| n | 29 | 4 | 33 | 2 | 2 | 4 | 12 | 2 | 14 |
| Surgical time (h:min) * | 8:45 ± 2:39 | 6:14 ± 0.26 | 8:26 ± 2:47 | 4:00 ± 0:00 | 3:00 ± 0.20 | 3:30 ± 0.33 | 11:19 ± 1:08 | 9:01 ± 3:01 | 10:59 ± 1:45 |
| Blood loss (mL) * | 711 ± 586 | 738 ± 569 | 715 ± 584 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 245 ± 197 | 100 ± 0 | 209 ± 182 |
| Discharge (POD) | 6.3 ± 1.4 | 5.8 ± 0.8 | 6.2 ± 1.3 | 7.0 ± 0.0 | 6.0 ± 0.0 | 6.5 ± 0.5 | 4.4 ± 1.0 | 4.0 ± 0.0 | 4.3 ± 1.0 |
| Complications (n,%) | 17 (58.6%) | 2 (50.0%) | 19 (57.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 6 (50.0%) | 0 (0.0%) | 6 (42.9%) |
| Graft failure (n,%) | 8 (28.6%) † | 1 (25.0%) | 9 (28.1%) † | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (16.7%) | 0 (0.0%) | 2 (14.3%) |
| Live birth (n,%) | 13 (46.4%) | 3 (75.0%) | 16 (48.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (8.3%) | 1 (50.0%) | 2 (14.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matoba, Y.; Kisu, I.; Banno, K.; Aoki, D. Operative and Clinical Outcomes of Minimally Invasive Living-Donor Surgery on Uterus Transplantation: A Literature Review. J. Clin. Med. 2021, 10, 349. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020349
Matoba Y, Kisu I, Banno K, Aoki D. Operative and Clinical Outcomes of Minimally Invasive Living-Donor Surgery on Uterus Transplantation: A Literature Review. Journal of Clinical Medicine. 2021; 10(2):349. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020349
Chicago/Turabian StyleMatoba, Yusuke, Iori Kisu, Kouji Banno, and Daisuke Aoki. 2021. "Operative and Clinical Outcomes of Minimally Invasive Living-Donor Surgery on Uterus Transplantation: A Literature Review" Journal of Clinical Medicine 10, no. 2: 349. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020349