Intercostal Catheters for Postoperative Pain Management in VATS Reduce Opioid Consumption

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patient Selection
2.2. Data Collection
2.3. Definitions
2.3.1. Study Endpoints
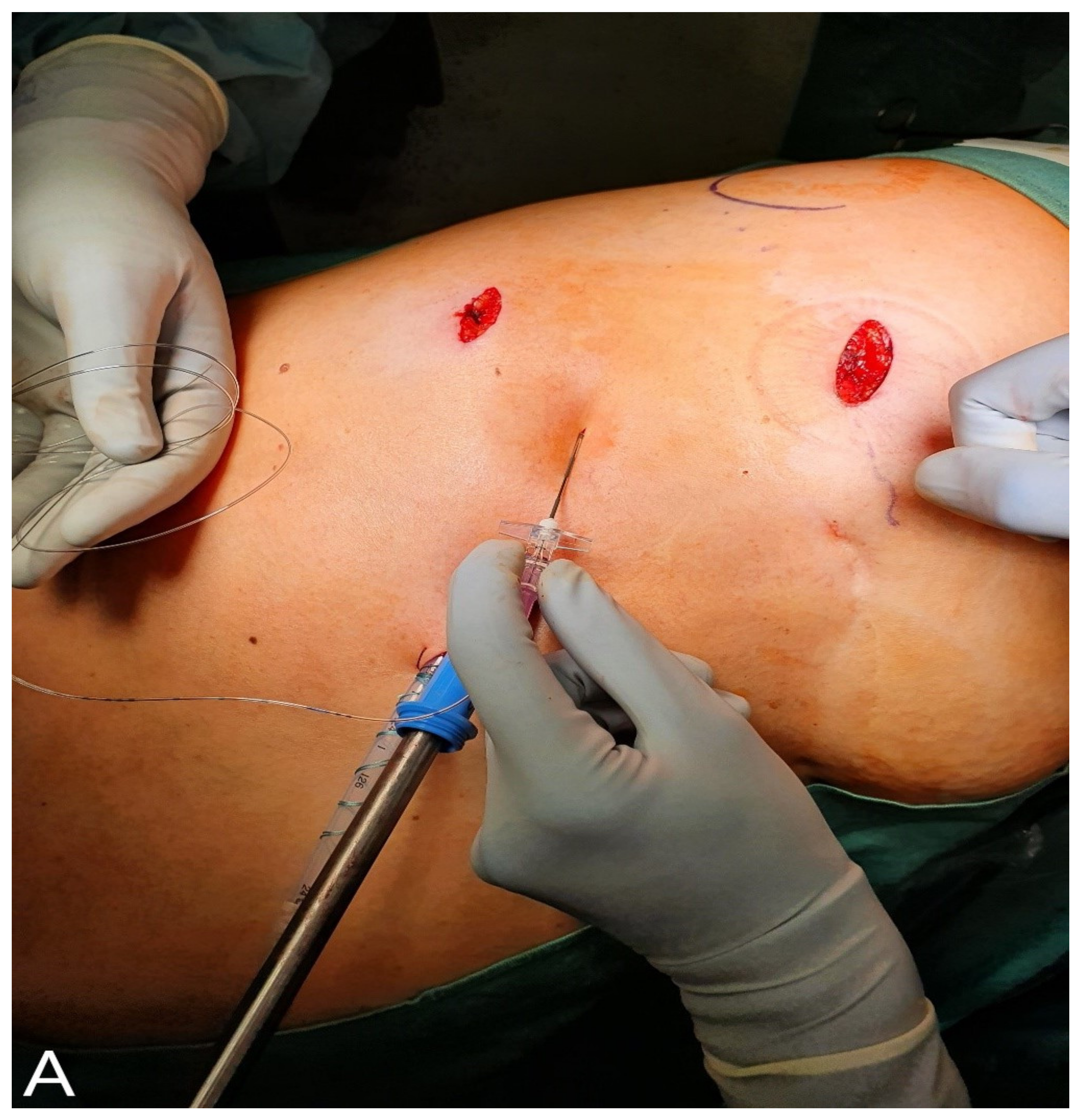
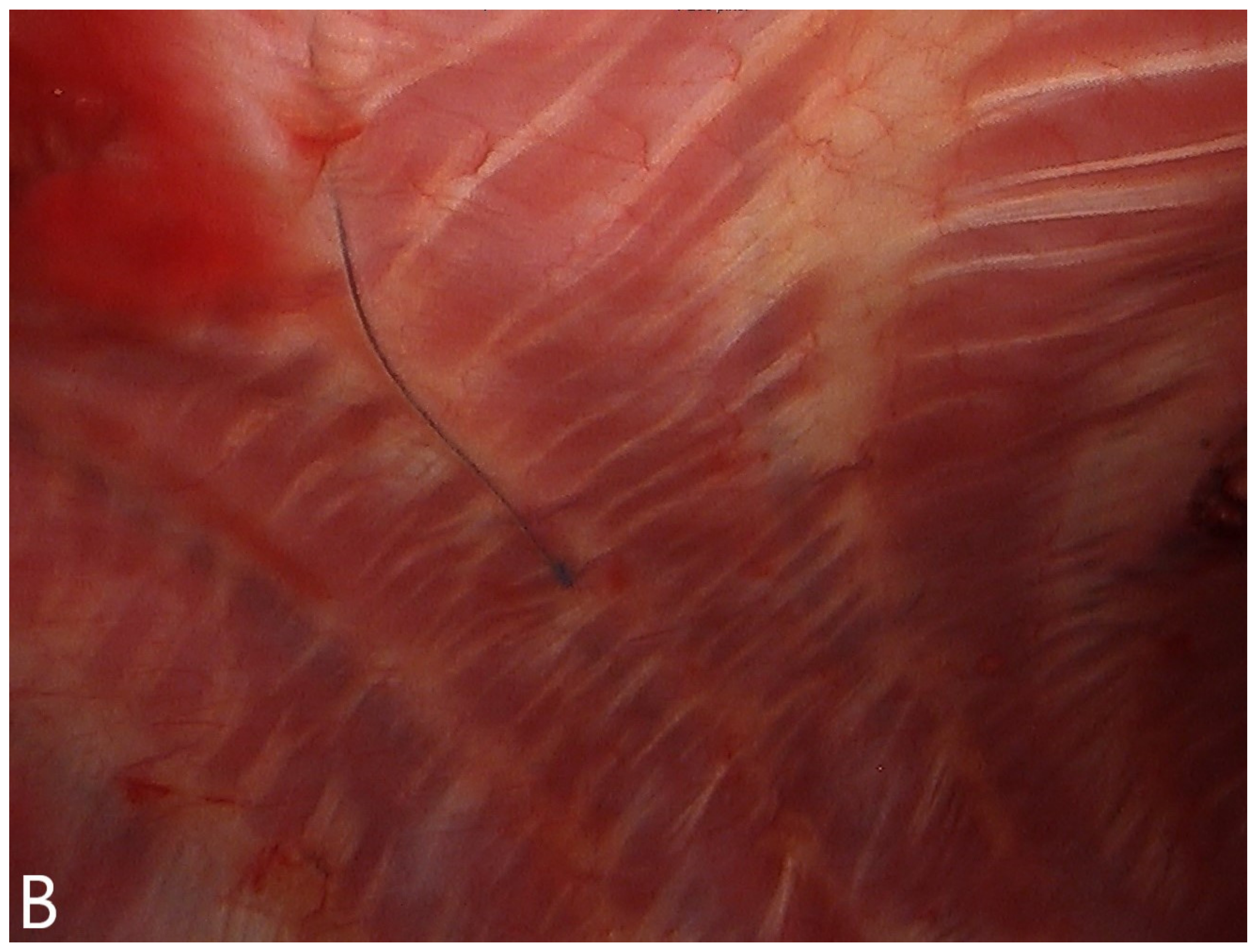
2.3.2. Surgical Technique
2.3.3. Analgesic Technique
2.3.4. Pain Scoring
2.3.5. Postoperative Complications
2.3.6. Statistical Analysis
3. Results
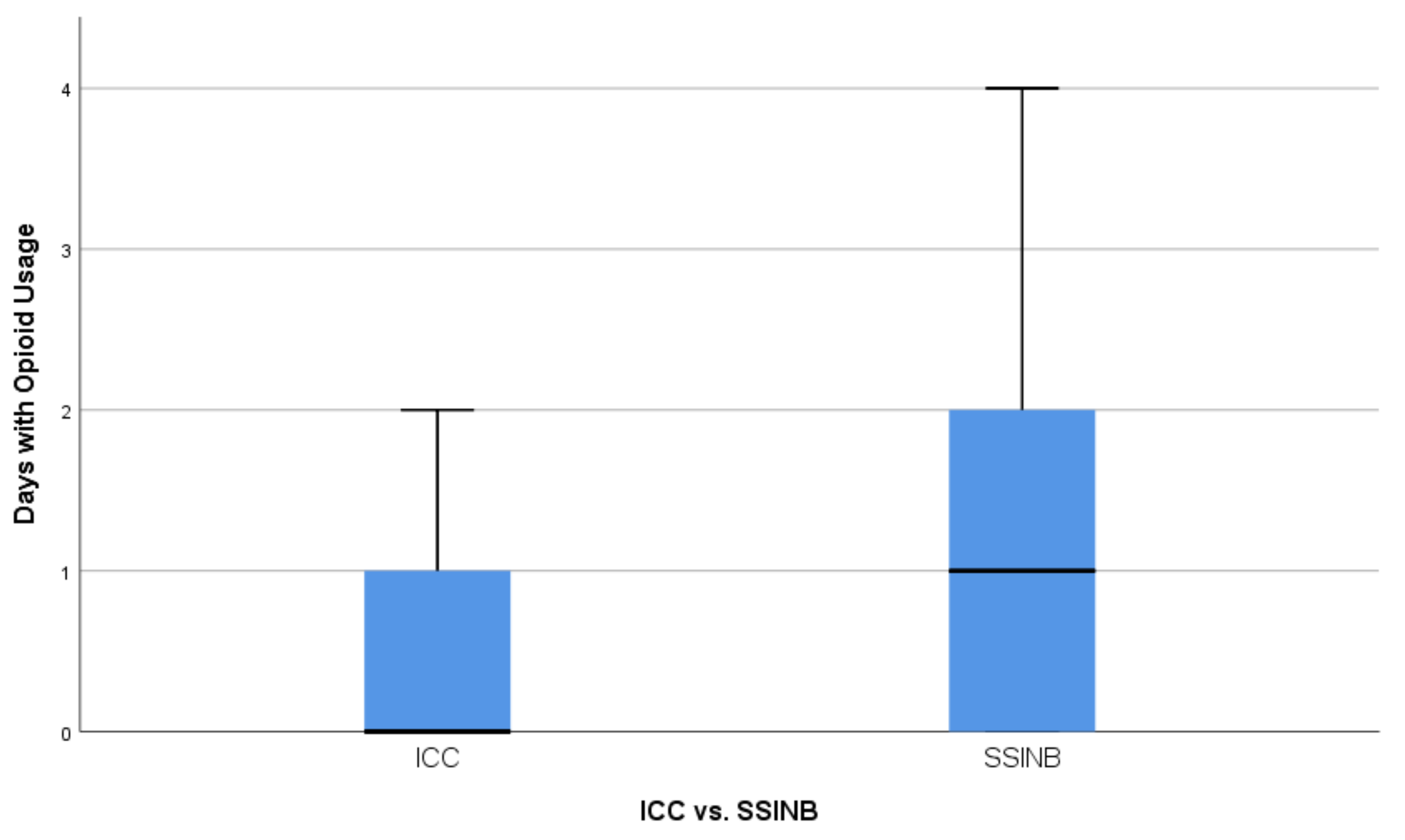
Opioid Usage
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goto, T. What is the best pain control after thoracic surgery? J. Thorac. Dis. 2018, 10, 1335–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercieri, M.; D’Andrilli, A.; Arcioni, R. Improving postoperative pain management after video-assisted thoracic surgery lung resection contributes to enhanced recovery, but guidelines are still lacking. J. Thorac. Dis. 2018, 10 (Suppl. 9), 983–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmore, B.; Nguyen, V.; Blank, R.; Yount, K.; Lau, C. Pain management following thoracic surgery. Thorac. Surg. Clin. 2015, 25, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Steinthorsdottir, K.J.; Wildgaard, L.; Hansen, H.J.; Petersen, R.H.; Wildgaard, K. Regional analgesia for video-assisted thoracic surgery: A systematic review. Eur. J. Cardiothorac. Surg. 2014, 45, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansdottir, V.; Philip, J.; Olsen, M.F.; Eduard, C.; Houltz, E.; Ricksten, S. Thoracic epidural versus intravenous patient-controlled analgesia after cardiac surgery: A randomized controlled trial on length of hospital stay and patient-perceived quality of recovery. Anesthesiology 2006, 104, 142–151. [Google Scholar] [CrossRef]
- Hewson, D.W.; Bedforth, N.M.; Hardman, J.G. Spinal cord injury arising in anaesthesia practice. Anaesthesia 2018, 73 (Suppl. 1), 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferré, F.; Martin, C.; Bosch, L.; Kurrek, M.; Lairez, O.; Minville, V. Control of spinal anesthesia-induced hypotension in adults. Local Reg. Anesth. 2020, 13, 39–46. [Google Scholar]
- Gleicher, Y.; Singer, O.; Choi, S.; McHardy, P. Thoracic epidural catheter placement in a preoperative block area improves operating room efficiency and decreases epidural failure rate. Reg. Anesth. Pain Med. 2017, 42, 649–651. [Google Scholar] [CrossRef]
- McLeod, G.; Davies, H.; Munnoch, N.; Bannister, J.; MacRae, W. Postoperative pain relief using thoracic epidural analgesia: Outstanding success and disappointing failures. Anaesthesia 2001, 56, 75–81. [Google Scholar] [CrossRef]
- Wu, C.F.; Hsieh, M.J.; Liu, H.P.; Gonzalez-Rivas, D.; Liu, Y.H.; Wu, Y.C.; Chao, Y.K.; Wu, C.Y. Management of post-operative pain by placement of an intraoperative intercostal catheter after single port video-assisted thoracoscopic surgery: A propensity-score matched study. J. Thorac. Dis. 2016, 8, 1087–1093. [Google Scholar] [CrossRef] [Green Version]
- Ghee, C.D.; Fortes, D.L.; Liu, C.; Khandhar, S.J. A randomized controlled trial of continuous subpleural bupivacaine after thoracoscopic surgery. Semin. Thorac. Cardiovasc. Surg. 2018, 30, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Bendixen, M.; Jørgensen, O.D.; Kronborg, C.; Andersen, C.; Licht, P.B. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: A randomised controlled trial. Lancet Oncol. 2016, 17, 836–844. [Google Scholar] [CrossRef]
- Martin, L.W.; Sarosiek, B.M.; Harrison, M.A.; Hedrick, T.; Isbell, J.M.; Krupnick, A.S.; Lau, C.L.; Mehaffey, J.H.; Thiele, R.H.; Walters, D.M.; et al. Implementing a thoracic enhanced recovery program: Lessons learned in the first year. Ann. Thorac. Surg. 2018, 105, 1597–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, D.; Stamer, U.M.; Pogatzki-Zahn, E.; Zaslansky, R.; Tanase, N.V.; Perruchoud, C.; Kranke, P.; Komann, M.; Lehman, T.; Meissner, W.; et al. Chronic postsurgical pain in Europe: An observational study. Eur. J. Anaesthesiol. 2015, 32, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes-Pereira, L.; Valdoleiros, I.; Reis, P.; Abelha, F. Evaluating persistent postoperative pain in one tertiary hospital: Incidence, quality of life, associated factors, and treatment. Anesth. Pain Med. 2016, 6, e36461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedegaard, H.; Miniño, A.M.; Warner, M. Drug Overdose Deaths in the United States, 1999–2017: NCHS Data Brief: National Center for Health Statistics 2018. Available online: https://www.cdc.gov/nchs/data/databriefs/db329-h.pdf (accessed on 19 October 2020).
- Singh, G.K.; Kim, I.E.; Girmay, M.; Perry, C.; Daus, G.P.; Vedamuthu, I.P.; De Los Reyes, A.A.; Ramey, C.T.; Martin, E.K.; Allender, M. Opioid epidemic in the United States: Empirical trends, and a literature review of social determinants and epidemiological, pain management, and treatment patterns. Int. J. MCH AIDS 2019, 8, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.J.; Petersen, R.H.; Christensen, M. Video-assisted thoracoscopic surgery (VATS) lobectomy using a standardized anterior approach. Surg. Endosc. 2011, 25, 1263–1269. [Google Scholar] [CrossRef]
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995, 61, 277–284. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Kehlet, H.; Jensen, T.S.; Woolf, C.J. Persistent postsurgical pain: Risk factors and prevention. Lancet 2006, 367, 1618–1625. [Google Scholar] [CrossRef]
- McKenna, R.J. Complications and learning curves for video-assisted thoracic surgery lobectomy. Thorac. Surg. Clin. 2008, 18, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Ziarnik, E.; Grogan, E.L. Postlobectomy early complications. Thorac. Surg. Clin. 2015, 25, 355–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karcz, M.; Papadakos, P.J. Respiratory complications in the postanesthesia care unit: A review of pathophysiological mechanisms. Can. J. Respir. Ther. 2013, 49, 21–29. [Google Scholar] [PubMed]
- Kamiyoshihara, M.; Nagashima, T.; Ibe, T.; Atsumi, J.; Shimizu, K.; Takeyoshi, I. Is epidural analgesia necessary after video-assisted thoracoscopic lobectomy? Asian Cardiovasc. Thorac. Ann. 2010, 18, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Wildgaard, K.; Petersen, R.H.; Hansen, H.J.; Møller-Sørensen, H.; Ringsted, T.K.; Kehlet, H. Multimodal analgesic treatment in video-assisted thoracic surgery lobectomy using an intraoperative intercostal catheter. Eur. J. Cardiothorac. Surg. 2012, 41, 1072–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T.; Carter, T.; Cassidy, C.L.; Chittenden, E.H.; Degenhardt, E.; et al. Management of postoperative pain: A clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar]
- Thompson, C.; French, D.G.; Costache, I. Pain management within an enhanced recovery program after thoracic surgery. J. Thorac. Dis. 2018, 10 (Suppl. 32), 3773–3780. [Google Scholar] [CrossRef]
- Luketich, J.D.; Land, S.R.; Sullivan, E.A.; Alvelo-Rivera, M.; Ward, J.; Buenaventura, P.O.; Landreneau, R.J.; Hart, L.A.; Fernando, H.C. Thoracic epidural versus intercostal nerve catheter plus patient-controlled analgesia: A randomized study. Ann. Thorac. Surg. 2005, 79, 1845–1850. [Google Scholar] [CrossRef]
- De Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.W.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | ICC, n = 51 | SSINB, n = 44 | p-Value |
|---|---|---|---|
| Age (years), median (range) | 65 (28–83) | 65 (37–80) | 0.993 |
| Gender (%) | 1.000 | ||
| Female | 26 (51.0) | 23 (52.3) | |
| Male | 25 (49.0) | 21 (47.7) | |
| Side (%) | 1.000 | ||
| Left lung | 16 (31.4) | 14 (31.8) | |
| Right Lung | 35 (68.6) | 30 (68.2) | |
| Lobe (%) | 1.000 | ||
| Upper Lobe | 24 (47.1) | 21 (47.7) | |
| Middle Lobe | 5 (9.8) | 4 (9.1) | |
| Lower Lobe | 21 (41.2) | 19 (43.2) | |
| Multilobar | 1 (2.0) | 0 (0.0) | |
| Comorbidities (%) | |||
| Coronary Artery Disease | 7 (13.7) | 7 (15.9) | 0.780 |
| Chronic Obstructive | 12 (23.5) | 13 (29.5) | 0.641 |
| Pulmonary Disease | |||
| Diabetes Mellitus | 5 (9.8) | 7 (15.9) | 0.537 |
| Postoperative Complications (%) | 0.721 | ||
| Clavien-Dindo I–II | 8 (15.7) | 9 (20.5) | |
| Clavien-Dindo III–IV | 3 (5.9) | 4 (9.1) | |
| No Complication | 40 (78.4) | 31 (70.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponholzer, F.; Ng, C.; Maier, H.; Dejaco, H.; Schlager, A.; Lucciarini, P.; Öfner, D.; Augustin, F. Intercostal Catheters for Postoperative Pain Management in VATS Reduce Opioid Consumption. J. Clin. Med. 2021, 10, 372. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020372
Ponholzer F, Ng C, Maier H, Dejaco H, Schlager A, Lucciarini P, Öfner D, Augustin F. Intercostal Catheters for Postoperative Pain Management in VATS Reduce Opioid Consumption. Journal of Clinical Medicine. 2021; 10(2):372. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020372
Chicago/Turabian StylePonholzer, Florian, Caecilia Ng, Herbert Maier, Hannes Dejaco, Andreas Schlager, Paolo Lucciarini, Dietmar Öfner, and Florian Augustin. 2021. "Intercostal Catheters for Postoperative Pain Management in VATS Reduce Opioid Consumption" Journal of Clinical Medicine 10, no. 2: 372. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020372