
Flexible Magnifying Endoscopy with Narrow Band Imaging for Diagnosing Uterine Cervical Neoplasms: A Multicenter Prospective Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Participants
Inclusion and Exclusion Criteria
2.3. Procedures and Evaluations
2.3.1. ME-NBI Procedure
2.3.2. Colposcopic Procedure
2.4. Patients’ Acceptability and Adverse Events
2.5. Histological Examination
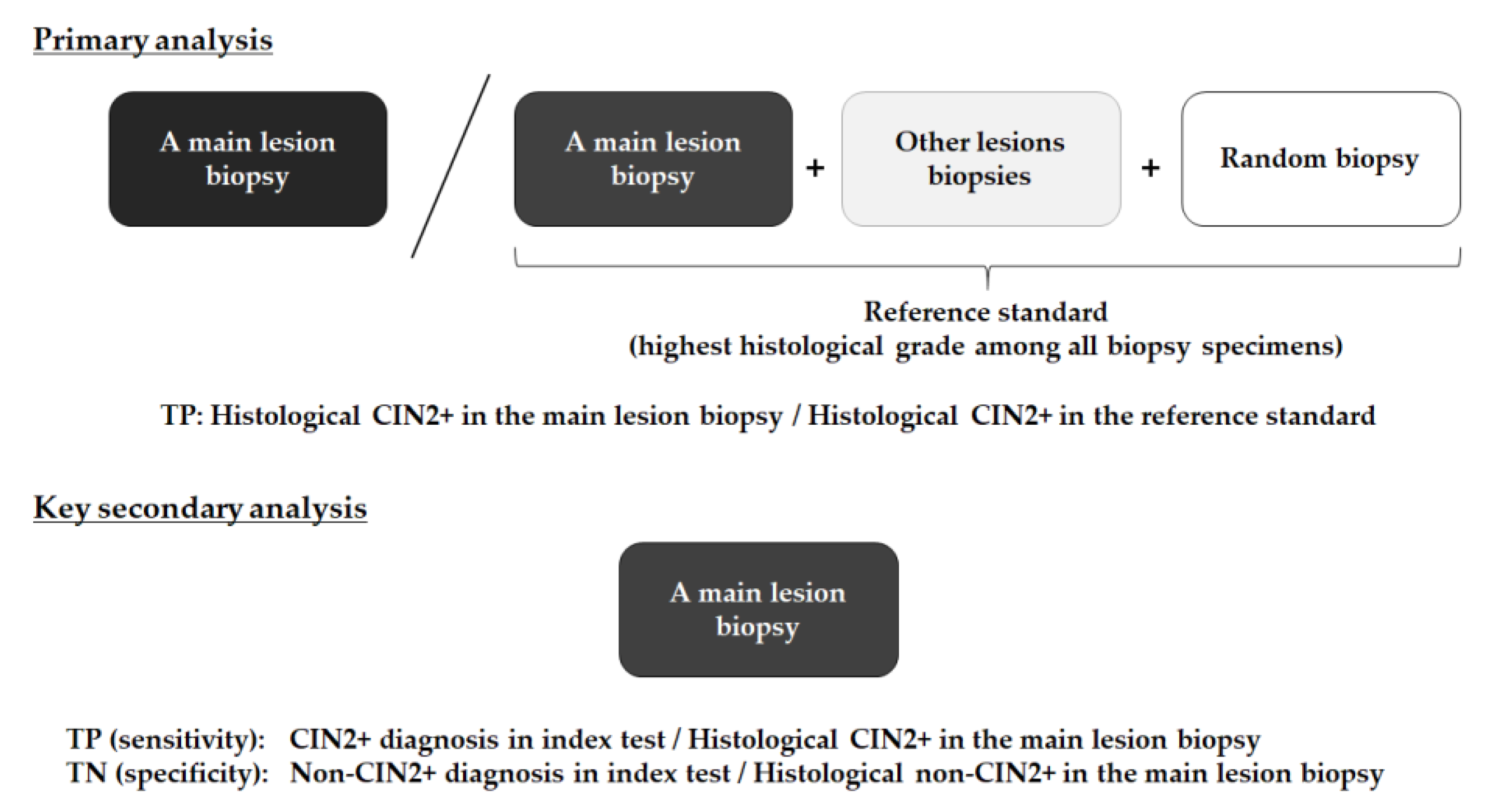
2.6. Outcome Measures
2.7. Statistical Methods
3. Results
3.1. Patient Enrollment
3.2. Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canfell, K.; Kim, J.J.; Brisson, M.; Keane, A.; Simms, K.T.; Caruana, M.; Burger, E.A.; Martin, D.; Nguyen, D.T.N.; Bénard, E.; et al. Mortality impact of achieving WHO cervical cancer elimination targets: A comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet 2020, 395, 591–603. [Google Scholar] [CrossRef] [Green Version]
- Kyrgiou, M.; Arbyn, M.; Bergeron, C.; Bosch, F.X.; Dillner, J.; Jit, M.; Kim, J.; Poljak, M.; Nieminen, P.; Sasieni, P.; et al. Cervical screening: ESGO-EFC position paper of the European Society of Gynaecologic Oncology (ESGO) and the European Federation of Colposcopy (EFC). Br. J. Cancer 2020, 123, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.H.; Tidy, J.A. The diagnostic accuracy of colposcopy—A review of research methodology and impact on the outcomes of quality assurance. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Selmouni, F.; Zidouh, A.; Alvarez-Plaza, C.; El Rhazi, K. Perception and satisfaction of cervical cancer screening by visual inspection with acetic acid (VIA) at Meknes-Tafilalet Region, Morocco: A population-based cross-sectional study. BMC Womens Health 2015, 15, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, P.W.Y.; Uedo, N.; Singh, R.; Gotoda, T.; Ng, E.K.W.; Yao, K.; Ang, T.L.; Ho, S.H.; Kikuchi, D.; Yao, F.; et al. An Asian consensus on standards of diagnostic upper endoscopy for neoplasia. Gut 2019, 68, 186–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gono, K.; Obi, T.; Yamaguchi, M.; Ohyama, N.; Machida, H.; Sano, Y.; Yoshida, S.; Hamamoto, Y.; Endo, T. Appearance of enhanced tissue features in narrow-band endoscopic imaging. J. Biomed. Opt. 2004, 9, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, R.; Kawahara, Y.; Okada, H.; Hori, K.; Inoue, M.; Kawano, S.; Tanioka, D.; Tsuzuki, T.; Uemura, M.; Ohara, N.; et al. Narrow-band imaging provides reliable screening for esophageal malignancy in patients with head and neck cancers. Am. J. Gastroenterol. 2009, 104, 2942–2948. [Google Scholar] [CrossRef] [PubMed]
- Muto, M.; Minashi, K.; Yano, T.; Saito, Y.; Oda, I.; Nonaka, S.; Omori, T.; Sugiura, T.; Goda, K.; Kaise, M.; et al. Early detection of superficial squamous cell carcinoma in the head and neck region and esophagus by narrow band imaging: A multicenter randomized controlled trial. J. Clin. Oncol. 2010, 28, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Nagami, Y.; Tominaga, K.; Machida, H.; Nakatani, M.; Kameda, N.; Sugimori, S.; Okazaki, H.; Tanigawa, T.; Yamagami, H.; Kubo, N.; et al. Usefulness of non-magnifying narrow-band imaging in screening of early esophageal squamous cell carcinoma: A prospective comparative study using propensity score matching. Am. J. Gastroenterol. 2014, 109, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Inoue, H.; Kaga, M.; Ikeda, H.; Sato, C.; Sato, H.; Minami, H.; Santi, E.G.; Hayee, B.; Eleftheriadis, N. Magnification endoscopy in esophageal squamous cell carcinoma: A review of the intrapapillary capillary loop classification. Ann. Gastroenterol. 2015, 28, 41–48. [Google Scholar]
- Nishiyama, N.; Kanenishi, K.; Mori, H.; Kobara, H.; Fujihara, S.; Chiyo, T.; Kobayashi, N.; Matsunaga, T.; Ayaki, M.; Yachida, T.; et al. Flexible magnifying endoscopy with narrow band imaging for the diagnosis of uterine cervical tumors: A cooperative study among gastrointestinal endoscopists and gynecologists to explore a novel micro-vascular classification system. Oncol. Lett. 2017, 14, 355–362. [Google Scholar] [CrossRef]
- Uchita, K.; Kanenishi, K.; Hirano, K.; Kobara, H.; Nishiyama, N.; Kawada, A.; Fujihara, S.; Ibuki, E.; Haba, R.; Takahashi, Y.; et al. Characteristic findings of high-grade cervical intraepithelial neoplasia or more on magnifying endoscopy with narrow band imaging. Int. J. Clin. Oncol. 2018, 23, 707–714. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.M.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. Towards complete and accurate reporting of studies of diagnostic accuracy: The STARD initiative. Fam. Pract. 2004, 21, 4–10. [Google Scholar] [CrossRef]
- Bornstein, J.; Bentley, J.; Bosze, P.; Girardi, F.; Haefner, H.; Menton, M.; Perrotta, M.; Prendiville, W.; Russell, P.; Sideri, M.; et al. 2011 Colposcopic terminology of the International Federation for Cervical Pathology and Colposcopy. Obstet. Gynecol. 2012, 120, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ctep.Cancer.Gov. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 8 May 2021).
- Japanese Society of Obstetrics and Gynecology and Japan Society of Pathology. The General Rules for Clinical and Pathological Management of Uterine Cervical Cancer, Pathological Edition, 4th ed.; Kanehara-shuppan: Tokyo, Japan, 2017. [Google Scholar]
- Wade, R.; Spackman, E.; Corbett, M.; Walker, S.; Light, K.; Naik, R.; Sculpher, M.; Eastwood, A. Adjunctive colposcopy technologies for examination of the uterine cervix-DySIS, LuViva Advanced Cervical Scan and Niris Imaging System: A systematic review and economic evaluation. Health Technol. Assess. 2013, 17, 1–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontham, E.T.H.; Wolf, A.M.D.; Church, T.R.; Etzioni, R.; Flowers, C.R.; Herzig, A.; Guerra, C.E.; Oeffinger, K.C.; Shih, Y.C.T.; Walter, L.C.; et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA. Cancer J. Clin. 2020, 70, 321–346. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.F.; Schottenfeld, D.; Tortolero-Luna, G.; Cantor, S.B.; Richards-Kortum, R. Colposcopy for the diagnosis of squamous intraepithelial lesions: A meta-analysis. Obstet. Gynecol. 1998, 91, 626–631. [Google Scholar] [CrossRef]
- Underwood, M.; Arbyn, M.; Parry-Smith, W.; De Bellis-Ayres, S.; Todd, R.; Redman, C.W.E.; Moss, E.L. Accuracy of colposcopically-directed punch biopsies: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Ishihara, R.; Kato, Y.; Matsunaga, T.; Nishida, T.; Yamada, T.; Ogiyama, H.; Horie, M.; Kinoshita, K.; Tada, T. Comparison of performances of artificial intelligence versus expert endoscopists for real-time assisted diagnosis of esophageal squamous cell carcinoma (with video). Gastrointest. Endosc. 2020, 92, 848–855. [Google Scholar] [CrossRef]
- Uchita, K.; Kobara, H.; Yorita, K.; Shigehisa, Y.; Kuroiwa, C.; Nishiyama, N.; Takahashi, Y.; Kai, Y.; Kunikata, J.; Shimokawa, T.; et al. Quality of assessment of endoscopic forceps biopsy samples under magnifying narrow band imaging for histological diagnosis of cervical intraepithelial neoplasia: A feasibility study. Diagnostics 2021, 11, 360. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, H.; Doyama, H.; Ishikawa, H.; Uedo, N.; Gotoda, T.; Kato, M.; Nagao, S.; Nagami, Y.; Aoyagi, H.; Imagawa, A.; et al. Evaluation of an e-learning system for diagnosis of gastric lesions using magnifying narrow-band imaging: A multicenter randomized controlled study. Endoscopy 2017, 49, 957–967. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Number of Patients | 88 |
|---|---|
| Median age, years (range) | 40 (21–67) |
| Indications, n (%) | |
| Positive Pap smear | 72 |
| High-grade cytology on follow-up | 13 |
| Definitive CIN3 | 3 |
| HPV infection, n (%) | |
| Positive | 25 |
| Negative | 5 |
| Not examined | 58 |
| HPV vaccination, n (%) | |
| Received | 5 |
| Not received | 83 |
| Institution, n (%) | |
| Kochi Red Cross Hospital | 60 |
| Kagawa University Hospital | 25 |
| OICI | 3 |
| Final histological diagnosis in the reference standard, n (%) | |
| Non-cancerous lesion | 8 |
| CIN1 | 32 |
| CIN2 | 13 |
| CIN3 | 34 |
| Microinvasive carcinoma | 1 |
| Measures | ME-NBI (n = 88) | Colposcopy (n = 88) | p Value |
|---|---|---|---|
| Detection rate for patients with CIN2+ | 79.2 (65.7–88.3) | 79.2 (65.7–88.3) | 1.000 |
| Diagnostic ability for histological CIN2+ lesions | |||
| Sensitivity | 86.8 (72.7–94.3) | 73.7 (58.0–85.0) | 0.15 |
| Specificity | 50.0 (36.6–63.4) | 68.0 (54.2–79.2) | 0.067 |
| Overall accuracy | 65.9 (55.5–75.0) | 70.5 (60.2–79.0) | 0.517 |
| Proportion of patients with visible whole circumferential transitional zones, % | 97.7 | 90.9 | 0.031 |
| Proportion of patients with visible external uterine orifice, % | 96.6 | 89.8 | 0.073 |
| Incidence of Grade 2 adverse events | 0 | 0 | |
| Acceptability of patients, grade, n (%) | |||
| Discomfort (n = 87) | |||
| 1 | 61 (69.3) | 9 (10.2) | |
| 2 | 23 (26.1) | 14 (15.9) | |
| 3 | 2 (2.3) | 14 (15.9) | |
| 4 | 1 (1.1) | 24 (27.3) | |
| 5 | 0 | 26 (29.5) | |
| Embarrassment (n = 88) | |||
| 1 | 45 (51.1) | 20 (22.7) | |
| 2 | 29 (33.0) | 11 (12.5) | |
| 3 | 8 (9.1) | 17 (19.3) | |
| 4 | 5 (5.7) | 16 (18.2) | |
| 5 | 1 (1.1) | 24 (27.2) | |
| Preference to next examination (n = 86), n (%) | 65 (75.6) | 2 (2.3) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobara, H.; Uchita, K.; Uedo, N.; Kunikata, J.; Yorita, K.; Tada, N.; Nishiyama, N.; Shigehisa, Y.; Kuroiwa, C.; Matsuura, N.; et al. Flexible Magnifying Endoscopy with Narrow Band Imaging for Diagnosing Uterine Cervical Neoplasms: A Multicenter Prospective Study. J. Clin. Med. 2021, 10, 4753. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204753
Kobara H, Uchita K, Uedo N, Kunikata J, Yorita K, Tada N, Nishiyama N, Shigehisa Y, Kuroiwa C, Matsuura N, et al. Flexible Magnifying Endoscopy with Narrow Band Imaging for Diagnosing Uterine Cervical Neoplasms: A Multicenter Prospective Study. Journal of Clinical Medicine. 2021; 10(20):4753. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204753
Chicago/Turabian StyleKobara, Hideki, Kunihisa Uchita, Noriya Uedo, Jun Kunikata, Kenji Yorita, Naoya Tada, Noriko Nishiyama, Yuriko Shigehisa, Chihiro Kuroiwa, Noriko Matsuura, and et al. 2021. "Flexible Magnifying Endoscopy with Narrow Band Imaging for Diagnosing Uterine Cervical Neoplasms: A Multicenter Prospective Study" Journal of Clinical Medicine 10, no. 20: 4753. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204753