
Evaluation of Vascular Endothelial Function in Children with Type 1 Diabetes Mellitus

 and
and
Abstract
:1. Introduction
The Aim of the Study
2. Materials and Methods
Ethical Issues
3. Results
4. Discussion
5. Conclusions
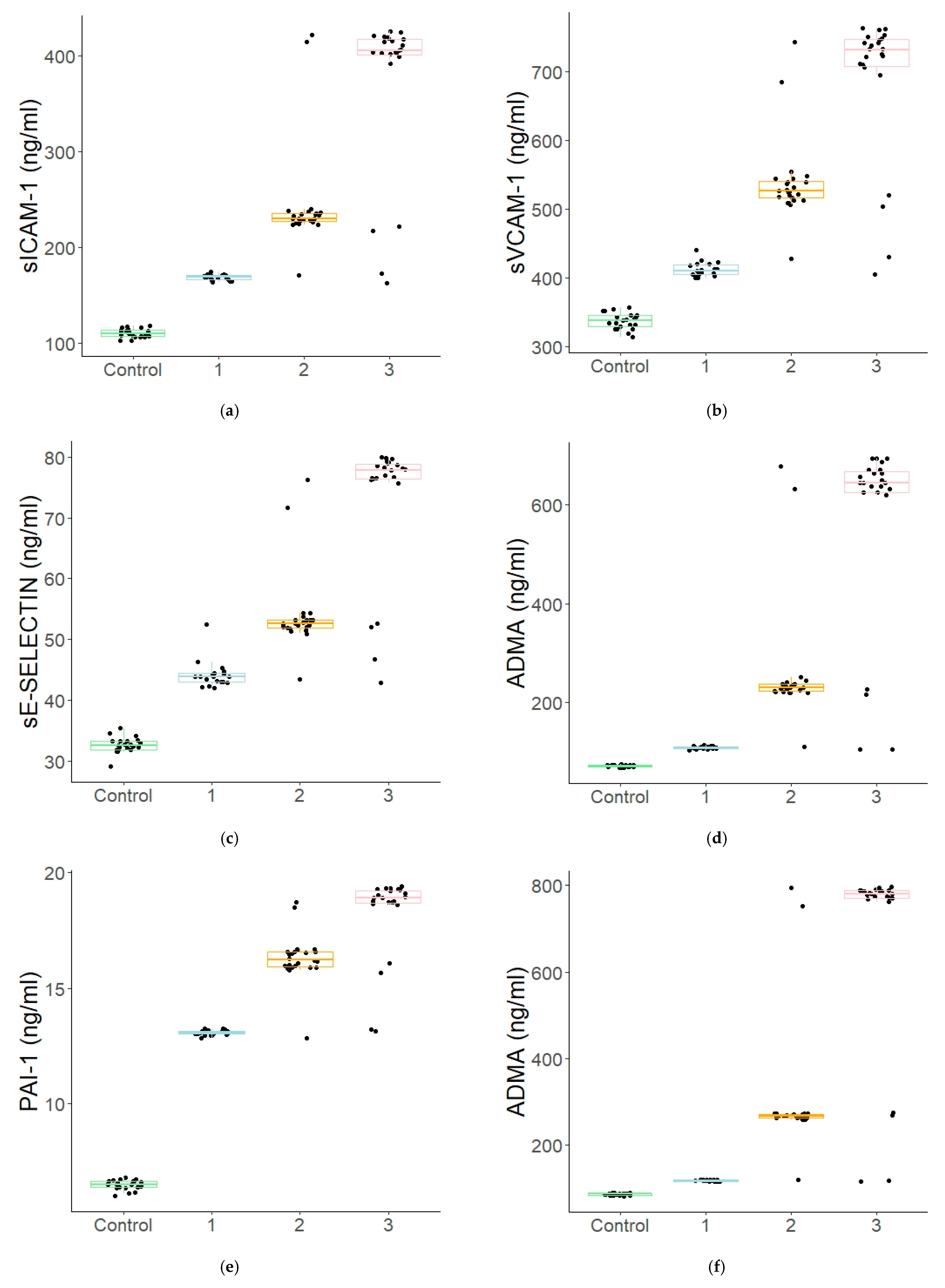
- In the patients with type 1 diabetes, statistically significantly higher concentrations were demonstrated for all the assayed markers when compared to the corresponding values in the control group.
- A significant increase in the concentrations of those markers was already observed at the early stages of the disease.
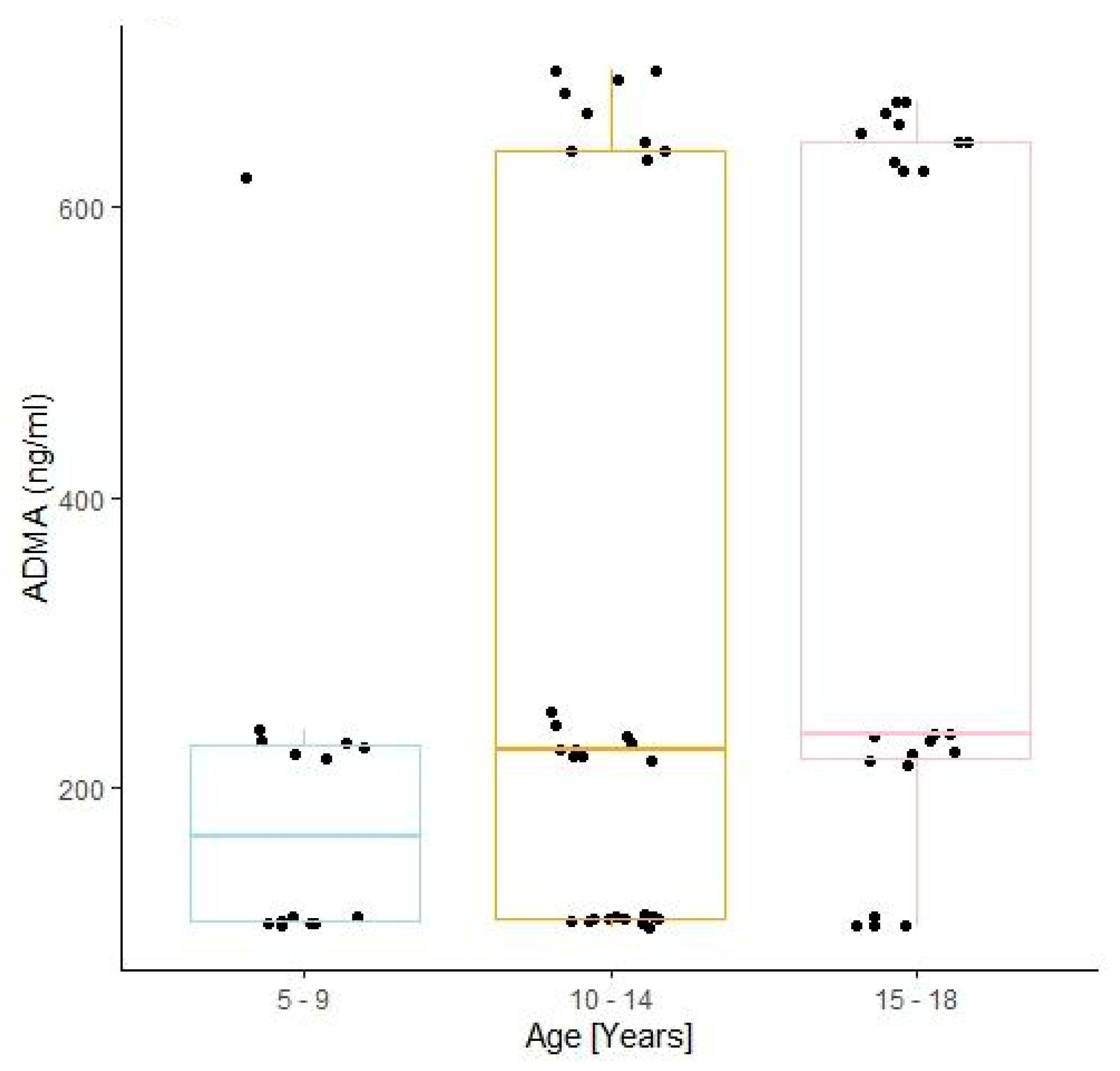
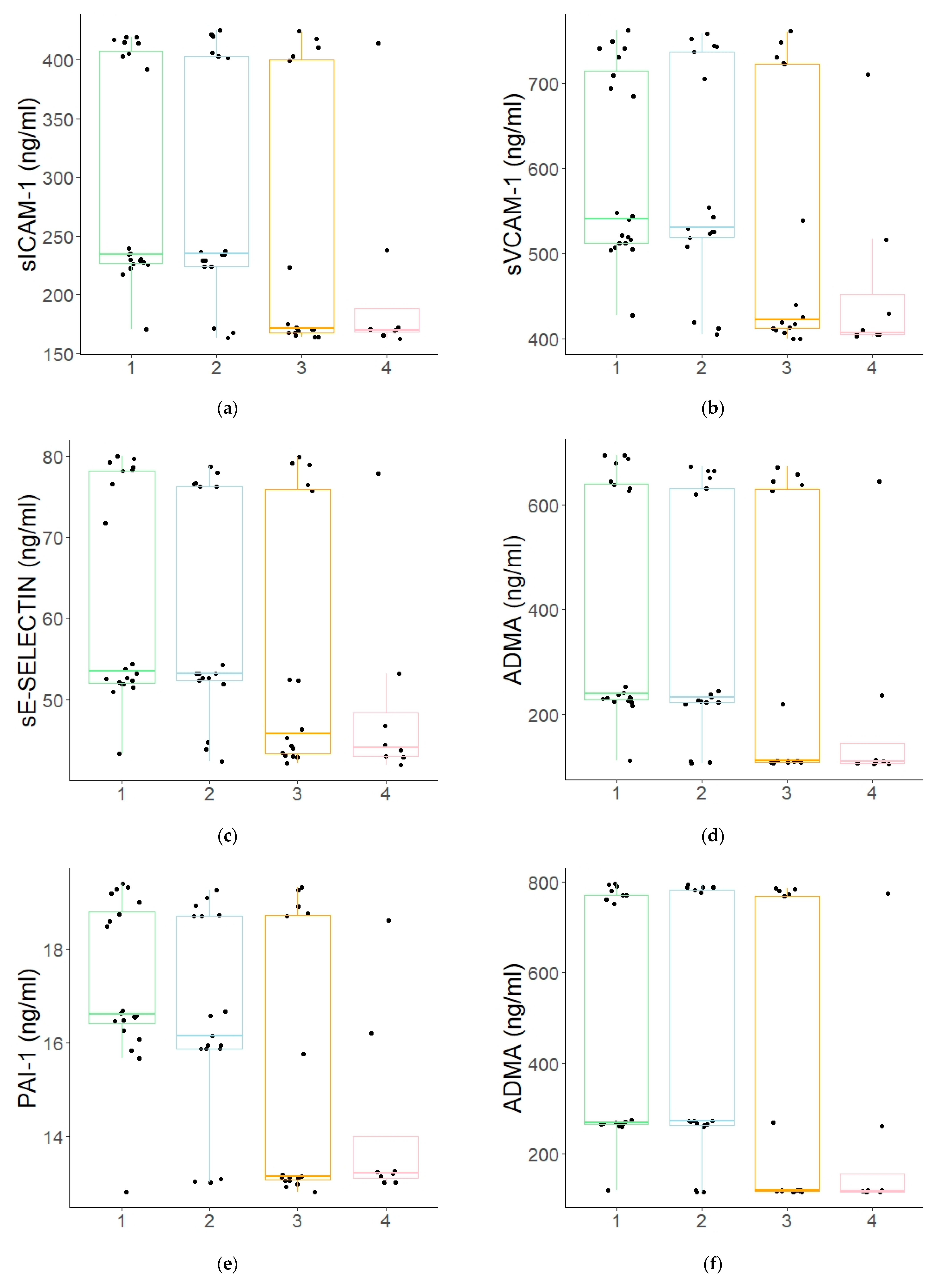
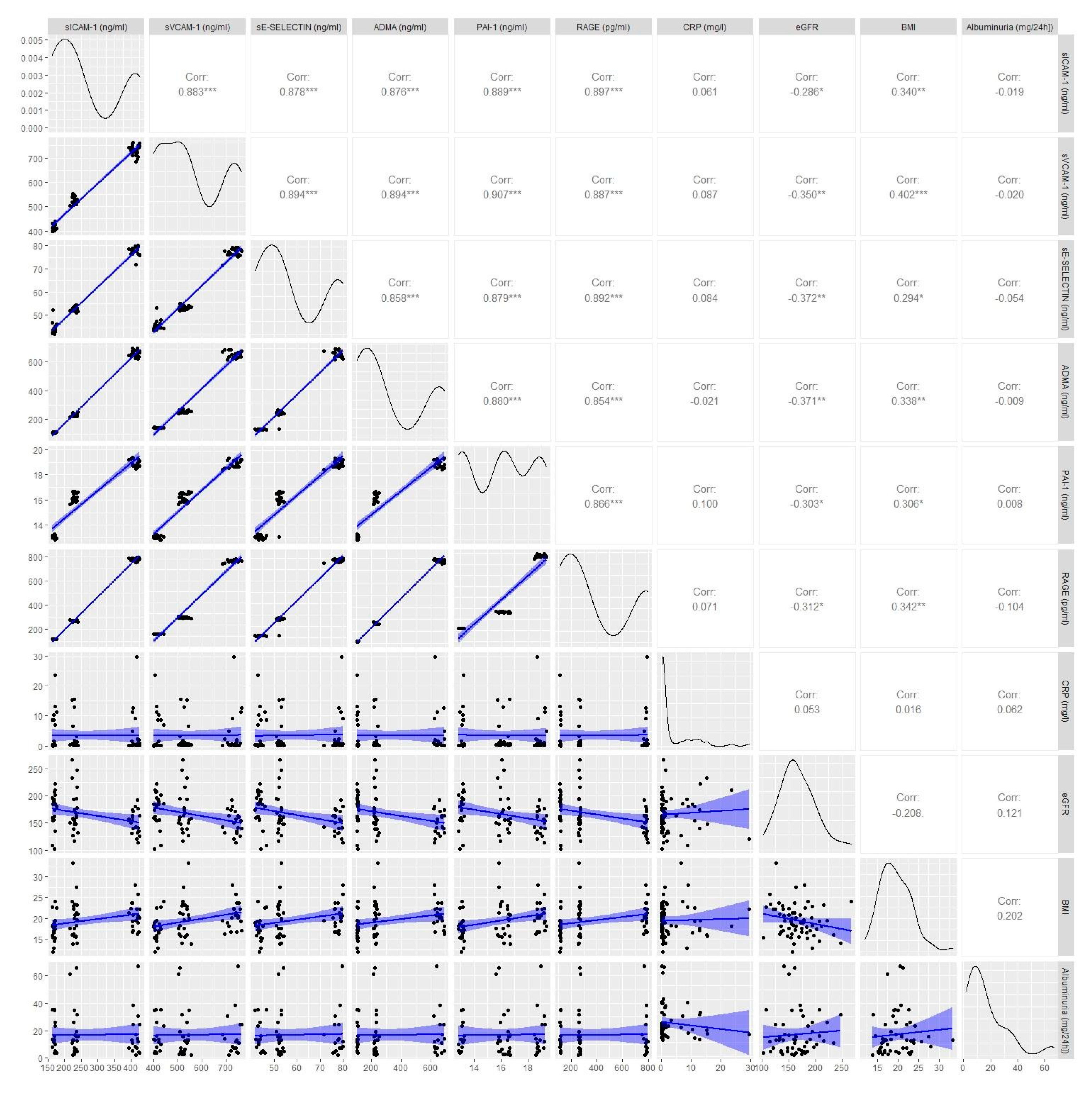
- All of the evaluated endothelial dysfunction markers were positively correlated with the disease duration, the age of the patients, and their BMI, while only PAI-1 and sE-SELECTIN were characteristic of linear correlations with the estimated glomerular filtration rate (eGFR).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guariguata, L.; Whiting, D.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Knapik-Kordecka, M.; Piwowar, A.; Warwas, M. Oxidative-antioxidant imbalances and risk factors for atherosclerosis and vascular complications in patients with type 2 diabetes. Med. News 2007, 40, 7–8. [Google Scholar]
- Giugliano, D.; Ceriello, A.; Paolisso, G. Oxidative stress and diabetic vascular complications. Diabetes Care 1996, 19, 257–267. [Google Scholar] [CrossRef]
- Lipinski, B. Pathophysiology of oxidative stress in diabetes mellitus. J. Diabetes Its Complicat. 2001, 15, 203–210. [Google Scholar] [CrossRef]
- Mogensen, C.E.; Christensen, C.K.; Vittinghus, E. The stages in diabetic renal disease: With emphasis on the stage of incipient diabetic nephropathy. Diabetes 1983, 32, 64–78. [Google Scholar] [CrossRef]
- Deckert, T.; Feldt-Rasmussen, B.; Borch-Johnsen, K.; Jensen, T.; Kofoed-Enevoldsen, A. Albuminuria reflects widespread vascular damage. Diabetologia 1989, 32, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Krol, G.L.; Kunisaki, M.; Nishio, T.; Inoguchi, T.; Shiba, P. Biochemical and molecular mechanisms in the development of diabetic vascular complications. Diabetes 1996, 45, S105–S108. [Google Scholar]
- Tatoń, J.; Czech, A.; Łaz, R. Angiotoxic Effects of Increased Oxidative Stress in Diabetes. Diabetic Heart Disease; Wydawnictwo Medyczne via Medica: Gdańsk, Poland, 2005; pp. 93–99. [Google Scholar]
- Astrup, A.S.; Tarnow, L.; Pietraszek, L.; Schalkwijk, C.G.; Stehouwer, C.D.; Parving, H.H.; Rossing, P. Markers of endothelial dysfunction and inflammation in type 1 diabetic patients with or without diabetic nephropathy followed for 10 years: Association with mortality and decline of glomerular filtration rate. Diabetes Care 2008, 31, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Polek, A.; Sobiczewski, W.; Matowicka-Karna, J. P-selektyna i jej rola w niektórych chorobach P-selectin and its role in some diseases. Postepy Hig. Med. Dosw. 2009, 63, 465–470. [Google Scholar]
- Chase, S.D.; Magnani, J.L.; Simon, S.I. E-selectin ligands as mechanosensitive receptors on neutrophils in health and disease. Ann. Biomed. Eng. 2012, 40, 849–859. [Google Scholar] [CrossRef] [Green Version]
- Abbassi, O.M.I.D.; Kishimoto, T.K.; McIntire, L.V.; Anderson, D.C.; Smith, C.W. E-selectin supports neutrophil rolling in vitro under conditions of flow. J. Clin. Investig. 1993, 92, 2719. [Google Scholar] [CrossRef] [Green Version]
- Lequin, R.M. Enzyme immunoassay (EIA)/enzyme-linked immunosorbent assay (ELISA). Clin. Chem. 2005, 51, 2415–2418. [Google Scholar] [CrossRef] [Green Version]
- Fossceco, S.L. Exploring Enzyme-Linked Immunosorbent Assay (ELISA) Data with the SAS®. Anal. Appl. 1999. Available online: https://stats.idre.ucla.edu/wpcontent/uploads/2016/02/analystelisa.pdf (accessed on 11 June 2018).
- Schwartz, G.J.; Haycock, G.B.; Edelmann, C.M.; Spitzer, A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 1976, 582, 259–263. [Google Scholar]
- Miklaszewska, M. Laboratory Indicators of Renal Function-Determination Method and Clinical Value. Available online: https://www.mp.pl/pediatria/praktyka-kliniczna/badania-laboratoryjne/176082,laboratoryjne-wskazniki-czynnosci-nerek (accessed on 11 June 2018).
- Korzeniowska, K.; Jabłecka, A. Diabetes (Part I). Farm. Współ. 2008, 1, 231–235. Available online: http://www.akademiamedycyny.pl/wp-content/uploads/2016/05/200804_Farmacja_003.pdf (accessed on 25 August 2021).
- Schalkwijk, C.G.; Stehouwer, C.D. Vascular complications in diabetes mellitus: The role of endothelial dysfunction. Clin. Sci. 2005, 109, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Wierusz-Wysocka, B. Pathogenetic relationships between diabetic micro- and macroangiopathy Part I. Diabetic microangiopathy-what’s new. Clin. Diabetol. 2009, 10, 151–156. [Google Scholar]
- Araszkiewicz, A.; Mackiewicz-Wysocka, M.; Wierusz-Wysocka, B. Skin dysfunction in diabetes. Part 2—Microcirculation and peripheral nerve function. Clin. Diabetol. 2014, 3, 117–124. [Google Scholar]
- Romero, P.; Salvat, M.; Fernandez, J.; Baget, M.; Martinez, I. Renal and retinal microangiopathy after 15 years of follow-up study in a sample of type 1 diabetes mellitus patients. J. Diabetes Its Complicat. 2007, 21, 93–100. [Google Scholar] [CrossRef]
- Karamanos, B.; Porta, M.; Songini, M.; Metelko, Z.; Kerenyi, Z.; Tamas, G.; Fuller, J.H. Different risk factors of microangiopathy in patients with type I diabetes mellitus of short versus long duration. The EURODIAB IDDM Complications Study. Diabetologia 2000, 43, 348–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, Z.; Kahe, F.; Jamil, A.; Marszalek, J.; Ghanbari, A.; Afarideh, M.; Chi, G. Intercellular adhesion molecule-1 in diabetic patients with and without microalbuminuria. Diabetes Metab. Syndrome 2018, 12, 365–368. [Google Scholar] [CrossRef]
- Liu, J.J.; Yeoh, L.Y.; Sum, C.F.; Tavintharan, S.; Ng, X.W.; Liu, S.; Lim, S.C. Vascular cell adhesion molecule-1, but not intercellular adhesion molecule-1, is associated with diabetic kidney disease in Asians with type 2 diabetes. J. Diabetes Its Complicat. 2015, 29, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Song, K.E.; Shin, D.S.; Ahn, S.M.; Ha, E.S.; Kim, D.J.; Lee, K.W. Alterations in peripheral blood levels of TIMP-1, MMP-2, and MMP-9 in patients with type-2 diabetes. Diabetes Res. Clin. Pract. 2005, 69, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Marfella, R.; Esposito, K.; Giunta, R.; Coppola, G.; De Angelis, L.; Farzati, B.; Giugliano, D. Circulating adhesion molecules in humans: Role of hyperglycemia and hyperinsulinemia. Circulation 2000, 101, 2247–2251. [Google Scholar] [CrossRef] [Green Version]
- El Amine, M.; Sohawon, S.; Lagneau, L.; Gaham, N.; Noordally, S. Plasma levels of icam-1 and circulating endothelial cells are elevated in unstable types 1 and 2 diabetes. Endocr. Regul. 2010, 44, 17–24. [Google Scholar] [CrossRef]
- Joy, N.G.; Hedrington, M.S.; Briscoe, V.J.; Tate, D.B.; Ertl, A.C.; Davis, S.N. Effects of acute hypoglycemia on inflammatory and pro-atherothrombotic biomarkers in individuals with type 1 diabetes and healthy individuals. Diabetes Care 2010, 33, 1529–1535. [Google Scholar]
- Kilpatrick, E.S.; Rigby, A.S.; Atkin, S.L. For debate. Glucose variability and diabetes complication risk: We need to know the answer. Diabet. Med. 2010, 27, 868–871. [Google Scholar] [CrossRef]
- Ceriello, A.; Ihnat, M.A. ‘Glycaemic variability’: A new therapeutic challenge in diabetes and the critical care setting. Diabet. Med. 2010, 27, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Lachin, J.M.; Bebu, I.; Bergenstal, R.M.; Pop-Busui, R.; Service, F.J.; Zinman, B.; Nathan, D.M. DCCT/EDIC Research Group. Association of Glycemic Variability in Type 1 Diabetes with Progression of Microvascular Outcomes in the Diabetes Control and Complications Trial. Diabetes Care 2017, 40, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Auwerx, J.; Bouillon, R.; Collen, D.; Geboers, J. Tissue-type plasminogen activator antigen and plasminogen activator inhibitor in diabetes mellitus. Arterioscler. Thromb. Vasc. Biol. 1988, 8, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Yarmolinsky, J.; Bordin Barbieri, N.; Weinmann, T. Plasminogen activator inhibitor-1 and type 2 diabetes: A systematic review and meta-analysis of observational studies. Sci. Rep. 2016, 6, 17714. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Lei, M.; Fu, S.; Fu, Y. Effect of diabetic duration on serum concentrations of endogenous inhibitor of nitric oxide synthase in patients and rats with diabetes. Life Sci. 2005, 77, 149–159. [Google Scholar] [CrossRef]
- Bogdanović, R. Diabetic nephropathy in children and adolescents. Pediatric Nephrol. 2008, 23, 507–525. [Google Scholar] [CrossRef]
- Głowińska, B.; Urban, M.; Peczyńska, J.; Florys, B. Soluble adhesion molecules (sICAM-1, sVCAM-1) and selectins (sE selectin, sP selectin, sL selectin) levels in children and adolescents with obesity, hypertension, and diabetes. Metabolism 2005, 54, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Juhan-Vague, I.; Roul, C.; Alessi, M.C.; Ardissone, J.P.; Heim, M. Increased plasminogen activator inhibitor activity in non insulin dependent diabetic patients-relationship with plasma insulin. Thromb. Haemost. 1989, 61, 370–373. [Google Scholar] [CrossRef]
- Juhan-Vague, I.; Alessi, M.C.; Vague, P. Increased plasma plasminogen activator inhibitor 1 levels. A possible link between insulin resistance and atherothrombosis. Diabetologia 1991, 34, 457–462. [Google Scholar] [CrossRef]
- Henry, M.; Tregouet, D.A.; Alessi, M.C.; Aillaud, M.F.; Visvikis, S.; Siest, G.; Tiret, L.; Juhan-Vague, I. Metabolic determinants are much more important than genetic polymorphisms in determining the PAI-1 activity and antigen plasma concentrations: A family study with part of the Stanislas Cohort. Arterioscler. Thromb. Vasc. Biol. 1988, 18, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Musiał, K.; Zwolińska, D. Matrix metalloproteinases (MMP-2, 9) and their tissue inhibitors (TIMP-1, 2) as novel markers of stress response and atherogenesis in children with chronic kidney disease (CKD) on conservative treatment. Cell Stress Chaperones 2011, 16, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Gheissari, A.; Meamar, R.; Abedini, A.; Roomizadeh, P.; Shafiei, M.; Samaninobandegani, Z.; Najafi, T.E. Association of matrix metalloproteinase-2 and matrix metalloproteinase-9 with endothelial dysfunction, cardiovascular disease risk factors and thrombotic events in children with end-stage renal disease. Iran. J. Kidney Dis. 2018, 12, 169–177. [Google Scholar] [PubMed]
- Meamar, R.; Shafiei, M.; Abedini, A.; Ghazvini MR, A.; Roomizadeh, P.; Taheri, S.; Gheissari, A. Association of E-selectin with hematological, hormonal levels and plasma proteins in children with end stage renal disease. Adv. Biomed. Res. 2016, 5, 118. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Studied Group n = 66 | Control Group n = 21 | p Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median Value | Mean ± SD | Median Value | ||
| Sex (female, n (%)) | 31 (46.97%) | 16 (76.19%) | 0.0367 | ||
| Age (years) | 12.69 ± 3.6 | 13.5 | 9.26 ± 2.9 | 9 | <0.001 |
| BMI (kg/m2) | 19.45 ± 3.9 | 19.02 | 17.47 ± 2.7 | 17 | 0.024 |
| Duration of diabetes (years) | 3.8 ± 4.2 | 2 | |||
| HbA1c (%) | 10.47 ± 3.07 | 9 | |||
| Haemoglobin (g/dL) | 13.21 ± 0.89 | 13.6 | 13.21 ± 0.89 | 13.21 | 1 |
| Leukocytes (thousand/μL) | 6.74 ± 1.81 | 6.9 | 6.83 ± 1.71 | 6.83 | 0.837 |
| PLT [thousand/μL] | 260.66 ± 76.07 | 261 | 305.2 ± 75.74 | 286 | 0.096 |
| Sodium (mmol/L) | 138 ± 3.15 | 138 | 138.5 ± 1.36 | 139 | 0.402 |
| Potassium (mmol/L) | 4.18 ± 0.45 | 4.2 | 4.19 ± 0.24 | 4.19 | 0.262 |
| CRP [mg/L] | 3.54 ± 6.0 | 0.67 | 0.77 ± 1.2 | 0.3 | 0.011 |
| AspAT | 26.33 ± 13.24 | 24 | 27.93 ± 5.80 | 28 | 0.566 |
| AlAT | 17.38 ± 8.53 | 16 | 15.73 ± 4.27 | 14.5 | 0.273 |
| TSH | 2.43 ± 1.45 | 2.06 | 2.22 ± 0.85 | 2.06 | 0.154 |
| Cholesterol | 165.52 ± 32.49 | 161 | 172.67 ± 11.67 | 175 | 0.104 |
| Triglycerides | 98.30 ± 41.53 | 92 | 83.5 ± 21.99 | 83.5 | 0.089 |
| Urea (mg/dL) | 21.13 ± 9.40 | 22.5 | 23.55 ± 5.71 | 23.55 | 0.353 |
| Creatinine (mg/dL) | 0.58 ± 0.14 | 0.56 | 0.66 ± 0.09 | 0.65 | 0.013 |
| eGFR (mL/min/1.73 m2) | 166.04 ± 32.86 | 160.26 | 114.11 ± 11.00 | 114.81 | <0.001 |
| sICAM-1 (ng/mL) | 267.15 ± 111.89 | 229.2 | 110.48 ± 4.53 | 110 | <0.001 |
| sVCAM-1 (ng/mL) | 554.01 ± 132.11 | 522.48 | 337.33 ± 11.73 | 337.45 | <0.001 |
| sE-SELECTIN (ng/mL) | 57.74 ± 14.19 | 52.49 | 32.64 ± 1.27 | 32.56 | <0.001 |
| ADMA (ng/mL) | 325.03 ± 233.39 | 227.75 | 71.91 ± 2.31 | 71.01 | <0.001 |
| PAI-1 (ng/mL) | 16.03 ± 2.41 | 16.12 | 6.51 ± 0.21 | 6.53 | <0.001 |
| RAGE (pg/mL) | 380.20 ± 282.90 | 265.52 | 84.94 ± 2.27 | 85.48 | <0.001 |
| Variables. | Control | Group 1 | Group 2 | Group 3 |
|---|---|---|---|---|
| Age (years) | (9.3 ± 2.9) e,f | (11.2 ± 3.4) c | (11.9 ± 3.8) b,e | (14.8 ± 2.5) b,c,f |
| BMI (kg/m2) | (17.5 ± 2.7) f | (17.3 ± 3.0) c | 19.8 ± 4.5 | (20.9 ± 3.1) c,f |
| HbA1c (%) | (12.2 ± 3.2) a | (9.2 ± 2.5) a | 10.3 ± 2.9 | |
| eGFR mL/min/1.73 m2 | (114.1 ± 1) d,e,f | (175.5 ± 28.0) c,d | (165.6 ± 33.6) e | (158.4 ± 35.2) c,f |
| S-creatinine (mg/dL) | (0.6 ± 0.1) d,e | (0.5 ± 0.1) c,d | (0.6 ± 0.1) b,e | (0.6 ± 0.1) b,c |
| Albuminuria (mg/24 h) | 15.2 ± 10.8 | 14.4 ± 14.2 | 21.5 ± 19.5 | |
| sICAM-1 (ng/mL) | (110.5 ± 4.5) d,e,f | (168.5 ± 3.0) a,c,d | (244.0 ± 55.2) a,b,e | (372.8 ± 85.3) b,c,f |
| sVCAM-1 (ng/mL) | (337.3 ± 11.7) d,e,f | (412.6 ± 10.3) a,c,d | (538.3 ± 59.8) a,b,e | (687.3 ± 107.8) b,c,f |
| sE-SELECTIN (ng/mL) | (5.4 ± 0.2) d,e,f | (44.2 ± 2.3) a,c,d | (54.0 ± 6.5) a,b,e | (72.8 ± 11.6) b,c,f |
| ADMA (ng/mL) | (71.9 ± 2.3) d,e,f | (109.3 ± 2.4) a,c,d | (261.1 ± 124.2) a,b,e | (570.0 ± 193.4) b,c,f |
| PAI-1 (ng/mL) | (6.5 ± 0.2) d,e,f | (13.1 ± 0.1) a,c,d | (16.3 ± 1.0) a,b,e | (18.2 ± 1.8) b,c,f |
| RAGE (pg/mL) | (84.9 ± 2.3) d,e,f | (116.8 ± 1.5) a,c,d | (301.9 ± 148.5) a,b,e | (679.5 ± 230.6) b,c,f |
| CRP (mg/L) | (0.8 ± 1.2) e,f | 3.0 ± 4.5 | (2.8 ± 4.8) e | (4.8 ± 7.9) f |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nocuń-Wasilewska, K.; Zwolińska, D.; Zubkiewicz-Kucharska, A.; Polak-Jonkisz, D. Evaluation of Vascular Endothelial Function in Children with Type 1 Diabetes Mellitus. J. Clin. Med. 2021, 10, 5065. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10215065
Nocuń-Wasilewska K, Zwolińska D, Zubkiewicz-Kucharska A, Polak-Jonkisz D. Evaluation of Vascular Endothelial Function in Children with Type 1 Diabetes Mellitus. Journal of Clinical Medicine. 2021; 10(21):5065. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10215065
Chicago/Turabian StyleNocuń-Wasilewska, Karolina, Danuta Zwolińska, Agnieszka Zubkiewicz-Kucharska, and Dorota Polak-Jonkisz. 2021. "Evaluation of Vascular Endothelial Function in Children with Type 1 Diabetes Mellitus" Journal of Clinical Medicine 10, no. 21: 5065. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10215065