
Long-Term Efficacy and Safety of Ibrutinib in the Treatment of CLL Patients: A Real Life Experience

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Overall Conduct
2.2. Study Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patients
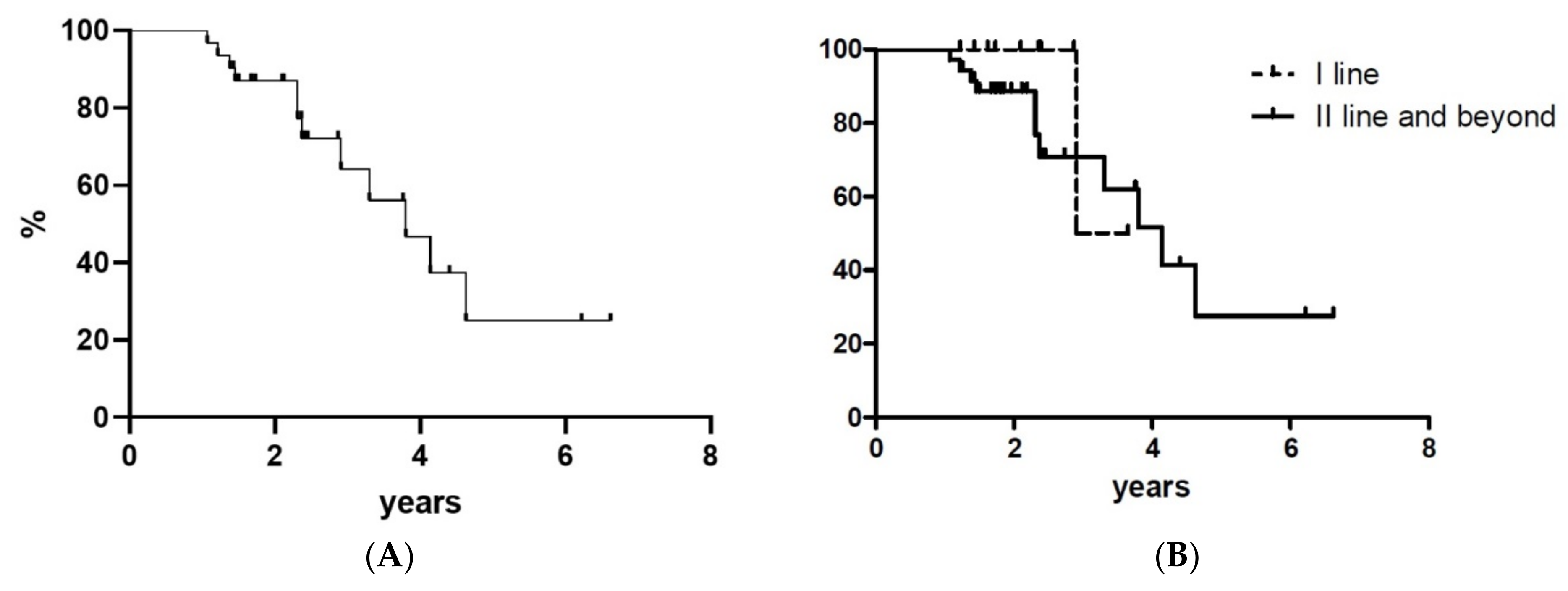
3.2. Response to Treatment and Survival Analysis
3.3. Treatment Administration
3.4. Safety
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Herman, S.E.; Gordon, A.L.; Hertlein, E.; Ramanunni, A.; Zhang, X.; Jaglowski, S.; Flynn, J.; Jones, J.; Blum, K.A.; Buggy, J.J.; et al. Bruton tyrosine kinase represents a promising therapeutic target for treatment of chronic lymphocytic leukemia and is effectively targeted by PCI-32765. Blood 2011, 117, 6287–6296. [Google Scholar] [CrossRef]
- Woyach, J.A.; Bojnik, E.; Ruppert, A.S.; Stefanovski, M.R.; Goettl, V.M.; Smucker, K.A.; Smith, L.L.; Dubovsky, J.A.; Towns, W.H.; MacMurray, J.; et al. Bruton’s tyrosine kinase (BTK) function is important to the development and expansion of chronic lymphocytic leukemia (CLL). Blood 2014, 123, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.; Furman, R.R.; Coutre, S.; Flinn, I.W.; Burger, J.A.; Blum, K.; Sharman, J.; Wierda, W.; Jones, J.; Zhao, W.; et al. Single-agent ibrutinib in treatment-naïve and relapsed/refractory chronic lymphocytic leukemia: A 5-year experience. Blood 2018, 131, 1910–1919. [Google Scholar] [CrossRef] [PubMed]
- Byrd, J.C.; Furman, R.R.; Coutre, S.E.; Flinn, I.W.; Burger, J.A.; Blum, K.; Sharman, J.P.; Wierda, W.; Zhao, W.; Heerema, N.A.; et al. Ibrutinib Treatment for First-Line and Relapsed/Refractory Chronic Lymphocytic Leukemia: Final Analysis of the Pivotal Phase Ib/II PCYC-1102 Study. Clin. Cancer. Res. 2020, 26, 3918–3927. [Google Scholar] [CrossRef] [Green Version]
- Byrd, J.C.; Brown, J.R.; O’Brien, S.; Barrientos, J.C.; Kay, N.E.; Reddy, N.M.; Coutre, S.; Tam, C.S.; Mulligan, S.P.; Jaeger, U.; et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N. Engl. J. Med. 2014, 371, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munir, T.; Brown, J.R.; O’Brien, S.; Barrientos, J.C.; Barr, P.M.; Reddy, N.M.; Coutre, S.; Tam, C.S.; Mulligan, S.P.; Jaeger, U.; et al. Final analysis from RESONATE: Up to six years of follow-up on ibrutinib in patients with previously treated chronic lymphocytic leukemia or small lymphocytic lymphoma. Am. J. Hematol. 2019, 94, 1353–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, J.A.; Tedeschi, A.; Barr, P.M.; Robak, T.; Owen, C.; Ghia, P.; Bairey, O.; Hillmen, P.; Bartlett, N.L.; Li, J.; et al. Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2015, 373, 2425–2437. [Google Scholar] [CrossRef] [PubMed]
- Burger, J.A.; Barr, P.M.; Robak, T.; Owen, C.; Ghia, P.; Tedeschi, A.; Bairey, O.; Hillmen, P.; Coutre, S.E.; Devereux, S.; et al. Long-term efficacy and safety of first-line ibrutinib treatment for patients with CLL/SLL: 5 years of follow-up from the phase 3 RESONATE-2 study. Leukemia 2020, 34, 787–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, S.; Jones, J.A.; Coutre, S.E.; Mato, A.R.; Hillmen, P.; Tam, C.; Österborg, A.; Siddiqi, T.; Thirman, M.J.; Furman, R.R.; et al. Ibrutinib for patients with relapsed or refractory chronic lymphocytic leukaemia with 17p deletion (RESONATE-17): A phase 2, open-label, multicentre study. Lancet. Oncol. 2016, 17, 1409–1418. [Google Scholar] [CrossRef]
- Arooqui, M.Z.; Valdez, J.; Martyr, S.; Aue, G.; Saba, N.; Niemann, C.U.; Herman, S.E.; Tian, X.; Marti, G.; Soto, S.; et al. Ibrutinib for previously untreated and relapsed or refractory chronic lymphocytic leukaemia with TP53 aberrations: A phase 2, single-arm trial. Lancet Oncol. 2015, 16, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Barr, P.M.; Robak, T.; Owen, C.; Tedeschi, A.; Bairey, O.; Bartlett, N.L.; Burger, J.A.; Hillmen, P.; Coutre, S.; Devereux, S.; et al. Sustained efficacy and detailed clinical follow-up of first-line ibrutinib treatment in older patients with chronic lymphocytic leukemia: Extended phase 3 results from RESONATE-2. Haematologica 2018, 103, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Tam, C.S.; O’Brien, S.M.; Wierda, W.G.; Stingo, F.; Plunkett, W.; Smith, S.C.; Kantarjian, H.M.; Freireich, E.J.; Keating, M.J. Fludarabine, cyclophosphamide, and rituximab treatment achieves long-term disease-free survival in IGHV-mutated chronic lymphocytic leukemia. Blood 2016, 127, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Advani, R.H.; Buggy, J.J.; Sharman, J.P.; Smith, S.M.; Boyd, T.E.; Grant, B.; Kolibaba, K.S.; Furman, R.R.; Rodriguez, S.; Chang, B.Y.; et al. Bruton tyrosine kinase inhibitor ibrutinib (PCI-32765) has significant activity in patients with relapsed/refractory B-cell malignancies. J. Clin. Oncol. 2013, 31, 88–94. [Google Scholar] [CrossRef]
- Winqvist, M.; Asklid, A.; Andersson, P.O.; Karlsson, K.; Karlsson, C.; Lauri, B.; Lundin, J.; Mattsson, M.; Norin, S.; Sandstedt, A.; et al. Real-world results of ibrutinib in patients with relapsed or refractory chronic lymphocytic leukemia: Data from 95 consecutive patients treated in a compassionate use program. A study from the Swedish Chronic Lymphocytic Leukemia Group. Haematologica 2016, 101, 1573–1580. [Google Scholar] [CrossRef]
- Ysebaert, L.; Aurran-Schleinitz, T.; Dartigeas, C.; Dilhuydy, M.S.; Feugier, P.; Michallet, A.S.; Tournilhac, O.; Dupuis, J.; Sinet, P.; Albrecht, C.; et al. Real-world results of ibrutinib in relapsed/refractory CLL in France: Early results on a large series of 428 patients. Am. J. Hematol. 2017, 92, E166–E168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pula, B.; Iskierka-Jazdzewska, E.; Dlugosz-Danecka, M.; Szymczyk, A.; Hus, M.; Szeremet, A.; Drozd-Sokolowska, J.; Waszczuk-Gajda, A.; Zaucha, J.M.; Holojda, J.; et al. Long-term Efficacy of Ibrutinib in Relapsed or Refractory Chronic Lymphocytic Leukemia: Results of the Polish Adult Leukemia Study Group Observational Study. Anticancer Res. 2020, 40, 4059–4066. [Google Scholar] [CrossRef] [PubMed]
- Van der Straten, L.; Levin, M.D.; Visser, O.; Blijlevens, N.M.A.; Cornelissen, J.J.; Doorduijn, J.K.; Kater, A.P.; Dinmohamed, A.G. The effectiveness of ibrutinib in chronic lymphocytic leukaemia: A nationwide, population-based study in the Netherlands. Br. J. Haematol. 2020, 188, e109–e112. [Google Scholar] [PubMed]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Döhner, H.; Hillmen, P.; Keating, M.; Montserrat, E.; Chiorazzi, N.; et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 2018, 131, 2745–2760. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.D.; Wang, X.V.; Kay, N.E.; Hanson, C.A.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Ibrutinib-Rituximab or Chemoimmunotherapy for Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2019, 381, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Woyach, J.A.; Ruppert, A.S.; Heerema, N.A.; Zhao, W.; Booth, A.M.; Ding, W.; Bartlett, N.L.; Brander, D.M.; Barr, P.M.; Rogers, K.A.; et al. Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL. N. Engl. J. Med. 2018, 379, 2517–2528. [Google Scholar] [CrossRef]
- Gordon, M.J.; Churnetski, M.; Alqahtani, H.; Rivera, X.; Kittai, A.; Amrock, S.M.; James, S.; Hoff, S.; Manda, S.; Spurgeon, S.E.; et al. Comorbidities predict inferior outcomes in chronic lymphocytic leukemia treated with ibrutinib. Cancer 2018, 124, 3192–3200. [Google Scholar] [CrossRef] [Green Version]
- Tedeschi, A.; Frustaci, A.M.; Mauro, F.R.; Chiarenza, A.; Coscia, M.; Ciolli, S.; Reda, G.; Laurenti, L.; Varettoni, M.; Murru, R.; et al. Do age, fitness and concomitant medications influence management and outcomes of CLL patients treated with ibrutinib? Blood Adv. 2021. [Google Scholar] [CrossRef]
- Mulder, T.A.; Peña-Pérez, L.; Berglöf, A.; Meinke, S.; Estupiñán, H.Y.; Heimersson, K.; Zain, R.; Månsson, R.; Smith, C.I.E.; Palma, M. Ibrutinib Has Time-dependent On- and Off-target Effects on Plasma Biomarkers and Immune Cells in Chronic Lymphocytic Leukemia. Hemasphere 2021, 5, e564. [Google Scholar] [CrossRef] [PubMed]
- Shatzel, J.J.; Olson, S.R.; Tao, D.L.; McCarty, O.J.T.; Danilov, A.V.; DeLoughery, T.G. Ibrutinib-associated bleeding: Pathogenesis, management and risk reduction strategies. J. Thromb. Haemost. 2017, 15, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Corradini, P.; Cuneo, A.; Falanga, A.; Foà, R.; Gaidano, G.; Ghia, P.P.; Martelli, M.; Marasca, R.; Massaia, M.; et al. Practical management of ibrutinib in the real life: Focus on atrial fibrillation and bleeding. Hematol. Oncol. 2018, 36, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.W.; Ma, S.; Kipps, T.J.; Coutre, S.E.; Davids, M.S.; Eichhorst, B.; Hallek, M.; Byrd, J.C.; Humphrey, K.; Zhou, L.; et al. Efficacy of venetoclax in relapsed chronic lymphocytic leukemia is influenced by disease and response variables. Blood 2019, 134, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Seymour, J.F.; Kipps, T.J.; Eichhorst, B.; Hillmen, P.; D’Rozario, J.; Assouline, S.; Owen, C.; Gerecitano, J.; Robak, T.; De la Serna, J.; et al. Venetoclax-Rituximab in Relapsed or Refractory Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2018, 378, 1107–1120. [Google Scholar] [CrossRef]
- Fischer, K.; Al-Sawaf, O.; Bahlo, J.; Fink, A.M.; Tandon, M.; Dixon, M.; Robrecht, S.; Warburton, S.; Humphrey, K.; Samoylova, O.; et al. Venetoclax and Obinutuzumab in Patients with CLL and Coexisting Conditions. N. Engl. J. Med. 2019, 380, 2225–2236. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients Treated Frontline (n = 10) | Patients Treated beyond First Line (n = 36) | |
|---|---|---|
| Median age at diagnosis, years (range) | 63.2 (54.1–76.1) | 61.6 (32.6–79.2) |
| Male/female, n | 8/2 | 23/13 |
| Previous treatments, median (range) | NA | 1 (1–4) |
| Binet A, n (%) | 4 (40.0%) | 9 (25.0%) |
| Binet B, n (%) | 5 (50.0%) | 14 (38.9%) |
| Binet C, n (%) | 1 (10.0%) | 10 (27.8%) |
| Unavailable, n (%) | 0 | 3 (8.3%) |
| CIRS, median (range) | 5 (1–8) | 5 (0–16) |
| TP53mut, n (%) | 4 (40.0%) | 1 (2.8%) |
| del(17p), n (%) | 6 (60.0%) | 5 (13.9%) |
| IGHVunmut, n (%) | 5 (50.0%) | 12 (33.3%) |
| Patients Treated Frontline (n = 10) | Patients Treated beyond First Line (n = 36) | |
|---|---|---|
| Best response | ||
| - complete response | 1 (10.0%) | 1 (2.8%) |
| - partial response | 9 (90.0%) | 34 (94.4%) |
| PFS, median (months) | 28.8 | 21.1 |
| OS, median (years) | NR | 4.9 |
| Toxicity | Any Grade, n (%) | Grade ≥ 3, n (%) | Drug Correlation, n (%) | Dose Reduction, n (%) | Resolved, n (%) |
|---|---|---|---|---|---|
| Neutropenia | 10 (16.7) | 10 (16.7) | 10 (16.7) | 6 (10.0) | 9 (15.0) |
| Piastrinopenia | 4 (6.7) | 2 (3.3) | 3 (5.0) | 2 (3.3) | 3 (5.0) |
| Anemia | 3 (5.0) | 3 (5.0) | 3 (5.0) | - | 3 (5.0) |
| Ibrutinib as 2nd Line Onward | |||||
|---|---|---|---|---|---|
| This Study | Winqvist 2016 (14) | Ysebaert 2017 (15) | Pula 2020 (16) | van der Straten 2020 (17) | |
| N | 36 | 95 | 428 | 171 | 155 |
| Median age | 62 | 69 | 70 | 64 | 70 |
| TP53mut | 3% | 63% (*) | 45% (*) | NA | 6% |
| del(17p) | 14% | 25% | 17% | ||
| IGHVunmut | 33% | NA | NA | NA | NA |
| Best ORR | 97% | 84% | 89% | 77% | 67% |
| Best CR rate | 3% (**) | 3% | NA | 18% | 13% |
| Follow-up | 26 mos | 10 mos | 3 mos | 40 mos | 14 mos |
| PFS | Median 21 mos 87% at 1 year 44% at 2 years | Median NR 77% at 10 mos | NA | Median NR 61% at 4 years | Median NR 73% at 1 year |
| OS | Median 59 mos 100% at 1 year 92% at 2 years | Median NR 83% at 10 mos | NA | Median NR 65% at 4 years | Median NR 77% at 1 year |
| Frontline Ibrutinib | Ibrutinib as 2nd Line Onward | ||||||
|---|---|---|---|---|---|---|---|
| This Study | Byrd 2020 (4) | Burger 2020 (8) | Farooqui 2015 (10) | This Study | Byrd 2020 (4) | Munir 2019 (6) | |
| N | 10 | 31 | 136 | 35 | 36 | 101 | 195 |
| Median age | 63 | 71 | 73 | 62 | 62 | 64 | 67 |
| TP53mut | 40% | NA | 10% | 6% | 3% | NA | NA |
| del(17p) | 60% | 6% | 0 (*) | 94% | 14% | 34% | 32% |
| IGHVunmut | 50% | 48% | 43% | 63% | 33% | 78% | NA |
| Best ORR | 90% | 87% | 92% | 70% | 97% | 89% | 91% |
| Best CR rate | 10% | 35% | 30% | 12% | 3% | 10% | 11% |
| Follow-up | 24 mos | 87 mos | 60 mos | 24 mos | 26 mos | 82 mos | 65 mos |
| Median PFS | 29 mos | NR | NR | NR | 21 mos | 52 mos | 44 mos |
| Median OS | NR | NR | NR | NR | 59 mos | 92 mos | 68 mos |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Broccoli, A.; Argnani, L.; Morigi, A.; Nanni, L.; Casadei, B.; Pellegrini, C.; Stefoni, V.; Zinzani, P.L. Long-Term Efficacy and Safety of Ibrutinib in the Treatment of CLL Patients: A Real Life Experience. J. Clin. Med. 2021, 10, 5845. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245845
Broccoli A, Argnani L, Morigi A, Nanni L, Casadei B, Pellegrini C, Stefoni V, Zinzani PL. Long-Term Efficacy and Safety of Ibrutinib in the Treatment of CLL Patients: A Real Life Experience. Journal of Clinical Medicine. 2021; 10(24):5845. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245845
Chicago/Turabian StyleBroccoli, Alessandro, Lisa Argnani, Alice Morigi, Laura Nanni, Beatrice Casadei, Cinzia Pellegrini, Vittorio Stefoni, and Pier Luigi Zinzani. 2021. "Long-Term Efficacy and Safety of Ibrutinib in the Treatment of CLL Patients: A Real Life Experience" Journal of Clinical Medicine 10, no. 24: 5845. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245845