
Instrumental Evaluation of COVID-19 Related Dysautonomia in Non-Critically-Ill Patients: An Observational, Cross-Sectional Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
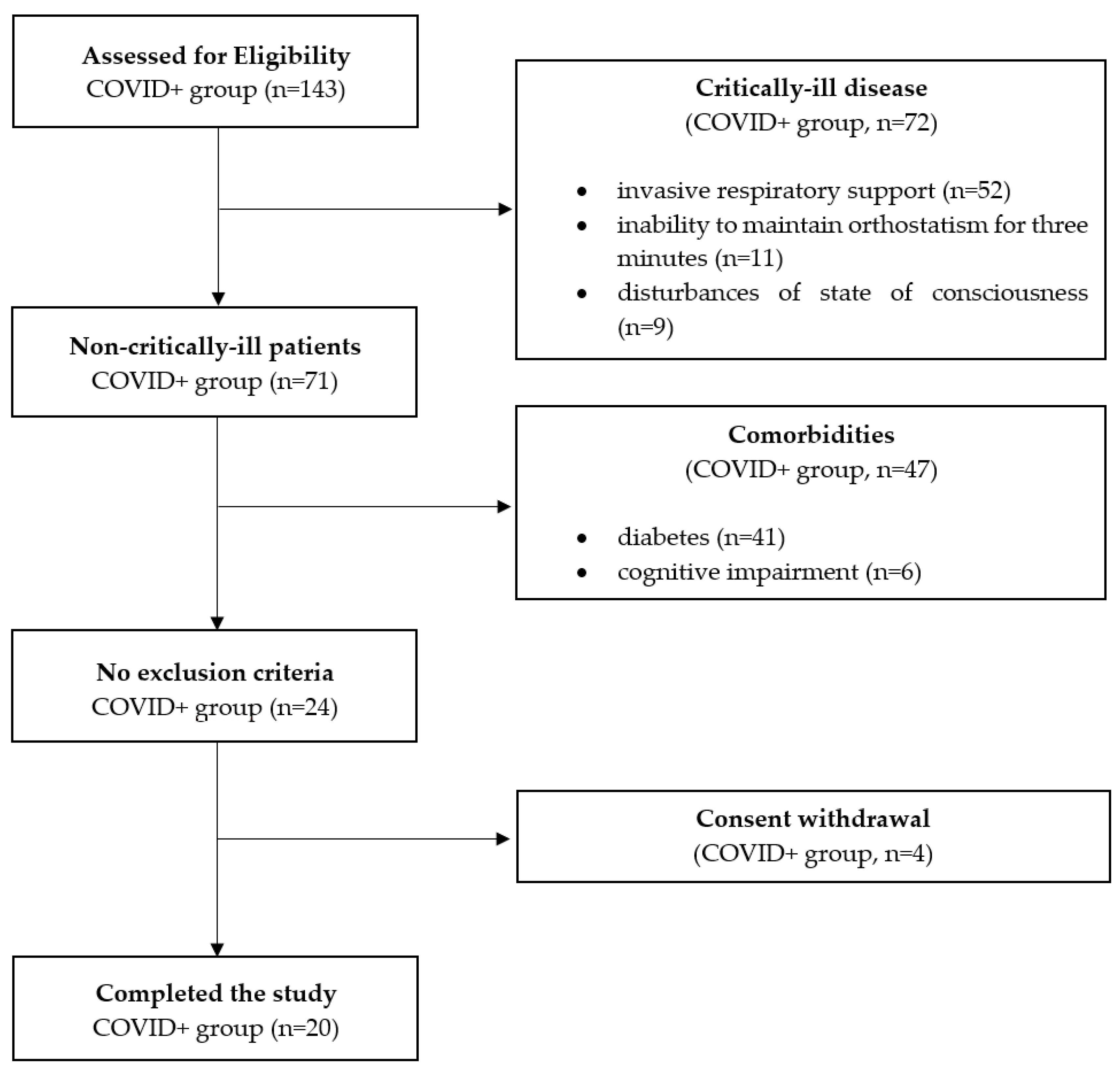
2.1. Study Design and Population
2.2. Control Group
2.3. Automated Pupillometry
2.4. Sudoscan
2.5. Heart Rate Variability
2.6. Pulse Transit Time
2.7. Statistical Analysis
3. Results
3.1. Pupillometry
3.2. Sudoscan
3.3. Heart Rate Variability
3.4. Pulse Transit Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Cantuti-Castelvetri, L.; Ojha, R.; Pedro, L.D.; Djannatian, M.; Franz, J.; Kuivanen, S.; Van Der Meer, F.; Kallio, K.; Kaya, T.; Anastasina, M.; et al. Neuropilin-1 facilitates SARS-CoV-2 cell entry and infectivity. Science 2020, 370, 856–860. [Google Scholar] [CrossRef] [PubMed]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S.; et al. Multiorgan and Renal Tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 590–592. [Google Scholar] [CrossRef] [PubMed]
- SSong, E.; Zhang, C.; Israelow, B.; Lu-Culligan, A.; Prado, A.V.; Skriabine, S.; Lu, P.; Weizman, O.-E.; Liu, F.; Dai, Y.; et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. J Exp Med. 2021, 218, e20202135. [Google Scholar] [CrossRef]
- Frisullo, G.; Scala, I.; Bellavia, S.; Broccolini, A.; Brunetti, V.; Morosetti, R.; Della Marca, G.; Calabresi, P. COVID-19 and stroke: From the cases to the causes. Rev. Neurosci. 2021, 32, 659–669. [Google Scholar] [CrossRef]
- Munz, M.; Wessendorf, S.; Koretsis, G.; Tewald, F.; Baegi, R.; Krämer, S.; Geissler, M.; Reinhard, M. Acute transverse myelitis after COVID-19 pneumonia. J. Neurol. 2020, 267, 2196–2197. [Google Scholar] [CrossRef]
- Zhao, H.; Shen, D.; Zhou, H.; Liu, J.; Chen, S. Guillain-Barré syndrome associated with SARS-CoV-2 infection: Causality or coincidence? Lancet Neurol. 2020, 19, 383–384. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Stella, A.B.; Furlanis, G.; Frezza, N.A.; Valentinotti, R.; Ajcevic, M.; Manganotti, P. Autonomic dysfunction in post-COVID patients with and witfhout neurological symptoms: A prospective multidomain observational study. J. Neurol. 2021, 1–10. [Google Scholar] [CrossRef]
- DDani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef]
- Sletten, D.M.; Suarez, G.A.; Low, P.A.; Mandrekar, J.; Singer, W. COMPASS 31: A Refined and Abbreviated Composite Autonomic Symptom Score. Mayo Clin. Proc. 2012, 87, 1196–1201. [Google Scholar] [CrossRef]
- Larson, M.D.; Behrends, M. Portable Infrared Pupillometry. Anesthesia Analg. 2015, 120, 1242–1253. [Google Scholar] [CrossRef]
- McDougal, D.H.; Gamlin, P.D. Autonomic Control of the Eye. Compr. Physiol. 2014, 5, 439–473. [Google Scholar] [CrossRef] [Green Version]
- Giza, E.; Fotiou, D.; Bostantjopoulou, S.; Katsarou, Z.; Karlovasitou, A. Pupil Light Reflex in Parkinson’s Disease: Evaluation With Pupillometry. Int. J. Neurosci. 2011, 121, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Bernabé-Ortiz, A.; Ticse, R.; Hernandez, A.; Huaylinos, Y.; Pinto, M.E.; Málaga, G.; Checkley, W.; Gilman, R.H.; Miranda, J.J.; et al. Type 2 diabetes and cardiac autonomic neuropathy screening using dynamic pupillometry. Diabet. Med. 2015, 32, 1470–1478. [Google Scholar] [CrossRef]
- Monaco, A.; Cattaneo, R.; Mesin, L.; Fiorucci, E.; Pietropaoli, D. Evaluation of autonomic nervous system in sleep apnea patients using pupillometry under occlusal stress: A pilot study. CRANIO® 2014, 32, 139–147. [Google Scholar] [CrossRef]
- Brunswick, P.; Mayaudon, H.; Albin, V.; Lair, V.; Ringuede, A.; Cassir, M. Use of Ni electrodes chronoamperometry for improved diagnostics of diabetes and cardiac diseases. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; Volume 2007, pp. 4544–4547. [Google Scholar] [CrossRef]
- Chizmadzhev, Y.A.; Indenbom, A.V.; Kuzmin, P.I.; Galichenko, S.; Weaver, J.C.; Potts, R.O. Electrical Properties of Skin at Moderate Voltages: Contribution of Appendageal Macropores. Biophys. J. 1998, 74, 843–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casellini, C.M.; Parson, H.K.; Richardson, M.S.; Nevoret, M.L.; Vinik, A.I. Sudoscan, a Noninvasive Tool for Detecting Diabetic Small Fiber Neuropathy and Autonomic Dysfunction. Diabetes Technol. Ther. 2013, 15, 948–953. [Google Scholar] [CrossRef] [Green Version]
- Luigetti, M.; Primiano, G.; Cuccagna, C.; Bernardo, D.; Sauchelli, D.; Vollono, C.; Servidei, S. Small fibre neuropathy in mitochondrial diseases explored with sudoscan. Clin. Neurophysiol. 2018, 129, 1618–1623. [Google Scholar] [CrossRef]
- Luigetti, M.; Bisogni, G.; Romano, A.; Di Paolantonio, A.; Barbato, F.; Primicerio, G.; Rossini, P.M.; Servidei, S.; Sabatelli, M. Sudoscan in the evaluation and follow-up of patients and carriers with TTR mutations: Experience from an Italian Centre. Amyloid 2018, 25, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, C.; Placidi, F.; Del Bianco, C.; Liguori, C.; Pisani, A.; Mercuri, N.B.; Izzi, F. Autonomic symptoms, cardiovascular and sudomotor evaluation in de novo type 1 narcolepsy. Clin. Auton. Res. 2020, 30, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Electrophysiology TFotESoCtNASoP. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Smith, R.P.; Argod, J.; Pépin, J.L.; Lévy, P. Pulse transit time: An appraisal of potential clinical applications. Thorax 1999, 54, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Grote, L.; Sommermeyer, D.; Zou, D.; Eder, D.N.; Hedner, J. Oximeter-Based Autonomic State Indicator Algorithm for Cardiovascular Risk Assessment. Chest 2011, 139, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Olson, D.M.; Fishel, M. The Use of Automated Pupillometry in Critical Care. Crit. Care Nurs. Clin. N. Am. 2016, 28, 101–107. [Google Scholar] [CrossRef]
- Chen, J.; Gombart, Z.; Rogers, S.; Gardiner, S.; Cecil, S.; Bullock, R. Pupillary reactivity as an early indicator of increased intracranial pressure: The introduction of the neurological pupil index. Surg. Neurol. Int. 2011, 2, 82. [Google Scholar] [CrossRef] [Green Version]
- Mayaudon, H.; Miloche, P.-O.; Bauduceau, B. A new simple method for assessing sudomotor function: Relevance in type 2 diabetes. Diabetes Metab. 2010, 36, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Krieger, S.-M.; Reimann, M.; Haase, R.; Henkel, E.; Hanefeld, M.; Ziemssen, T. Sudomotor Testing of Diabetes Polyneuropathy. Front. Neurol. 2018, 9, 803. [Google Scholar] [CrossRef] [PubMed]
- Vinik, A.I.; Nevoret, M.-L.; Casellini, C.M. The New Age of Sudomotor Function Testing: A Sensitive and Specific Biomarker for Diagnosis, Estimation of Severity, Monitoring Progression, and Regression in Response to Intervention. Front. Endocrinol. 2015, 6, 94. [Google Scholar] [CrossRef] [Green Version]
- NNiskanen, J.-P.; Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P.A. Software for advanced HRV analysis. Comput. Methods Programs Biomed. 2004, 76, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Electrophysiology TFotESoCtNASoP. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Ding, X.; Zhang, Y. Pulse transit time technique for cuffless unobtrusive blood pressure measurement: From theory to algorithm. Biomed. Eng. Lett. 2019, 9, 37–52. [Google Scholar] [CrossRef]
- Opic, P.; Rüegg, S.; Marsch, S.; Gut, S.S.; Sutter, R. Automated Quantitative Pupillometry in the Critically Ill. Neurol. 2021, 97, e629–e642. [Google Scholar] [CrossRef]
- Vrettou, C.S.; Korompoki, E.; Sarri, K.; Papachatzakis, I.; Theodorakopoulou, M.; Chrysanthopoulou, E.; Andrianakis, I.A.; Routsi, C.; Zakynthinos, S.; Kotanidou, A. Pupillometry in critically ill patients with COVID-19: A prospective study. Clin. Auton. Res. 2020, 30, 563–565. [Google Scholar] [CrossRef] [PubMed]
- Battaglini, D.; Santori, G.; Chandraptham, K.; Iannuzzi, F.; Bastianello, M.; Tarantino, F.; Ball, L.; Giacobbe, D.R.; Vena, A.; Bassetti, M.; et al. Neurological Complications and Noninvasive Multimodal Neuromonitoring in Critically Ill Mechanically Ventilated COVID-19 Patients. Front. Neurol. 2020, 11, 602114. [Google Scholar] [CrossRef] [PubMed]
- Karahan, M.; Demirtaş, A.A.; Hazar, L.; Erdem, S.; Ava, S.; Dursun, M.E.; Keklikçi, U. Autonomic dysfunction detection by an automatic pupillometer as a non-invasive test in patients recovered from COVID-19. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 2821–2826. [Google Scholar] [CrossRef]
- Hinduja, A.; Moutairou, A.; Calvet, J.-H. Sudomotor dysfunction in patients recovered from COVID-19. Neurophysiol. Clin. Neurophysiol. 2021, 51, 193–196. [Google Scholar] [CrossRef]
- Aragón-Benedí, C.; Oliver-Forniés, P.; Galluccio, F.; Altinpulluk, E.Y.; Ergonenc, T.; Allam, A.E.S.; Salazar, C.; Fajardo-Pérez, M. Is the heart rate variability monitoring using the analgesia nociception index a predictor of illness severity and mortality in critically ill patients with COVID-19? A pilot study. PLoS ONE 2021, 16, e0249128. [Google Scholar] [CrossRef]
- Pan, Y.; Yu, Z.; Yuan, Y.; Han, J.; Wang, Z.; Chen, H.; Wang, S.; Wang, Z.; Hu, H.; Zhou, L.; et al. Alteration of Autonomic Nervous System Is Associated With Severity and Outcomes in Patients With COVID-19. Front. Physiol. 2021, 12, 630038. [Google Scholar] [CrossRef]
- Hasty, F.; García, G.; Dávila, C.H.; Wittels, S.H.; Hendricks, S.; Chong, S. Heart Rate Variability as a Possible Predictive Marker for Acute Inflammatory Response in COVID-19 Patients. Mil. Med. 2021, 186, e34–e38. [Google Scholar] [CrossRef]
- Pavlov, V.; Tracey, K.J. Neural regulation of immunity: Molecular mechanisms and clinical translation. Nat. Neurosci. 2017, 20, 156–166. [Google Scholar] [CrossRef]
- Szeghy, R.E.; Province, V.M.; Stute, N.L.; Augenreich, M.A.; Koontz, L.K.; Stickford, J.L.; Stickford, A.S.L.; Ratchford, S.M. Carotid stiffness, intima–media thickness and aortic augmentation index among adults with SARS-CoV-2. Exp. Physiol. 2021. [Google Scholar] [CrossRef]
- Schnaubelt, S.; Oppenauer, J.; Tihanyi, D.; Mueller, M.; Maldonado-Gonzalez, E.; Zejnilovic, S.; Haslacher, H.; Perkmann, T.; Strassl, R.; Anders, S.; et al. Arterial stiffness in acute COVID-19 and potential associations with clinical outcome. J. Intern. Med. 2021, 290, 437–443. [Google Scholar] [CrossRef]
- Sabharwal, R.; Zhang, Z.; Lu, Y.; Abboud, F.; Russo, A.; Chapleau, M.W. Receptor Activity-Modifying Protein 1 Increases Baroreflex Sensitivity and Attenuates Angiotensin-Induced Hypertension. Hypertens 2010, 55, 627–635. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Clinical Features | COVID+ (n = 20) | COVID− (n = 20) | |
|---|---|---|---|
| Male sex | n (%) | 14 (70%) | 13 (65%) |
| Age—years | Mean ± SD | 56.05 ± 19.15 | 52.55 ± 13.71 |
| BMI | Mean ± SD | 25.75 ± 3.86 | 26.40 ± 3.39 |
| COVID symptoms | |||
| Dyspnoea | n (%) | 15 (75%) | 0 (0%) |
| Fever at time of evaluation | n (%) | 0 (0%) | 0 (0%) |
| Diarrhoea | n (%) | 10 (50%) | 3 (15%) |
| Dizziness | n (%) | 12 (60%) | 1 (5%) |
| Pneumonia | n (%) | 14 (70%) | 0 (0%) |
| ∆ symptoms onset-registration time | Median (IQR) | 6 (4–8) | |
| Comorbidities | |||
| Hypertension | n (%) | 10 (50%) | 7 (35%) |
| Heart disease | n (%) | 4 (20%) | 1 (5%) |
| Dysthyroidism | n (%) | 1 (5%) | 2 (10%) |
| Renal failure | n (%) | 1 (5%) | 0 (0%) |
| Ocular disease | n (%) | 0 (0%) | 2 (10%) |
| Pharmacological Treatments | COVID+ (n = 20) | COVID− (n = 20) |
|---|---|---|
| α-blockers, n (%) | 0 (0%) | 1 (5%) |
| β-blockers, n (%) | 5 (25%) | 3 (15%) |
| ACE-inhibitors, n (%) | 1 (5%) | 2 (10%) |
| Sartans, n (%) | 6 (30%) | 1 (5%) |
| Calcium channel blockers, n (%) | 3 (15%) | 1 (5%) |
| Antiarrhythmics, n (%) | 0 (0%) | 0 (0%) |
| Antiepileptic drugs, n (%) | 0 (0%) | 1 (5%) |
| Antidepressants, n (%) | 1 (5%) | 0 (0%) |
| Antipsychotics, n (%) | 1 (5%) | 0 (0%) |
| Hypnotic drugs, n (%) | 2 (10%) | 3 (15%) |
| COVID+ (n = 20) | COVID− (n = 20) | Mann-Whitney | Pearson’s χ2 | ||||
|---|---|---|---|---|---|---|---|
| PUPILLOMETRY | U-Test | p | Test | p | |||
| Sympathetic parameters | |||||||
| Dilatation velocity (mm/s) | Median (IQR) | 1.1 (1.0–1.3) | 0.9 (0.8–1.2) | 276.000 | 0.040 | ||
| Parasympathetic parameters | |||||||
| Reflex latency (ms) | Median (IQR) | 240 (215–250) | 233 (211–250) | 220.000 | 0.581 | ||
| Constriction velocity (mm/s) | Median (IQR) | 2.3 (1.9–2.7) | 2.1 (1.7–2.7) | 250.00 | 0.176 | ||
| Maximum constriction velocity (mm/s) | Median (IQR) | 3.7 (3.2–4.4) | 3.1 (2.8–4.4) | 241.000 | 0.267 | ||
| Minimum pupil diameter (mm) | Median (IQR) | 2.8 (2.5–3.1) | 2.6 (2.2–2.7) | 259.500 | 0.107 | ||
| Absolute constriction amplitude (mm) | Median (IQR) | 1.4 (1.1–1.9) | 1.0 (0.9–1.5) | 277.000 | 0.037 | ||
| Constriction index (%) | Median (IQR) | 34.0 (30.3–37.3) | 30.5 (25.0–34.0) | 276.000 | 0.040 | ||
| Mixed parameters | |||||||
| Baseline pupil diameter (mm) | Median (IQR) | 4.2 (3.6–4.7) | 3.7 (3.1–4.1) | 276.500 | 0.039 | ||
| Neuro-pupillary index | Median (IQR) | 4.4 (4.1–4.6) | 4.5 (4.2–4.6) | 172.000 | 0.445 | ||
| Neuro-pupillary index < 3 | n (%) | 0 (0%) | 1 (5%) | 1.026 | 0.500 | ||
| COVID+ (n = 20) | COVID− (n = 20) | t-Test | Pearson’s χ2 | ||||
|---|---|---|---|---|---|---|---|
| SUDOSCAN | t-Test | p | Test | p | |||
| Hands | |||||||
| Mean ESC hands | mean ± SD | 66.5 ± 17.3 | 70.3 ± 13.4 | 0.767 | 0.448 | ||
| Mean ESC right hand | mean ± SD | 66.8 ± 17.4 | 69.1 ± 12.9 | 0.485 | 0.631 | ||
| Mean ESC left hand | mean ± SD | 66.6 ± 17.9 | 68.9 ± 14.6 | 0.437 | 0.665 | ||
| Sudomotor impairment | |||||||
| ESC hands < 60 mcs | n (%) | 6 (30%) | 5 (25%) | 0.125 | 0.723 | ||
| ESC right hand < 60 mcs | n (%) | 6 (30%) | 4 (20%) | 0.533 | 0.465 | ||
| ESC left hand < 60 mcs | n (%) | 7 (35%) | 6 (30%) | 0.114 | 0.736 | ||
| Feet | |||||||
| Mean ESC feet | mean ± SD | 67.5 ± 22.3 | 76.8 ± 11.8 | 1.647 | 0.108 | ||
| Mean ESC right foot | mean ± SD | 68.8 ± 21.9 | 75.0 ± 19.2 | 0.945 | 0.351 | ||
| Mean ESC left foot | mean ± SD | 69.0 ± 23.9 | 76.8 ± 12.0 | 1.294 | 0.204 | ||
| Sudomotor impairment | |||||||
| ESC feet < 70 mcs | n (%) | 9 (45%) | 3 (15%) | 4.286 | 0.038 | ||
| ESC right foot < 70 mcs | n (%) | 8 (40%) | 4 (20%) | 1.905 | 0.168 | ||
| ESC left foot < 70 mcs | n (%) | 8 (40%) | 3 (15%) | 3.135 | 0.077 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellavia, S.; Scala, I.; Luigetti, M.; Brunetti, V.; Gabrielli, M.; Zileri Dal Verme, L.; Servidei, S.; Calabresi, P.; Frisullo, G.; Della Marca, G. Instrumental Evaluation of COVID-19 Related Dysautonomia in Non-Critically-Ill Patients: An Observational, Cross-Sectional Study. J. Clin. Med. 2021, 10, 5861. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245861
Bellavia S, Scala I, Luigetti M, Brunetti V, Gabrielli M, Zileri Dal Verme L, Servidei S, Calabresi P, Frisullo G, Della Marca G. Instrumental Evaluation of COVID-19 Related Dysautonomia in Non-Critically-Ill Patients: An Observational, Cross-Sectional Study. Journal of Clinical Medicine. 2021; 10(24):5861. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245861
Chicago/Turabian StyleBellavia, Simone, Irene Scala, Marco Luigetti, Valerio Brunetti, Maurizio Gabrielli, Lorenzo Zileri Dal Verme, Serenella Servidei, Paolo Calabresi, Giovanni Frisullo, and Giacomo Della Marca. 2021. "Instrumental Evaluation of COVID-19 Related Dysautonomia in Non-Critically-Ill Patients: An Observational, Cross-Sectional Study" Journal of Clinical Medicine 10, no. 24: 5861. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10245861