Impact of Chronic Kidney Disease on Chronic Total Occlusion Revascularization Outcomes: A Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Methods
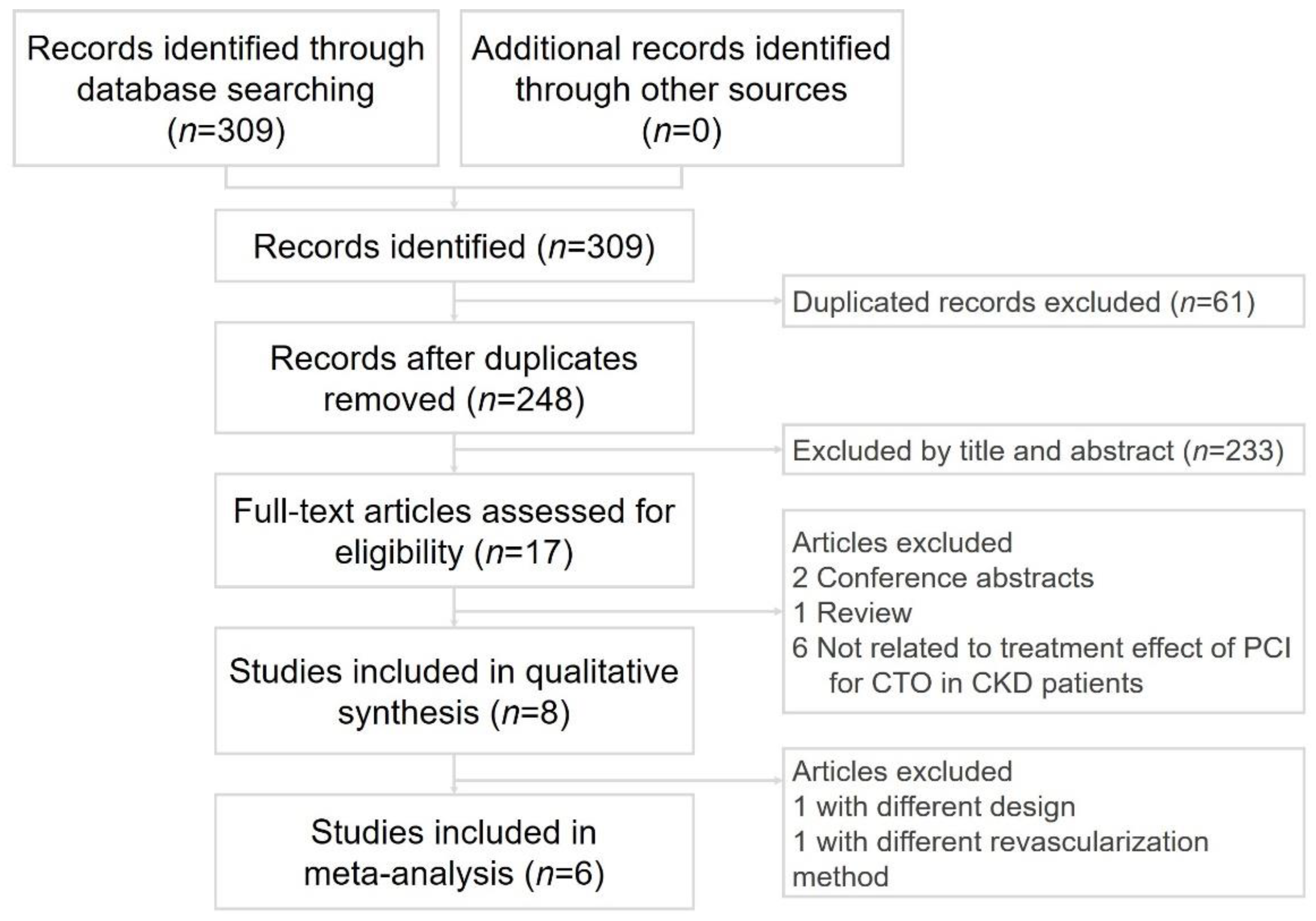
2.1. Search Strategies, Trial Selection, and Quality Assessment and Data Extraction
2.2. Definitions
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Patient Demographics and CTO Target Vessel
3.3. Pooled ORs of CIN, AKI, or RRT after PCI
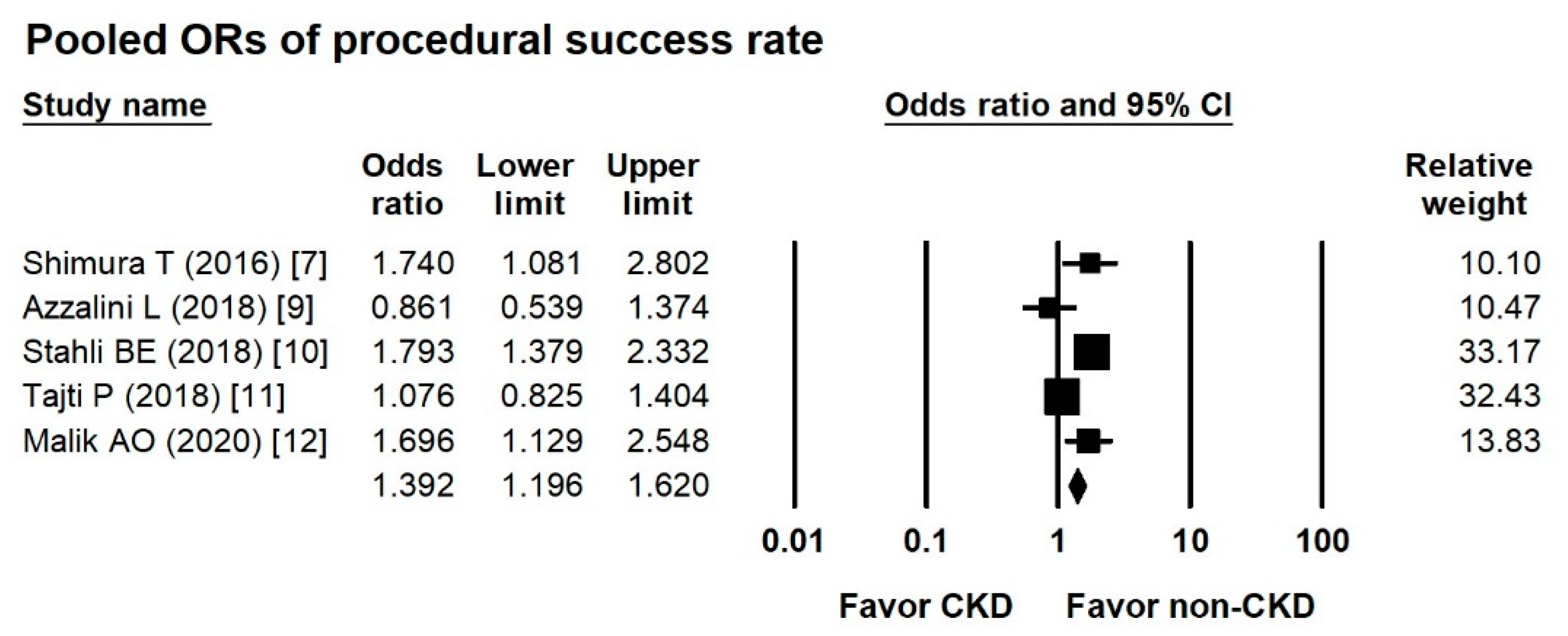
3.4. Pooled ORs of Procedural Success Rate between Groups
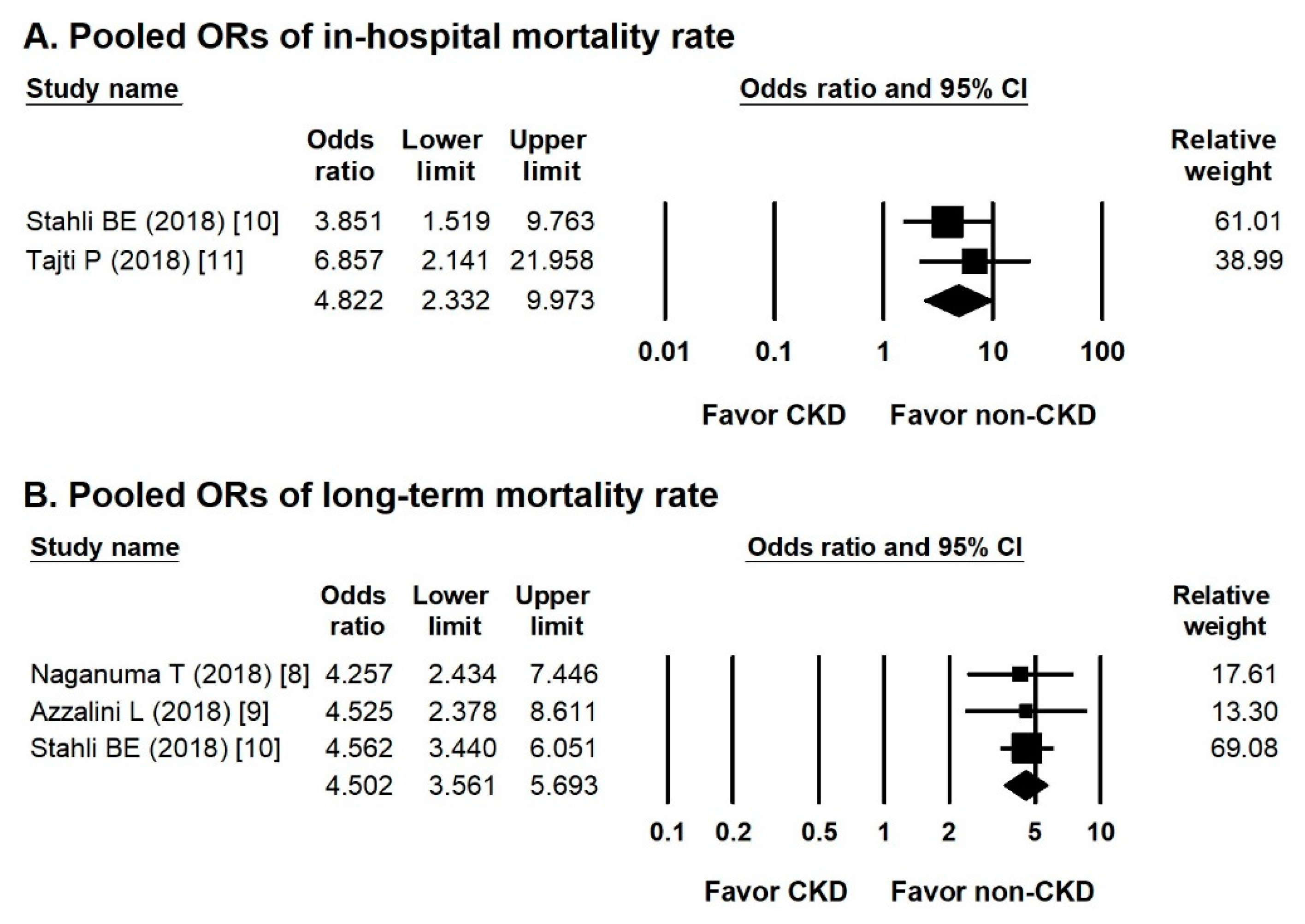
3.5. Pooled ORs of in-Hospital and Long-Term Mortality Rates
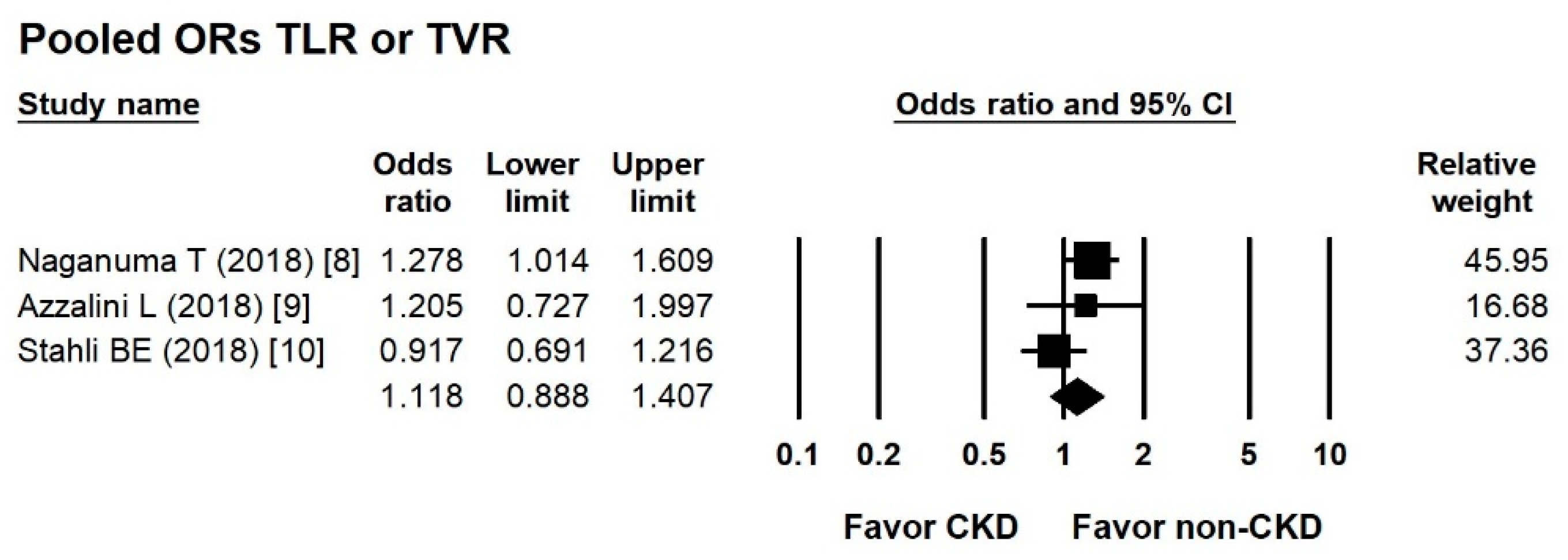
3.6. Pooled ORs of TLR or TVR between Groups
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| CKD | chronic kidney disease |
| CTO | chronic total occlusion |
| PCI | percutaneous coronary intervention |
| TIMI | Thrombolysis In Myocardial Infarction |
| eGFR | estimated glomerular filtration rate |
| CIN | contrast-induced nephropathy |
| AKI | acute kidney injury |
| RRT | renal replacement therapy |
| RCA | right coronary artery |
| LM | left main |
| LCX | left circumflex |
| J-CTO | Japan CTO |
| OR | odds ratio |
| TLR | target lesion revascularization |
| TVR | target vessel revascularization |
References
- George, S.; Cockburn, J.; Clayton, T.C.; Ludman, P.; Cotton, J.; Spratt, J.; Redwood, S.; de Belder, M.; de Belder, A.; Hill, J.; et al. Long-term follow-up of elective chronic total coronary occlusion angioplasty: Analysis from the U.K. Central Cardiac Audit Database. J. Am. Coll. Cardiol. 2014, 64, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujadas, S.; Martin, V.; Rosselló, X.; Carreras, F.; Barros, A.; Leta, R.; Alomar, X.; Cinca, J.; Sabate, M.; Pons-Llado, G. Improvement of myocardial function and perfusion after successful percutaneous revascularization in patients with chronic total coronary occlusion. Int. J. Cardiol. 2013, 169, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Pujadas, S.; Serra, A.; Bajo, E.; Carreras, F.; Barros, A.; Cinca, J.; Pons-Lladó, G.; Vaquerizo, B. Assessment of Inducible Myocardial Ischemia, Quality of Life, and Functional Status After Successful Percutaneous Revascularization in Patients with Chronic Total Coronary Occlusion. Am. J. Cardiol. 2016, 117, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Peri-Okonny, P.A.; Spertus, J.A.; Grantham, J.A.; Gosch, K.; Kirtane, A.; Sapontis, J.; Lombardi, W.; Karmpaliotis, D.; Moses, J.; Nicholson, W.; et al. Physical Activity After Percutaneous Coronary Intervention for Chronic Total Occlusion and Its Association With Health Status. J. Am. Heart Assoc. 2019, 8, e011629. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Liu, Y.H.; Chen, J.Y.; Tan, N.; Zhou, Y.L.; Li, H.L.; Guo, W.; Duan, C.Y.; Chen, P.Y. A simple pre-procedural risk score for contrast-induced nephropathy among patients with chronic total occlusion undergoing percutaneous coronary intervention. Int. J. Cardiol. 2015, 180, 69–71. [Google Scholar] [CrossRef] [Green Version]
- Aguiar-Souto, P.; Ferrante, G.; Del Furia, F.; Barlis, P.; Khurana, R.; Di Mario, C. Frequency and predictors of contrast-induced nephropathy after angioplasty for chronic total occlusions. Int. J. Cardiol. 2010, 139, 68–74. [Google Scholar] [CrossRef]
- Shimura, T.; Yamamoto, M.; Tsuchikane, E.; Teramoto, T.; Kimura, M.; Matsuo, H.; Kawase, Y.; Suzuki, Y.; Kano, S.; Habara, M.; et al. Rates of future hemodialysis risk and beneficial outcomes for patients with chronic kidney disease undergoing recanalization of chronic total occlusion. Int. J. Cardiol. 2016, 222, 707–713. [Google Scholar] [CrossRef]
- Naganuma, T.; Tsujita, K.; Mitomo, S.; Ishiguro, H.; Basavarajaiah, S.; Sato, K.; Kobayashi, T.; Obata, J.; Nagamatsu, S.; Yamanaga, K.; et al. Impact of Chronic Kidney Disease on Outcomes After Percutaneous Coronary Intervention for Chronic Total Occlusions (from the Japanese Multicenter Registry). Am. J. Cardiol. 2018, 121, 1519–1523. [Google Scholar] [CrossRef]
- Azzalini, L.; Ojeda, S.; Demir, O.M.; Dens, J.; Tanabe, M.; La Manna, A.; Benincasa, S.; Bellini, B.; Poletti, E.; Maccagni, D.; et al. Recanalization of Chronic Total Occlusions in Patients with vs. Without Chronic Kidney Disease: The Impact of Contrast-Induced Acute Kidney Injury. Can. J. Cardiol. 2018, 34, 1275–1282. [Google Scholar] [CrossRef]
- Stähli, B.E.; Gebhard, C.; Gick, M.; Ferenc, M.; Mashayekhi, K.; Buettner, H.J.; Neumann, F.J.; Toma, A. Outcomes after percutaneous coronary intervention for chronic total occlusion according to baseline renal function. Clin. Res. Cardiol. 2018, 107, 259–267. [Google Scholar] [CrossRef]
- Tajti, P.; Karatasakis, A.; Danek, B.A.; Alaswad, K.; Karmpaliotis, D.; Jaffer, F.A.; Choi, J.W.; Yeh, R.W.; Patel, M.; Mahmud, E.; et al. In-Hospital Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention in Patients with Chronic Kidney Disease. J. Invasive Cardiol. 2018, 30, E113–E121. [Google Scholar] [PubMed]
- Malik, A.O.; Spertus, J.A.; Grantham, J.A.; Peri-Okonny, P.; Gosch, K.; Sapontis, J.; Moses, J.; Lombardi, W.; Karmpaliotis, D.; Nicholson, W.J.; et al. Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention in Patients with Renal Dysfunction. Am. J. Cardiol. 2020, 125, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Di Mario, C.; Werner, G.S.; Sianos, G.; Galassi, A.R.; Büttner, J.; Dudek, D.; Chevalier, B.; Lefevre, T.; Schofer, J.; Koolen, J.; et al. European perspective in the recanalisation of Chronic Total Occlusions (CTO): Consensus document from the EuroCTO Club. EuroIntervention 2007, 3, 30–43. [Google Scholar] [PubMed]
- Sianos, G.; Werner, G.S.; Galassi, A.R.; Papafaklis, M.I.; Escaned, J.; Hildick-Smith, D.; Christiansen, E.H.; Gershlick, A.; Carlino, M.; Karlas, A.; et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention 2012, 8, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Bailie, G.R.; Uhlig, K.; Levey, A.S. Clinical practice guidelines in nephrology: Evaluation, classification, and stratification of chronic kidney disease. Pharmacotherapy 2005, 25, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Stacul, F.; van der Molen, A.J.; Reimer, P.; Webb, J.A.; Thomsen, H.S.; Morcos, S.K.; Almén, T.; Aspelin, P.; Bellin, M.F.; Clement, O.; et al. Contrast induced nephropathy: Updated ESUR Contrast Media Safety Committee guidelines. Eur. Radiol. 2011, 21, 2527–2541. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, A.N.; Jones, D.A.; Sirker, A.; Mathur, A.; Smith, E.J. Prevention of contrast-induced acute kidney injury after percutaneous coronary intervention for chronic total coronary occlusions. Am. J. Cardiol. 2015, 115, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Wilson, W.; Smith, W.; McEntegart, M.; Oldroyd, K.; Sidik, N.; Bagnall, A.; Egred, M.; Irving, J.; Strange, J.; et al. Comparison of Characteristics and Complications in Men Versus Women Undergoing Chronic Total Occlusion Percutaneous Intervention. Am. J. Cardiol. 2017, 119, 535–541. [Google Scholar] [CrossRef] [Green Version]
- Donfrancesco, C.; Palleschi, S.; Palmieri, L.; Rossi, B.; Noce, C.L.; Pannozzo, F.; Spoto, B.; Tripepi, G.; Zoccali, C.; Giampaoli, S. Estimated Glomerular Filtration Rate, All-Cause Mortality and Cardiovascular Diseases Incidence in a Low Risk Population: The MATISS Study. PLoS ONE 2013, 8, e78475. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Jia, J.; Li, Z.; Pan, H.; Wang, A.; Guo, X.; Wu, S.; Zhao, X. Association of estimated glomerular filtration rate and proteinuria with all-cause mortality in community-based population in China: A Result from Kailuan Study. Sci. Rep. 2018, 8, 2157. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Kang, J.; Lee, E.; Hwang, D.; Rhee, T.M.; Park, J.; Kim, H.L.; Lee, S.E.; Han, J.K.; Yang, H.M.; et al. Chronic Kidney Disease in the Second-Generation Drug-Eluting Stent Era: Pooled Analysis of the Korean Multicenter Drug-Eluting Stent Registry. JACC Cardiovasc. Interv. 2016, 9, 2097–2109. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) | The Definition of Procedural Success | Procedural Successful Rate (CKD vs. Non-CKD) |
|---|---|---|
| Shimura T. (2016) [7] | TIMI flow grade 3 and a residual stenosis of ≤50% and without MACE | 83.1% vs. 89.5% |
| Naganuma T. (2018) [8] | N/A | N/A |
| Azzalini L. (2018) [9] | TIMI flow grade = 3 and a residual stenosis < 30% | 79% vs. 86% |
| Stahli B.E. (2018) [10] | TIMI flow grade = 3 and a residual stenosis < 30% | 75.8% vs. 84.9% |
| Tajti P. (2018) [11] | TIMI flow grade = 3 and a residual stenosis < 30% | 83.0% vs. 84.0 |
| Malik A.O. (2020) [12] | TIMI flow grade ≥ 2 and a residual stenosis < 50% and no side branch occlusion | 81.8% vs. 88.4% |
| First Author (Year) | Patients Number (Female %) | Age (Years) | Study Period | The Prevalence of CKD (%) | Comparison of Groups | Follow-Up |
|---|---|---|---|---|---|---|
| Shimura T. (2016) [7] | 739 (16.6) | 65.9 ± 10.8 | January 2006–December 2013 | 24.0 | CKD PCI (177) vs. non-CKD PCI (562) | 4.3 ± 2.4 years |
| Naganuma T. (2018) [8] | 1463 (17.4) | 66.6 ± 10.4 | August 2004–December 2014 | 37.9 | CKD PCI (555) vs. non-CKD PCI (908) | 4.6 (2.3–6.7) years |
| Azzalini L. (2018) [9] | 1092 (10.6) | 64.9 ± 10.3 | July 2011–June 2017 | 19.6 | CKD PCI (214) vs. non-CKD PCI (878) | 1.3 (0.9–3.1) years |
| Stahli B.E. (2018) [10] | 2002 (16.6) | 65.9 ± 8.6 | January 2005–December 2013 | 20.9 | CKD PCI (418) vs. non-CKD PCI (1584) | 2.6 (1.1–3.1) years |
| Tajti P. (2018) [11] | 1979 (14.4) | 65.0 ± 10.0 | May 2012–November 2017 | 27.0 | CKD PCI (535) vs. non-CKD PCI (1444) | In-hospital |
| Malik A.O. (2020) [12] | 957 (19.4) | 65.3 ± 10.3 | January 2014–July 2015 | 23.6 | CKD PCI (225) vs. non-CKD PCI (732) | 1 year |
| CKD | Non-CKD | p Value | |
|---|---|---|---|
| Age (years) | 70.6 ± 8.9 (2124) | 63.9 ± 9.4 (6108) | <0.001 |
| Female sex (%) | 20.4 (434) | 14.1 (862) | <0.001 |
| Diabetes mellitus (%) | 46.3 (983) | 33.3 (2036) | <0.001 |
| Heart failure (%) | 39.1 (545) | 22.1 (1025) | <0.001 |
| LVEF (%) | 49.3 ± 13.8 (1529) | 52.8 ± 12.6 (3962) | <0.001 |
| Previous CABG (%) | 30.3 (475) | 19.9 (1033) | <0.001 |
| eGFR (mL/min/1.73m2) | 40.7 ± 17.4 (2124) | 85.1 ± 16.3 (6108) | <0.001 |
| J-CTO score | 2.4 ± 1.3 (995) | 2.2 ± 1.3 (3094) | <0.001 |
| Procedure time (mins) | 139.2 ± 69.3 (1172) | 130.9 ± 71.9 (3656) | <0.001 |
| Fluoroscopy time (mins) | 43.0 ± 27.7 (1413) | 39.1 ± 26.7 (4678) | <0.001 |
| Contrast volume (mL) | 255.4 ± 106.7 (1590) | 285.0 ± 116.3 (5240) | <0.001 |
| Retrograde wire escalation and retrograde dissection and reentry (%) | 30.0 (395) | 29.0 (1358) | 0.701 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, W.-C.; Wu, P.-J.; Fang, C.-Y.; Chen, H.-C.; Wu, C.-J.; Fang, H.-Y. Impact of Chronic Kidney Disease on Chronic Total Occlusion Revascularization Outcomes: A Meta-Analysis. J. Clin. Med. 2021, 10, 440. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030440
Lee W-C, Wu P-J, Fang C-Y, Chen H-C, Wu C-J, Fang H-Y. Impact of Chronic Kidney Disease on Chronic Total Occlusion Revascularization Outcomes: A Meta-Analysis. Journal of Clinical Medicine. 2021; 10(3):440. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030440
Chicago/Turabian StyleLee, Wei-Chieh, Po-Jui Wu, Chih-Yuan Fang, Huang-Chung Chen, Chiung-Jen Wu, and Hsiu-Yu Fang. 2021. "Impact of Chronic Kidney Disease on Chronic Total Occlusion Revascularization Outcomes: A Meta-Analysis" Journal of Clinical Medicine 10, no. 3: 440. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030440