
Effects of Methylprednisolone on Ventilator-Free Days in Mechanically Ventilated Patients with Acute Respiratory Distress Syndrome and COVID-19: A Retrospective Study

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Outcome Measures
2.2. Clinical and Laboratory Data
2.3. Statistical Analysis
3. Results
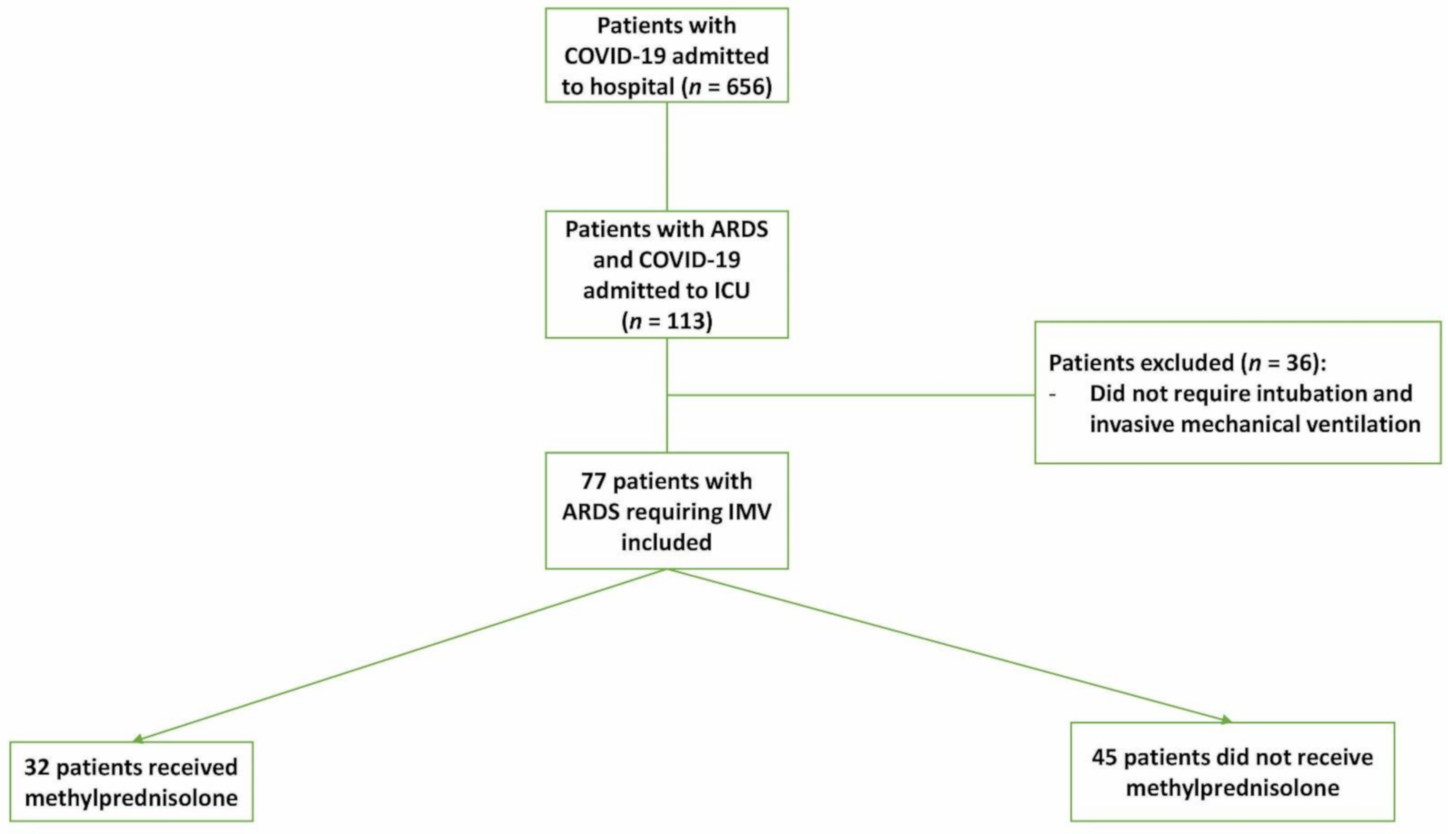
3.1. Study Population
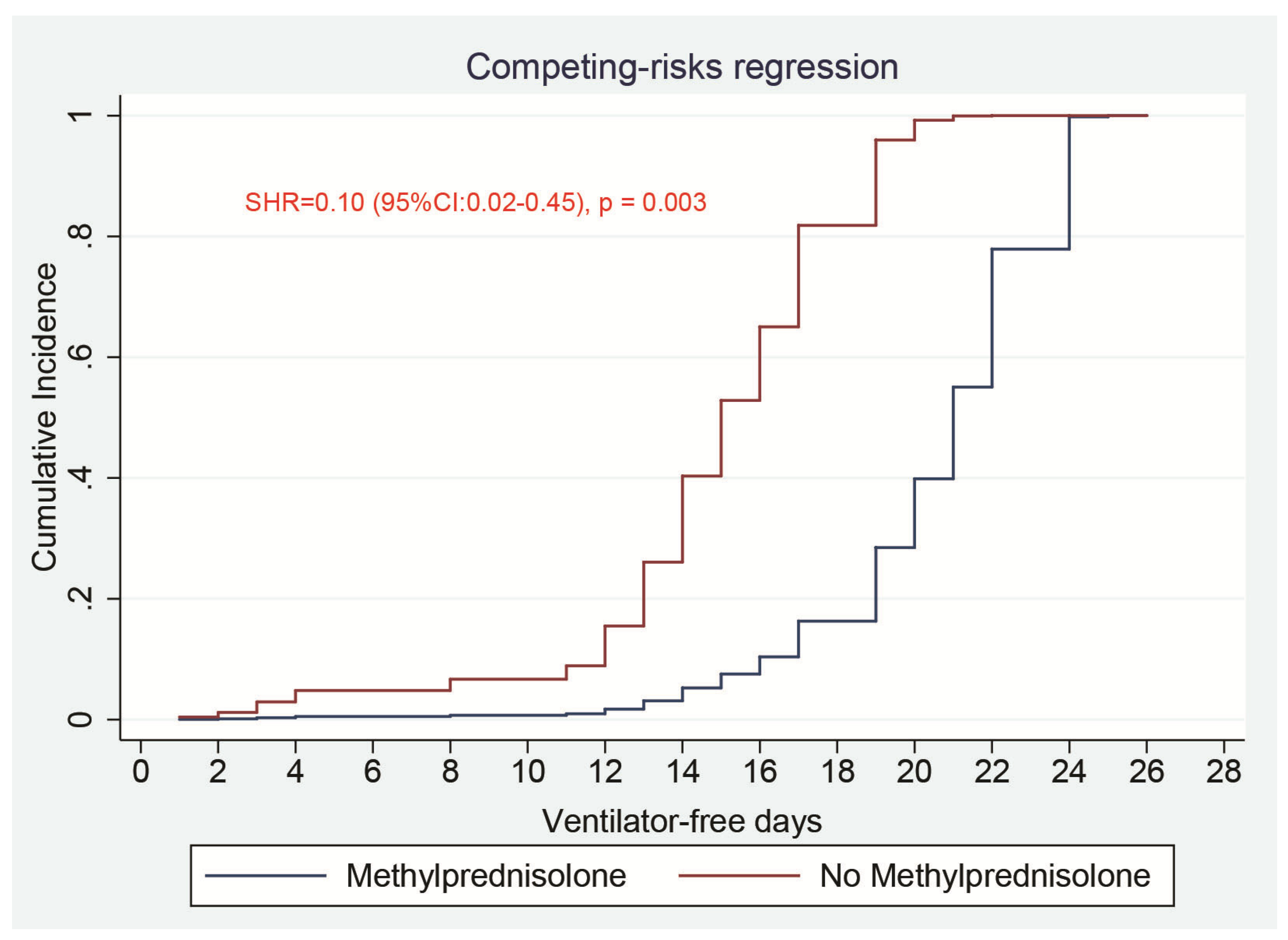
3.2. Primary Clinical Outcome
3.3. Secondary Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, L.C.; Hui, C.D.S.; et al. China Medical Treatment Expert Group for Covid-19: Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Ferrando, C.; Suarez-Sipmann, F.; Mellado-Artigas, R.; Hernández, M.; Gea, A.; Arruti, E.; Villar, J.; Martínez-Pallí, G.; Martínez-González, M.A.; Slutsky, A.S.; et al. Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. 2020, 46, 2200–2211. [Google Scholar] [CrossRef]
- Nadeem, A.; Hamed, F.; Saleh, K.; Abduljawad, B.; Mallat, J. ICU outcomes of COVID-19 critically ill patients: An international comparative study. Anaesth. Crit. Care Pain Med. 2020, 39, 487–489. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. ISARIC4C investigators: Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. COVID-19 Lombardy ICU Network: Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhen, T.; Cidlowski, J.A. Antiinflammatory action of glucocorticoids—New mechanisms for old drugs. N. Engl. J. Med. 2005, 353, 1711–1723. [Google Scholar] [CrossRef] [Green Version]
- Arabi, Y.M.; Chrousos, G.P.; Meduri, G.U. The ten reasons why corticosteroid therapy reduces mortality in severe COVID-19. Intensive Care Med. 2020, 46, 2067–2070. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.; Mafham, M.; Bell, J.; Linsell, L. RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with Covid-19—Preliminary report. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- De Backer, D.; Azoulay, E.; Vincent, J.L. Corticosteroids in severe COVID-19: A critical view of the evidence. Crit. Care 2020, 24, 627. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B.; et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Efect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syn- drome and COVID-19: The CoDEX randomized clinical trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.C.; Laracy, J.; Shoucri, S.; Dietz, D.; Zucker, J.; Patel, N.; Sobieszczyk, M.E.; Kubin, C.J.; Gomez-Simmonds, A. Clinical Outcomes Associated with Methylprednisolone in Mechanically Ventilated Patients with COVID-19. Clin. Infect. Dis. 2020, 9, ciaa1163. [Google Scholar] [CrossRef]
- Force, ARDS Definition Task; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.; Ferguson, N.; Caldwell, E. ARDS Definition Task Force. Acute respiratory distress syndrome: The Berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Yehya, N.; Harhay, M.O.; Curley, M.A.Q.; Schoenfeld, D.A.; Reeder, R.W. Reappraisal of Ventilator-Free Days in Critical Care Research. Am. J. Respir. Crit. Care Med. 2019, 200, 828–836. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Mandourah, Y.; Al-Hameed, F.; Sindi, A.A.; Almekhlafi, G.A.; Hussein, M.A.; Jose, J.; Pinto, R.; Al-Omari, A.; Kharaba, A.; et al. Saudi Critical Care Trial Group: Corticosteroid Therapy for critically ill patients with Middle East respiratory syndrome. Am. J. Respir. Crit Care Med. 2018, 197, 757–767. [Google Scholar] [CrossRef]
- Lee, N.; Chan, K.C.A.; Hui, D.S.; Ng, E.K.O.; Wu, A.; Chiu, R.W.K.; Wong, V.W.S.; Chan, P.K.S.; Wong, K.T.; Wong, E.; et al. Effects of early corticosteroid treatment on plasma SARS-associated Coronavirus RNA concentrations in adult patients. J. Clin. Virol. 2004, 31, 304–309. [Google Scholar] [CrossRef]
- Lansbury, L.E.; Rodrigo, C.; Leonardi-Bee, J.; Nguyen-Van-Tam, J.; Shen Lim, W. Corticosteroids as adjunctive therapy in the treatment of influenza: An updated cochrane systematic review and meta-analysis. Crit. Care Med. 2020, 48, E98–E106. [Google Scholar] [CrossRef] [PubMed]
- Stockman, L.J.; Bellamy, R.; Garner, P. SARS: Systematic review of treatment effects. PLoS Med. 2006, 3, 1525–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeronimo, C.M.P.; Farias, M.E.L.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Safe, I.P.; Borba, M.G.S.; Abreu-Netto, R.L.; Maciel, A.B.S.; et al. Methylprednisolone as Adjunctive Therapy for Patients Hospitalized With COVID-19 (Metcovid): A Randomised, Double-Blind, Phase IIb, Placebo-Controlled Trial. Clin. Infect. Dis. 2020, ciaa1177. [Google Scholar] [CrossRef]
- Wu, C.; Hou, D.; Du, C.; Cai, Y.; Zheng, J.; Xu, J.; Chen, X.; Chen, C.; Hu, X.; Zhang, Y.; et al. Corticosteroid therapy for coronavirus disease 2019-related acute respiratory distress syndrome: A cohort study with propensity score analysis. Crit. Care 2020, 24, 643. [Google Scholar] [CrossRef]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.V.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Papazian, L.; Forel, J.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.; Perez, D.; Seghboyan, J.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guérin, C.; Reignier, J.; Richard, J.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Patients (n = 77) | Methylprednisolone (n = 32) | Non-Methylprednisolone (n = 45) | p-Value |
|---|---|---|---|---|
| Age, year | 50 (41–59) | 49 (41–55) | 51 (41–61) | 0.52 |
| Male, n (%) | 72 (93.5) | 30 (93.7) | 42 (93.3) | 1.00 |
| Body mass index, kg·m−2 | 25.8 (23.1–29.0) | 25.8 (22.2–29.7) | 25.9 (23.8–28.0) | 0.96 |
| SOFA score | 7 (4–10) | 7 (4–9) | 7 (4–10) | 0.80 |
| SAPS II score | 36 (27–48) | 38 (28–49) | 35 (27–46) | 0.67 |
| Patients with at least one comorbidity, n (%) | 49 (63.4) | 21 (65.6) | 28 (62.2) | 0.76 |
| Comorbidities distribution, n (%) | ||||
| Diabetes mellitus | 36 (46.7) | 18 (56.2) | 18 (40.0) | 0.16 |
| Hypertension | 35 (45.4) | 15 (46.9) | 20 (44.4) | 0.83 |
| Chronic artery disease | 7 (9.1) | 4 (12.5) | 3 (6.7) | 0.44 |
| Chronic kidney disease | 2 (2.6) | 1 (3.1) | 1 (2.2) | 1.00 |
| Time from symptoms to ICU admission, day | 5 (4–7) | 5 (4–11) | 5 (4–7) | 0.21 |
| Time from ICU admission to intubation, day | 0 (0–1) | 0 (0–2) | 0 (0–1) | 0.50 |
| Time from symptoms to intubation, day | 5 (3–10) | 6 (3–11) | 5 (3–9) | 0.46 |
| Vital signs on ICU admission | ||||
| Temperature (max) ≥ 38 °C, n (%) | 28 (36.4) | 11 (34.4) | 17 (37.8) | 0.76 |
| Heart rate (max), beats·min−1 | 105 ± 20 | 105 ± 21 | 105 ± 20 | 0.99 |
| Respiratory rate (max), breaths·min−1 | 32 ± 8 | 30 ± 8 | 32 ± 8 | 0.30 |
| Laboratory data on ICU admission | ||||
| C–reactive protein, mg·L−1 | 159 (68–244) | 104 (58–166) | 198 (99–295) | 0.003 |
| Leucocytes count, × 109·L−1 | 9.8 (7.6–13.0) | 10.6 (7.4–14.3) | 9.7 (7.7–12.2) | 0.53 |
| Lymphocytes count, × 109·L−1 | 0.79 (0.49–1.00) | 0.88 (0.54–1.06) | 0.71 (0.47–0.99) | 0.22 |
| Lymphocytes ≤ 1 × 109·L−1; n (%) | 58 (75.3) | 23 (71.9) | 35 (77.8) | 0.55 |
| Platelet count, × 109·L−1 | 251 (183–320) | 245 (160–319) | 256 (197–320) | 0.51 |
| Procalcitonin, ng·mL−1 | 0.60 (0.21–3.71) | 0.44 (0.21–2.07) | 0.96 (0.23–7.58) | 0.11 |
| International normalized ratio | 1.2 (1.1–1.3) | 1.2 (1.1–1.3) | 1.2 (1.1–1.4) | 0.18 |
| Activated partial thromboplastin time; s | 34.1 (30.0–38.3) | 33.2 (28.1–37.7) | 34.6 (31.2–38.4) | 0.25 |
| D–dimer, µg·mL−1 (normal reference: <0.05) | 3.7 (1.7–4.0) | 3.4 (1.3–4.0) | 4.0 (1.9–4.0) | 0.35 |
| D–dimer ≥ 2 µg·mL−1, n (%) | 56 (72.7%) | 23 (71.9) | 33 (73.3) | 0.89 |
| Fibrinogen, g·L−1 | 6.1 (4.6–7.2) | 5.8 (4.1–6.7) | 6.3 (5.2–7.7) | 0.21 |
| Ferritin, µg·L−1 (reference range: 36–480) | 1561 (895–2484) | 1854 (968–2479) | 1406 (748–2582) | 0.32 |
| Interleukin 6, ng·L−1 | 279 (130–1130) | 174 (103–466) | 665 (176–2438) | 0.005 |
| Alanine aminotransferase, IU·mL−1 | 37 (27–65) | 37 (30–66) | 38 (25–63) | 0.67 |
| Aspartate aminotransferase, IU·mL−1 | 55 (36–91) | 50 (36–84) | 59 (36–95) | 0.28 |
| Total bilirubin, µmol·L−1 | 11.6 (8.1–18.2) | 10.5 (8.1–15.8) | 12.0 (8.3–20.4) | 0.55 |
| Creatinine, µmol·L−1 | 83 (65–154) | 74 (63–123) | 91 (65–155) | 0.19 |
| Albumin, g·L−1 | 30 (27–34) | 31 (27–34) | 29 (27–33) | 0.39 |
| Variables | All Patients (n = 77) | Methylprednisolone (n = 32) | Non-Methylprednisolone (n = 45) | p-Value |
|---|---|---|---|---|
| Oxygenation variables on ICU admission | ||||
| PaO2, mmHg | 68 (57–83) | 70 (61–84) | 67 (56–81) | 0.71 |
| PaCO2, mmHg | 44 (34–56) | 46 (33–54) | 43 (34–58) | 0.74 |
| FiO2 | 0.9 (0.6–1) | 0.8 (0.6–1) | 1 (0.6–1) | 0.43 |
| PaO2/FiO2 ratio, mmHg | 83 (62–131) | 85 (67–134) | 83 (61–128) | 0.83 |
| SaO2, % | 92 (88–94) | 93 (88–94) | 91 (88–93) | 0.33 |
| Lactate levels, mmol·L−1 | 1.45 (1.20–1.90) | 1.40 (1.20–1.90) | 1.45 (1.20–1.90) | 0.83 |
| Treatments during the ICU stay, n (%) | ||||
| Vasopressor support | 65 (84.2) | 23 (71.9) | 42 (93.3) | 0.01 |
| Renal replacement therapy | 24 (31.2) | 8 (25.0) | 16 (35.6) | 0.32 |
| Prone position | 50 (64.9) | 22 (68.7) | 28 (62.2) | 0.55 |
| Neuromuscular blocker agents | 63 (81.2) | 26 (81.2) | 37 (82.2) | 1.00 |
| Tocilizumab | 67 (87.0) | 26 (81.2) | 41 (91.1) | 0.30 |
| Hydroxychloroquine | 30 (39.0) | 12 (37.5) | 18 (40.0) | 0.82 |
| Favipiravir | 23 (29.9) | 11 (34.4) | 12 (26.7) | 0.47 |
| Lopinavir/ritonavir | 18 (23.4) | 8 (25.0) | 10 (22.2) | 0.78 |
| Ventilator parameters on ICU admission | ||||
| Tidal volume, mL·kg−1 IBW | 6.5 (6.0–7.0) | 6.5 (6.1–7.0) | 6.5 (5.7–7.2) | 0.65 |
| Plateau pressure, cmH2O | 28 (26–30) | 28 (26–30) | 28 (27–30) | 0.84 |
| Positive end expiratory pressure, cmH2O | 12 (10–14) | 12 (10–14) | 12 (10–14) | 0.58 |
| Driving pressure, cmH2O | 16 (13–18) | 16 (13–19) | 17 (14–18) | 0.59 |
| Static compliance, mL.cmH2O−1 | 27.0 (22.0–34.1) | 28.6 (22.5–35.4) | 25.0 (21.1–32.5) | 0.21 |
| Variables | SHR | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Methylprednisolone treatment (refer: no) | 0.10 | 0.02–0.45 | 0.003 |
| Age, year | 1.04 | 0.95–1.14 | 0.42 |
| Body mass index, kg·m−2 | 1.16 | 1.01–1.33 | 0.03 |
| SOFA score | 0.92 | 0.75–1.13 | 0.44 |
| Lactate, mmol·L−1 | 3.93 | 1.78–8.70 | 0.001 |
| PaO2/FiO2 ratio, mmHg | 1.00 | 0.98–1.02 | 0.98 |
| SaO2, % | 1.09 | 0.88–1.36 | 0.41 |
| D-dimer, µg·mL−1 | 0.54 | 0.31–0.94 | 0.03 |
| Procalcitonin, ng·mL−1 | 1.02 | 1.002–1.046 | 0.03 |
| Interleukin 6, ng·L−1 | 1.00 | 0.99–1.00 | 0.98 |
| C-reactive protein, mg·L−1 | 1.00 | 0.99–1.00 | 0.49 |
| Time from symptoms onset to Methylprednisolone, day | 1.02 | 0.78–1.34 | 0.86 |
| Creatinine, µmol·L−1 | 1.00 | 0.99–1.00 | 0.22 |
| Vasopressor support, (refer: no) | 4.33 | 0.47–40.15 | 0.20 |
| Renal replacement therapy, (refer: no) | 1.90 | 0.51–7.10 | 0.34 |
| Prone position, (refer: no) | 16.70 | 1.70–260.62 | 0.04 |
| Neuromuscular blocker agents, (refer: no) | 2.60 | 0.12–56.41 | 0.54 |
| Tocilizumab, (refer: no) | 0.20 | 0.02–2.43 | 0.21 |
| Comorbidities, (refer: no) | 2.35 | 0.71–7.74 | 0.16 |
| Tidal volume, mL·kg−1 IBW | 0.99 | 0.54–1.79 | 0.97 |
| Plateau pressure, cmH2O | 0.97 | 0.70–1.34 | 0.86 |
| Positive end expiratory pressure, cmH2O | 0.74 | 0.49–1.11 | 0.15 |
| Driving pressure, cmH2O | 0.91 | 0.72–1.16 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badr, M.; De Oliveira, B.; Abdallah, K.; Nadeem, A.; Varghese, Y.; Munde, D.; Salam, S.; Abduljawad, B.; Saleh, K.; Elkambergy, H.; et al. Effects of Methylprednisolone on Ventilator-Free Days in Mechanically Ventilated Patients with Acute Respiratory Distress Syndrome and COVID-19: A Retrospective Study. J. Clin. Med. 2021, 10, 760. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10040760
Badr M, De Oliveira B, Abdallah K, Nadeem A, Varghese Y, Munde D, Salam S, Abduljawad B, Saleh K, Elkambergy H, et al. Effects of Methylprednisolone on Ventilator-Free Days in Mechanically Ventilated Patients with Acute Respiratory Distress Syndrome and COVID-19: A Retrospective Study. Journal of Clinical Medicine. 2021; 10(4):760. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10040760
Chicago/Turabian StyleBadr, Mohamed, Bruno De Oliveira, Khaled Abdallah, Ashraf Nadeem, Yeldho Varghese, Dnyaseshwar Munde, Shameen Salam, Baraa Abduljawad, Khaled Saleh, Hussam Elkambergy, and et al. 2021. "Effects of Methylprednisolone on Ventilator-Free Days in Mechanically Ventilated Patients with Acute Respiratory Distress Syndrome and COVID-19: A Retrospective Study" Journal of Clinical Medicine 10, no. 4: 760. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10040760