
Five-Year Outcome of Aflibercept Monotherapy for Exudative Age-Related Macular Degeneration with Good Baseline Visual Acuity

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Follow Up
2.3. Genotyping
2.4. Statistical Analysis
3. Results
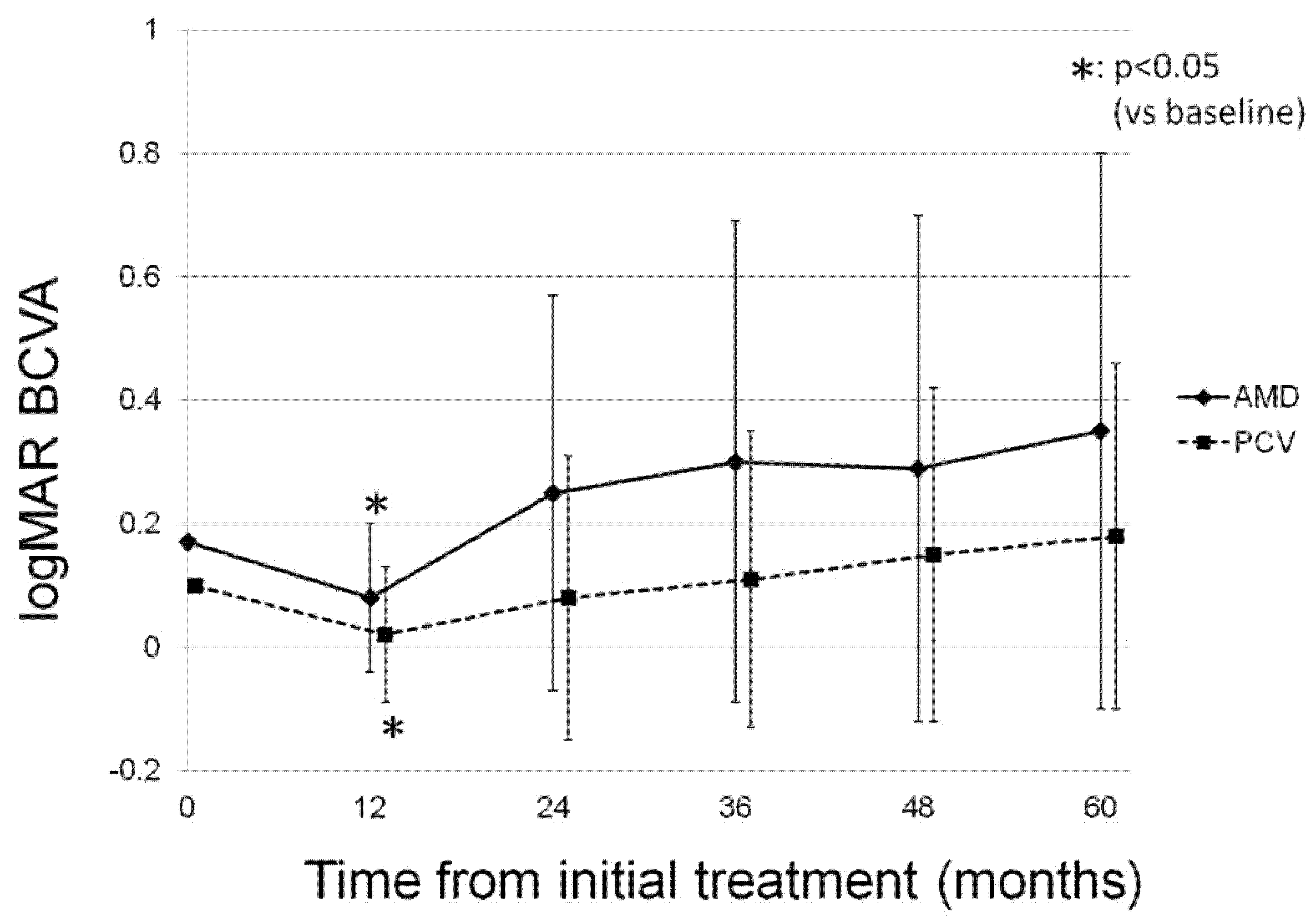
3.1. Change in Log MAR BCVA
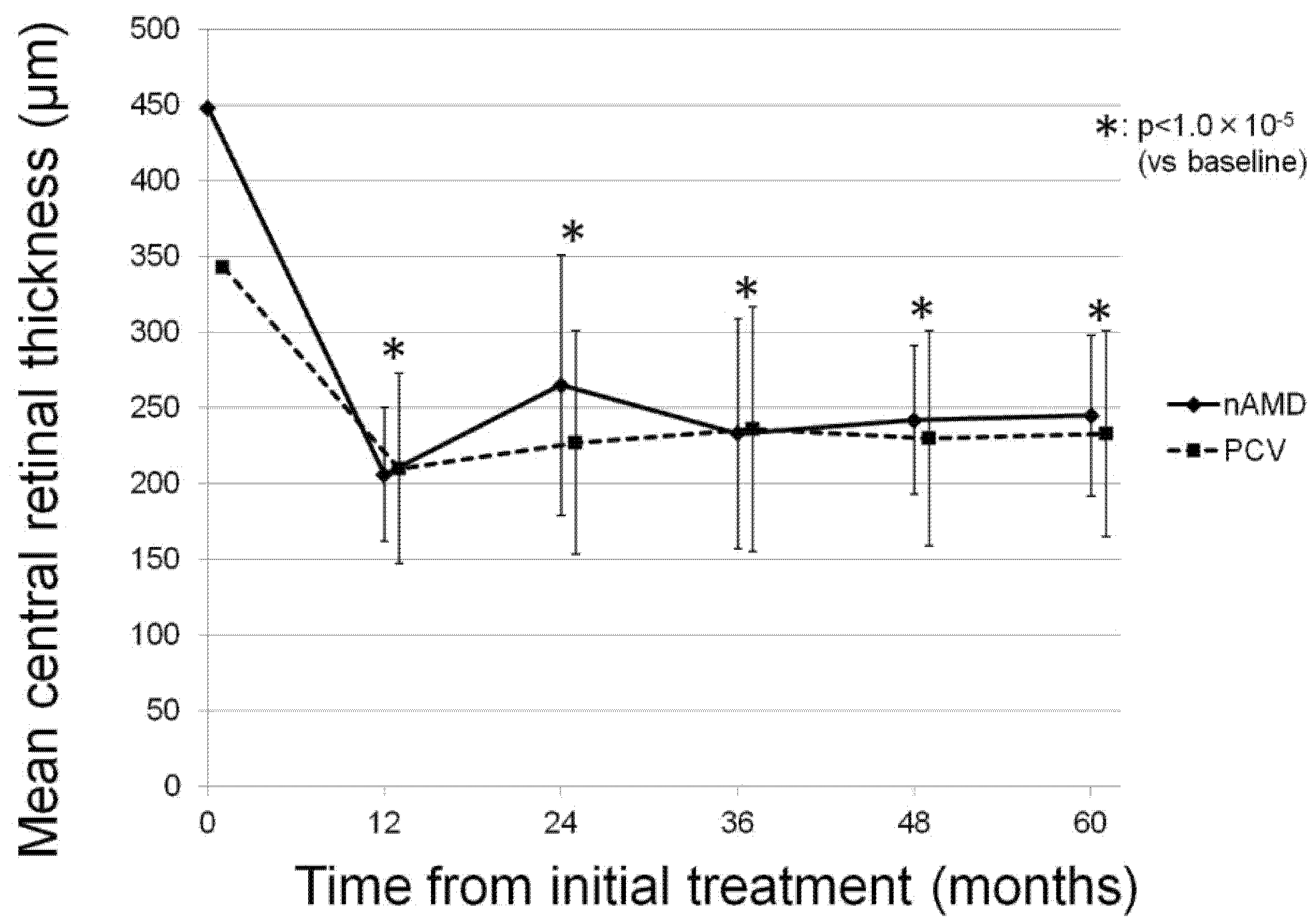
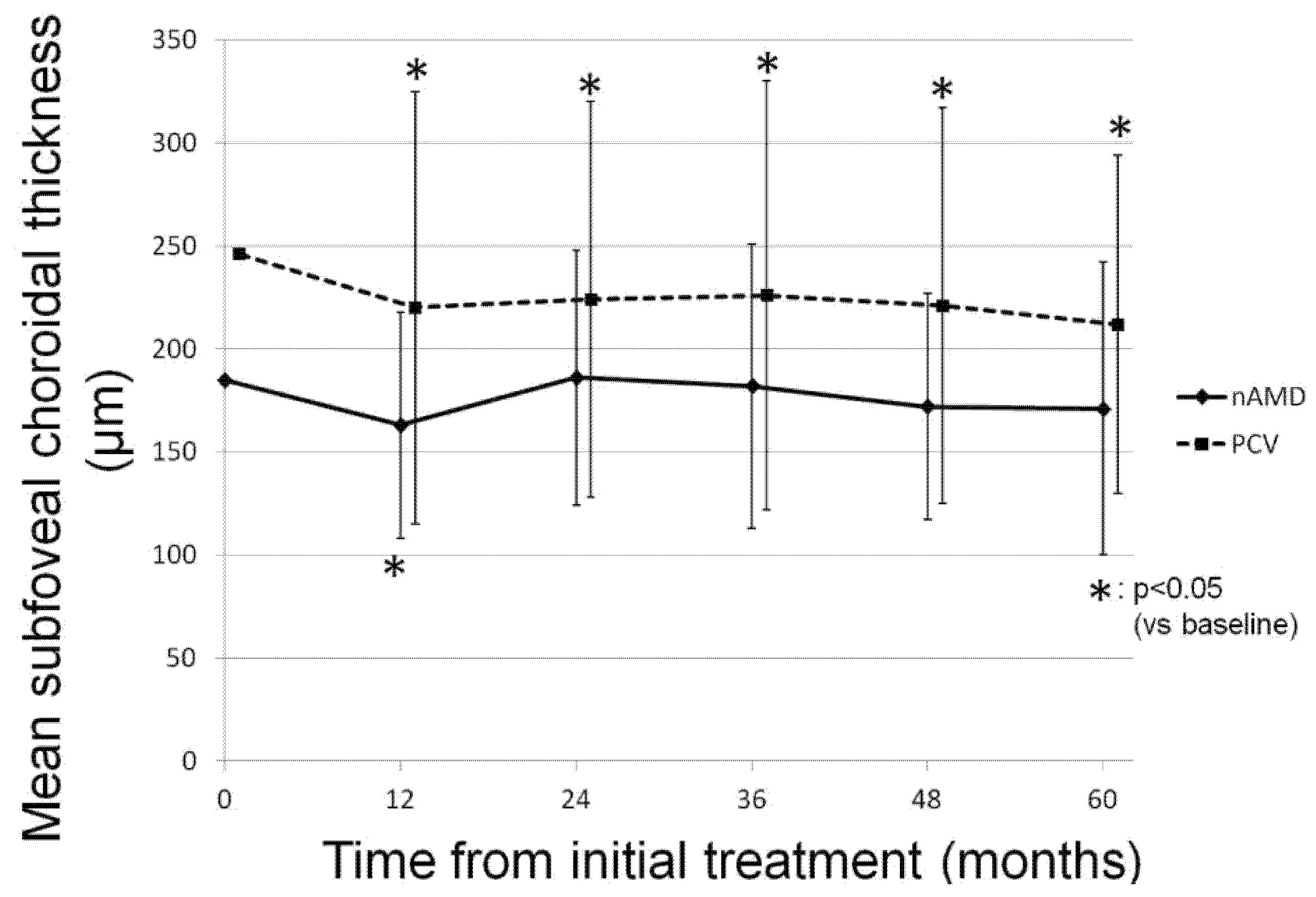
3.2. Change in OCT Parameters
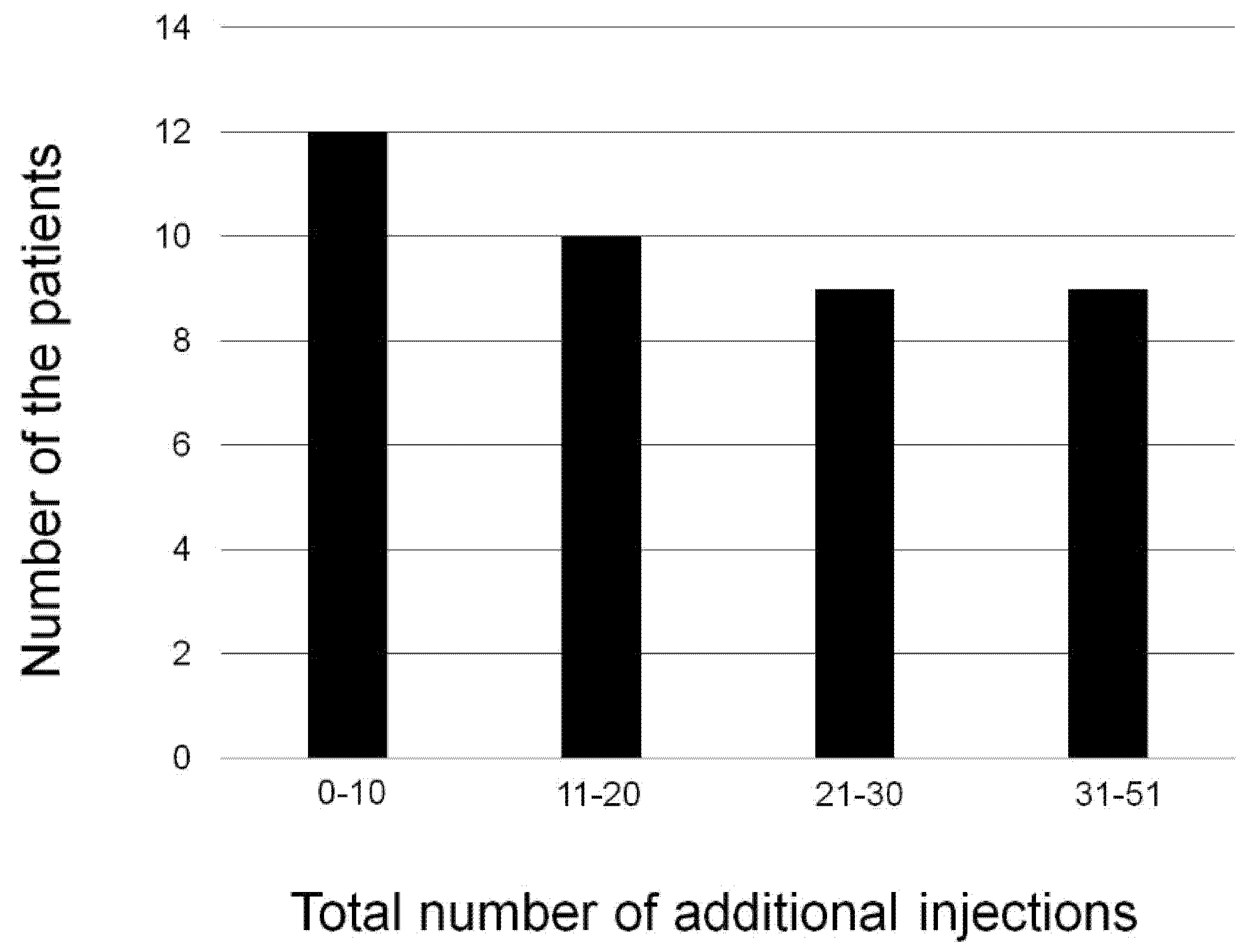
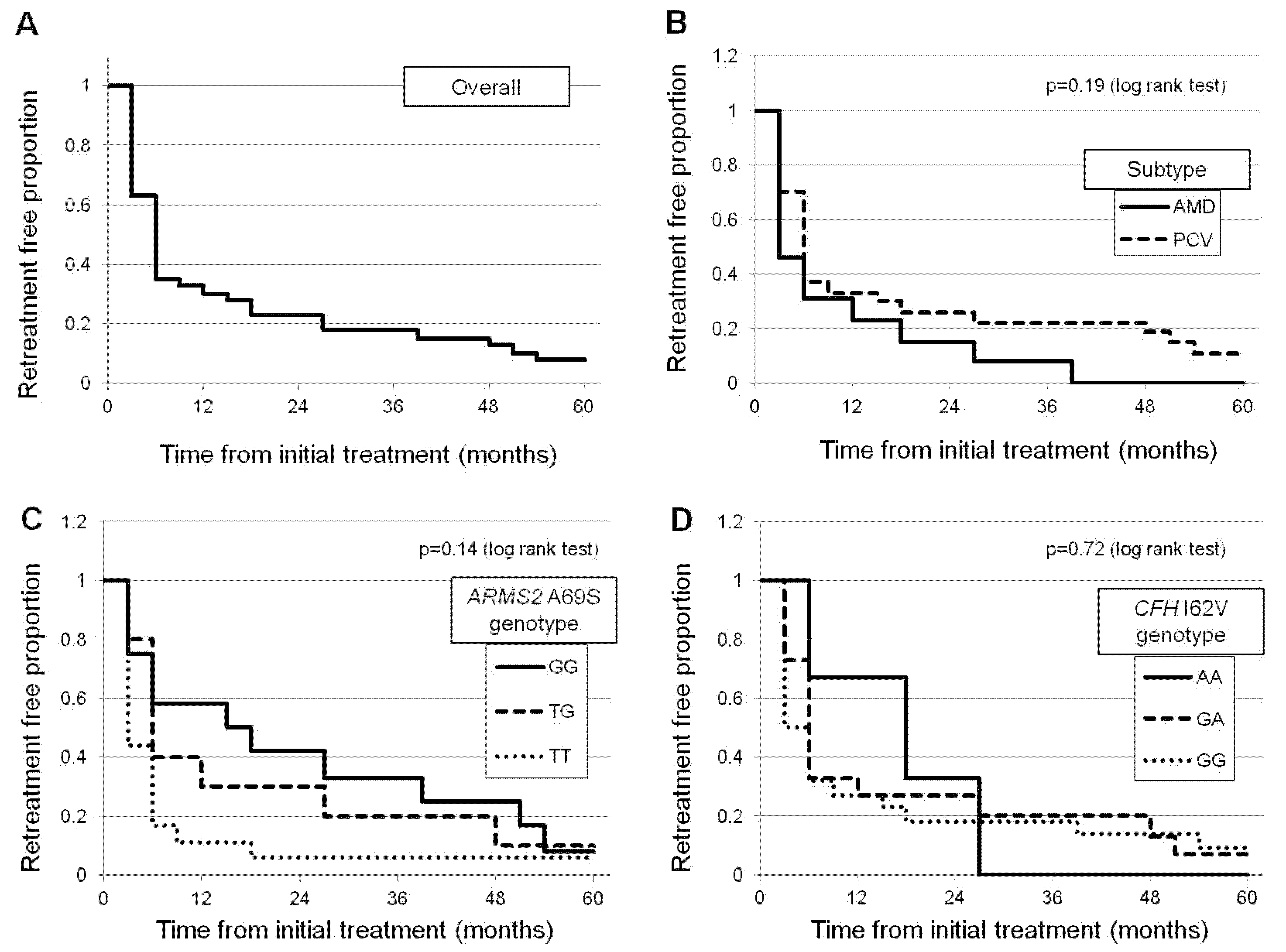
3.3. Retreatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kawasaki, R.; Yasuda, M.; Song, S.J.; Chen, S.J.; Jonas, J.B.; Wang, J.J.; Mitchell, P.; Wong, T.Y. The prevalence of age-related macular degeneration in Asians: A systematic review and meta-analysis. Ophthalmology 2010, 117, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Shijo, T.; Sakurada, Y.; Fukuda, Y.; Yoneyama, S.; Sugiyama, A.; Matsubara, M.; Kikushima, W.; Tanabe, N.; Parikh, R.; Kashiwagi, K. Association of CRP levels with ARMS2 and CFH variants in age-related macular degeneration. Int. Ophthalmol. 2020, 40, 2735–2742. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Kaiser, P.K.; Michels, M.; Soubrane, G.; Heier, J.S.; Kim, R.Y.; Sy, J.P.; Schneider, S. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1432–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regillo, C.D.; Brown, D.M.; Abraham, P.; Yue, H.; Ianchulev, T.; Schneider, S.; Shams, N.; PIER Study Group. Randomized, double-masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER Study year 1. Am. J. Ophthalmol. 2008, 145, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Lalwani, G.A.; Rosenfeld, P.J.; Fung, A.E.; Dubovy, S.R.; Michels, S.; Feuer, W.; Davis, J.L.; Flynn, H.W., Jr.; Esquiabro, M. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: Year 2 of the PrONTO Study. Am. J. Ophthalmol. 2009, 148, 43–58.e1. [Google Scholar] [CrossRef] [PubMed]
- CATT Research Group. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2011, 364, 1897–1908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef] [PubMed]
- Minami, S.; Nagai, N.; Suzuki, M.; Kurihara, T.; Sonobe, H.; Kamoshita, M.; Uchida, A.; Shinoda, H.; Takagi, H.; Sonoda, S.; et al. Benefits of aflibercept treatment for age-related macular degeneration patients with good best-corrected visual acuity at baseline. Sci. Rep. 2018, 8, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedi, F.; Wickremasinghe, S.; Islam, A.F.; Inglis, K.M.; Guymer, R.H. Anti-VEGF treatment in neovascular age-related macular degeneration: A treat-and-extend protocol over 2 years. Retina 2014, 34, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Kikushima, W.; Sakurada, Y.; Sugiyama, A.; Tanabe, N.; Kume, A.; Iijima, H. Factors Predictive of Visual Outcome 1 Year after Intravitreal Aflibercept Injection for Typical Neovascular Age-Related Macular Degeneration. J. Ocul. Pharm. Ther. 2016, 32, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Yoneyama, S.; Sakurada, Y.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Fukuda, Y.; Tanabe, N.; Parikh, R.; Mabuchi, F.; Kashiwagi, K.; et al. Genetic factors associated with response to as-needed aflibercept therapy for typical neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Sci. Rep. 2020, 10, 7188. [Google Scholar] [CrossRef] [PubMed]
- Shijo, T.; Sakurada, Y.; Yoneyama, S.; Kikushima, W.; Sugiyama, A.; Matsubara, M.; Fukuda, Y.; Mabuchi, F.; Kashiwagi, K. Association between Polygenic Risk Score and One-Year Outcomes Following As-Needed Aflibercept Therapy for Exudative Age-Related Macular Degeneration. Pharmaceuticals 2020, 13, 257. [Google Scholar] [CrossRef] [PubMed]
- Khanani, A.M.; Gahn, G.M.; Koci, M.M.; Dang, J.M.; Brown, S.M.; Hill, L.F. Five-year outcomes of intravitreal drug therapy for neovascular age-related macular degeneration in eyes with baseline vision 20/60 or better. Clin. Ophthalmol. 2019, 13, 347–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javidi, S.; Dirani, A.; Antaki, F.; Saab, M.; Rahali, S.; Cordahi, G. Long-Term Visual Outcomes for a Treat-and-Extend Antivascular Endothelial Growth Factor Regimen in Eyes with Neovascular Age-Related Macular Degeneration: Up to Seven-Year Follow-Up. J. Ophthalmol. 2020, 2020, 3207614. [Google Scholar] [CrossRef] [PubMed]
- Maguire, M.G.; Martin, D.F.; Ying, G.S.; Jaffe, G.J.; Daniel, E.; Grunwald, J.E.; Toth, C.A.; Ferris, F.L., III; Fine, S.L.; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Five-Year Outcomes with Anti-Vascular Endothelial Growth Factor Treatment of Neovascular Age-Related Macular Degeneration: The Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology 2016, 123, 1751–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikushima, W.; Sakurada, Y.; Yoneyama, S.; Sugiyama, A.; Tanabe, N.; Kume, A.; Mabuchi, F.; Iijima, H. Incidence and risk factors of retreatment after three-monthly aflibercept therapy for exudative age-related macular degeneration. Sci. Rep. 2017, 7, 44020. [Google Scholar] [CrossRef] [PubMed]
- Kikushima, W.; Sakurada, Y.; Sugiyama, A.; Yoneyama, S.; Tanabe, N.; Matsubara, M.; Mabuchi, F.; Iijima, H. Comparison of two-year outcomes after photodynamic therapy with ranibizumab or aflibercept for polypoidal choroidal vasculopathy. Sci. Rep. 2017, 7, 16461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wataru, K.; Sugiyama, A.; Yoneyama, S.; Matsubara, M.; Fukuda, Y.; Parikh, R.; Sakurada, Y. Five-year outcomes of photodynamic therapy combined with intravitreal injection of ranibizumab or aflibercept for polypoidal choroidal vasculopathy. PLoS ONE 2020, 15, e0229231. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Subjects n = 40 | nAMD n = 13 | PCV n = 27 | p-Value (nAMD vs. PCV) | |
|---|---|---|---|---|
| Age | 71.8 ± 8.0 | 74.0 ± 9.3 | 70.8 ± 7.2 | 0.38 |
| Gender male | 31(77.5%) | 11(84.6%) | 20(74.1%) | 0.45 |
| Baseline BCVA | 0.12 ± 0.09 | 0.17 ± 0.07 | 0.10 ± 0.09 | 0.02 |
| Baseline CRT | 377 ± 155 | 448 ± 231 | 343 ± 88 | 0.28 |
| Baseline SCT | 226 ± 98 | 185 ± 56 | 246 ± 108 | 0.10 |
| Baseline GLD | 2767 ± 1385 | 3049 ± 1554 | 2631 ± 1306 | 0.41 |
| ARMS2 A69S (rs10490924) | ||||
| GG:TG:TT (T allele frequency) | 12:10:18 (57.5%) | 1:4:8 (76.9%) | 11:6:10 (48.1%) | 0.015 |
| CFH I62V (rs800292) | ||||
| AA:GA:GG (G allele frequency) | 3:15:22 (73.8%) | 0:3:10 (88.5%) | 3:12:12 (66.7%) | 0.038 |
| Variables | β-Coefficient | p-Value |
|---|---|---|
| Age | 0.01 | 0.25 |
| Male gender | −0.36 | 0.023 |
| Baseline log MAR BCVA | −0.23 | 0.76 |
| Greatest linear dimension | −2.8 × 10−6 | 0.95 |
| Central retinal thickness | 4.1 × 10−4 | 0.41 |
| Subfoveal choroidal thickness | −4.5 × 10−4 | 0.50 |
| Subtype (nAMD = 0, PCV = 1) | 0.02 | 0.91 |
| ARMS2 A69S T allele | 2.0 × 10−3 | 0.98 |
| CFH I62V G allele | 0.14 | 0.16 |
| Cataract surgery | 0.046 | 0.82 |
| Total number of IAIs | 5.6 × 10−4 | 0.90 |
| Total (0–60 Months) | 1st Year (0–12 Months) | 2nd Year (13–24 Months) | 3rd Year (25–36 Months) | 4th Year (37–48 Months) | 5th Year (49–60 Months) |
|---|---|---|---|---|---|
| 18.4 ± 14.0 | 2.4 ± 2.5 | 3.8 ± 3.1 | 3.7 ± 3.4 | 3.8 ± 3.4 | 4.4 ± 3.9 |
| Variables | β-Coefficient | p-Value |
|---|---|---|
| Age | 0.44 | 0.23 |
| Male gender | −5.61 | 0.36 |
| Baseline log MAR BCVA | 39.3 | 0.18 |
| Greatest linear dimension | −2.0 × 10−3 | 0.32 |
| Central retinal thickness | 0.023 | 0.22 |
| Subfoveal choroidal thickness | −0.029 | 0.27 |
| Subtype (nAMD = 0, PCV = 1) | 7.09 | 0.27 |
| ARMS2 A69S T allele | 6.63 | 0.025 |
| CFH I62V G allele | 0.87 | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikushima, W.; Sakurada, Y.; Sugiyama, A.; Yoneyama, S.; Matsubara, M.; Fukuda, Y.; Kashiwagi, K. Five-Year Outcome of Aflibercept Monotherapy for Exudative Age-Related Macular Degeneration with Good Baseline Visual Acuity. J. Clin. Med. 2021, 10, 1098. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051098
Kikushima W, Sakurada Y, Sugiyama A, Yoneyama S, Matsubara M, Fukuda Y, Kashiwagi K. Five-Year Outcome of Aflibercept Monotherapy for Exudative Age-Related Macular Degeneration with Good Baseline Visual Acuity. Journal of Clinical Medicine. 2021; 10(5):1098. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051098
Chicago/Turabian StyleKikushima, Wataru, Yoichi Sakurada, Atsushi Sugiyama, Seigo Yoneyama, Mio Matsubara, Yoshiko Fukuda, and Kenji Kashiwagi. 2021. "Five-Year Outcome of Aflibercept Monotherapy for Exudative Age-Related Macular Degeneration with Good Baseline Visual Acuity" Journal of Clinical Medicine 10, no. 5: 1098. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051098