
Impact of Medication Regimen Simplification on Medication Incidents in Residential Aged Care: SIMPLER Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
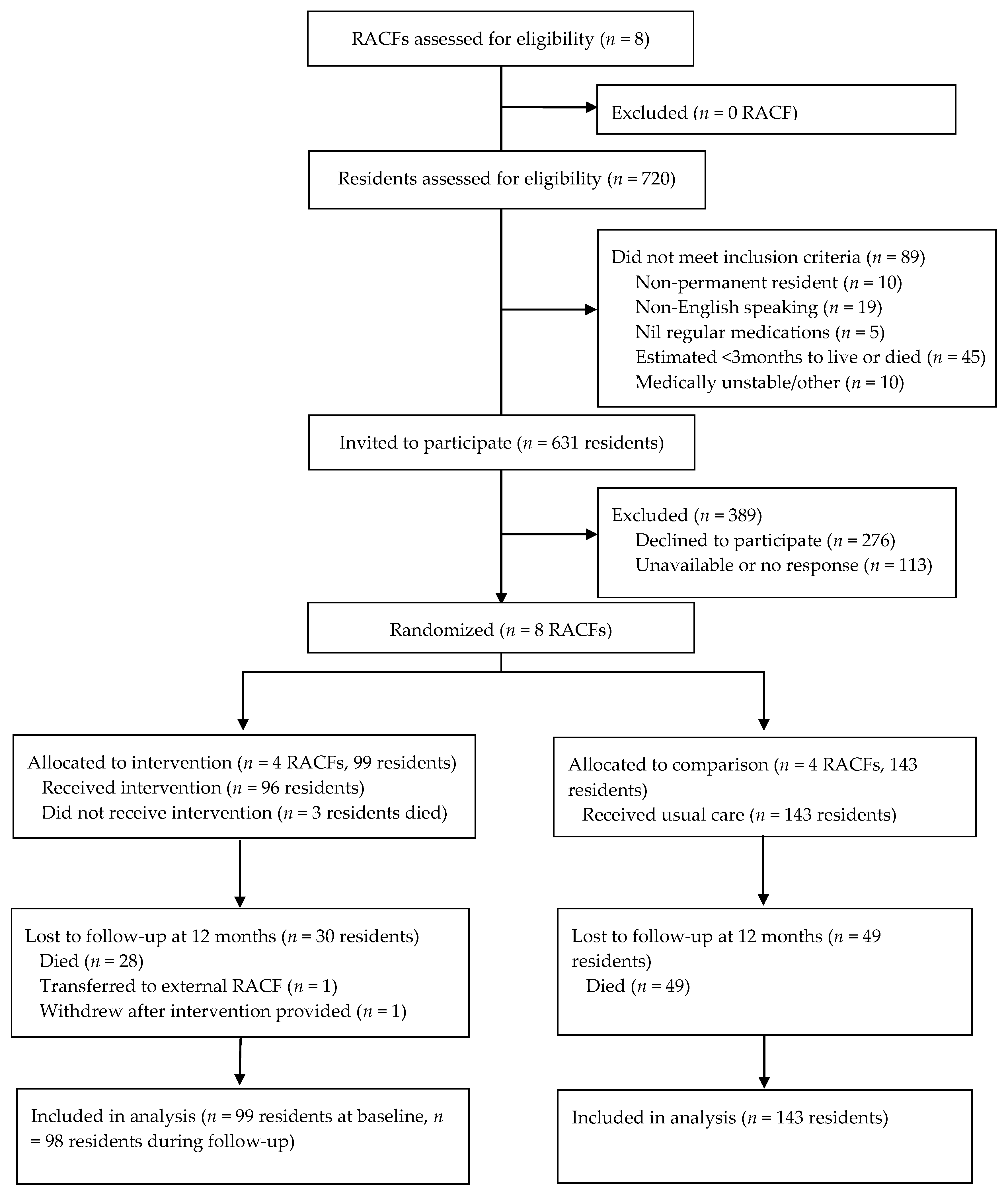
2.2. Participants
2.3. Intervention
2.4. Outcomes
2.5. Covariates
2.6. Analysis
3. Results
3.1. Demographics
3.2. Number and Type of Medication Incidents during Follow-Up
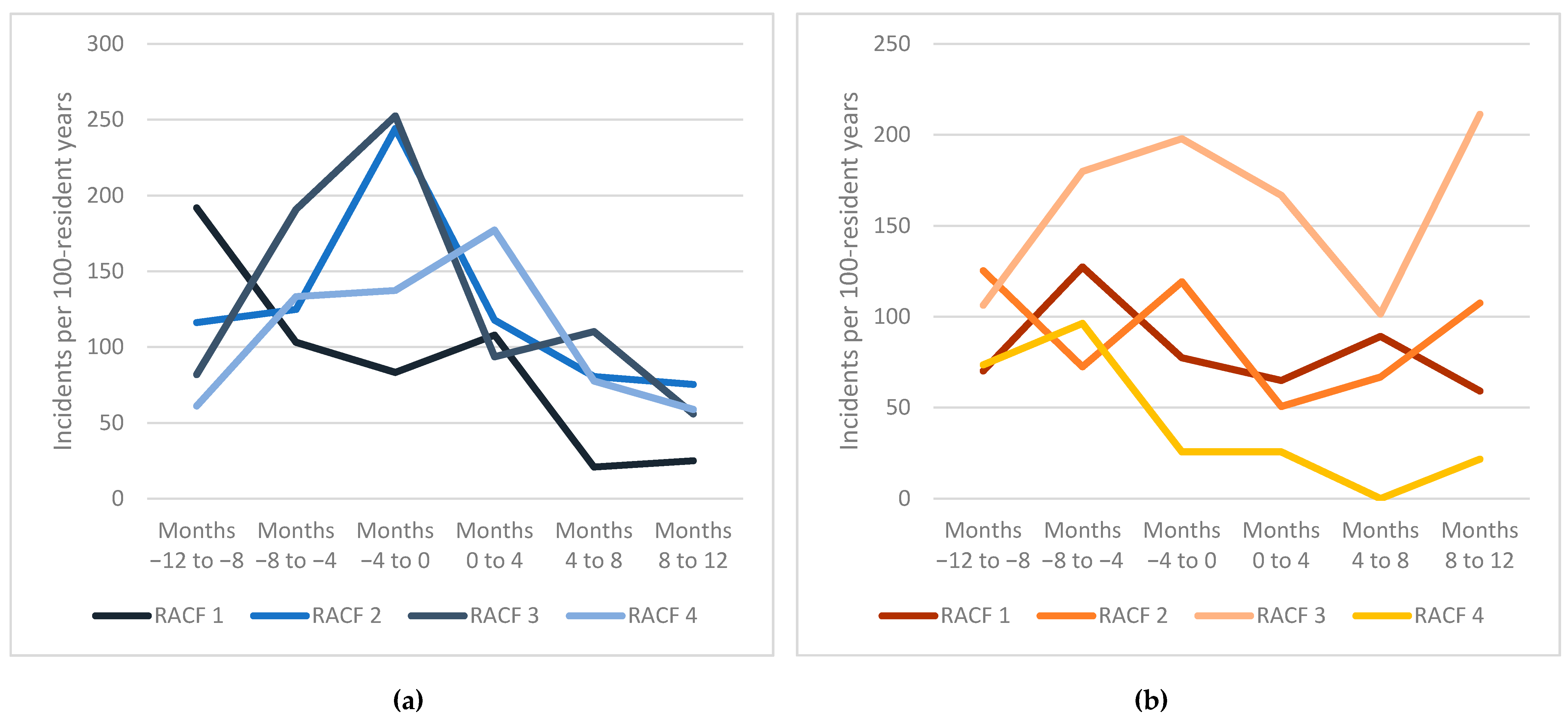
3.3. Medication Incident Rates
3.4. Per Protocol Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aitken, M.; Gorokhovich, L. Advancing the responsible use of medicines: Applying levers for change. SSRN Electron. J. 2012. [CrossRef] [Green Version]
- World Health Organization. Medication without Harm- Global Patient Safety Challenge on Medication Safety; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Pharmaceutical Society of Australia. PSA19: Minister Hunt Reaffirms Commitment to Addressing Medicine Safety. Available online: https://www.psa.org.au/psa19-minister-hunt-reaffirms-commitment-to-addressing-medicine-safety/ (accessed on 30 August 2020).
- National Coordinating Council for Medication Error Reporting and Prevention. about Medication Errors. Available online: https://www.nccmerp.org/about-medication-errors (accessed on 30 August 2020).
- Stowasser, D.A.; Allinson, Y.M.; O’Leary, K.M. Understanding the medicines management pathway. J. Pharm. Pract. Res. 2004, 34, 293–296. [Google Scholar] [CrossRef]
- Australian Pharmaceutical Advisory Council. Guiding Principles to Achieve Continuity in Medication Management; Commonwealth of Australia: Canberra, Australia, 2005. [Google Scholar]
- Elliott, R.; Camacho, E.; Campbell, F.; Jankovic, D.; St James, M.M.; Kaltenthaler, E.; Wong, R.; Sculpher, M.; Faria, R. Prevalence and economic burden of medication errors in the NHS in England. In Rapid Evidence Synthesis and Economic Analysis of the Prevalence and Burden of Medication Error in the UK; Policy Research Unit in Economic Evaluation of Health and Care Interventions; Available online: http://www.eepru.org.uk/wp-content/uploads/2020/03/medication-error-report-edited-27032020.pdf/ (accessed on 30 August 2020).
- Keers, R.N.; Williams, S.D.; Cooke, J.; Ashcroft, D.M. Prevalence and nature of medication administration errors in health care settings: A systematic review of direct observational evidence. Ann. Pharmacother. 2013, 47, 237–256. [Google Scholar] [CrossRef]
- Jokanovic, N.; Tan, E.C.; Dooley, M.J.; Kirkpatrick, C.M.; Bell, J.S. Prevalence and factors associated with polypharmacy in long-term care facilities: A systematic review. J. Am. Med. Dir. Assoc. 2015, 16, 535.e1–535.e12. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Medication Errors: Technical Series on Safer Primary Care; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Tariq, A.; Georgiou, A.; Westbrook, J. Medication incident reporting in residential aged care facilities: Limitations and risks to residents’ safety. BMC Geriatr. 2012, 12, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roughead, L.; Semple, S. Literature Review: Medication Safety in Acute Care in Australia. 2013. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/Literature-Review-Medication-Safety-in-Australia-2013.pdf (accessed on 30 August 2020).
- Alldred, D.P.; Standage, C.; Fletcher, O.; Savage, I.; Carpenter, J.; Barber, N.; Raynor, D.K. The influence of formulation and medicine delivery system on medication administration errors in care homes for older people. BMJ Qual. Saf. 2011, 20, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Aged Care Complaints Commissioner. Annual Report 2017–2018; Australian Government: Canberra, Australia, 2018.
- Ferrah, N.; Lovell, J.J.; Ibrahim, J.E. Systematic review of the prevalence of medication errors resulting in hospitalization and death of nursing home residents. J. Am. Geriatr. Soc. 2017, 65, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Barber, N.D.; Alldred, D.P.; Raynor, D.K.; Dickinson, R.; Garfield, S.; Jesson, B.; Lim, R.; Savage, I.; Standage, C.; Buckle, P.; et al. Care homes’ use of medicines study: Prevalence, causes and potential harm of medication errors in care homes for older people. Qual. Saf. Health Care 2009, 18, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Szczepura, A.; Wild, D.; Nelson, S. Medication administration errors for older people in long-term residential care. BMC Geriatr. 2011, 11, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handler, S.M.; Perera, S.; Olshansky, E.F.; Studenski, S.A.; Nace, D.A.; Fridsma, D.B.; Hanlon, J.T. Identifying modifiable barriers to medication error reporting in the nursing home setting. J. Am. Med. Dir. Assoc. 2007, 8, 568–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alldred, D.P.; Kennedy, M.C.; Hughes, C.; Chen, T.F.; Miller, P. Interventions to optimise prescribing for older people in care homes. Cochrane Database Syst. Rev. 2016, 2, CD009095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiruchelvam, K.; Hasan, S.S.; Wong, P.S.; Kairuz, T. Residential aged care medication review to improve the quality of medication use: A systematic review. J. Am. Med. Dir. Assoc. 2017, 18, 87.e1–87.e14. [Google Scholar] [CrossRef]
- Gilmartin-Thomas, J.F.; Smith, F.; Wolfe, R.; Jani, Y. A comparison of medication administration errors from original medication packaging and multi-compartment compliance aids in care homes: A prospective observational study. Int. J. Nurs. Stud. 2017, 72, 15–23. [Google Scholar] [CrossRef]
- Baril, C.; Gascon, V.; St-Pierre, L.; Lagace, D. Technology and medication errors: Impact in nursing homes. Int. J. Health Care Qual. Assur. 2014, 27, 244–258. [Google Scholar] [CrossRef] [PubMed]
- McDerby, N.; Kosari, S.; Bail, K.; Shield, A.; Peterson, G.; Naunton, M. The effect of a residential care pharmacist on medication administration practices in aged care: A controlled trial. J. Clin. Pharm. Ther. 2019, 44, 595–602. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Phun, Y.T.; Bailey, M.J.; Kong, D.C.M.; Stewart, K. Development and validation of the medication regimen complexity index. Ann. Pharmacother. 2004, 38, 1369–1376. [Google Scholar] [CrossRef]
- Alves-Conceição, V.; Silva, D.T.D.; Santana, V.L.; Dos Santos, E.G.; Santos, L.M.C.; de Lyra, D.P. Evaluation of pharmacotherapy complexity in residents of long-term care facilities: A cross-sectional descriptive study. BMC Pharmacol. Toxicol. 2017, 18, 59. [Google Scholar] [CrossRef] [Green Version]
- Lalic, S.; Sluggett, J.K.; Ilomaki, J.; Wimmer, B.C.; Tan, E.C.; Robson, L.; Emery, T.; Bell, J.S. Polypharmacy and medication regimen complexity as risk factors for hospitalization among residents of long-term care facilities: A prospective cohort study. J. Am. Med. Dir. Assoc. 2016, 17, 1067.e1–1067.e6. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.; Yoon, D.; Ahn, E.K.; Hwang, H.; Park, R.W. Provider risk factors for medication administration error alerts: Analyses of a large-scale closed-loop medication administration system using RFID and barcode. Pharmacoepidemiol. Drug Saf. 2016, 25, 1387–1396. [Google Scholar] [CrossRef]
- Sluggett, J.K.; Chen, E.Y.H.; Ilomaki, J.; Corlis, M.; Hilmer, S.N.; Van Emden, J.; Ooi, C.E.; Nguyen, K.H.; Comans, T.; Hogan, M.; et al. SImplification of Medications Prescribed to Long-tErm care Residents (SIMPLER): Study protocol for a cluster randomised controlled trial. Trials 2018, 19, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sluggett, J.K.; Chen, E.Y.H.; Ilomaki, J.; Corlis, M.; Van Emden, J.; Hogan, M.; Caporale, T.; Keen, C.; Hopkins, R.; Ooi, C.E.; et al. Reducing the burden of complex medication regimens: SImplification of Medications Prescribed to Long-tErm care Residents (SIMPLER) cluster randomized controlled trial. J. Am. Med. Dir. Assoc. 2020, 21, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Hopkins, R.E.; Chen, E.Y.H.; Ilomäki, J.; Corlis, M.; Van Emden, J.; Hogan, M.; Caporale, T.; Ooi, C.E.; Hilmer, S.N.; et al. Impact of medication regimen simplification on medication administration times and health outcomes in residential aged care: 12 Month follow up of the SIMPLER randomized controlled trial. J. Clin. Med. 2020, 9, 1053. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. GEN Aged Care Data. Available online: https://www.gen-agedcaredata.gov.au (accessed on 30 April 2020).
- Chen, E.Y.H.; Sluggett, J.K.; Ilomaki, J.; Hilmer, S.N.; Corlis, M.; Picton, L.J.; Dean, L.; Alderman, C.P.; Farinola, N.; Gailer, J.; et al. Development and validation of the Medication Regimen Simplification Guide for Residential Aged CarE (MRS GRACE). Clin. Interv. Aging 2018, 13, 975–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SA Health. Patient Incident Management Tool: Safety Assessment Code Matrix. Available online: https://sahealth.sa.gov.au (accessed on 14 December 2020).
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC Classification and DDD Assignment; WHO: Oslo, Norway, 2020. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kaehr, E.; Visvanathan, R.; Malmstrom, T.K.; Morley, J.E. Frailty in nursing homes: The FRAIL-NH scale. J. Am. Med. Dir. Assoc. 2015, 16, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Paradis, E.; Sutkin, G. Beyond a good story: From Hawthorne Effect to reactivity in health professions education research. Med. Educ. 2017, 51, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Desai, R.J.; Williams, C.E.; Greene, S.B.; Pierson, S.; Caprio, A.J.; Hansen, R.A. Exploratory evaluation of medication classes most commonly involved in nursing home errors. J. Am. Med. Dir. Assoc. 2013, 14, 403–408. [Google Scholar] [CrossRef]
- Chen, E.Y.H.; Bell, J.S.; Ilomaki, J.; Keen, C.; Corlis, M.; Hogan, M.; Van Emden, J.; Hilmer, S.N.; Sluggett, J.K. Medication regimen complexity in 8 Australian residential aged care facilities: Impact of age, length of stay, comorbidity, frailty, and dependence in activities of daily living. Clin. Interv. Aging 2019, 14, 1783–1795. [Google Scholar] [CrossRef] [Green Version]
- Lampert, A.; Seiberth, J.; Haefeli, W.E.; Seidling, H.M. A systematic review of medication administration errors with transdermal patches. Expert Opin. Drug Saf. 2014, 13, 1101–1114. [Google Scholar] [CrossRef]
- Chen, E.Y.H.; Bell, J.S.; Ilomaki, J.; Corlis, M.; Hogan, M.E.; Caporale, T.; Van Emden, J.; Westbrook, J.I.; Hilmer, S.N.; Sluggett, J.K. Medication administration in Australian residential aged care: A time-and-motion study. J. Eval. Clin. Pract. 2020. [CrossRef] [PubMed]
- Australian Government Department of Health. Guiding Principles for Medication Management in Residential Aged Care Facilities. Available online: https://www.health.gov.au/resources/publications/guiding-principles-for-medication-management-in-residential-aged-care-facilities (accessed on 14 December 2020).
- Picton, L.; Lalic, S.; Ryan-Atwood, T.E.; Stewart, K.; Kirkpatrick, C.M.; Dooley, M.J.; Turner, J.P.; Bell, J.S. The role of medication advisory committees in residential aged care services. Res. Soc. Admin. Pharm. 2020, 16, 1401. [Google Scholar] [CrossRef] [PubMed]
- Jheeta, S.; Franklin, B.D. The impact of a hospital electronic prescribing and medication administration system on medication administration safety: An observational study. BMC Health Serv. Res. 2017, 17, 547. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.A.; Lee, C.Y.; Hussainy, S.Y. Evaluation of a hybrid paper-electronic medication management system at a residential aged care facility. Aust. Health Rev. 2015, 40, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Ooi, C.E.; Gibson, S.; Angley, M.T.; Corlis, M.; E Hogan, M.; Caporale, T.; A Hughes, G.; Van Emden, J.; Bell, J.S. Simplifying medication regimens for people receiving community-based home care services: Outcomes of a non-randomized pilot and feasibility study. Clin. Interv. Aging 2020, 15, 797–809. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Intervention Group (n = 99) | Comparison Group (n = 143) |
|---|---|---|
| Age, years (median, IQR *) | 86 (80–92) | 88 (81–92) |
| Female (n, %) | 67 (67.7) | 112 (78.3) |
| Urban location (n, %) | 67 (67.7) | 127 (88.8) |
| Length of stay in RACF †, years (median, IQR) | 2.3 (0.9–3.6) | 3.7 (14.9) |
| Number of medications charted (median, IQR) | 12 (9–16) | 13 (10–18) |
| Number of daily regular medication administration times (median, IQR) | 4 (3–5) | 4 (3–5) |
| FRAIL-NH ‡ score (median, IQR) | 6 (3–9) | 7 (3–10) |
| Charlson Comorbidity Index score (median, IQR) | 2 (1–4) | 2 (1–3) |
| n (%) | Intervention Group Incidents = 72 | Comparison Group Incidents = 76 |
|---|---|---|
| Incident classification | ||
| Administration error | 64 (88.8) | 62 (81.5) |
| Wrong drug/dose/route | 3 (4.1) | 1 (1.3) |
| Wrong time/date | 1 (1.3) | 2 (2.6) |
| Medication missing or N/A | 8 (11.1) | 22 (28.9) |
| Omission | 19 (26.4) | 18 (23.7) |
| Other | 28 (38.9) | 17 (22.3) |
| Not defined | 5 (6.9) | 2 (2.6) |
| Client error | 4 (5.5) | 0 |
| Pharmacy error | 3 (4.1) | 14 (18.4) |
| Prescribing error | 0 | 0 |
| Adverse reaction | 0 | 0 |
| Other | 1 (1.3) | 0 |
| Severity assessment classification (SAC) code (if reported) | ||
| 1 | 0 | 0 |
| 2 | 0 | 0 |
| 3 | 6 (8.3) | 2 (2.7) |
| 4 | 66 (91.7) | 71 (93.4) |
| WHO Anatomical Therapeutic Chemical (ATC) code * | ||
| A—Alimentary tract and metabolism | 9 | 7 |
| B—Blood/blood forming organs | 6 | 6 |
| C—Cardiovascular | 13 | 1 |
| D—Dermatologicals | 1 | 0 |
| H—Systemic hormonal preparations | 0 | 1 |
| J—Anti-infectives for systematic use | 2 | 1 |
| M—Musculoskeletal system | 2 | 2 |
| N—Nervous system | 16 | 15 |
| R—Respiratory system | 0 | 1 |
| S—Sensory organs | 1 | 0 |
| Other | ||
| DDA †, not specified | 18 | 35 |
| Dose administration aid, not specified | 0 | 2 |
| Unknown/not recorded | 5 | 1 |
| Medication administration route | ||
| Oral | 41 (56.9) | 41 (53.9) |
| Transdermal | 21 (29.1) | 32 (42.1) |
| Intramuscular | 3 (4.1) | 0 |
| Subcutaneous | 4 (5.5) | 3 (3.9) |
| Topical | 1 (1.3) | 0 |
| Rectal | 1 (1.3) | 0 |
| Other | 1 (1.3) | 0 |
| Months | Intervention Group (Incidents/100 Person-Years) | Comparison Group (Incidents/100 Person-Years) | Unadjusted Incidence Rate Ratio (95% CI †) | Adjusted * Incidence Rate Ratio (95% CI †) |
|---|---|---|---|---|
| 0 to 4 | 118 | 59 | 1.99 (1.06–3.76) | 1.40 (0.75–2.61) |
| 5 to 8 | 79 | 58 | 1.37 (0.59–3.14) | 1.09 (0.46–2.59) |
| 9 to 12 | 58 | 85 | 0.69 (0.31–1.53) | 0.58 (0.25–1.35) |
| 0 to 12 | 95 | 66 | 1.44 (0.83–2.48) | 1.13 (0.53–2.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dugré, N.; Bell, J.S.; Hopkins, R.E.; Ilomäki, J.; Chen, E.Y.H.; Corlis, M.; Van Emden, J.; Hogan, M.; Sluggett, J.K. Impact of Medication Regimen Simplification on Medication Incidents in Residential Aged Care: SIMPLER Randomized Controlled Trial. J. Clin. Med. 2021, 10, 1104. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051104
Dugré N, Bell JS, Hopkins RE, Ilomäki J, Chen EYH, Corlis M, Van Emden J, Hogan M, Sluggett JK. Impact of Medication Regimen Simplification on Medication Incidents in Residential Aged Care: SIMPLER Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(5):1104. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051104
Chicago/Turabian StyleDugré, Nicolas, J. Simon Bell, Ria E. Hopkins, Jenni Ilomäki, Esa Y. H. Chen, Megan Corlis, Jan Van Emden, Michelle Hogan, and Janet K. Sluggett. 2021. "Impact of Medication Regimen Simplification on Medication Incidents in Residential Aged Care: SIMPLER Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 5: 1104. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051104