
Role of Preoperative Assessment in Predicting Tumor-Induced Plasticity in Patients with Diffuse Gliomas

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Imaging
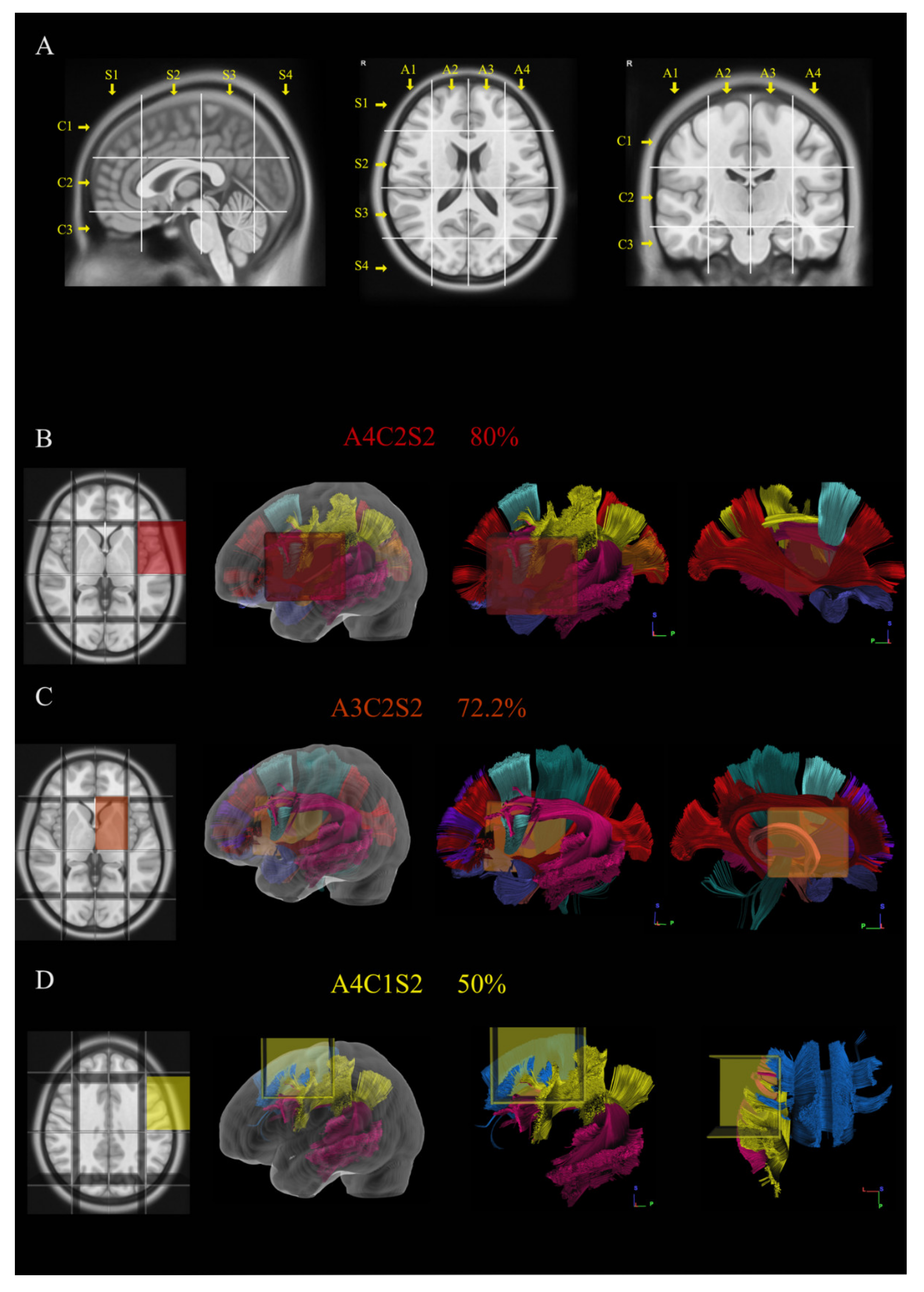
2.3. Brain-Grid Analysis
2.4. Language and Neuropsychological Evaluation
2.5. Surgical and Stimulation Technique
2.6. Postoperative Analysis of Eloquent Points
2.7. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Radiological Features
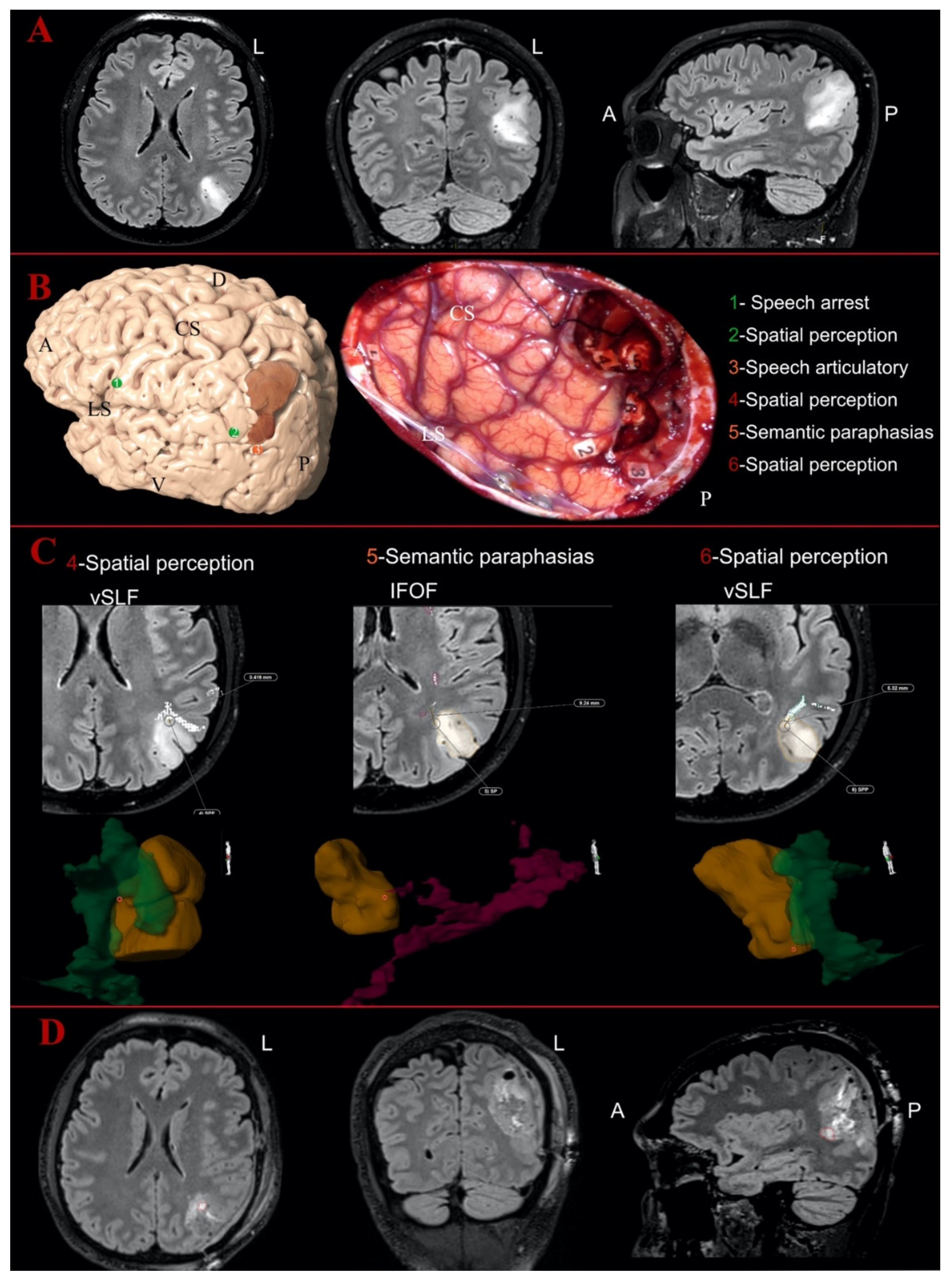
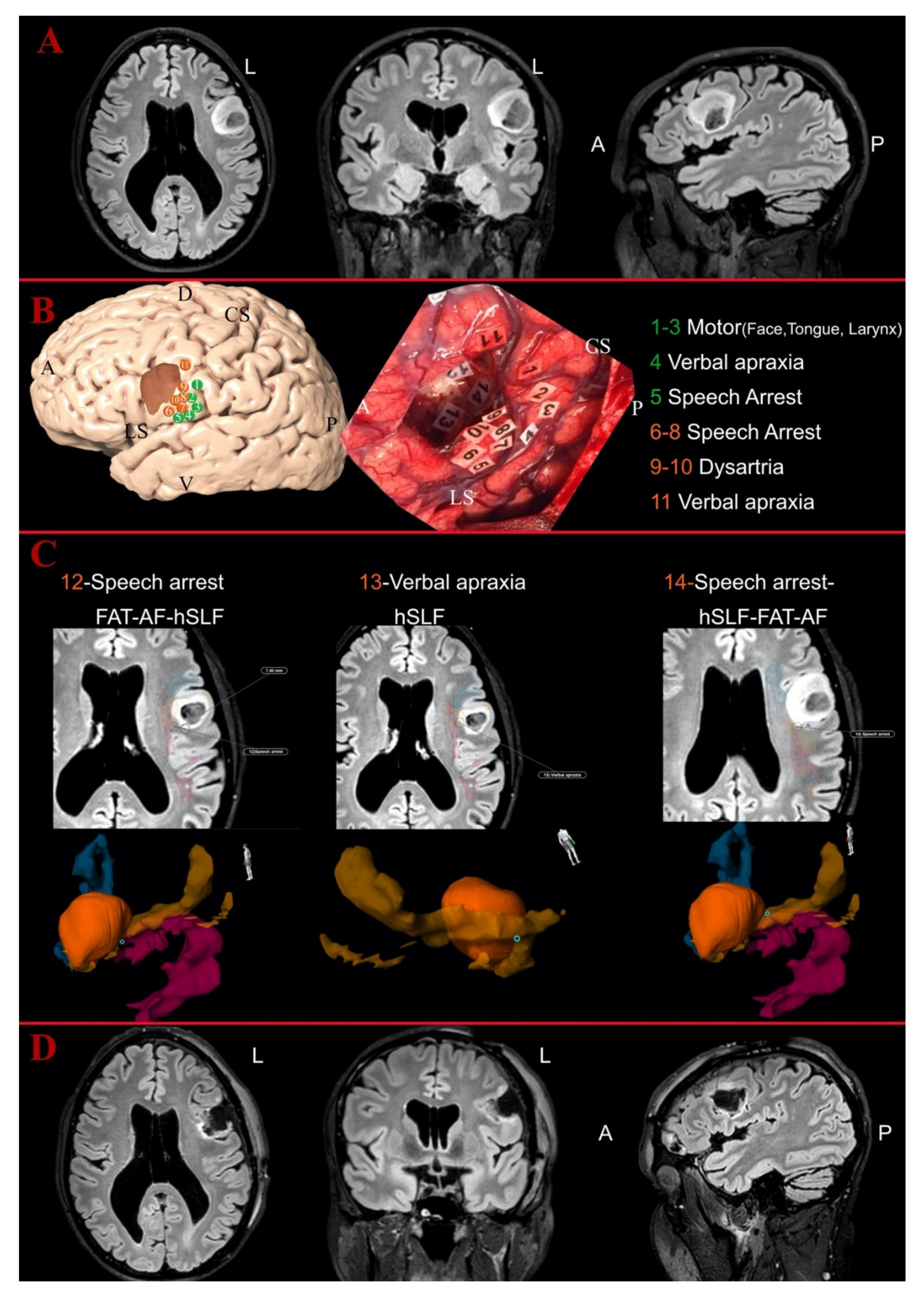
3.3. Intraoperative Findings
3.4. Postoperative Analysis
3.5. Statistical Results
4. Discussion
4.1. Preoperative NPS Assessment Was Linked with Intraoperative Findings
4.2. Correlations between Clinical Variables and Radiological/Topographical Features
4.3. Patterns of Tumor-Induced Changes in the Peritumoral White Matter Networks
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, P.; Legault, J.; Litcofsky, K.A. Neuroplasticity as a function of second language learning: Anatomical changes in the human brain. Cortex 2014, 58, 301–324. [Google Scholar] [CrossRef]
- Kong, N.W.; Gibb, W.R.; Tate, M.C. Neuroplasticity: Insights from Patients Harboring Gliomas. Neural Plast. 2016, 2016, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourdillon, P.; Apra, C.; Guénot, M.; Duffau, H. Similarities and differences in neuroplasticity mechanisms between brain gliomas and nonlesional epilepsy. Epilepsia 2017, 58, 2038–2047. [Google Scholar] [CrossRef] [Green Version]
- Duffau, H. Diffuse low-grade gliomas and neuroplasticity. Diagn. Interv. Imaging 2014, 95, 945–955. [Google Scholar] [CrossRef] [Green Version]
- Duffau, H. Hodotopy, neuroplasticity and diffuse gliomas. Neurochirurgie 2017, 63, 259–265. [Google Scholar] [CrossRef]
- Fuchs, E.; Flügge, G. Adult Neuroplasticity: More Than 40 Years of Research. Neural Plast. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Herbet, G.; Maheu, M.; Costi, E.; LaFargue, G.; Duffau, H. Mapping neuroplastic potential in brain-damaged patients. Brain 2016, 139, 829–844. [Google Scholar] [CrossRef] [PubMed]
- Desmurget, M.; Bonnetblanc, F.; Duffau, H. Contrasting acute and slow-growing lesions: A new door to brain plasticity. Brain 2006, 130, 898–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiel, A.; Habedank, B.; Herholz, K.; Kessler, J.; Winhuisen, L.; Haupt, W.F.; Heiss, W.-D. From the left to the right: How the brain compensates progressive loss of language function. Brain Lang. 2006, 98, 57–65. [Google Scholar] [CrossRef]
- Duffau, H.; Capelle, L.; Denvil, D.; Sichez, N.; Gatignol, P.; Lopes, M.; Mitchell, M.-C.; Sichez, J.-P.; Van Effenterre, R. Functional recovery after surgical resection of low grade gliomas in eloquent brain: Hypothesis of brain compensation. J. Neurol. Neurosurg. Psychiatry 2003, 74, 901–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarubbo, S.; Latini, F.; Sette, E.; Milani, P.; Granieri, E.; Fainardi, E.; Cavallo, M.A. Is the resection of gliomas in Wernicke’s area reliable? Acta Neurochir. 2012, 154, 1653–1662. [Google Scholar] [CrossRef]
- Duffau, H. Awake surgery for incidental WHO grade II gliomas involving eloquent areas. Acta Neurochir. 2011, 154, 575–584. [Google Scholar] [CrossRef]
- Picart, T.; Duffau, H. Awake resection of a left operculo-insular low-grade glioma guided by cortico-subcortical mapping. Neurosurg. Focus 2018, 45, V1. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Dong, J.W.; Del Ferraro, G.; Brennan, N.P.; Peck, K.K.; Tabar, V.; Makse, H.A.; Holodny, A.I. Functional Translocation of Broca’s Area in a Low-Grade Left Frontal Glioma: Graph Theory Reveals the Novel, Adaptive Network Connectivity. Front. Neurol. 2019, 10, 702. [Google Scholar] [CrossRef]
- Prat-Acín, R.; Galeano-Senabre, I.; López-Ruiz, P.; Ayuso-Sacido, A.; Espert-Tortajada, R. Intraoperative brain mapping of language, cognitive functions, and social cognition in awake surgery of low-grade gliomas located in the right non-dominant hemisphere. Clin. Neurol. Neurosurg. 2021, 200, 106363. [Google Scholar] [CrossRef] [PubMed]
- Vilasboas, T.; Herbet, G.; Duffau, H. Challenging the Myth of Right Nondominant Hemisphere: Lessons from Corticosubcortical Stimulation Mapping in Awake Surgery and Surgical Implications. World Neurosurg. 2017, 103, 449–456. [Google Scholar] [CrossRef]
- Nakajima, R.; Kinoshita, M.; Okita, H.; Yahata, T.; Matsui, M.; Nakada, M. Neural Networks Mediating High-Level Mentalizing in Patients With Right Cerebral Hemispheric Gliomas. Front. Behav. Neurosci. 2018, 12, 33. [Google Scholar] [CrossRef] [Green Version]
- Nibali, M.C.; Leonetti, A.; Puglisi, G.; Rossi, M.; Sciortino, T.; Gay, L.G.; Arcidiacono, U.A.; Howells, H.; Viganò, L.; Zito, P.C.; et al. Preserving Visual Functions During Gliomas Resection: Feasibility and Efficacy of a Novel Intraoperative Task for Awake Brain Surgery. Front. Oncol. 2020, 10, 1485. [Google Scholar] [CrossRef] [PubMed]
- Szalisznyo, K.; Silverstein, D.N.; Duffau, H.; Smits, A. Pathological Neural Attractor Dynamics in Slowly Growing Gliomas Supports an Optimal Time Frame for White Matter Plasticity. PLoS ONE 2013, 8, e69798. [Google Scholar] [CrossRef]
- Smits, A.; Jakola, A.S. Clinical Presentation, Natural History, and Prognosis of Diffuse Low-Grade Gliomas. Neurosurg. Clin. N. Am. 2019, 30, 35–42. [Google Scholar] [CrossRef]
- Berger, M.S.; Ghatan, S.; Haglund, M.M.; Dobbins, J.; Ojemann, G.A. Low-grade gliomas associated with intractable epilepsy: Seizure outcome utilizing electrocorticography during tumor resection. J. Neurosurg. 1993, 79, 62–69. [Google Scholar] [CrossRef]
- Pallud, J.; Audureau, E.; Blonski, M.; Sanai, N.; Bauchet, L.; Fontaine, D.; Mandonnet, E.; Dezamis, E.; Psimaras, D.; Guyotat, J.; et al. Epileptic seizures in diffuse low-grade gliomas in adults. Brain 2014, 137, 449–462. [Google Scholar] [CrossRef] [Green Version]
- Pallud, J.; McKhann, G.M. Diffuse Low-Grade Glioma-Related Epilepsy. Neurosurg. Clin. N. Am. 2019, 30, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Rudà, R.; Bello, L.; Duffau, H.; Soffietti, R. Seizures in low-grade gliomas: Natural history, pathogenesis, and outcome after treatments. Neuro Oncol. 2012, 14, iv55–iv64. [Google Scholar] [CrossRef]
- De Groot, M.; Reijneveld, J.C.; Aronica, E.; Heimans, J.J. Epilepsy in patients with a brain tumour: Focal epilepsy requires focused treatment. Brain 2011, 135, 1002–1016. [Google Scholar] [CrossRef] [PubMed]
- Douw, L.; Van Dellen, E.; De Groot, M.; Heimans, J.J.; Klein, M.; Stam, C.J.; Reijneveld, J.C. Epilepsy is related to theta band brain connectivity and network topology in brain tumor patients. BMC Neurosci. 2010, 11, 103. [Google Scholar] [CrossRef] [Green Version]
- Smits, A.; Zetterling, M.; Lundin, M.; Melin, B.; Fahlstrãm, M.; Grabowska, A.; Larsson, E.-M.; Berntsson, S.G. Neurological Impairment Linked with Cortico-Subcortical Infiltration of Diffuse Low-Grade Gliomas at Initial Diagnosis Supports Early Brain Plasticity. Front. Neurol. 2015, 6, 137. [Google Scholar] [CrossRef] [PubMed]
- Ius, T.; Angelini, E.; de Schotten, M.T.; Mandonnet, E.; Duffau, H. Evidence for potentials and limitations of brain plasticity using an atlas of functional resectability of WHO grade II gliomas: Towards a “minimal common brain. ” NeuroImage 2011, 56, 992–1000. [Google Scholar] [CrossRef]
- Sarubbo, S.; De Benedictis, A.; Merler, S.; Mandonnet, E.; Balbi, S.; Granieri, E.; Duffau, H. Towards a functional atlas of human white matter. Hum. Brain Mapp. 2015, 36, 3117–3136. [Google Scholar] [CrossRef]
- Latini, F.; Fahlström, M.; Berntsson, S.G.; Larsson, E.-M.; Smits, A.; Ryttlefors, M. A novel radiological classification system for cerebral gliomas: The Brain-Grid. PLoS ONE 2019, 14, e0211243. [Google Scholar] [CrossRef] [Green Version]
- Latini, F.; Fahlström, M.; Hesselager, G.; Zetterling, M.; Ryttlefors, M. Differences in the preferential location and invasiveness of diffuse low-grade gliomas and their impact on outcome. Cancer Med. 2020, 9, 5446–5458. [Google Scholar] [CrossRef]
- Sanai, N.; Berger, M.S. GLIOMA EXTENT OF RESECTION AND ITS IMPACT ON PATIENT OUTCOME. Neurosurgery 2008, 62, 753–766. [Google Scholar] [CrossRef] [Green Version]
- Sanai, N.; Polley, M.-Y.; Berger, M.S. Insular glioma resection: Assessment of patient morbidity, survival, and tumor progression. J. Neurosurg. 2010, 112, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Satoer, D.; Visch-Brink, E.; Dirven, C.; Vincent, A. Glioma surgery in eloquent areas: Can we preserve cognition? Acta Neurochir. 2016, 158, 35–50. [Google Scholar] [CrossRef] [Green Version]
- Satoer, D.; Visch-Brink, E.; Smits, M.; Kloet, A.; Looman, C.; Dirven, C.; Vincent, A. Long-term evaluation of cognition after glioma surgery in eloquent areas. J. Neuro-Oncol. 2014, 116, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. Awake mapping of the brain connectome in glioma surgery: Concept is stronger than technology. Eur. J. Surg. Oncol. (EJSO) 2015, 41, 1261–1263. [Google Scholar] [CrossRef] [PubMed]
- Farquharson, S.; Tournier, J.-D.; Calamante, F.; Fabinyi, G.; Schneider-Kolsky, M.; Jackson, G.D.; Connelly, A. White matter fiber tractography: Why we need to move beyond DTI. J. Neurosurg. 2013, 118, 1367–1377. [Google Scholar] [CrossRef] [Green Version]
- Duffau, H. Diffusion Tensor Imaging Is a Research and Educational Tool, but Not Yet a Clinical Tool. World Neurosurg. 2014, 82, e43–e45. [Google Scholar] [CrossRef]
- Nibali, M.C.; Rossi, M.; Sciortino, T.; Riva, M.; Gay, L.G.; Pessina, F.; Bello, L. Preoperative surgical planning of glioma: Limitations and reliability of fMRI and DTI tractography. J. Neurosurg. Sci. 2019, 63, 127–134. [Google Scholar] [CrossRef]
- Duffau, H. Brain plasticity: From pathophysiological mechanisms to therapeutic applications. J. Clin. Neurosci. 2006, 13, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. Is non-awake surgery for supratentorial adult low-grade glioma treatment still feasible? Neurosurg. Rev. 2017, 41, 133–139. [Google Scholar] [CrossRef]
- Duffau, H. Mapping the connectome in awake surgery for gliomas: An update. J. Neurosurg. Sci. 2017, 61, 612–630. [Google Scholar]
- De Witt Hamer, P.C.; Gil Robles, S.; Zwinderman, A.H.; Duffau, H.; Berger, M.S. Impact of Intraoperative Stimulation Brain Mapping on Glioma Surgery Outcome: A Meta-Analysis. J. Clin. Oncol. 2012, 30, 2559–2565. [Google Scholar] [CrossRef] [Green Version]
- Freyschlag, C.F.; Krieg, S.M.; Kerschbaumer, J.; Pinggera, D.; Forster, M.-T.; Cordier, D.; Rossi, M.; Miceli, G.; Roux, A.; Reyes, A.; et al. Imaging practice in low-grade gliomas among European specialized centers and proposal for a minimum core of imaging. J. Neuro Oncol. 2018, 139, 699–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thust, S.C.; Heiland, S.; Falini, A.; Jäger, H.R.; Waldman, A.D.; Sundgren, P.C.; Godi, C.; Katsaros, V.K.; Ramos, A.; Bargallo, N.; et al. Glioma imaging in Europe: A survey of 220 centres and recommendations for best clinical practice. Eur. Radiol. 2018, 28, 3306–3317. [Google Scholar] [CrossRef] [Green Version]
- Dodo, T.; Okada, T.; Yamamoto, A.; Kanagaki, M.; Fushimi, Y.; Okada, T.; Sakata, A.; Arakawa, Y.; Miyamoto, S.; Togashi, K. T1-weighted MR imaging of glioma at 3T: A comparative study of 3D MPRAGE vs. conventional 2D spin-echo imaging. Clin. Imaging 2016, 40, 1257–1261. [Google Scholar] [CrossRef]
- Latini, F.; Larsson, E.-M.; Ryttlefors, M. Rapid and Accurate MRI Segmentation of Peritumoral Brain Edema in Meningiomas. Clin. Neuroradiol. 2015, 27, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Catani, M.; De Schotten, M.T. A diffusion tensor imaging tractography atlas for virtual in vivo dissections. Cortex 2008, 44, 1105–1132. [Google Scholar] [CrossRef] [PubMed]
- Mori, S.; Kaufmann, W.E.; Davatzikos, C.; Stieltjes, B.; Amodei, L.; Fredericksen, K.; Pearlson, G.D.; Melhem, E.R.; Solaiyappan, M.; Raymond, G.V.; et al. Imaging cortical association tracts in the human brain using diffusion-tensor-based axonal tracking. Magn. Reson. Med. 2002, 47, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Wakana, S.; Caprihan, A.; Panzenboeck, M.M.; Fallon, J.H.; Perry, M.; Gollub, R.L.; Hua, K.; Zhang, J.; Jiang, H.; Dubey, P.; et al. Reproducibility of quantitative tractography methods applied to cerebral white matter. NeuroImage 2007, 36, 630–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riva, M.; Fava, E.; Gallucci, M.; Comi, A.; Casarotti, A.; Alfiero, T.; Raneri, F.A.; Pessina, F.; Bello, L. Monopolar high-frequency language mapping: Can it help in the surgical management of gliomas? A comparative clinical study. J. Neurosurg. 2016, 124, 1479–1489. [Google Scholar] [CrossRef] [Green Version]
- Rossi, M.; Sani, S.; Nibali, M.C.; Fornia, L.; Bello, L.; Byrne, R.W. Mapping in Low-Grade Glioma Surgery. Neurosurg. Clin. N. Am. 2019, 30, 55–63. [Google Scholar] [CrossRef]
- Verst, S.; De Aguiar, P.; Joaquim, M.; Vieira, V.; Sucena, A.; Maldaun, M. Monopolar 250–500 Hz language mapping: Results of 41 patients. Clin. Neurophysiol. Pr. 2019, 4, 1–8. [Google Scholar] [CrossRef]
- Gogos, A.J.; Young, J.S.; Morshed, R.A.; Hervey-Jumper, S.L.; Berger, M.S. Awake glioma surgery: Technical evolution and nuances. J. Neuro-Oncol. 2020, 147, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Gerard, I.J.; Kersten-Oertel, M.; Petrecca, K.; Sirhan, D.; Hall, J.A.; Collins, D.L. Brain shift in neuronavigation of brain tumors: A review. Med. Image Anal. 2017, 35, 403–420. [Google Scholar] [CrossRef]
- Ohue, S.; Kumon, Y.; Nagato, S.; Kohno, S.; Harada, H.; Nakagawa, K.; Kikuchi, K.; Miki, H.; Ohnishi, T. Evaluation of intraoperative brain shift using an ultrasound-linked navigation system for brain tumor surgery. Neurol. Med. Chir. 2010, 50, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, I.-A., Jr.; Lindseth, F.; Rygh, O.M.; Berntsen, E.M.; Selbekk, T.; Xu, J.; Hernes, T.A.N.; Harg, E.; Håberg, A.; Unsgaard, G. Functional neuronavigation combined with intra-operative 3D ultrasound: Initial experiences during surgical resections close to eloquent brain areas and future directions in automatic brain shift compensation of preoperative data. Acta Neurochir. 2007, 149, 365–378. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Schiff, D. Low-grade Gliomas. Contin. Lifelong Learn. Neurol. 2017, 23, 1564–1579. [Google Scholar] [CrossRef]
- Smith, J.S.; Chang, E.F.; Lamborn, K.R.; Chang, S.M.; Prados, M.D.; Cha, S.; Tihan, T.; Vandenberg, S.; McDermott, M.W.; Berger, M.S. Role of Extent of Resection in the Long-Term Outcome of Low-Grade Hemispheric Gliomas. J. Clin. Oncol. 2008, 26, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Hottinger, A.F.; Hegi, M.E.; Baumert, B.G. Current management of low-grade gliomas. Curr. Opin. Neurol. 2016, 29, 782–788. [Google Scholar] [CrossRef] [Green Version]
- Cochereau, J.; Herbet, G.; Duffau, H. Patients with incidental WHO grade II glioma frequently suffer from neuropsychological disturbances. Acta Neurochir. 2015, 158, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. Toward an “Active” Cognitive Assessment in Patients with Diffuse Low-Grade Glioma. World Neurosurg. 2014, 82, e129–e131. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. Functional Mapping before and after Low-Grade Glioma Surgery: A New Way to Decipher Various Spatiotemporal Patterns of Individual Neuroplastic Potential in Brain Tumor Patients. Cancers 2020, 12, 2611. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H. Does post-lesional subcortical plasticity exist in the human brain? Neurosci. Res. 2009, 65, 131–135. [Google Scholar] [CrossRef]
- Esposito, R.; Mattei, P.A.; Briganti, C.; Romani, G.L.; Tartaro, A.; Caulo, M. Modifications of Default-Mode Network Connectivity in Patients with Cerebral Glioma. PLoS ONE 2012, 7, e40231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briganti, C.; Sestieri, C.; Mattei, P.; Esposito, R.; Galzio, R.; Tartaro, A.; Romani, G.; Caulo, M. Reorganization of Functional Connectivity of the Language Network in Patients with Brain Gliomas. Am. J. Neuroradiol. 2012, 33, 1983–1990. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Liang, Y.; Chen, H.; Wang, W.; Wang, Y.; Liang, Y.; Zhang, Y. Structural changes in white matter lesion patients and their correlation with cognitive impairment. Neuropsychiatr. Dis. Treat. 2019, ume 15, 1355–1363. [Google Scholar] [CrossRef] [Green Version]
- Onay, A.; Eser, H.Y.; Yildiz, C.U.; Aslan, S.; Tali, E.T. A combined VBM and DTI study of schizophrenia: Bilateral decreased insula volume and cerebral white matter disintegrity corresponding to subinsular white matter projections unlinked to clinical symptomatology. Diagn. Interv. Radiol. 2017, 23, 390–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Wang, X.; Wu, Q.; Spagna, A.; Yang, J.; Yuan, C.; Wu, Y.; Gao, Z.; Hof, P.R.; Fan, J. Anterior insular cortex is a bottleneck of cognitive control. NeuroImage 2019, 195, 490–504. [Google Scholar] [CrossRef]
- Mandonnet, E.; Delattre, J.-Y.; Tanguy, M.-L.; Swanson, K.R.; Carpentier, A.F.; Duffau, H.; Cornu, P.; Alvord, E.C.; Capelle, L. Continuous growth of mean tumor diameter in a subset of grade II gliomas. Ann. Neurol. 2003, 53, 524–528. [Google Scholar] [CrossRef]
- Lima, G.L.D.O.; Zanello, M.; Mandonnet, E.; Taillandier, L.; Pallud, J.; Duffau, H. Incidental diffuse low-grade gliomas: From early detection to preventive neuro-oncological surgery. Neurosurg. Rev. 2015, 39, 377–384. [Google Scholar] [CrossRef]
- Zetterling, M.; Roodakker, K.R.; Berntsson, S.G.; Edqvist, P.-H.; Latini, F.; Landtblom, A.-M.; Pontén, F.; Alafuzoff, I.; Larsson, E.-M.; Smits, A. Extension of diffuse low-grade gliomas beyond radiological borders as shown by the coregistration of histopathological and magnetic resonance imaging data. J. Neurosurg. 2016, 125, 1155–1166. [Google Scholar] [CrossRef] [Green Version]
- Bosma, I.; Douw, L.; Bartolomei, F.; Heimans, J.J.; Van Dijk, B.W.; Postma, T.J.; Stam, C.J.; Reijneveld, J.C.; Klein, M. Synchronized brain activity and neurocognitive function in patients with low-grade glioma: A magnetoencephalography study. Neuro-Oncol. 2008, 10, 734–744. [Google Scholar] [CrossRef]
- Bartolomei, F.; Bosma, I.; Klein, M.; Baayen, J.C.; Reijneveld, J.C.; Postma, T.J.; Heimans, J.J.; Van Dijk, B.W.; De Munck, J.C.; De Jongh, A.; et al. How do brain tumors alter functional connectivity? A magnetoencephalography study. Ann. Neurol. 2005, 59, 128–138. [Google Scholar] [CrossRef]
- Ponten, S.; Bartolomei, F.; Stam, C. Small-world networks and epilepsy: Graph theoretical analysis of intracerebrally recorded mesial temporal lobe seizures. Clin. Neurophysiol. 2007, 118, 918–927. [Google Scholar] [CrossRef]
- Duffau, H.; Capelle, L. Preferential brain locations of low-grade gliomas. Cancer 2004, 100, 2622–2626. [Google Scholar] [CrossRef]
- Ghinda, C.D.; Duffau, H. Network Plasticity and Intraoperative Mapping for Personalized Multimodal Management of Diffuse Low-Grade Gliomas. Front. Surg. 2017, 4, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Young, K. White matter plasticity in adulthood. Neuroscience 2014, 276, 148–160. [Google Scholar] [CrossRef]
- Yu, C.S.; Li, K.C.; Xuan, Y.; Ji, X.M.; Qin, W. Diffusion tensor tractography in patients with cerebral tumors: A helpful technique for neurosurgical planning and postoperative assessment. Eur. J. Radiol. 2005, 56, 197–204. [Google Scholar] [CrossRef]
- Sarubbo, S.; Tate, M.; De Benedictis, A.; Merler, S.; Moritz-Gasser, S.; Herbet, G.; Duffau, H. Mapping critical cortical hubs and white matter pathways by direct electrical stimulation: An original functional atlas of the human brain. NeuroImage 2020, 205, 116237. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Type of Variables | Values | |
|---|---|---|
| Demographic variables | ||
| Age | mean (SD) | 40.36 (10.8) |
| Gender | m (%)/f (%) | 25 (69.4)/11(30.6) |
| Radiological variables | ||
| Tumor volume | mean (SD) | 57.30 (47.4) |
| Tumor border | sharp (%)/diffuse (%) | 14 (38.9)/22(61.1) |
| Brain-Grid voxels | median (IQR) | 6 (4–8) |
| Clinical variables | ||
| Onset symptoms | n (%) | |
| EP focal | 15(41.7) | |
| Ep generalized | 11(30.6) | |
| Headache | 1 (2.8) | |
| Incidental | 9 (25.0) | |
| Preoperative language imp. | y (%)/n (%) | 24 (66.7)/12 (33.3) |
| Preoperative NPS imp.* * only in 26 patients | y (%)/n (%) | 22 (84.6)/4 (15.4) |
| Histo-pathological variables | ||
| Histology | n (%) | |
| Astrocytomas | 23 (63.9) | |
| Oligodendrogliomas | 13 (36.1) | |
| Grade | n (%) | |
| A2 | 12 (33.3) | |
| A3 | 11 (30.6) | |
| O2 | 4 (11.1) | |
| O3 | 9 (25.0) | |
| IDH 1-2 status | (m/NOS) | |
| A2 | 8/4 | |
| A3 | 9/2 | |
| O2 | 2/2 | |
| O3 | 7/2 | |
| Surgical variables | ||
| Eloquent tumor | y (%)/n (%) | 27 (75)/9 (25) |
| Intra-tumoral spots cortical. | mean (SD) | 0.36 (0.93) |
| Intra-tumoral spots Subcortical | mean (SD) | 1.33 (1.37) |
| Peritumoral spots cortical | mean (SD) | 1.39 (1.47) |
| Peritumoral subcortical | mean (SD) | 1.00 (1.37) |
| Intra-tumoral spots | mean (SD) | 1.61 (1.69) |
| Peritumoral spots | mean (SD) | 2.36 (2.1) |
| Cortical spots total | mean (SD) | 4.33 (2.7) |
| Subcortical spots total | mean (SD) | 2.72 (2.17) |
| Resection grade | mean (SD) | 79.07 (15.8) |
| Outcome variables | ||
| Survival | years (SD) | 3.36 (1.8) |
| Pat N | Localization | Intratumoral | Peritumoral | Outside Tumor Border | Total Number | ||||
|---|---|---|---|---|---|---|---|---|---|
| C | SC | C | SC | C | SC | C | SC | ||
| 1 | F-o L | SO | SO | 1 | 1 | ||||
| 2 | F L | SO | SA | SO | 1 | 2 | |||
| 3 | F-T-I L | Hand (M) | SO Face (M) | 2 | 1 | ||||
| 4 | F-T-I L | Arm (M) | SOx2 | 2 | 1 | ||||
| 5 | F-I L | SP SP | SO SA | SO | 3 | 2 | |||
| 6 | T-I L | SA SO | SO x3 Mouth (M) | 6 | 0 | ||||
| 7 | F-T-I L | An | SO SA | SO Mouth (M) | 4 | 1 | |||
| 8 | F-T-I L | SA, Mouth (M) | 2 | 0 | |||||
| 9 | F-I L | SP | SO, Mouth (M) | 2 | 1 | ||||
| 10 | F L | SOx2 Mouth (M) | SAx2 | Hand (M) Face (M) Mouth (M)x2 Tongue (M) An x2 SA | 11 | 2 | |||
| 11 | T-I L | SO | SOx2 Hand (M) SA | 5 | 0 | ||||
| 12 | DLPFC L | SA | SA Mc | Hand (M)x3 PP SA | 6 | 2 | |||
| 13 | F-T-I L | SO | SP SA Mouth (M) | Mouth (M) Tongue (M) | SP SAx2 An | 6 | 3 | ||
| 14 | F-T-I L | An | SP SA | SOx2 Face (M) An | 5 | 2 | |||
| 15 | F-I L | SA | SAx2 | SO Mouth (M) SAx2 | 6 | 1 | |||
| 16 | DLPFC R | Mc | Hand (M) | Hand (M) Arm (M) Tongue (M) | 4 | 1 | |||
| 17 | F o L | SOx3 SAx3 | SA Sox2 | Face (M) Mouth (M)x2 SO SA | 11 | 3 | |||
| 18 | P L | WMx3 | Hand (S) Arm (S) | Arm (S) | Leg (M) Arm (M) | 4 | 4 | ||
| 19 | T-P-O L | Anx3 Vifx2 Mouth (M) | Anx2 | Tongue (S) | 3 | 6 | |||
| 20 | F-I L | An Mouth (M) SO | Tongue (M) Mouth (M) SOx2 | Tongue (M)x2 Mouth (M) | 7 | 3 | |||
| 21 | P L | SAx2 Mouth (S) | SO Mouth (M) Tongue (S) | Mouth (M) Hand (M) | 3 | 5 | |||
| 22 | F-T-I L | SO SP | SP | Mouth (M)x2 Face (M) Tongue (M)x2 SAx2 PPx2 | 11 | 1 | |||
| 23 | T-P-I L | SAX2 SO Aux2 | SP | SP | Mouth (M) SA PP | SP | 8 | 3 | |
| 24 | T-O L | R | Anx2 SA | SPx2 | SA | VifX2 | 4 | 5 | |
| 25 | F L | An | WM SA | Ha (M) SA | 3 | 2 | |||
| 26 | F-I L | SAx2 SP | SA Tongue (M) SO SA | VA SA | SOx2 | Arm (M) Hand (M) Face (M) | 6 | 8 | |
| 27 | F L | SP | Anx3 SA SP | SO | 1 | 6 | |||
| 28 | T-I-O R | SO Face (M) | 2 | 0 | |||||
| 29 | T-I L | PPx2 | Vis PPx2 | SO Face (M) | 2 | 5 | |||
| 30 | T-I L | SP | SP Vis | SO | 1 | 3 | |||
| 31 | T-I L | SP | SP | SOx3 | Arm (M) SO | 4 | 3 | ||
| 32 | P L | SA | Hand (M) SPP | An x2 | Face (M) | 3 | 3 | ||
| 33 | F-T-I L | PPx2 An Mc | PPx2 Mc | SOx2 | 5 | 4 | |||
| 34 | P L | Mouth (S) | SA Mouth (M) | PP SAx4 | SOx2 Mouth (M) | SAx2 SO Vis | 6 | 9 | |
| 35 | P L | SPPx2 | SPP | SP | SO SA | 3 | 3 | ||
| 36 | SMA L | Mc | Mc, AN | SO | Hand (M) | 2 | 3 | ||
| Variables | Age | Tumor Volume | Brain-Grid Voxels | Intratumoral Cortical | Intratumoral Subcortical | Peritumoral Cortical | Peritumoral Subcortical | Resection Grade | |
|---|---|---|---|---|---|---|---|---|---|
| Age | Corr. Co | 1 | 0.161 | 0.101 | 0.406 * | −0.161 | −0.451 * | −0.089 | −0.127 |
| p | 0.349 | 0.557 | 0.014 | 0.399 | 0.006 | 0.605 | 0.462 | ||
| Tumor volume | Corr. Co | 0.161 | 1 | 0.689 * | 0.17 | 0.094 | −0.226 | −0.511 * | −0.627 * |
| p | 0.349 | 0 | 0.32 | 0.587 | 0.184 | 0.001 | 0 | ||
| Brain-Grid voxels | Corr. Co | 0.101 | 0.689 * | 1 | 0.012 | 0.155 | −0.112 | −0.326 | −0.316 |
| p | 0.557 | 0 | 0.944 | 0.366 | 0.517 | 0.052 | 0.06 | ||
| Intratumoral eloquent spots cortical | Corr. Co | 0.406 * | 0.17 | 0.012 | 1 | 0.024 | −0.366 * | −0.037 | −0.411 * |
| p | 0.014 | 0.32 | 0.944 | 0.891 | 0.028 | 0.828 | 0.013 | ||
| Intratumoral eloquent spots Subcortical | Corr. Co | −0.145 | 0.094 | 0.155 | 0.024 | 1 | 0.264 | −0.281 | −0.122 |
| p | 0.399 | 0.587 | 0.366 | 0.891 | 0.119 | 0.097 | 0.477 | ||
| Peritumoral eloquent spots cortical | Corr. Co | −0.451 * | −0.226 | −0.112 | −0.366 * | 0.264 | 1 | 0.068 | 0.153 |
| p | 0.006 | 0.184 | 0.517 | 0.028 | 0.119 | 0.695 | 0.372 | ||
| Peritumoral eloquent spots subcortical | Corr. Co | −0.089 | −0.511 * | −0.326 | −0.037 | −0.281 | 0.068 | 1 | 0.501 * |
| p | 0.605 | 0.001 | 0.052 | 0.828 | 0.097 | 0.695 | 0.002 | ||
| Resection grade | Corr. Co | −0.127 | −0.627 * | −0.316 | −0.411 * | −0.122 | 0.153 | 0.501 * | 1 |
| p | 0.462 | 0 | 0.06 | 0.013 | 0.477 | 0.372 | 0.002 | ||
| Variables | Correlation Analysis | ||
|---|---|---|---|
| X2 | |||
| p | Coefficient | Strength/Direction | |
| Eloquent tumors/Age cut-off | 0.439 | 0.128 | |
| Eloquent tumors/Gender | 0.531 | 0.104 | |
| Eloquent tumors/Tumor volume cut-off | 1.00 | 0.000 | |
| Eloquent tumors/Radiological border | 0.693 | 0.066 | |
| Eloquent tumors/BG voxels cut-off | 0.654 | 0.074 | |
| Eloquent tumors/A3C2S2 | 0.197 | 0.210 | |
| Eloquent tumors/A4C1S2 | 0.700 | 0.064 | |
| Eloquent tumors/A4C2S2 | 0.808 | 0.040 | |
| Epilepsy/Age cut-off | 0.739 | 0.055 | |
| Epilepsy/Gender | 0.446 | 0.126 | |
| Epilepsy/Tumor volume cut-off | 0.001 * | 0.494 | Moderate/+ |
| Epilepsy/Radiological border | 0.497 | 0.112 | |
| Epilepsy/BG voxels cut-off | 0.244 | 191 | |
| Epilepsy/A3C2S2 | 0.007 * | 0.407 | Moderate/+ |
| Epilepsy/A4C1S2 | 0.457 | 0.123 | |
| Epilepsy/A4C2S2 | 0.000 * | 0.536 | High/+ |
| NPS impairment/Age cut-off | 0.208 | 0.240 | |
| NPS impairment/Gender | 0.102 | 0.305 | |
| NPS impairment/Tumor volume cut-off | 0.356 | 0.178 | |
| NPS impairment/Radiological border | 0.150 | 0.272 | |
| NPS impairment/BG voxels cut-off | 0.019 * | 0.418 | Moderate/+ |
| NPS impairment/A3C2S2 | 0.482 | 0.137 | |
| NPS impairment/A4C1S2 | 0.054 | 0.307 | |
| NPS impairment/A4C2S2 | 0.187 | 0.251 | |
| Language impairment/Age cut-off | 0.058 | 0.302 | |
| Language impairment/Gender | 0.798 | 0.043 | |
| Language impairment/Tumor volume cu-off | 0.058 | 0.302 | |
| Language impairment/Radiological border | 0.091 | 0.271 | |
| Language impairment/BG voxels cut-off | 0.236 | 0.194 | |
| Language impairment/A3C2S2 | 0.188 | 0.214 | |
| Language impairment/A4C1S2 | 0.157 | 0.229 | |
| Language impairment/A4C2S2 | 0.766 | 0.050 | |
| Eloquent tumors/Epilepsy | 0.667 | 0.071 | |
| Eloquent tumors/NPS impairment | 0.562 | 0.113 | |
| Eloquent tumors/Language impairment | 1.00 | 0.000 | |
| Epilepsy/NPS impairment | 0.114 | 0.296 | |
| Epilepsy/Language impairment | 0.792 | 0.044 | |
| NPS impairment/Language impairment | 0.065 | 0.340 | |
| Variables | Binary Logistic Regression | ||
|---|---|---|---|
| Univariate | p | HR | CI (95%) |
| NPS impairment/intratumoral eloquent spots cortical | 0.201 | 3.679 | 0.501–27.036 |
| NPS impairment/intratumoral eloquent spots subcortical | 0.019 * | 2.200 | 1.140–4.244 |
| NPS impairment/peritumoral eloquent spots cortical | 0.096 | 1.464 | 0.935–2.294 |
| NPS impairment/peritumoral eloquent spots subcortical | 0.112 | 1.548 | 0.903–2.651 |
| Epilepsy/intratumoral eloquent spots cortical | 0.105 | 5.429 | 0.704–41.875 |
| Epilepsy/intratumoral eloquent spots subcortical | 0.028 * | 1.766 | 1.064–2.929 |
| Epilepsy/peritumoral eloquent spots cortical | 0.047 * | 1.533 | 1.069–2.337 |
| Epilepsy/peritumoral eloquent spots subcortical | 0.251 | 1.288 | 0.836–1.985 |
| Language impairment/Intratumoral eloquent spots cortical | 0.196 | 2.554 | 0.616–10.583 |
| Language impairment/Intratumoral eloquent spots subcortical | 0.098 | 1.421 | 0.937–2.153 |
| Language impairment/Peritumoral eloquent spots cortical | 0.511 | 1.118 | 0.802–1.558 |
| Language impairment/Peritumoral eloquent spots subcortical | 0.693 | 0.924 | 0.624–1.368 |
| NPS impairment/A3C2S2 infiltration | 0.007 * | 7.500 | 1.715–32.796 |
| NPS impairment/A4C1S2 infiltration | 0.121 | 2.500 | 0.784–7.971 |
| NPS impairment/A4C2S2 infiltration | 0.019 * | 3.750 | 1.245–11.299 |
| Epilepsy/A3C2S2 infiltration | 0.002 * | 5.500 | 1.895–15.960 |
| Epilepsy/A4C1S2 infiltration | 0.127 | 3.500 | 1.152–10.633 |
| Epilepsy/A4C2S2 infiltration | 0.001 * | 6.250 | 2.175–17.958 |
| Language impairment/A3C2S2 infiltration | 0.024 * | 2.714 | 1.141–6.457 |
| Language impairment/A4C1S2 infiltration | 0.638 | 1.250 | 0.493–3.167 |
| Language impairment/A4C2S2 infiltration | 0.100 | 1.900 | 0.883–4.086 |
| Multivariate | |||
| Eloquent tumors/Preoperative NPS impairment | 0.003 * | 6.333 | 1.874–21.402 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latini, F.; Axelson, H.; Fahlström, M.; Jemstedt, M.; Alberius Munkhammar, Å.; Zetterling, M.; Ryttlefors, M. Role of Preoperative Assessment in Predicting Tumor-Induced Plasticity in Patients with Diffuse Gliomas. J. Clin. Med. 2021, 10, 1108. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051108
Latini F, Axelson H, Fahlström M, Jemstedt M, Alberius Munkhammar Å, Zetterling M, Ryttlefors M. Role of Preoperative Assessment in Predicting Tumor-Induced Plasticity in Patients with Diffuse Gliomas. Journal of Clinical Medicine. 2021; 10(5):1108. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051108
Chicago/Turabian StyleLatini, Francesco, Hans Axelson, Markus Fahlström, Malin Jemstedt, Åsa Alberius Munkhammar, Maria Zetterling, and Mats Ryttlefors. 2021. "Role of Preoperative Assessment in Predicting Tumor-Induced Plasticity in Patients with Diffuse Gliomas" Journal of Clinical Medicine 10, no. 5: 1108. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051108