
Challenges and Advances in Managing Thrombocytopenic Cancer Patients


1
Institute of Hematology, Davidoff Cancer Center, Rabin Medical Center, Petah Tikva 4941492, Israel
2
Sackler School of Medicine, Tel Aviv University, Tel Aviv 6997801, Israel
3
Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, 6229 ER Maastricht, The Netherlands
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2021, 10(6), 1169; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10061169
Submission received: 31 January 2021
/
Revised: 2 March 2021
/
Accepted: 8 March 2021
/
Published: 11 March 2021
(This article belongs to the Special Issue The Latest Clinical Advances in Thrombocytopenia)
Abstract
:Cancer patients have varying incidence, depth and duration of thrombocytopenia. The mainstay of managing severe chemotherapy-induced thrombocytopenia (CIT) in cancer is the use of platelet transfusions. While prophylactic platelet transfusions reduce the bleeding rate, multiple unmet needs remain, such as high residual rates of bleeding, and anticancer treatment dose reductions/delays. Accordingly, the following promising results in other settings, antifibrinolytic drugs have been evaluated for prevention and treatment of bleeding in patients with hematological malignancies and solid tumors. In addition, Thrombopoeitin receptor agonists have been studied for two major implications in cancer: treatment of severe thrombocytopenia associated with myelodysplastic syndrome and acute myeloid leukemia; primary and secondary prevention of CIT in solid tumors in order to maintain dose density and intensity of anti-cancer treatment. Furthermore, thrombocytopenic cancer patients are often prescribed antithrombotic medication for indications arising prior or post cancer diagnosis. Balancing the bleeding and thrombotic risks in such patients represents a unique clinical challenge. This review focuses upon non-transfusion-based approaches to managing thrombocytopenia and the associated bleeding risk in cancer, and also addresses the management of antithrombotic therapy in thrombocytopenic cancer patients.
1. Introduction
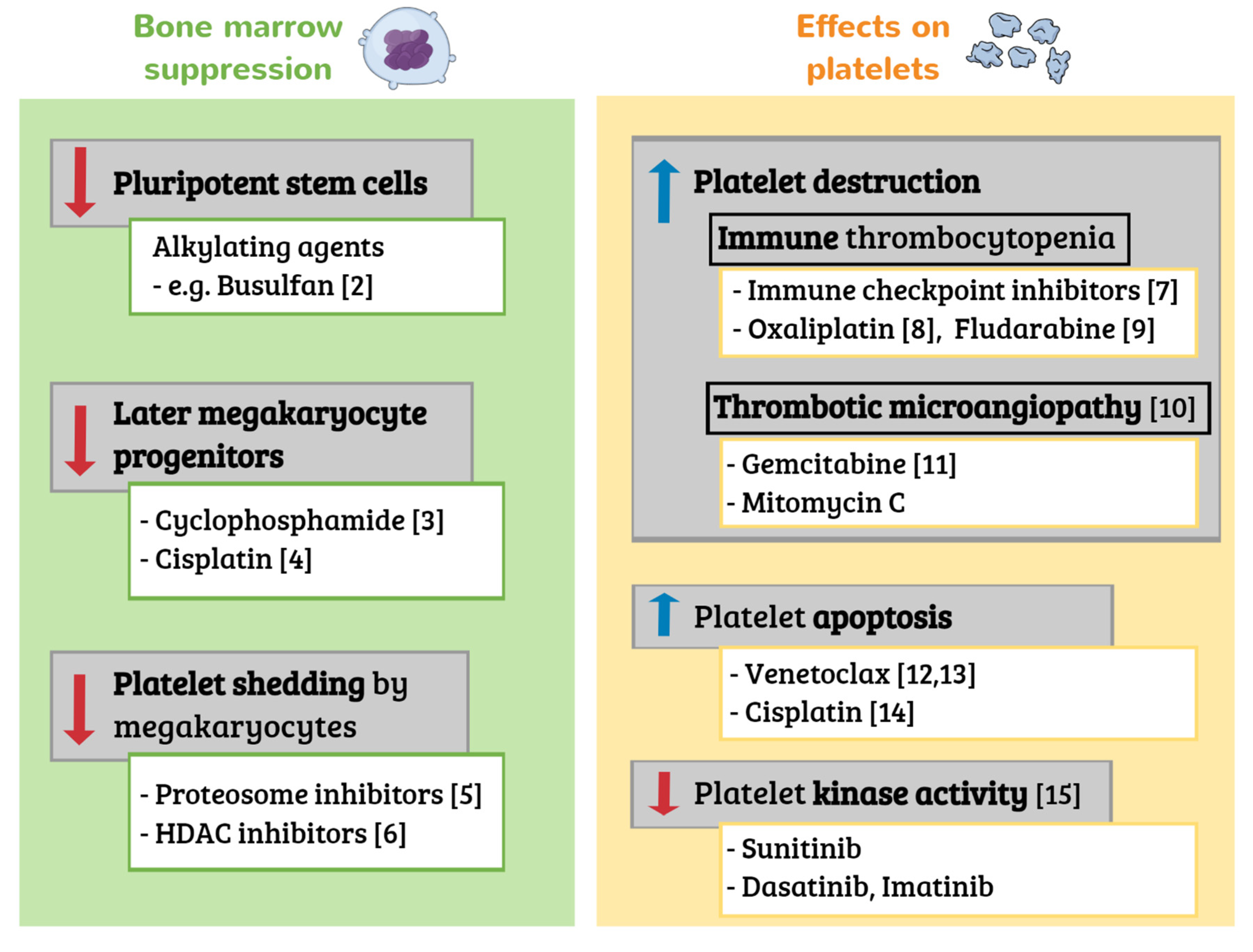
Cancer patients have varying incidence, depth and duration of thrombocytopenia, depending on cancer type, anticancer treatment, bone marrow involvement and comorbidities [1]. For example, patients with hematological malignancies and those receiving carboplatin or oxaliplatin based chemotherapy regimens, have a higher risk of severe thrombocytopenia. Anticancer drugs can cause thrombocytopenia via various mechanisms [2,3,4,5,6,7,8,9,10,11,12,13,14,15], as previously reviewed [1] and as shown in Figure 1. While pancytopenia due to general bone marrow suppression is most common, some antineoplastic drugs, such as proteosome inhibitors used primarily in multiple myeloma, can cause isolated thrombocytopenia. Bortezomib, a first-generation proteasome inhibitor, was found to reduce the mean platelet number by approximately 60%, independent of the baseline platelet count [9]. Proteosome inhibitor associated thrombocytopenia has a cyclic, transient pattern [16,17]. The mechanism was first suggested to be related to the prevention of the activation of NF-κB which may potentially prevent platelet budding from megakaryocytes. Further studies found that the pharmacologic inhibition of proteasome activity blocks proplatelet formation, due to the upregulation and hyperactivation of the small GTPase RhoA, rather than NF-κB [18]. Although thrombocytopenia is commonly observed, there are only a few reports of serious bleeding complications with proteosome inhibitors [17,19].
Severe thrombocytopenia (<10 × 109/L) is associated with an increased risk of bleeding in cancer [20,21]. However, individual platelet counts between 10 and 50 × 109/L do not clearly predict bleeding [22,23,24]. Multiple other factors affect the bleeding risk, such as fever, sex, renal failure, liver dysfunction, hematocrit ≤25% and use of antithrombotic drugs [21,24,25]. These factors should be considered when assessing bleeding risk and addressed when modifiable. In addition, emerging data show that patients with cancer-associated thrombocytopenia have additional hemostatic defects, such as platelet and endothelial dysfunction, as well as coagulation abnormalities, such as hyperfibrinolysis [26,27,28].
The mainstay of managing severe chemotherapy-induced thrombocytopenia (CIT) in cancer is the use of platelet transfusions. In most cancer settings, platelet transfusions are indicated prophylactically when platelets counts are <10 × 109/L or therapeutically when bleeding occurs with platelets below 50 × 109/L [29]. Different platelet transfusion thresholds may be warranted in the context of invasive procedures, sepsis, autologous stem cell transplantation and chronic stable disease-related thrombocytopenia, among other scenarios [21,29]. While prophylactic platelet transfusions reduce the rate of WHO grade ≥2 bleeding [22,23], multiple unmet needs remain in patients with cancer and thrombocytopenia, including the following: high rates of bleeding despite platelet transfusion [22]; thrombocytopenia-driven anticancer treatment dose reductions or delay; platelet-transfusion refractoriness [30]; managing antithrombotic drugs when indicated.
This review focuses upon non-transfusion-based approaches to managing thrombocytopenia and the associated bleeding risk in cancer, and also addresses the management of antithrombotic therapy in thrombocytopenic cancer patients. The topic of platelet transfusions in cancer patients has been previously reviewed [29] and is covered elsewhere in this issue of the Journal.
2. Managing Thrombocytopenia in Cancer
2.1. Antifibrinolytic Therapy
Tranexamic acid (TXA) and aminocaproic acid (EACA) are synthetic antifibrinolytic drugs that lead to the inhibition of the conversion of plasminogen to plasmin and to the decrease in the lysis of fibrin clots [31]. Antifibrinolytic therapy has been shown to aid in the management of bleeding in multiple clinical scenarios such as trauma, postpartum hemorrhage, menorrhagia, and surgical bleeding [32]. On the other hand, recent negative findings of a randomized controlled trial (RCT) of TXA in acute gastrointestinal bleeding and a higher rate venous thromboembolism (VTE) in the TXA arm, serve as a reminder that setting-specific evidence is needed [33]. In light of this, the utility of antifibrinolytic drugs in solid tumors and hematological malignancies has also been evaluated. This review focuses on CIT or cancer-related thrombocytopenia, outside the context of disseminated intravascular coagulation (DIC) [34,35].
2.1.1. Solid Tumors
A number of small RCTs and retrospective cohort studies were performed to assess the effect of perioperative antifibrinolytics on bleeding during and after cancer surgery, in a variety of solid malignancies. The studies including patients with liver, prostate and gynecological cancer found a reduction in blood transfusion requirements during and after surgery in the TXA arms [36,37,38,39,40,41]. In contrast, antifibrinolytics did not influence bleeding outcomes in major orthopedic cancer surgery or in oncologic spinal canal, head and neck and neurosurgeries [42,43,44,45].
Data on the use of antifibrinolytics for the treatment of active bleeding in solid cancer is scarce and limited to case reports and series. Several case reports showed favorable bleeding outcomes with TXA in the management of bleeding from malignant mesothelioma with hemothorax [46], hemoptysis due to bronchogenic carcinoma [47] and DIC after a prostatic biopsy [48]. One small case series (n = 16) demonstrated high rates of bleeding control with TXA and EACA for cancer associated bleeding in the palliative care setting [49].
2.1.2. Hematological Malignancies with Thrombocytopenia
EACA and TXA have been studied over the years in patients with hematological malignancies and thrombocytopenia (generally <50 × 109/L) with or without bleeding. However, most of the studies are small, non-controlled and retrospective with various treatment protocols and doses. Since EACA and TXA have not been compared directly, the evidence on each of these drugs is presented separately, first as treatment and then as prophylaxis.
Treatment of Bleeding
Two studies published in 1980 and 1985 evaluated the use of EACA for the control of bleeding in patients with various hematological malignancies and thrombocytopenia (<20 × 109/L) and reported the improvement in bleeding control and a reduction in platelet transfusions [50,51]. An additional study published in 1998 evaluated 15 patients with bleeding and severe thrombocytopenia (platelets <20 × 109/L) and showed a positive effect with a maximum EACA dose of 6 g/day [52]. In 2006, a retrospective study from the Cleveland clinic reviewed the use of EACA in 77 patients with thrombocytopenic (median platelet count = 7 × 109/L) hemorrhage (mostly mucosal and gastrointestinal). The majority of patients had hematological malignancies, predominantly acute leukemia and non-Hodgkin lymphoma, and the remainder had solid tumors. The median average dose was also 6 g/day. Complete (i.e., cessation of bleeding at all sites) and partial response were achieved in 51 (66%) and 13 (17%) patients, respectively, resulting in a decrease in platelet and red blood cell transfusions [53]. In 2008, a retrospective study evaluating EACA in acute promyelocytic leukemia (APL) patients with coagulopathy defined as low alpha-2-antiplasmin levels suggested a lower incidence of severe hemorrhagic events [54].
A recent Dutch survey indicated that TXA is more commonly used for the control of bleeding in hematological malignancies than as prophylaxis [55], even though most studies of TXA were in the context of prophylaxis. There is currently scarce evidence supporting the use of this specific agent in this context.
Prophylaxis of Bleeding
EACA as prophylactic treatment was evaluated in 1983 in a randomized controlled trial versus placebo in patients undergoing remission induction for acute leukemia. There was no difference in major bleeding between the two groups; however, there was a non-significant reduction in platelet transfusions in the EACA group [56]. A subsequent retrospective study in 2013 reported on EACA treatment in 44 chronically and severely thrombocytopenic patients with hematological malignancies and median platelet counts of 8 × 109/L. EACA was associated with a low risk of major spontaneous bleeding and was well tolerated [57]. Two additional retrospective studies (2016, 2018) provided additional safety data by demonstrating no increase in VTE rates with EACA as prophylactic therapy in thrombocytopenic patients with hematological malignancy [58,59]. The PROBLEMA Trial, a phase II control trial study evaluating the effectiveness and safety of EACA versus prophylactic platelet transfusions to prevent bleeding in thrombocytopenic patients with hematological malignancies, is still ongoing [60]. Table 1 details the ongoing studies of antifibrinolytics in thrombocytopenic cancer patients.
Up until recently, only three small RCTs evaluating TXA in hematological malignancies had been published (1989 thru 1995) including patients with acute leukemia, APL, aplastic anemia and myelodysplastic syndrome (MDS) [61,62,63]. TXA was associated with fewer bleeding episodes and fewer transfusion requirements in two of these studies [61,62]. In the third pilot study evaluating eight patients with MDS and aplastic anemia, TXA did not appear to be efficacious [63]. It should be noted that only three patients completed the randomized portion of this study and that patients were used as their own control. In addition, a prospective single arm study published in 1990 demonstrated a significant reduction in platelet transfusion with prophylactic TXA during induction and consolidation treatment in acute leukemia, compared to historical controls [64]. Of concern is a case series of three allogenic hematopoietic stem cell transplant patients who developed veno-occlusive disease (VOD) shortly after receiving TXA. The authors postulated a role for plasminogen activator inhibitor-1 in the development of hepatic VOD and that TXA could trigger or accelerate this process [65].
Accordingly, a systematic review and meta-analysis of antifibrinolytics for the prevention of bleeding in patients with hematological disorders concluded that there is uncertainty whether antifibrinolytics reduce the risk of bleeding in such patients, due to the small number of participants and low quality of evidence [66]. The question whether or not antifibrinolytics increase the risk of thromboembolic events or other adverse events could not be answered. A subsequent meta-analysis published in 2017 evaluated the safety and efficacy of lysine analogues in a total of 1177 cancer patients (both hematological and solid tumors) [67]. No increased risk of venous thromboembolism was observed among patients receiving lysine analogues compared to controls, and their use significantly decreased blood loss and transfusion risk.
The results of the randomized controlled A-TREAT trial, assessing prophylactic TXA administration in addition to routine platelet transfusion, were recently presented and published in abstract form [68]. The study included 165 patients in each arm and demonstrated that prophylactic TXA did not decrease the rate of WHO grade 2+ bleeding and did not change platelet and blood cell transfusions rates. Of note, the rate of central line occlusions was increased in the TXA arm. This preliminary publication suggests that TXA should not be currently used for preventing bleeding in addition to prophylactic platelet transfusions. The results of the sister TREAT-T trial conducted in the UK and Australia are eagerly anticipated (Table 1) [69]. Knowledge gaps not currently addressed by published or ongoing trials that we are aware of, include the use of antifibrinolytic therapy for breakthrough bleeding and as prophylaxis in patients with platelet transfusion refractoriness.
2.2. Thrombopoeitin Receptor Agonists in Cancer and Thrombocytopenia
Thrombopoetin receptor agonists (TPO-RAs), such as eltrombopag and romiplostim, increase platelet production through interactions with the thrombopoietin receptor on megakaryocytes. Eltrombopag is a small molecule agonist, while romiplostim is a peptibody (i.e., fusion of a novel peptide and antibody) that can stimulate the TPO receptor. The binding of romiplostim to the distal domain of the thrombopoietin receptor or binding of eltrombopag to the transmembrane region of the receptor triggers a number of signal transduction pathways, including activation of the JAK-STAT signaling pathway, which induce proliferation and differentiation of megakaryocytes [70]. Eltrombopag and romipostim were both licensed in the United States for the treatment of immune thrombocytopenia in 2008. Eltrombopag is also licensed for the treatment of aplastic anemia and the treatment of thrombocytopenia in patients with hepatitis C receiving interferon-based therapy [71].
Recombinant IL-11 (oprelvekin) is the only approved treatment in the United States for CIT. However, its use is very limited because of side effects [72]. Clinical development of recombinant human thrombopoietins (rhTPO) and pegylated recombinant megakaryocyte growth and development factor (PEG-rhMGDF) have stopped due to the development of neutralizing antibodies to PEG-rhMGDF [73]. The rhTPO, TPIAO™, is widely used to treat CIT in China and is unavailable elsewhere [74].
TPO-RAs have been studied for two major implications in cancer related thrombocytopenia. In the field of hematological disorders, they were mainly studied for MDS and acute myeloid leukemia (AML), in order to treat severe thrombocytopenia and avoid platelet transfusions, as summarized in Table 2. In the field of solid tumors, they were used to prevent CIT and enable scheduled anti-cancer treatment. Prevention was either primary, before anti-cancer treatment, or secondary, after the development of thrombocytopenia. Selected studies on TPO-RAs in CIT are detailed in Table 3.
2.2.1. Low-Intermediate Risk MDS
Giagouinidis et al. included 250 patients with low to intermediate (low-int) risk MDS to receive romiplostim or placebo (2:1) [75]. This study was terminated early because of an increase in peripheral blasts in the romiplostim group. Despite this initial signal, there was no increased risk of progression to AML in the romiplostim group [75], including in an analysis after five years follow-up [76]. Romiplostim increased platelet counts, and decreased platelet transfusions and overall bleeding, but did not affect clinically significant bleeding rates. Initial similar results were published for eltrombopag in low-int MDS [77]. That study reported improved quality of life in patients who received eltrombopag. The full study has not been published yet. Eltrombopag was also shown to increase white blood cell counts and hemoglobin levels in some patients in a small study of low-int risk MDS patients [78].
2.2.2. High Risk MDS/AML
In a phase 1/2 study of advanced MDS or AML, eltrombopag was well tolerated in 64 patients, and no difference in the percentage of blasts was observed [79]. In a phase 3 trial of intermediate-high risk MDS treated with azacitidine, eltrombopag did not reduce the need for platelet transfusions. In fact, this study was terminated early due to inferiority of the eltrombopag/azacitidine arm (16% vs. 31%) and a trend towards increased progression to AML [80]. Furthermore, in a phase 2 placebo controlled trial of eltrombopag in patients with AML undergoing induction chemotherapy, eltrombopag did not decrease the time to platelet recovery, while more serious adverse events and numerically higher death rates were observed in the eltrombopag group [81].
2.2.3. After Bone Marrow Transplantation
Persistent thrombocytopenia is a common complication after allogeneic hematopoietic cell transplantation. In a phase 1/2 single arm study, romiplostim given to patients after allogeneic stem cell transplantation who had persistent severe thrombocytopenia <20 × 109/L (median of 84 days after transplantation), was effective in most patients. The median time to platelet counts >50 × 109/L was 45 days [82]. Eltrombopag was also reported to achieve good platelet response in approximately 60% of patients in three small retrospective studies [83,84,85].
2.2.4. High Grade Lymphoma
In a phase 1/2 open label in patients with Hodgkin or non-Hodgkin lymphoma, who experienced grade 3–4 thrombocytopenia (<50 × 109/L), romiplostim given one day after chemotherapy did not have a beneficial effect on platelet nadir [86]. In contrast, in patients receiving the RHyper-CVAD/RArac-MTX protocol, romiplostim, given 5 days before and after chemotherapy, significantly (for a total of 2 doses) increased the platelet nadir and decreased the duration of thrombocytopenia [87].
2.2.5. CIT in Solid Tumors
CIT in solid tumors is defined as platelet count below 100 × 109/L with no other reason for thrombocytopenia. CIT may carry a risk of bleeding and may delay anti-cancer treatment and, therefore, it could potentially affect patients’ prognosis. A recent Cochrane review assessed the effects of TPO-RAs to treat and prevent CIT [88]. No certain conclusions could be made due to the weak available data. Selected studies for treatment of CIT are presented in Table 3. These were mostly retrospective studies that reported off-label use of romiplostim for this indication as well as several phase 2 studies. The main type of tumor was of gastrointestinal origin. Romiplostim rapidly increased platelet counts and could enable the scheduled anti-cancer treatments in most patients (Table 3). In the largest retrospective study to date, predictors of non-response to romiplostim included bone marrow tumor invasion, prior pelvic irradiation and exposure to temozolomide [89]. Nonetheless, in an open label phase II study of romiplostim in patients with glioblastoma receiving temozolomide, 60% of patients had good response and only 20% had no response [90]. The rate of thrombotic complications in patients who received romiplostim was reported between 5–15% (Table 3). Most of the events were VTE and only a small number of arterial events were reported. It is unclear whether TPO-RAs increase thrombosis in patients with cancer since no comparison group was included in most of the studies. A phase 3 study of avatrombopag vs. placebo in cancer patients who experienced grade 3–4 thrombocytopenia, was recently terminated due to futility, but is yet to be published. The press release reported that although avatrombopag increased platelet counts relative to placebo as expected, the study did not meet the composite primary endpoint of avoiding platelet transfusions, chemotherapy dose reductions by ≥15%, and chemotherapy dose delays by ≥4 days [91,92].
2.2.6. Summary
TPO-RA studies in cancer are mainly retrospective or phase 2 trials. In these trials, both romiplostim and eltrombopag showed a potential benefit in patients experiencing severe thrombocytopenia related to low risk MDS and post allogeneic transplantation. In patients receiving chemotherapy for solid tumors TPO-RAs may improve platelet counts and the ability to prescribe scheduled anti-cancer treatments. The only two phase 3 trials of eltrombopag in patients with high risk MDS and avatrombopag in solid tumors did not meet the primary outcome. TPO-RAs may carry a risk in patients with advanced MDS in combination with azacitidine and in patients with AML undergoing induction chemotherapy. More phase 3 trials are indicated to investigate the role of TPO-RAs in cancer patients, some of which are planned or underway, as detailed in Table 4.
3. Managing Antithrombotic Therapy in Thrombocytopenic Patients
Cancer is associated with an increased risk of both venous and arterial thrombosis [99,100,101]. Moreover, contemporary anticancer therapy and supportive care allow for the treatment of older patients with comorbid cardiovascular disease. This means that cancer patients, who are also at risk of thrombocytopenia, often have an indication for antithrombotic therapy (i.e., anticoagulation or antiplatelet therapy) before or after cancer diagnosis. Thrombocytopenic cancer patients remain at risk of venous and arterial thrombosis, since thrombocytopenia does not afford protection and is associated with adverse outcomes [102,103,104,105,106,107,108]. Multiple mechanisms, not dependent on the platelet compartment, contribute to cancer associated thrombosis, as recently reviewed [109]. These include tumor-driven increases in procoagulant activity and inhibition of fibrinolytic and natural anticoagulant pathways which lead to increased thrombin generation, as well as effects on leukocytes and endothelial cells. On the other hand, cancer patients are at increased risk of anticoagulation-associated bleeding [110,111], which is complicated by thrombocytopenia and other hemostatic defects [26,27,28]. Therefore, balancing the thrombotic and bleeding risk in thrombocytopenic risk remains a clinical challenge. Unfortunately, prospective data are scarce, meaning that management is currently informed mainly by expert opinion [112] and retrospective studies on VTE and ischemic heart disease [102,106,113,114,115,116], since clinical trials of anticoagulants in cancer-associated VTE exclude patients with thrombocytopenia (<50–100 × 109/L) [117,118,119,120,121].
3.1. Management Concepts
We generally manage antithrombotic medication within the framework of international guidelines for treatment of VTE in thrombocytopenic cancer patients [122]. Importantly, these recommendations do not apply to other indications such as atrial fibrillation or antiplatelet medication, which generally lack specific guidelines. Therefore, we adjust management after considering context-specific evidence (see Section 3.2 and Section 3.3) and the risk-benefit ratio for the individual patient, bearing in mind the low level of evidence driving these recommendations.
3.1.1. Risk Assessment
We always reevaluate the indication for antithrombotic therapy, and assess the associated thrombotic risk. We then estimate the anticipated duration of platelet counts below 50 × 109/L, which may range from days to weeks in case of CIT or months to years for chronic disease-related thrombocytopenia, such as in MDS or graft versus host disease. Of note, the vast majority of evidence pertains to short-term thrombocytopenia. We also identify additional factors associated with higher bleeding risk in this setting, including a history of bleeding, hematological malignancy and increasing bilirubin, creatinine, and prothrombin time [113,114]. An important concept guiding management decisions is that these patients have a high short-term risk of clinically significant bleeding, especially with full anticoagulation [22,24,102,113,123,124,125]. Accordingly, the thrombotic risk should be sufficiently high to justify anticoagulation.
3.1.2. Management Plan
Using the above information, we formulate a clear management plan, to be reassessed frequently, often on a daily basis. We first decide whether to continue or hold the antithrombotic medication. If continued, we consider changes in the dose and/or class of antithrombotic medication, and modifications in platelet transfusion thresholds. When anticoagulation is discontinued, mechanical measures to possibly mitigate thrombotic risk are considered on a case-by-case basis. These include inferior vena cava filter placement for acute lower extremity deep vein thrombosis (DVT) [122] or removal of the central venous catheter in case of catheter-related DVT [126]. Finally, once the platelet count is consistently above the threshold for full antithrombotic medication, we consider restarting full antithrombotic therapy, even between treatment cycles, if the indication remains [123].
3.2. Anticoagulation
Changes in anticoagulation management are generally recommended when platelets are <50 × 109/L [112,122,127], since the bleeding risk appears to increase below this threshold [102,123]. The two main indications for therapeutic anticoagulation in this setting are VTE and atrial fibrillation. The evidence and guidelines relate almost exclusively to low-molecular weight heparin (LMWH). The lack of data on direct oral anticoagulants with platelets <50 × 109/L, and increased bleeding risk even with prophylactic doses indicate that they should currently be avoided in this setting [119,121,122,128]. Retrospective cohort studies of VTE patients show varying bleeding and thrombotic rates, as summarized in a prior review [109].
The first month of anticoagulation for VTE is a high risk period for both recurrent bleeding and thrombosis [110], with higher rates of recurrent VTEs in populations enriched with acute VTE (i.e., within 30 days) [109]. Higher VTE burden (e.g., pulmonary embolism or proximal lower extremity DVT) is also considered to carry a higher thrombotic risk [122]. The CHA2DS2VASC score may be used to assess the thrombotic risk in patients with atrial fibrillation. Lower thrombotic risk scenarios where full-dose anticoagulation may not be justified include non-acute VTE (especially in autologous hematopoietic stem cell transplantation), catheter-related thrombosis and low risk atrial fibrillation [114,125,126,129]. Strategies for mitigating the high bleeding risk associated with continued anticoagulation include increased platelet transfusion threshold (e.g., 40–50 × 109/L) and anticoagulation dose reductions, but evidence proving the safety and efficacy of both approaches is lacking [130].
Current guidelines use VTE acuity, risk of thrombus progression and platelet count to direct decisions regarding anticoagulation in thrombocytopenic cancer patients with VTE [122]. In case of acute VTE, high risk of thrombus progression and platelets <50 × 109/L, increased platelet transfusion thresholds are recommended to enable full-dose anticoagulation. In patients with acute VTE and a lower risk of thrombus progression or those with non-acute VTE, LMWH dose reduction by 50% or prophylactic LMWH doses are recommended when platelets are 25–50 × 109/L. Anticoagulation should generally be discontinued at platelet counts below 25 × 109/L.
A recent study of 774 hypothetical case vignettes managed by 168 physicians suggested that the management process was compatible with these guidelines but that management varied according to physician characteristics and practice setting [131]. Of note, prior major bleeding and the type of hematological disease and treatment influenced management, and may be considered in the decision-making process, although not incorporated in the guidelines. Two recent retrospective analyses suggest that current management may achieve a reasonable balance between bleeding and thrombotic risk in VTE patients [116,129], but this remains to be confirmed prospectively by ongoing observational studies [132].
3.3. Antiplatelet Therapy
We generally discontinue aspirin used for primary prevention of arterial disease in patients with thrombocytopenia. The platelet threshold requiring changes in aspirin management appears lower than 50 × 109/L, but the exact threshold is unknown [106,115]. There are sufficient data to suggest that aspirin use in acute myocardial infarction in thrombocytopenic patients (especially if platelets >30 × 109/L) should be considered [106], but evidence on other indications is lacking.
Formal ischemic heart disease and stroke guidelines do not provide recommendations for management of thrombocytopenic cancer patients. In a consensus statement from the Society for Cardiovascular Angiography and Interventions (SCAI), aspirin was recommended when platelet counts were >10 × 109/L, while dual antiplatelet therapy was reserved for platelets >30 × 109/L [133]. A recent review, not specific to cancer, provided higher platelet thresholds (aspirin >50 × 109/L; dual antiplatelet therapy >100 × 109/L) [134].
A case vignette study assessing the decision-making process among 145 physicians across three countries, outlined the patient and physician factors influencing management. This study indicated that physicians considered ST elevation myocardial infarction to be a high-risk thrombotic scenario that warrants dual antiplatelet therapy despite thrombocytopenia [135]. Furthermore, platelet transfusion was used in 34% of cases continuing antiplatelet therapy to theoretically mitigate the risk of bleeding; however, there is no evidence to support this practice.
4. Summary
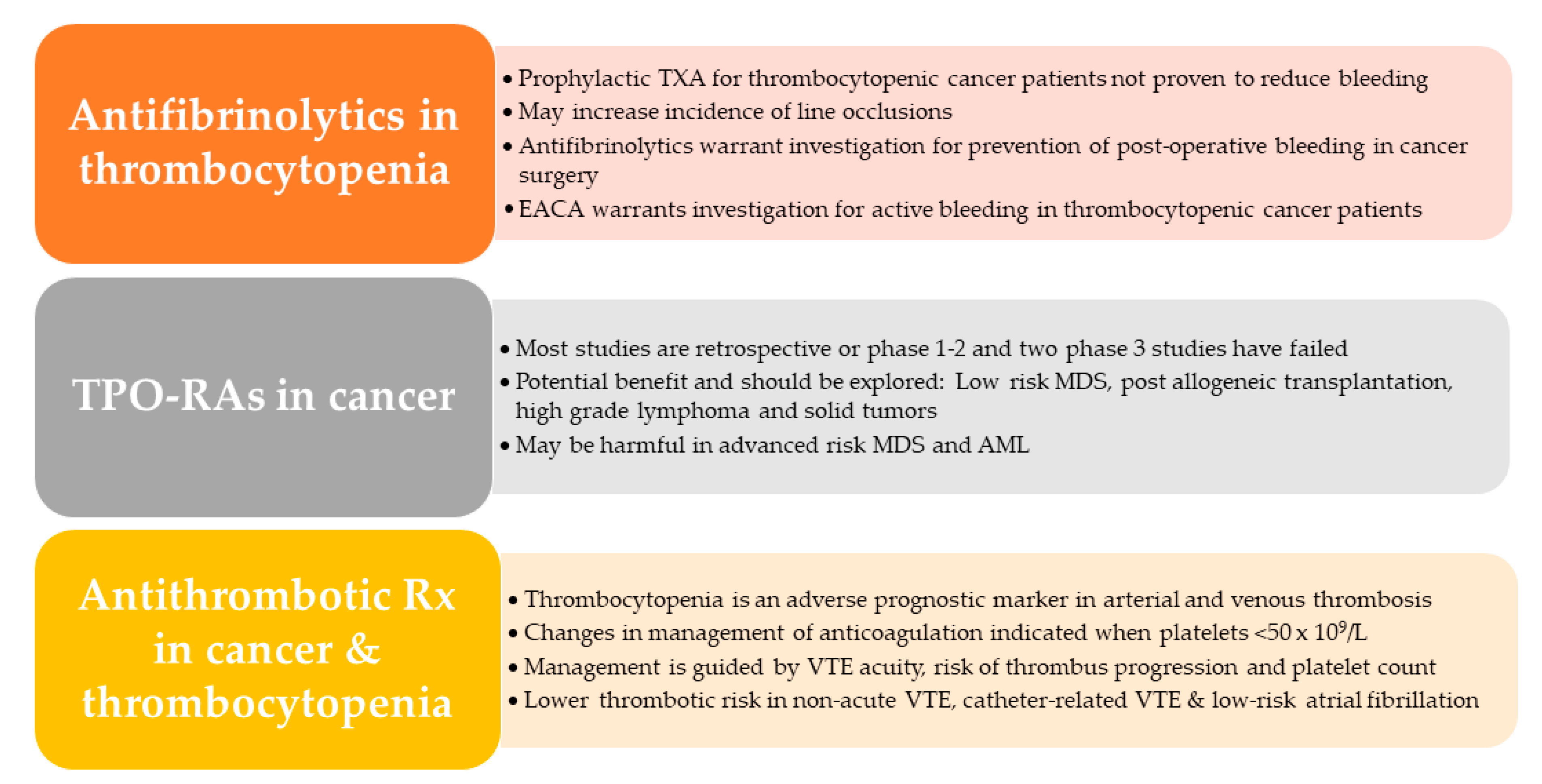
The main take home messages regarding antifibrinolytics, TPO-RAs and antithrombotic medication in thrombocytopenic patients are shown in Figure 2. Platelet transfusion remains the cornerstone of managing thrombocytopenia in cancer, while we eagerly await the results of ongoing studies on antifibrinolytics and TPO-RAs.
Author Contributions
Literature review, writing—original draft preparation, writing—review and editing, A.L., L.H., G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
A.L. declares personal fees for consultancy and scientific advisory boards from Bayer, Novartis, Pfizer, Sanofi, outside the scope of this manuscript; G.S. declares personal fees for consultancy and scientific advisory from Bayer, Boehringer Ingelheim, Medison, Novartis, Pfizer, Sanofi, outside the scope of this manuscript. L.H. declares no conflict of interest.
References
- Liebman, H.A. Thrombocytopenia in cancer patients. Thromb. Res. 2014, 133, 63. [Google Scholar] [CrossRef]
- McManus, P.M.; Weiss, L. Busulfan-induced chronic bone marrow failure: Changes in cortical bone, marrow stromal cells, and adherent cell colonies. Blood 1984, 64, 1036–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dezern, A.E.; Petri, M.; Drachman, D.B.; Kerr, D.; Hammond, E.R.; Kowalski, J.; Tsai, H.L.; Loeb, D.M.; Anhalt, G.; Wigley, F.; et al. High-dose cyclophosphamide without stem cell rescue in 207 patients with aplastic anemia and other autoimmune diseases. Medicine 2011, 90, 89–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Nimmer, P.M.; Tahir, S.K.; Chen, J.; Fryer, R.M.; Hahn, K.R.; Iciek, L.A.; Morgan, S.J.; Nasarre, M.C.; Nelson, R.; et al. Bcl-2 family proteins are essential for platelet survival. Cell Death Differ. 2007, 14, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Suvarna, V.; Singh, V.; Murahari, M. Current overview on the clinical update of Bcl-2 anti-apoptotic inhibitors for cancer therapy. Eur. J. Pharmacol. 2019, 862, 172655. [Google Scholar] [CrossRef]
- Zhang, W.; Zhao, L.; Liu, J.; Du, J.; Wang, Z.; Ruan, C.; Dai, K. Cisplatin induces platelet apoptosis through the ERK signaling pathway. Thromb. Res. 2012, 130, 81–91. [Google Scholar] [CrossRef]
- Tullemans, B.M.E.; Heemskerk, J.W.M.; Kuijpers, M.J.E. Acquired platelet antagonism: Off-target antiplatelet effects of malignancy treatment with tyrosine kinase inhibitors. J. Thromb. Haemost. 2018, 16, 1686–1699. [Google Scholar] [CrossRef] [Green Version]
- Zeuner, A.; Signore, M.; Martinetti, D.; Bartucci, M.; Peschle, C.; De Maria, R. Chemotherapy-induced thrombocytopenia derives from the selective death of megakaryocyte progenitors and can be rescued by stem cell factor. Cancer Res. 2007, 67, 4767–4773. [Google Scholar] [CrossRef] [Green Version]
- Lonial, S.; Waller, E.K.; Richardson, P.G.; Jagannath, S.; Orlowski, R.Z.; Giver, C.R.; Jaye, D.L.; Francis, D.; Giusti, S.; Torre, C.; et al. Risk factors and kinetics of thrombocytopenia associated with bortezomib for relapsed, refractory multiple myeloma. Blood 2005, 106, 3777–3784. [Google Scholar] [CrossRef]
- Bishton, M.J.; Harrison, S.J.; Martin, B.P.; McLaughlin, N.; James, C.; Josefsson, E.C.; Henley, K.J.; Kile, B.T.; Prince, H.M.; Johnstone, R.W. Deciphering the molecular and biologic processes that mediate histone deacetylase inhibitor—Induced thrombocytopenia. Blood 2011, 117, 3658–3668. [Google Scholar] [CrossRef]
- Michot, J.M.; Lazarovici, J.; Tieu, A.; Champiat, S.; Voisin, A.L.; Ebbo, M.; Godeau, B.; Michel, M.; Ribrag, V.; Lambotte, O. Haematological immune-related adverse events with immune checkpoint inhibitors, how to manage? Eur. J. Cancer 2019, 122, 72–90. [Google Scholar] [CrossRef] [PubMed]
- Curtis, B.R.; Kaliszewski, J.; Marques, M.B.; Saif, M.W.; Nabelle, L.; Blank, J.; McFarland, J.G.; Aster, R.H. Immune-mediated thrombocytopenia resulting from sensitivity to oxaliplatin. Am. J. Hematol. 2006, 81, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Leach, M.; Parsons, R.M.; Reilly, J.T.; Winfield, D.A. Autoimmune thrombocytopenia: A complication of fludarabine therapy in lymphoproliferative disorders. Clin. Lab. Haematol. 2000, 22, 175–178. [Google Scholar] [CrossRef]
- Thomas, M.; Scully, M. How I Treat Microangiopathic Hemolytic Anemia in Patients with Cancer. Blood 2021. [Google Scholar] [CrossRef]
- Zupancic, M.; Shah, P.C.; Shah-Khan, F.; Nagendra, S. Gemcitabine-associated thrombotic thrombocytopenic purpura. Lancet Oncol. 2007, 8, 634–641. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Goldschmidt, H.; Niesvizky, R.; Joshua, D.; Chng, W.J.; Oriol, A.; Orlowski, R.Z.; Ludwig, H.; Facon, T.; Hajek, R.; et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): An interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 1327–1337. [Google Scholar] [CrossRef]
- Gandolfi, S.; Laubach, J.P.; Hideshima, T.; Chauhan, D.; Anderson, K.C.; Richardson, P.G. The proteasome and proteasome inhibitors in multiple myeloma. Cancer Metastasis Rev. 2017, 36, 561–584. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.S.; Smith, M.C.P.; Campbell, R.A.; Zimmerman, P.W.; Franks, Z.B.; Kraemer, B.F.; Machlus, K.R.; Ling, J.; Kamba, P.; Schwertz, H.; et al. Proteasome function is required for platelet production. J. Clin. Invest. 2014, 124, 3757–3766. [Google Scholar] [CrossRef] [PubMed]
- Cengiz Seval, G.; Beksac, M. The safety of bortezomib for the treatment of multiple myeloma. Expert Opin. Drug Saf. 2018, 17, 953–962. [Google Scholar] [CrossRef]
- Slichter, S.J.; Kaufman, R.M.; Assmann, S.F.; McCullough, J.; Triulzi, D.J.; Strauss, R.G.; Gernsheimer, T.B.; Ness, P.M.; Brecher, M.E.; Josephson, C.D.; et al. Dose of prophylactic platelet transfusions and prevention of hemorrhage. N. Engl. J. Med. 2010, 362, 600–613. [Google Scholar] [CrossRef] [Green Version]
- Stanworth, S.J.; Hudson, C.L.; Estcourt, L.J.; Johnson, R.J.; Wood, E.M. Risk of bleeding and use of platelet transfusions in patients with hematologic malignancies: Recurrent event analysis. Haematologica 2015, 100, 740–747. [Google Scholar] [CrossRef] [Green Version]
- Stanworth, S.J.; Estcourt, L.J.; Powter, G.; Kahan, B.C.; Dyer, C.; Choo, L.; Bakrania, L.; Llewelyn, C.; Littlewood, T.; Soutar, R.; et al. A No-Prophylaxis Platelet-Transfusion Strategy for Hematologic Cancers. N. Engl. J. Med. 2013, 368, 1771–1780. [Google Scholar] [CrossRef] [Green Version]
- Wandt, H.; Schaefer-Eckart, K.; Wendelin, K.; Pilz, B.; Wilhelm, M.; Thalheimer, M.; Mahlknecht, U.; Ho, A.; Schaich, M.; Kramer, M.; et al. Therapeutic platelet transfusion versus routine prophylactic transfusion in patients with haematological malignancies: An open-label, multicentre, randomised study. Lancet 2012, 380, 1309–1316. [Google Scholar] [CrossRef]
- Uhl, L.; Assmann, S.F.; Hamza, T.H.; Harrison, R.W.; Gernsheimer, T.; Slichter, S.J. Laboratory predictors of bleeding and the effect of platelet and RBC transfusions on bleeding outcomes in the PLADO trial. Blood 2017, 130, 1247–1258. [Google Scholar] [CrossRef] [Green Version]
- Webert, K.; Cook, R.J.; Sigouin, C.S.; Rebulla, P.; Heddle, N.M. The risk of bleeding in thrombocytopenic patients with acute myeloid leukemia. Haematologica 2006, 91, 1530–1537. [Google Scholar]
- Estcourt, L.J.; Stanworth, S.J.; Harrison, P.; Powter, G.; McClure, M.; Murphy, M.F.; Mumford, A.D. Prospective observational cohort study of the association between thromboelastometry, coagulation and platelet parameters and bleeding in patients with haematological malignancies-The ATHENA study. Br. J. Haematol. 2014, 166, 581–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heubel-Moenen, F.C.J.I.; Henskens, Y.M.C.; Verhezen, P.W.M.; Wetzels, R.J.H.; Schouten, H.C.; Beckers, E.A.M. Fibrinolysis in patients with chemotherapy-induced thrombocytopenia and the effect of platelet transfusion. J. Thromb. Haemost. 2019, 17, 1073–1084. [Google Scholar] [CrossRef] [PubMed]
- Ypma, P.F.; van Geloven, N.; Kerkhoffs, J.L.H.; te Boekhorst, P.; Zwaginga, J.J.; Beckers, E.A.M.; Brand, A.; van der Meer, P.F.; Eikenboom, J.C.J. The association between haemorrhage and markers of endothelial insufficiency and inflammation in patients with hypoproliferative thrombocytopenia: A cohort study. Br. J. Haematol. 2020, 189, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, C.A.; Bohlke, K.; Delaney, M.; Hume, H.; Magdalinski, A.J.; McCullough, J.J.; Omel, J.L.; Rainey, J.M.; Rebulla, P.; Rowley, S.D.; et al. Platelet Transfusion for Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Juskewitch, J.E.; Norgan, A.P.; De Goey, S.R.; Duellman, P.M.; Wakefield, L.L.; Gandhi, M.J.; Stubbs, J.R.; Kreuter, J.D. How do I … manage the platelet transfusion–refractory patient? Transfusion 2017, 57, 2828–2835. [Google Scholar] [CrossRef]
- Pereira, J.; Phan, T. Management of bleeding in patients with advanced cancer. Oncologist 2004, 9, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.; Ribkoff, J.; Olson, S.; Raghunathan, V.; Al-Samkari, H.; DeLoughery, T.G.; Shatzel, J.J. The many roles of tranexamic acid: An overview of the clinical indications for TXA in medical and surgical patients. Eur. J. Haematol. 2020, 104, 79–87. [Google Scholar] [CrossRef]
- Roberts, I.; Shakur-Still, H.; Afolabi, A.; Akere, A.; Arribas, M.; Brenner, A.; Chaudhri, R.; Gilmore, I.; Halligan, K.; Hussain, I.; et al. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): An international randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 1927–1936. [Google Scholar] [CrossRef]
- Squizzato, A.; Hunt, B.J.; Kinasewitz, G.T.; Wada, H.; ten Cate, H.; Thachil, J.; Levi, M.; Vicente, V.; D’Angelo, A.; Di Nisio, M. Supportive management strategies for disseminated intravascular coagulation: An international consensus. Thromb. Haemost. 2016, 115, 896–904. [Google Scholar] [CrossRef]
- Levi, M.; Scully, M. How I treat disseminated intravascular coagulation. Blood 2018, 131, 845–854. [Google Scholar] [CrossRef]
- Celebi, N.; Celebioglu, B.; Selcuk, M.; Canbay, O.; Karagoz, A.H.; Aypar, U. The role of antifibrinolytic agents in gynecologic cancer surgery. Saudi Med. J. 2006, 27, 637–641. [Google Scholar] [CrossRef]
- Zhang, H.Z.; Dong, L.; Wang, H.M.; Hu, F.; Shao, Q.; Chen, X.; Chen, L. Safety and efficacy of tranexamic acid in spinal canal tumors: A retrospective cohort study. Br. J. Neurosurg. 2020, 34, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Chattopadhyay, S.; Mandal, D.; Chhaule, S.; Mitra, T.; Mukherjee, A.; Mandal, S.K.; Chattopadhyay, S. Does the preoperative administration of tranexamic acid reduce perioperative blood loss and transfusion requirements after head neck cancer surgery? A randomized, controlled trial. Anesth. Essays Res. 2015, 9, 384–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-C.; Ho, W.-M.; Cheng, S.-B.; Yeh, D.-C.; Wen, M.-C.; Liu, T.-J.; P’eng, F.-K. Perioperative parenteral tranexamic acid in liver tumor resection: A prospective randomized trial toward a “blood transfusion”-free hepatectomy. Ann. Surg. 2006, 243, 173–180. [Google Scholar] [CrossRef]
- Crescenti, A.; Borghi, G.; Bignami, E.; Bertarelli, G.; Landoni, G.; Casiraghi, G.M.; Briganti, A.; Montorsi, F.; Rigatti, P.; Zangrillo, A. Intraoperative use of tranexamic acid to reduce transfusion rate in patients undergoing radical retropubic prostatectomy: Double blind, randomised, placebo controlled trial. BMJ 2011, 343, d5701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundin, E.S.; Johansson, T.; Zachrisson, H.; Leandersson, U.; Bäckman, F.; Falknäs, L.; Kjølhede, P. Single-dose tranexamic acid in advanced ovarian cancer surgery reduces blood loss and transfusions: Double-blind placebo-controlled randomized multicenter study. Acta Obstet. Gynecol. Scand. 2014, 93, 335–344. [Google Scholar] [CrossRef]
- Amar, D.; Grant, F.M.; Zhang, H.; Boland, P.J.; Leung, D.H.; Healey, J.A. Antifibrinolytic therapy and perioperative blood loss in cancer patients undergoing major orthopedic surgery. Anesthesiology 2003, 98, 337–342. [Google Scholar] [CrossRef]
- Damade, C.; Tesson, G.; Gilard, V.; Vigny, S.; Foulongne, E.; Gauthé, R.; Ould-Slimane, M. Blood loss and perioperative transfusions related to surgery for spinal tumors. Relevance of tranexamic acid. Neurochirurgie. 2019, 65, 377–381. [Google Scholar] [CrossRef]
- Vel, R.; Udupi, B.P.; Satya Prakash, M.V.S.; Adinarayanan, S.; Mishra, S.; Babu, L. Effect of low dose tranexamic acid on intra-operative blood loss in neurosurgical patients. Saudi J. Anaesth. 2015, 9, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A.P.; Chaukar, D.A.; Patil, V.P.; Metgudmath, R.B.; Hawaldar, R.W.; Divatia, J.V. Does tranexamic acid reduce blood loss during head and neck cancer surgery? Indian J. Anaesth. 2016, 60, 19–24. [Google Scholar] [CrossRef] [PubMed]
- De Boer, W.A.; Koolen, M.G.; Roos, C.M.; Ten Cate, J.W. Tranexamic acid treatment of hemothorax in two patients with malignant mesothelioma. Chest 1991, 100, 847–848. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, B.; Wise, A. Antifibrinolytic therapy for haemoptysis related to bronchial carcinoma. Postgrad. Med. J. 1993, 69, 80. [Google Scholar] [CrossRef] [Green Version]
- Prokopchuk-Gauk, O.; Brose, K. Tranexamic Acid to Treat Life-threatening Hemorrhage in Prostate Cancer Associated Disseminated Intravascular Coagulation with Excessive Fibrinolysis. Cureus 2015, 7, e428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, A.; Tuffin, P. Fibrinolytic inhibitors for cancer-associated bleeding problems. J. Pain Symptom Manag. 1997, 13, 20–24. [Google Scholar] [CrossRef]
- Gardner, F.H.; Helmer III, R.E. Aminocaproic Acid: Use in Control of Hemorrhage in Patients With Amegakaryocytic Thrombocytopenia. JAMA 1980, 243, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Garewal, H.S.; Durie, B.G. Anti-fibrinolytic therapy with aminocaproic acid for the control of bleeding in thrombocytopenic patients. Scand. J. Haematol. 1985, 35, 497–500. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Varma, S.; Singh, S.; Kumari, S. Low dose bolus aminocaproic acid: An alternative to platelet transfusion in thrombocytopenia? Eur. J. Haematol. 1998, 60, 313–314. [Google Scholar] [CrossRef]
- Kalmadi, S.; Tiu, R.; Lowe, C.; Jin, T.; Kalaycio, M. Epsilon aminocaproic acid reduces transfusion requirements in patients with thrombocytopenic hemorrhage. Cancer 2006, 107, 136–140. [Google Scholar] [CrossRef]
- Wassenaar, T.; Black, J.; Kahl, B.; Schwartz, B.; Longo, W.; Mosher, D.; Williams, E. Acute promyelocytic leukaemia and acquired alpha-2-plasmin inhibitor deficiency: A retrospective look at the use of epsilon-aminocaproic acid (Amicar) in 30 patients. Hematol. Oncol. 2008, 26, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, L.L.; Caram-Deelder, C.; Meier, R.T.; Zwaginga, J.J.; Evers, D. Platelet transfusion and tranexamic acid to prevent bleeding in outpatients with a hematological disease: A Dutch nationwide survey. Eur. J. Haematol. 2020. [Google Scholar] [CrossRef]
- Gallardo, R.L.; Gardner, F.H. Antifibrinolytic therapy for bleeding control during remission induction for acute leukemia. Blood 1983, 62, 202a. [Google Scholar]
- Antun, A.G.; Gleason, S.; Arellano, M.; Langston, A.A.; McLemore, M.L.; Gaddh, M.; el Rassi, F.; Bernal-Mizrachi, L.; Galipeau, J.; Heffner, L.T.J.; et al. Epsilon aminocaproic acid prevents bleeding in severely thrombocytopenic patients with hematological malignancies. Cancer 2013, 119, 3784–3787. [Google Scholar] [CrossRef]
- Marshall, A.; Li, A.; Drucker, A.; Dzik, W. Aminocaproic acid use in hospitalized patients with hematological malignancy: A case series. Hematol. Oncol. 2016, 34, 147–153. [Google Scholar] [CrossRef]
- Juhl, R.C.; Roddy, J.V.F.; Wang, T.-F.; Li, J.; Elefritz, J.L. Thromboembolic complications following aminocaproic acid use in patients with hematologic malignancies. Leuk. Lymphoma 2018, 59, 2377–2382. [Google Scholar] [CrossRef] [PubMed]
- NCT02074436 Prevention of Bleeding in hEmatological Malignancies With Antifibrinolytic (Epsilon Aminocaproic Acid). Available online: https://clinicaltrials.gov/ct2/show/NCT02074436 (accessed on 24 January 2021).
- Shpilberg, O.; Blumenthal, R.; Sofer, O.; Katz, Y.; Chetrit, A.; Ramot, B.; Eldor, A.; Ben-Bassat, I. A controlled trial of tranexamic acid therapy for the reduction of bleeding during treatment of acute myeloid leukemia. Leuk. Lymphoma 1995, 19, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Avvisati, G.; ten Cate, J.W.; Büller, H.R.; Mandelli, F. Tranexamic acid for control of haemorrhage in acute promyelocytic leukaemia. Lancet 1989, 2, 122–124. [Google Scholar] [CrossRef]
- Fricke, W.; Alling, D.; Kimball, J.; Griffith, P.; Klein, H. Lack of efficacy of tranexamic acid in thrombocytopenic bleeding. Transfusion 1991, 31, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Ben-Bassat, I.; Douer, D.; Ramot, B. Tranexamic acid therapy in acute myeloid leukemia: Possible reduction of platelet transfusions. Eur. J. Haematol. 1990, 45, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Aisa, Y.; Shimizu, T.; Yamazaki, R.; Mihara, A.; Yajima, T.; Hibi, T.; Ikeda, Y.; Okamoto, S. Hepatic veno-occlusive disease after tranexamic acid administration in patients undergoing allogeneic hematopoietic stem cell transplantation. Am. J. Hematol. 2007, 82, 838–839. [Google Scholar] [CrossRef] [PubMed]
- Estcourt, L.J.; Desborough, M.; Brunskill, S.J.; Doree, C.; Hopewell, S.; Murphy, M.F.; Stanworth, S.J. Antifibrinolytics (lysine analogues) for the prevention of bleeding in people with haematological disorders. Cochrane Database Syst. Rev. 2016, 3, CD009733. [Google Scholar] [CrossRef] [Green Version]
- Montroy, J.; Fergusson, N.A.; Hutton, B.; Lavallée, L.T.; Morash, C.; Cagiannos, I.; Cnossen, S.; Fergusson, D.A.; Breau, R.H. The Safety and Efficacy of Lysine Analogues in Cancer Patients: A Systematic Review and Meta-Analysis. Transfus. Med. Rev. 2017, 31, 141–148. [Google Scholar] [CrossRef]
- Gernsheimer, T.B.; Brown, S.P.; Triulzi, D.J.; Key, N.S.; El Kassar, N.; Herren, H.; May, S. Effects of Tranexamic Acid Prophylaxis on Bleeding Outcomes in Hematologic Malignancy: The a-TREAT Trial. Blood 2020, 136, 1–2. [Google Scholar] [CrossRef]
- Estcourt, L.J.; McQuilten, Z.; Powter, G.; Dyer, C.; Curnow, E.; Wood, E.M.; Stanworth, S.J. The TREATT Trial (TRial to EvaluAte Tranexamic acid therapy in Thrombocytopenia): Safety and efficacy of tranexamic acid in patients with haematological malignancies with severe thrombocytopenia: Study protocol for a double-blind randomised controlled tr. Trials 2019, 20, 592. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Porras, J.R.; Bastida, J.M. Eltrombopag in immune thrombocytopenia: Efficacy review and update on drug safety. Ther. Adv. Drug Saf. 2018, 9, 263–285. [Google Scholar] [CrossRef]
- Ghanima, W.; Cooper, N.; Rodeghiero, F.; Godeau, B.; Bussel, J.B. Thrombopoietin receptor agonists: Ten years later. Haematologica 2019, 104, 1112–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirley Neumann, T.A.; Foote, M. Megakaryocyte growth and development factor (MGDF): An Mpl ligand and cytokine that regulates thrombopoiesis. Cytokines Cell. Mol. Ther. 2000, 6, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Vadhan-Raj, S. Management of Chemotherapy-Induced Thrombocytopenia: Current Status of Thrombopoietic Agents. Semin. Hematol. 2009, 46. [Google Scholar] [CrossRef] [PubMed]
- Consensus on clinical diagnosis, treatment and prevention management of chemotherapy induced thrombocytopenia in China. Zhonghua Zhong Liu Za Zhi 2018, 40, 714–720. [CrossRef]
- Giagounidis, A.; Mufti, G.J.; Fenaux, P.; Sekeres, M.A.; Szer, J.; Platzbecker, U.; Kuendgen, A.; Gaidano, G.; Wiktor-Jedrzejczak, W.; Hu, K.; et al. Results of a randomized, double-blind study of romiplostim versus placebo in patients with low/intermediate-1-risk myelodysplastic syndrome and thrombocytopenia. Cancer 2014, 120, 1838–1846. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.M.; Fenaux, P.; Sekeres, M.A.; Szer, J.; Platzbecker, U.; Kuendgen, A.; Gaidano, G.; Wiktor-Jedrzejczak, W.; Carpenter, N.; Mehta, B.; et al. Long-term follow-up for up to 5 years on the risk of leukaemic progression in thrombocytopenic patients with lower-risk myelodysplastic syndromes treated with romiplostim or placebo in a randomised double-blind trial. Lancet Haematol. 2018, 5, e117–e126. [Google Scholar] [CrossRef]
- Oliva, E.N.; Alati, C.; Santini, V.; Poloni, A.; Molteni, A.; Niscola, P.; Salvi, F.; Sanpaolo, G.; Balleari, E.; Germing, U.; et al. Eltrombopag versus placebo for low-risk myelodysplastic syndromes with thrombocytopenia (EQoL-MDS): Phase 1 results of a single-blind, randomised, controlled, phase 2 superiority trial. Lancet Haematol. 2017, 4, e127–e136. [Google Scholar] [CrossRef]
- Vicente, A.; Patel, B.A.; Gutierrez-Rodrigues, F.; Groarke, E.M.; Giudice, V.; Lotter, J.; Feng, X.; Kajigaya, S.; Weinstein, B.; Barranta, E.; et al. Eltrombopag monotherapy can improve hematopoiesis in patients with low to intermediate risk-1 myelodysplastic syndrome. Haematologica 2020, 105, 2785–2794. [Google Scholar] [CrossRef]
- Platzbecker, U.; Wong, R.S.M.; Verma, A.; Abboud, C.; Araujo, S.; Chiou, T.J.; Feigert, J.; Yeh, S.P.; Götze, K.; Gorin, N.C.; et al. Safety and tolerability of eltrombopag versus placebo for treatment of thrombocytopenia in patients with advanced myelodysplastic syndromes or acute myeloid leukaemia: A multicentre, randomised, placebo-controlled, double-blind, phase 1/2 trial. Lancet Haematol. 2015, 2, e417–e426. [Google Scholar] [CrossRef]
- Dickinson, M.; Cherif, H.; Fenaux, P.; Mittelman, M.; Verma, A.; Portella, M.S.O.; Burgess, P.; Ramos, P.M.; Choi, J.; Platzbecker, U. Azacitidine with or without eltrombopag for first-line treatment of intermediate- or high-risk MDS with thrombocytopenia. Blood 2018, 132, 2629–2638. [Google Scholar] [CrossRef]
- Frey, N.; Jang, J.H.; Szer, J.; Illés, Á.; Kim, H.J.; Ram, R.; Chong, B.H.; Rowe, J.M.; Borisenkova, E.; Liesveld, J.; et al. Eltrombopag treatment during induction chemotherapy for acute myeloid leukaemia: A randomised, double-blind, phase 2 study. Lancet Haematol. 2019, 6, e122–e131. [Google Scholar] [CrossRef]
- De Latour, R.P.; Chevret, S.; Ruggeri, A.L.; Suarez, F.; Souchet, L.; Michonneau, D.; De Fontbrune, F.S.; Coman, T.; Dhedin, N.; Rubio, M.T.; et al. Romiplostim in patients undergoing hematopoietic stem cell transplantation: Results of a phase 1/2 multicenter trial. Blood 2020, 135, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Inamoto, Y.; Yamashita, T.; Fuji, S.; Okinaka, K.; Kurosawa, S.; Kim, S.W.; Tanosaki, R.; Fukuda, T. Eltrombopag for Treatment of Thrombocytopenia after Allogeneic Hematopoietic Cell Transplantation. Biol. Blood Marrow Transplant. 2016, 22, 919–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halahleh, K.; Gale, R.P.; Da’na, W.; Ma’koseh, M.; Saadeh, S.; Alan, W.; Yousef, D.; AL-Far, R.; Muradi, I.; Abujazar, H.; et al. Therapy of posttransplant poor graft function with eltrombopag. Bone Marrow Transplant. 2021, 56, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Marotta, S.; Marano, L.; Ricci, P.; Cacace, F.; Frieri, C.; Simeone, L.; Trastulli, F.; Vitiello, S.; Cardano, F.; Pane, F.; et al. Eltrombopag for post-transplant cytopenias due to poor graft function. Bone Marrow Transplant. 2019, 54, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Fanale, M.; Stiff, P.; Noonan, K.; McCoy, J.; Rutstein, M.; Moskowitz, C. 9209 Safety of romiplostim for treatment of severe chemotherapy induced thrombocytopenia (CIT) in patients with lymphoma receiving multi-cycle chemotherapy: Results from an open-label dose- and schedule-finding study. Eur. J. Cancer Suppl. 2009, 7, 563. [Google Scholar] [CrossRef]
- Vadhan-Raj, S.; Hagemeister, F.; Fayad, L.E.; Zhou, X.; ORoark, S.S.; Ames, K.; Rodriguez, M.A.; Fanale, M.A.; Pro, B.; Johnson, M.M.; et al. Randomized, Double-Blind, Placebo-Controlled, Dose and Schedule-Finding Study of AMG 531 In Chemotherapy-Induced Thrombocytopenia (CIT): Results of a Phase I/II Study. Blood 2010, 116, 1544. [Google Scholar] [CrossRef]
- Zhang, X.; Chuai, Y.; Nie, W.; Wang, A.; Dai, G. Thrombopoietin receptor agonists for prevention and treatment of chemotherapy-induced thrombocytopenia in patients with solid tumours. Cochrane Database Syst. Rev. 2017, 2017. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Parnes, A.D.; Goodarzi, K.; Weitzman, J.I.; Connors, J.M.; Kuter, D.J. A multicenter study of romiplostim for chemotherapy-induced thrombocytopenia in solid tumors and hematologic malignancies. Haematologica 2020. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Devos, P.; Houillier, C.; Cartalat, S.; Chinot, O.; Di Stefano, A.L.; Lepage, C.; Reyns, N.; Dubois, F.; Weller, M. Romiplostim for temozolomide-induced thrombocytopenia in glioblastoma: The PLATUM trial. Neurology 2019, 93, e1799–e1806. [Google Scholar] [CrossRef]
- Sobi Announces Topline Phase 3 Data of Avatrombopag for the Treatment of Chemotherapy-Induced Thrombocytopenia | Sobi. Available online: https://www.sobi.com/en/press-releases/sobi-announces-topline-phase-3-data-avatrombopag-treatment-chemotherapy-induced (accessed on 29 January 2021).
- Avatrombopag for the Treatment of Chemotherapy-Induced Thrombocytopenia in Adults With Active Non-Hematological Cancers—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03471078 (accessed on 30 January 2021).
- Al-Samkari, H.; Marshall, A.L.; Goodarzi, K.; Kuter, D.J. The use of romiplostim in treating chemotherapy-induced thrombocytopenia in patients with solid tumors. Haematologica 2018, 103, e169–e172. [Google Scholar] [CrossRef] [Green Version]
- Parameswaran, R.; Lunning, M.; Mantha, S.; Devlin, S.; Hamilton, A.; Schwartz, G.; Soff, G. Romiplostim for management of chemotherapy-induced thrombocytopenia. Support. Care Cancer 2014, 22, 1217–1222. [Google Scholar] [CrossRef]
- Miao, J.; Leblebjian, H.; Scullion, B.; Parnes, A. A single center experience with romiplostim for the management of chemotherapy-induced thrombocytopenia. Am. J. Hematol. 2018, 93, E86–E88. [Google Scholar] [CrossRef] [Green Version]
- Soff, G.A.; Miao, Y.; Bendheim, G.; Batista, J.; Mones, J.V.; Parameswaran, R.; Wilkins, C.R.; Devlin, S.M.; Abou-Alfa, G.K.; Cercek, A.; et al. Romiplostim treatment of chemotherapy-induced thrombocytopenia. J. Clin. Oncol. 2019, 37, 2892–2898. [Google Scholar] [CrossRef] [PubMed]
- Natale, R.; Charu, V.; Schütte, W.; Albert, I.; Tehenes, S.; McCoy, J.; Berger, D. 9248 Safety of romiplostim for treatment of chemotherapy-induced thrombocytopenia (CIT) in patients with advanced non-small cell lung cancer (NSCLC). Eur. J. Cancer Suppl. 2009, 7, 574. [Google Scholar] [CrossRef]
- Winer, E.S.; Safran, H.; Karaszewska, B.; Bauer, S.; Khan, D.; Doerfel, S.; Burgess, P.; Kalambakas, S.; Mostafa Kamel, Y.; Forget, F. Eltrombopag for thrombocytopenia in patients with advanced solid tumors receiving gemcitabine-based chemotherapy: A randomized, placebo-controlled phase 2 study. Int. J. Hematol. 2017, 106, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, E.; Khorana, A.A. Cancer and Venous Thromboembolic Disease: A Review. Oncologist 2017, 22, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Okin, P.M.; Elkind, M.S.V.; Panageas, K.S.; DeAngelis, L.M. Risk of Arterial Thromboembolism in Patients With Cancer. J. Am. Coll. Cardiol. 2017, 70, 926–938. [Google Scholar] [CrossRef]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Okin, P.M.; Tagawa, S.T.; Panageas, K.S.; DeAngelis, L.M. Arterial thromboembolic events preceding the diagnosis of cancer in older persons. Blood 2018, 133, 781–789. [Google Scholar] [CrossRef]
- Khanal, N.; Bociek, R.G.; Chen, B.; Vose, J.M.; Armitage, J.O.; Bierman, P.J.; Maness, L.J.; Lunning, M.A.; Gundabolu, K.; Bhatt, V.R. Venous thromboembolism in patients with hematologic malignancy and thrombocytopenia. Am. J. Hematol. 2016, 91, E468–E472. [Google Scholar] [CrossRef]
- Labrador, J.; Lopez-Anglada, L.; Perez-Lopez, E.; Lozano, F.S.; Lopez-Corral, L.; Sanchez-Guijo, F.M.; Vazquez, L.; Perez Rivera, J.A.; Martin-Herrero, F.; Sanchez-Barba, M.; et al. Analysis of incidence, risk factors and clinical outcome of thromboembolic and bleeding events in 431 allogeneic hematopoietic stem cell transplantation recipients. Haematologica 2013, 98, 437–443. [Google Scholar] [CrossRef] [Green Version]
- Gerber, D.E.; Segal, J.B.; Levy, M.Y.; Kane, J.; Jones, R.J.; Streiff, M.B. The incidence of and risk factors for venous thromboembolism (VTE) and bleeding among 1514 patients undergoing hematopoietic stem cell transplantation: Implications for VTE prevention. Blood 2008, 112, 504–510. [Google Scholar] [CrossRef]
- Hakim, D.A.; Dangas, G.D.; Caixeta, A.; Nikolsky, E.; Lansky, A.J.; Moses, J.W.; Claessen, B.; Sanidas, E.; White, H.D.; Ohman, E.M.; et al. Impact of baseline thrombocytopenia on the early and late outcomes after ST-elevation myocardial infarction treated with primary angioplasty: Analysis from the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction (HORIZONS-AMI). Am. Heart J. 2011, 161, 391–396. [Google Scholar] [CrossRef]
- Feher, A.; Kampaktsis, P.N.; Parameswaran, R.; Stein, E.M.; Steingart, R.; Gupta, D. Aspirin Is Associated with Improved Survival in Severely Thrombocytopenic Cancer Patients with Acute Myocardial Infarction. Oncologist 2017, 22, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Del Prete, C.; Kim, T.; Lansigan, F.; Shatzel, J.; Friedman, H. The Epidemiology and Clinical Associations of Stroke in Patients With Acute Myeloid Leukemia: A Review of 10,972 Admissions From the 2012 National Inpatient Sample. Clin. Lymphoma. Myeloma Leuk. 2018, 18, 74–77.e1. [Google Scholar] [CrossRef]
- Wang, T.Y.; Ou, F.-S.; Roe, M.T.; Harrington, R.A.; Ohman, E.M.; Gibler, W.B.; Peterson, E.D. Incidence and prognostic significance of thrombocytopenia developed during acute coronary syndrome in contemporary clinical practice. Circulation 2009, 119, 2454–2462. [Google Scholar] [CrossRef] [Green Version]
- Leader, A.; ten Cate, H.; Spectre, G.; Beckers, E.A.M.; Falanga, A. Antithrombotic medication in cancer-associated thrombocytopenia: Current evidence and knowledge gaps. Crit. Rev. Oncol. Hematol. 2018, 132, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Lensing, A.W.A.; Piccioli, A.; Bernardi, E.; Simioni, P.; Girolami, B.; Marchiori, A.; Sabbion, P.; Prins, M.H.; Noventa, F.; et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood 2002, 100, 3484–3488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melloni, C.; Shrader, P.; Carver, J.; Piccini, J.P.; Thomas, L.; Fonarow, G.C.; Ansell, J.; Gersh, B.; Go, A.S.; Hylek, E.; et al. Management and outcomes of patients with atrial fibrillation and a history of cancer: The ORBIT-AF registry. Eur. Hear. J. Qual. Care Clin. Outcomes 2017, 3, 192–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napolitano, M.; Saccullo, G.; Marietta, M.; Carpenedo, M.; Castaman, G.; Cerchiara, E.; Chistolini, A.; Contino, L.; De Stefano, V.; Falanga, A.; et al. Platelet cut-off for anticoagulant therapy in thrombocytopenic patients with blood cancer and venous thromboembolism: An expert consensus. Blood Transfus. 2019, 17, 171–180. [Google Scholar] [CrossRef]
- Kopolovic, I.; Lee, A.Y.Y.; Wu, C. Management and outcomes of cancer-associated venous thromboembolism in patients with concomitant thrombocytopenia: A retrospective cohort study. Ann. Hematol. 2015, 94, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Davis, C.; Wu, Q.; Li, S.; Kesten, M.F.; Holmberg, L.A.; Gopal, A.K.; Garcia, D.A. Management of venous thromboembolism during thrombocytopenia after autologous hematopoietic cell transplantation. Blood Adv. 2017, 1, 707–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iliescu, C.; Balanescu, D.V.; Donisan, T.; Giza, D.E.; Muñoz Gonzalez, E.D.; Cilingiroglu, M.; Song, J.; Mukerji, S.S.; Lopez-Mattei, J.C.; Kim, P.Y.; et al. Safety of Diagnostic and Therapeutic Cardiac Catheterization in Cancer Patients With Acute Coronary Syndrome and Chronic Thrombocytopenia. Am. J. Cardiol. 2018, 122, 1465–1470. [Google Scholar] [CrossRef] [PubMed]
- Lecumberri, R.; Ruiz-Artacho, P.; Trujillo-Santos, J.; Brenner, B.; Barillari, G.; Ruiz-Ruiz, J.; Lorente, M.A.; Verhamme, P.; Vázquez, F.J.; Weinberg, I.; et al. Management and outcomes of cancer patients with venous thromboembolism presenting with thrombocytopenia. Thromb. Res. 2020, 195, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.Y.Y.; Kamphuisen, P.W.; Meyer, G.; Bauersachs, R.; Janas, M.S.; Jarner, M.F.; Khorana, A.A. Tinzaparin vs Warfarin for Treatment of Acute Venous Thromboembolism in Patients With Active Cancer: A Randomized Clinical Trial. JAMA 2015, 314, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.Y.Y.; Levine, M.N.; Baker, R.I.; Bowden, C.; Kakkar, A.K.; Prins, M.; Rickles, F.R.; Julian, J.A.; Haley, S.; Kovacs, M.J.; et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N. Engl. J. Med. 2003, 349, 146–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raskob, G.E.; Van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef]
- Samuelson Bannow, B.T.; Lee, A.; Khorana, A.A.; Zwicker, J.I.; Noble, S.; Ay, C.; Carrier, M. Management of cancer-associated thrombosis in patients with thrombocytopenia: Guidance from the SSC of the ISTH. J. Thromb. Haemost. JTH 2018. [Google Scholar] [CrossRef] [Green Version]
- Samuelson Bannow, B.T.; Walter, R.B.; Gernsheimer, T.B.; Garcia, D.A. Patients treated for acute VTE during periods of treatment-related thrombocytopenia have high rates of recurrent thrombosis and transfusion-related adverse outcomes. J. Thromb. Thrombolysis 2017, 44, 442–447. [Google Scholar] [CrossRef]
- Houghton, D.E.; Key, N.S.; Zakai, N.A.; Laux, J.P.; Shea, T.C.; Moll, S. Analysis of anticoagulation strategies for venous thromboembolism during severe thrombocytopenia in patients with hematologic malignancies: A retrospective cohort. Leuk. Lymphoma 2017, 1–9. [Google Scholar] [CrossRef]
- Livneh, N.; Braeken, D.; Drozdinsky, G.; Gafter-Gvili, A.; Seelig, J.; Rozovski, U.; Raanani, P.; Falanga, A.; ten Cate, H.; Spectre, G.; et al. Anticoagulation management and outcomes in thrombocytopenic cancer patients with atrial fibrillation. Res Pr. Thromb Haemost 2019, 3, PB0909. [Google Scholar]
- Shatzel, J.J.; Mart, D.; Bien, J.Y.; Maniar, A.; Olson, S.; Liem, T.K.; DeLoughery, T.G. The efficacy and safety of a catheter removal only strategy for the treatment of PICC line thrombosis versus standard of care anticoagulation: A retrospective review. J. Thromb. Thrombolysis 2019, 47, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Easaw, J.C.; Shea-Budgell, M.A.; Wu, C.M.J.; Czaykowski, P.M.; Kassis, J.; Kuehl, B.; Lim, H.J.; MacNeil, M.; Martinusen, D.; McFarlane, P.A.; et al. Canadian consensus recommendations on the management of venous thromboembolism in patients with cancer. Part 2: Treatment. Curr. Oncol. 2015, 22, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Carrier, M.; Abou-Nassar, K.; Mallick, R.; Tagalakis, V.; Shivakumar, S.; Schattner, A.; Kuruvilla, P.; Hill, D.; Spadafora, S.; Marquis, K.; et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. N. Engl. J. Med. 2019, 380, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Htun, K.T.; Ma, M.J.Y.; Lee, A.Y.Y. Incidence and outcomes of catheter related thrombosis (CRT) in patients with acute leukemia using a platelet-adjusted low molecular weight heparin regimen. J. Thromb. Thrombolysis 2018, 46, 386–392. [Google Scholar] [CrossRef]
- Samuelson Bannow, B.R.; Lee, A.Y.; Khorana, A.A.; Zwicker, J.I.; Simon, N.; Cihan, A.; Marc, C. Management of anticoagulation for cancer-associated thrombosis in patients with thrombocytopenia: A systematic review. Res. Pract. Thromb. Haemost. 2018, 0. [Google Scholar] [CrossRef]
- Leader, A.; Hamulyák, E.N.; Carney, B.J.; Avrahami, M.; Knip, J.J.; Rozenblatt, S.; Beenen, L.F.; Yust-Katz, S.; Coppens, M.; Raanani, P.; et al. Intracranial Hemorrhage with Direct Oral Anticoagulants in Patients with Brain Metastases [abstract]. Res. Pr. Thromb. Haemost. 2020, 4, 6291–6297. [Google Scholar]
- Leader, A.; Spectre, G.; ten Cate, H.; Falanga, A.; for the MATTER investigators. Prospective Cohort Study on Management and Outcomes in Thrombocytopenic Patients Receiving Antithrombotic Therapy. In Proceedings of the 27th International Society of Thrombosis and Haemostasis (ISTH) Congress and 65rd Annual Scientific and Standardization Committee (SSC) Meeting, Melbourne, Australia, 6–10 July 2019. [Google Scholar]
- Iliescu, C.; Grines, C.L.; Herrmann, J.; Yang, E.H.; Cilingiroglu, M.; Charitakis, K.; Hakeem, A.; Toutouzas, K.; Leesar, M.A.; Marmagkiolis, K. SCAI expert consensus statement: Evaluation, management, and special considerations of cardio-oncology patients in the cardiac catheterization laboratory (Endorsed by the Cardiological Society of India, and Sociedad Latino Americana de Cardiologıa Interve. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2016, 87, 895–899. [Google Scholar] [CrossRef]
- McCarthy, C.P.; Steg, G.; Bhatt, D.L. The management of antiplatelet therapy in acute coronary syndrome patients with thrombocytopenia: A clinical conundrum. Eur. Heart J. 2017, 38, 3488–3492. [Google Scholar] [CrossRef] [Green Version]
- Leader, A.; Ten Cate, V.; Ten Cate-Hoek, A.J.; Spectre, G.; Beckers, E.A.M.; Raanani, P.; Giaccherini, C.; Pereg, D.; Schouten, H.C.; Falanga, A.; et al. Managing Anti-Platelet Therapy in Thrombocytopaenic Patients with Haematological Malignancy: A Multinational Clinical Vignette-Based Experiment. Thromb. Haemost. 2019, 119, 163–174. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Selected mechanisms of drug induced thrombocytopenia in cancer. Examples of implicated drugs are given for each mechanism. HDAC, histone deacetylase.
Figure 1.
Selected mechanisms of drug induced thrombocytopenia in cancer. Examples of implicated drugs are given for each mechanism. HDAC, histone deacetylase.

Figure 2.
Take-home messages. AML, acute myeloid leukemia; EACA, epsilon aminocaproic acid; MDS, myelodysplastic syndrome; TPO-RA, thrombopoietin receptor agonists; TXA, tranexamic acid; VTE, venous thromboembolism.
Figure 2.
Take-home messages. AML, acute myeloid leukemia; EACA, epsilon aminocaproic acid; MDS, myelodysplastic syndrome; TPO-RA, thrombopoietin receptor agonists; TXA, tranexamic acid; VTE, venous thromboembolism.


{kind=link}
{kind=link}
Table 1.
Ongoing and planned clinical trials of antifibrinolytic agents in thrombocytopenic cancer patients 1.
Table 1.
Ongoing and planned clinical trials of antifibrinolytic agents in thrombocytopenic cancer patients 1.
| Name, Identifier | Study Design (Status) | Interventions 2 | Study Population 3 | Primary Outcome | Time Frame | Planned Completion |
|---|---|---|---|---|---|---|
| Antifibrinolytics in Thrombocytopenia | ||||||
| TRial to EvaluAte Tranexamic Acid Therapy in Thrombocytopenia (TREATT), NCT03136445 | Interventional Randomized Phase 3 (recruiting) | Arm A: TXA 1 g q8hrs IV; Arm B: TXA 1.5 g q8hrs PO. | Thrombocytopenic patients (platelet count of ≤10 × 10⁹/L for ≥ 5 days) with hematological malignancies (n = 616) | Death or bleeding (WHO grade ≥ 2) | 30 days | March 2021 |
| PRevention of BLeeding in hEmatological Malignancies with Antifibrinolytic (PROBLEMA), NCT02074436 | Interventional Randomized Phase 2 (recruiting) | Arm A: EACA 1000 mg q12hrs; Arm B: standard prophylactic platelet transfusion | Thrombocytopenic patients (platelet count < 20 × 10⁹/L) with hematological malignancies (n = 100) | Major bleeding episodes (WHO grades 3–4) | 6 mo. | May 2021 |
| Evolution of Thromboelastography During Tranexamic Acid Treatment (TTRAP-Bleeding), NCT03801122 | Interventional Randomized Phase 2 (recruiting) | Arm A: TXA 3 g/day; Arm B: TXA 1.5 g/day; Arm C: No TXA | Thrombocytopenic patients (platelet count of ≤10 × 10⁹/L for ≥ 5 days) with hematological malignancies (n = 18) | Level of clot amplitude in thrombo-elastography | 30 days | 1 April 2022 |
1 Interventional phase 2 and 3 studies shown, as identified in https://www.clinicaltrials.gov/ (accessed on 31 January 2021). 2 The ratio between intervention arms is 1:1 or 1:1:1 unless otherwise specified. 3 All participants are aged 18 years or older, unless otherwise specified. EACA, epsilon aminocaproic acid; IV, intravenous; PLT, platelet count (×109/L); TXA, tranexamic acid.
Table 2.
Summary of studies on TPO-RAs in MDS and AML.
| Design | Population | PLT, 109/L | Intervention | TPO-RA Dose | Participants, n | Primary Outcome | Follow up | Results | Comments | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|
| Phase 2 randomized | Low-int 1 MDS | <20 | Romiplostim or placebo | 250–1000 µg (750 µg start) | n(romi) = 167; n(placebo) = 83 | CSBE | 58 wks. | No difference in CSBE. Decreased overall bleeding. PLT increased. Transfusion reduced. | Early termination due to transient increase in peripheral blasts with romi. No increase in AML (18% vs. 20.5%) | [75] |
| n(romi) = 139; n(placebo) = 83 | OS and leukemic progression | 5 years | No difference in OS or leukemic progression | [76] | ||||||
| Phase I of single blind randomized phase 2 trial | Low-Int 1 MDS | <30 | Eltrombopag or placebo | 50–300 mg | n(el-pag) = 59; n(placebo) = 39 | Platelet response | 11 wks. (median) | 47% platelet response. Less bleeding | No difference in AML progression | [77] |
| Phase 2 | Low risk MDS | <30 | Eltrombopag | 50–150 mg | 25 | Hematologic response | 16 wks. | 44% response | 24% bi-lineage response | [78] |
| Phase 1/2 | Advanced MDS or AML | <30 | Eltrombopag or placebo | 50–300 mg | n(el-pag) = 64; n(placebo) = 34 | Safety & tolerability | 6 mo. (optional 6 mo. extension) | Acceptable safety profile | No increase in marrow or peripheral blasts | [79] |
| Phase 3 | Int-High risk MDS receiving azacitidine | <75 | Eltrombopag or placebo | 200–300 mg | n(el-pag) = 179; n(placebo) = 177 | Platelet transfusion free | Cycles 1–4 | More transfusion free with placebo (31%) than eltrombopag (16%). Worse PLT recovery | Terminated early due to futility and safety. Trend to AML progression. | [80] |
| Phase 2 double blind randomized | AML induction | Eltrombopag or placebo | 200 mg | n(el-pag) = 74; n(placebo) = 74 | Safety & tolerability | Until PLT > 200 or 42 days post-induction | More SAEs with eltrombopag | Numerically more deaths with eltrombopag. Same VTE rates. | [81] |
AML, acute myeloid leukemia; CSBE, clinically significant bleeding events; el-pag, eltrombopag; MDS, myelodysplastic syndrome; OS, overall survival; PLT, platelet count; romi, romiplostim; SAE. Serious adverse events; TPO-RA, thrombopoietin receptor agonists; VTE, venous thromboembolism; wk, week.
Table 3.
Selected studies on TPO-RAs for preventing or treating CIT in solid tumors.
| Design | Cancer Type | PLT, 109/L | Intervention | TPO-RA Dose | Participants, n | Primary Outcome | Follow up | Key Results | Comments | Ref |
|---|---|---|---|---|---|---|---|---|---|---|
| Retrospective cohort | Wide range, mostly GI | 75 (median) | Romiplostim | 3 µg/kg/wk (median starting) | 22 | ChemoRx dose delay and/or reduction | NR | Reduced dose delay (36% vs. 94%) and reduction | No thrombosis | [93] |
| Retrospective cohort | Wide range | <100 for ≥6 weeks (mean 58; range 3–97) | Romiplostim | 2.9 µg/kg/wk (mean) | 20 | PLT > 100; ChemoRx delay | NR | 95% PLT >100; 75% resumed ChemoRx without TCP | 3 DVT patients (15%) could continue ChemoRx | [94] |
| Retrospective cohort | Wide range, mostly GI | <100 | Romiplostim | 2 µg/kg/wk (median starting) | 37 | PLT > 100; ChemoRx continued | 18 wk (median) | 95% PLT < 100; 92% continued ChemoRx | 14% (n = 6) thrombosis. Mostly in pancreatic cancer (5/6) | [95] |
| Phase 2 randomized open label | Wide range, mostly GI | <100 | Romiplostim or placebo | 1 µg/kg/wk (starting) | n(romi) = 15; n(placebo) = 8; n(open-label-romi) = 37 | PLT > 100 within 3 wks | 6 wk | Overall response (n = 54) 85% | 10% VTE | [96] |
| Phase 2 | NSCLC with Gemcitabine and carboplatin/ cisplatin Rx | <50–100 | Romiplostim or placebo | 250–750 µg/wk | n(romi) = 50; n(placebo) = 12 | Adverse events | ≤5 cycles | Well tolerated. No effect on PLT or dose reduction | 6% thrombosis | [97] |
| Retrospective cohort | Wide range | <100 for 3 weeks | Romiplostim | 3 µg/kg/wk (median starting) | 153 | PLT response = Median PLT >75 or baseline +30 | NR | 71% response. 79% avoided dose delays or reduction | Less bleeding. 5.2% VTE (similar to historical controls) | [89] |
| Phase 2 open label single arm | Glioblastoma | <50 | Romiplostim | 750 µg/wk (starting; dose adjusted) | 20 | Proportion completing 6 cycles | 6 cycles | 60% completed 6 cycles | 5% lower limb ischemia; 5% VTE | [90] |
| Phase 2 | Advanced solid tumors, with Gemcitabine ± Carboplatin Rx | <150 | Eltrombopag or placebo | 100 mg/day | n(el-pag) = 53; n(placebo) = 23 | PLT pre + post ChemoRx | 6 cycles | Less time to PLT recovery; Fewer dose delays or reduction | Reduced rates of anemia and leukopenia | [98] |
| Phase 3 | Ovarian, small cell lung cancer, NSCLC, bladder cancer | <50 in a previous treatment cycle | Avatrombopag or placebo | 60 mg/day (5 days pre and post Rx) | 122 (ava-pag:placebo, 2:1) | PLT transfusion or dose delays or reduction | No difference between ava-pag and placebo | Higher PLT in ava-pag group | [91,92] |
ava-pag; avatrombopag; ChemoRx, chemotherapy; CIT, chemotherapy-induced thrombocytopenia; DVT, deep vein thrombosis; el-pag; eltrombopag; GI, gastrointestinal; NR, not reported; NSCLC, non-small cell lung cancer; PLT, platelet count; romi, romiplostim; Rx, treatment; TCP, thrombocytopenia; TPO-RA, thrombopoietin receptor agonists; VTE, venous thromboembolism; wk, week.
Table 4.
Ongoing and planned clinical trials of TPO-RAs in thrombocytopenia and cancer 1.
| Name, Identifier | Study Design (Status) | Interventions 2 | Study Population 3 | Primary Outcome | Time Frame | Planned Completion |
|---|---|---|---|---|---|---|
| TPO-RAs in Hematological Malignancies | ||||||
| Eltrombopag for the Treatment of Thrombocytopenia Due to Low- and Intermediate Risk Myelodysplastic Syndromes, NCT02912208 | Interventional Randomized Phase 2 (recruiting) | >Arm A: eltrombopag 50–300 mg/day; Arm B: placebo | Stable low or int 1 MDS with PLT < 30, ineligible to receive other treatment options (n = 174) | Platelet response rate (complete or any) | 6 mo. | August 2019 |
| Phase II Study of Lenalidomide and Eltrombopag in Patients with Symptomatic Anemia in Low or Intermediate I Myelodysplastic Syndrome (MDS), NCT01772420 | Interventional non-randomized Phase 2 with parallel assignment (recruiting) | Arm A if PLT > 50: lenalidomide and eltrombopag; Arm B if PLT < 50: eltrombopag until PLT > 50 for 2 wks. Then, Arm A. | Low-int 1 MDS or chronic myelomonocytic leukemia (n = 60) | Hematologic improvement as defined by the IWG 2006 criteria | 8 weeks | January 2020 |
| Eltrombopag in Myelodysplastic Syndrome (MDS) Patients with Thrombocytopenia, NCT01286038 | Interventional single arm Phase 1–2 (active, not recruiting) | Eltrombopag | MDS after hypomethylating agent failure and PLT < 50 (n = 37) | Maximum tolerated dose | 24 mo. | September 2021 |
| Validation of a predictive model of response to romiplostim in patients with IPSS low or intermediate-1 risk MDS and thrombocytopenia (EUROPE-trial), | Interventional non-randomized Phase 2 with parallel assignment (recruiting) | Romiplostim stratified using TPO-based model to Arm A (score +3), Arm B (−1 or −2), Arm C (−6) | Low or int 1 MDS with PLT < 30 or PLT < 50 and bleeding (n = 84) | Hematologic improvement of platelets (HI-P) after 4 months on therapy | 12 mo. | December 2021 |
| Eltrombopag Olamine in Treating Thrombocytopenia in Patients with Chronic Myeloid Leukemia or Myelofibrosis Receiving Tyrosine Kinase Therapy, NCT01428635 | Interventional single arm Phase 2 (active, not recruiting) | Eltrombopag | CML or MF patients with platelets <50 × 109/L (CML) or <100 × 109/L (MF) after 3 mo. of TKIs (n = 39) | Complete platelet response | 30 days after last dose of eltrombopag | 31 January 2022 |
| Using Romiplostim to Treat Low Platelet Counts Following Chemotherapy and Autologous Hematopoietic Cell Transplantation in People with Blood Cancer, NCT04478123 | Interventional single arm Phase 2 (recruiting) | Romiplostim 3 µg/kg on day 1+ after transplant (start dose) | Patients with multiple myeloma or lymphoma undergoing high dose chemotherapy with autologous stem cell transplant (n = 60) | No. of days post-transplant requiring platelet transfusions or grade 4 thrombocytopenia | 42 days | July 2022 |
| Using Romiplostim to Treat Low Platelet Counts during Chemotherapy in People with Lymphoma, NCT04673266 | Interventional single arm Phase 2 (recruiting) | 3 µg/kg/wk. on day 1 of chemotherapy cycle, titrated weekly | Lymphoma patients receiving chemotherapy, with grade 4 thrombocytopenia during previous cycle or PLT < 50 on day 1 of current cycle (n = 20) | PLT indication for dose delay (see definition) | 1 year | December 2022 |
| Study Impact on Outcome of Eltrombopag in Elderly Patients with Acute Myeloid Leukemia Receiving Induction Chemotherapy (EPAG2015), NCT03603795 | Interventional Randomized Phase 2 (recruiting) | Arm A: eltrombopag 200 mg/day; Arm B: placebo | Patients aged ≥ 60yrs with de novo AML eligible for intensive induction chemotherapy (n = 110) | Overall survival rate | 12 mo. | September 2024 |
| TPO-RAs for CIT in solid tumors | ||||||
| A Study of Romiplostim to Prevent Low Platelet Counts in Children and Young Adults Receiving Chemotherapy for Solid Tumors, NCT04671901 | Interventional single arm Phase 2 (recruiting) | 3 µg/kg/wk. from cycle 4, titrated weekly | Patients aged 1–21 years with a primary solid tumor undergoing N8/EFT chemotherapy treatment (n = 30) | No. of platelet transfusions | 6 mo. | 10 December 2022 |
| Study of Romiplostim for Chemotherapy-induced Thrombocytopenia in Adult Subjects with Gastrointestinal, Pancreatic, or Colorectal Cancer (RECITE), NCT03362177 | Randomized double-blind placebo controlled Phase 3 (recruiting) | Arm A: romiplostim 3 µg/kg/wk., titrated weekly; Arm B: placebo (2:1 ratio) | Patients receiving oxaliplatin-based chemotherapy for gastrointestinal/ colorectal/ pancreatic cancer, with PLT < 75 at or after scheduled start of next cycle (n = 162) | Thrombocytopenia-induced chemotherapy dose modification during the second or third on study chemotherapy cycles | 48 days | 1 June 2023 |
| Study of Romiplostim for Chemotherapy-induced Thrombocytopenia in Adult Subjects with Non-small Cell Lung Cancer (NSCLC), Ovarian Cancer, or Breast Cancer, NCT03937154 | Randomized double-blind placebo controlled Phase 3 (recruiting) | Arm A: romiplostim; Arm B: placebo (2:1 ratio) | Patients receiving carboplatin-based chemotherapy for locally advanced or metastatic non-small cell lung cancer, ovarian cancer, or breast cancer, with PLT < 75 at or after scheduled start of next cycle (n = 162) | Chemotherapy dose delay or reduction | 48 days | 28 June 2023 |
| Avatrombopag on the Treatment of Thrombocytopenia Induced by Chemotherapy of Malignant Tumors, NCT04609891 | Interventional single arm Phase 2 (recruiting) | Avatrombopag 40 mg or 60 mg, depending on PLT. Duration differs between prevention and treatment | Patients with solid tumors receiving chemotherapy, and 10 < PLT < 75 after the last cycle (n = 80) | Chemotherapy dose delay or reduction, or platelet transfusion | 2 mo. | 31 August 2021 |
1 Interventional phase 2 and 3 studies shown, as identified in https://www.clinicaltrials.gov/ (accessed on 31 January 2021). 2 The ratio between intervention arms is 1:1 or 1:1:1 unless otherwise specified. 3 All participants are aged 18 years or older, unless otherwise specified. AML, acute myeloid leukemia; CIT, chemotherapy induced thrombocytopenia; CML, chronic myeloid leukemia; MDS, myelodysplastic syndrome; MF, myelofibrosis; mo., months; PLT, platelet count (x109/L); TKI, tyrosine kinase inhibitor; TPO-RA, thrombopoietin receptor agonist.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Leader, A.; Hofstetter, L.; Spectre, G. Challenges and Advances in Managing Thrombocytopenic Cancer Patients. J. Clin. Med. 2021, 10, 1169. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10061169
AMA Style
Leader A, Hofstetter L, Spectre G. Challenges and Advances in Managing Thrombocytopenic Cancer Patients. Journal of Clinical Medicine. 2021; 10(6):1169. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10061169
Chicago/Turabian StyleLeader, Avi, Liron Hofstetter, and Galia Spectre. 2021. "Challenges and Advances in Managing Thrombocytopenic Cancer Patients" Journal of Clinical Medicine 10, no. 6: 1169. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10061169
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.