
Diagnostic Accuracy of Non-Imaging and Ultrasound-Based Assessment of Hepatic Steatosis Using Controlled Attenuation Parameter (CAP) as Reference

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Clinical Assessment
2.3. CAP Measurements
2.4. Ultrasound Examination: Hamaguchi’s Score and the HRI
2.5. Fatty Liver Disease Algorithms
2.6. Statistical Analysis
3. Results
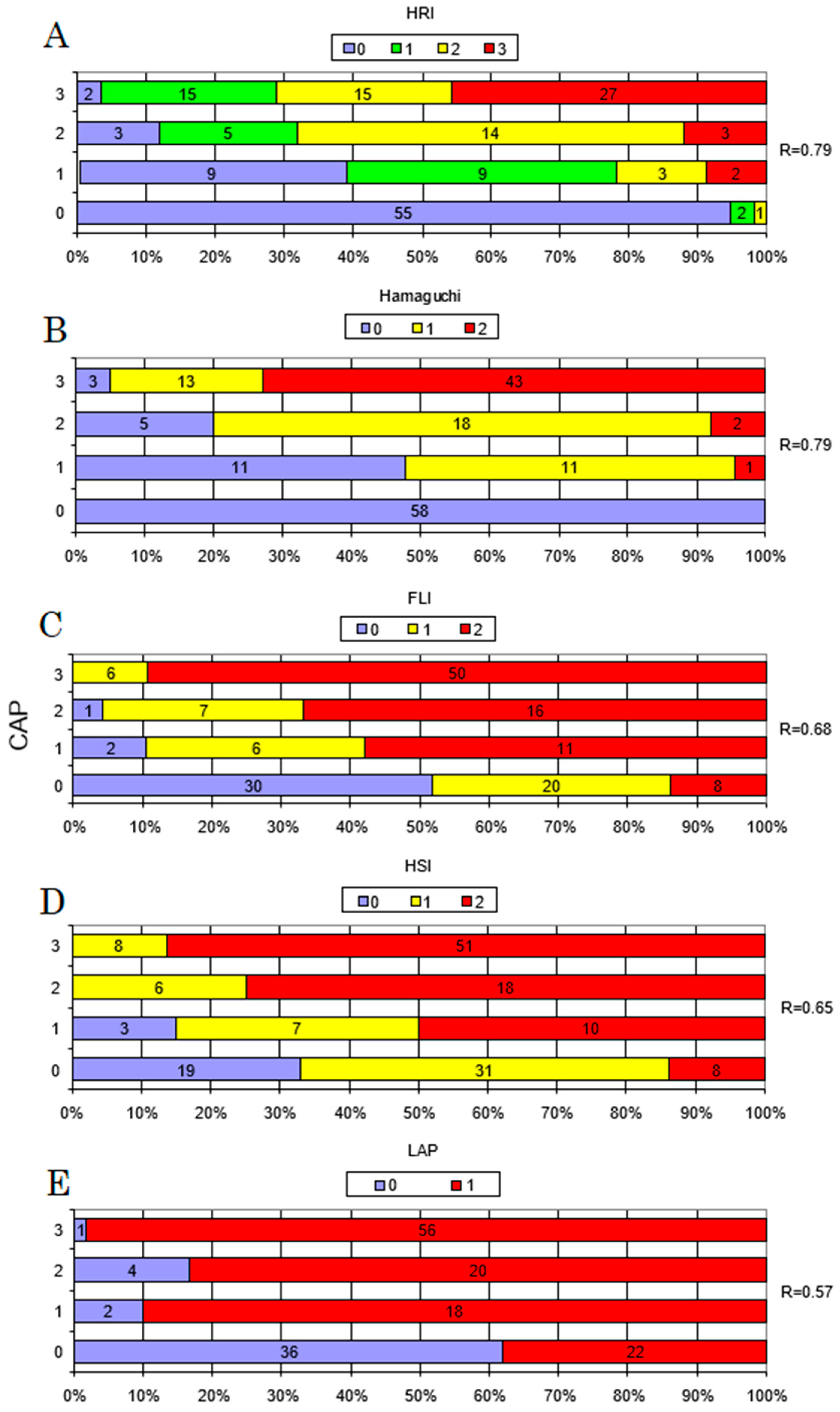
3.1. Correlation between CAP and Non-Invasive Indexes
3.2. Optimal Thresholds
3.3. Optimal Steatosis Prediction Model
4. Discussion
4.1. Main Findings
4.1.1. Ultrasound-Based Techniques
4.1.2. Biomarkers
4.2. Strengths and Limitations of the Study
4.3. Implications for Clinical Use
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Tsai, E.; Lee, T.-P. Diagnosis and Evaluation of Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis, Including Noninvasive Biomarkers and Transient Elastography. Clin. Liver Dis. 2018, 22, 73–92. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, M.; Zhang, X. Non-Alcoholic Fatty Liver Disease: An Expanded Review. World J. Hepatol. 2017, 9, 715. [Google Scholar] [CrossRef]
- Ratziu, V.; Charlotte, F.; Heurtier, A.; Gombert, S.; Giral, P.; Bruckert, E.; Grimaldi, A.; Capron, F.; Poynard, T.; LIDO Study Group. Sampling Variability of Liver Biopsy in Nonalcoholic Fatty Liver Disease. Gastroenterology 2005, 128, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the Epidemic of Nonalcoholic Fatty Liver Disease Demonstrates an Exponential Increase in Burden of Disease: Estes et al. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic Review: The Epidemiology and Natural History of Non-Alcoholic Fatty Liver Disease and Non-Alcoholic Steatohepatitis in Adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef]
- Pu, K.; Wang, Y.; Bai, S.; Wei, H.; Zhou, Y.; Fan, J.; Qiao, L. Diagnostic Accuracy of Controlled Attenuation Parameter (CAP) as a Non-Invasive Test for Steatosis in Suspected Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2019, 19, 51. [Google Scholar] [CrossRef] [Green Version]
- Karlas, T.; Petroff, D.; Sasso, M.; Fan, J.-G.; Mi, Y.-Q.; de Lédinghen, V.; Kumar, M.; Lupsor-Platon, M.; Han, K.H.; Cardoso, A.C.; et al. Individual Patient Data Meta-Analysis of Controlled Attenuation Parameter (CAP) Technology for Assessing Steatosis. Hepatology 2017, 66, 1022–1030. [Google Scholar] [CrossRef]
- Karlas, T.; Petroff, D.; Garnov, N.; Böhm, S.; Tenckhoff, H.; Wittekind, C.; Wiese, M.; Schiefke, I.; Linder, N.; Schaudinn, A.; et al. Non-Invasive Assessment of Hepatic Steatosis in Patients with NAFLD Using Controlled Attenuation Parameter and 1H-MR Spectroscopy. PLoS ONE 2014, 9, e91987. [Google Scholar] [CrossRef] [Green Version]
- Eddowes, P.J.; Sasso, M.; Allison, M.; Tsochatzis, E.; Anstee, Q.M.; Sheridan, D.; Guha, I.N.; Cobbold, J.F.; Deeks, J.J.; Paradis, V.; et al. Accuracy of FibroScan Controlled Attenuation Parameter and Liver Stiffness Measurement in Assessing Steatosis and Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1717–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalhana, S.; Leitão, J.; Alves, A.C.; Bourbon, M.; Cortez-Pinto, H. How Good is Controlled Attenuation Parameter and Fatty Liver Index for Assessing Liver Steatosis in General Population: Correlation with Ultrasound. Liver Int. 2014, 34, e111–e117. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G.; Monteiro, L.B.S. Ultrasound-Based Techniques for the Diagnosis of Liver Steatosis. World J. Gastroenterol. 2019, 25, 6053–6062. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. Hepatology 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Itoh, Y.; Harano, Y.; Fujii, K.; Nakajima, T.; Kato, T.; Takeda, N.; Okuda, J.; Ida, K.; et al. The Severity of Ultrasonographic Findings in Nonalcoholic Fatty Liver Disease Reflects the Metabolic Syndrome and Visceral Fat Accumulation. Am. J. Gastroenterol. 2007, 102, 2708–2715. [Google Scholar] [CrossRef]
- Webb, M.; Yeshua, H.; Zelber-Sagi, S.; Santo, E.; Brazowski, E.; Halpern, Z.; Oren, R. Diagnostic Value of a Computerized Hepatorenal Index for Sonographic Quantification of Liver Steatosis. Am. J. Roentgenol. 2009, 192, 909–914. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic Steatosis Index: A Simple Screening Tool Reflecting Nonalcoholic Fatty Liver Disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Bedogni, G.; Kahn, H.S.; Bellentani, S.; Tiribelli, C. A Simple Index of Lipid Overaccumulation is a Good Marker of Liver Steatosis. BMC Gastroenterol. 2010, 10, 98. [Google Scholar] [CrossRef] [Green Version]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic Accuracy and Reliability of Ultrasonography for the Detection of Fatty Liver: A Meta-Analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [Green Version]
- Marshall, R.H.; Eissa, M.; Bluth, E.I.; Gulotta, P.M.; Davis, N.K. Hepatorenal Index as an Accurate, Simple, and Effective Tool in Screening for Steatosis. Am. J. Roentgenol. 2012, 199, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Borges, V.F.; Diniz, A.L.D.; Cotrim, H.P.; Rocha, H.L.O.G.; Andrade, N.B. Sonographic Hepatorenal Ratio: A Noninvasive Method to Diagnose Nonalcoholic Steatosis. J. Clin. Ultrasound 2013, 41, 18–25. [Google Scholar] [CrossRef]
- Chauhan, A.; Sultan, L.R.; Furth, E.E.; Jones, L.P.; Khungar, V.; Sehgal, C.M. Diagnostic Accuracy of Hepatorenal Index in the Detection and Grading of Hepatic Steatosis: Factors Affecting the Accuracy Of HRI. J. Clin. Ultrasound 2016, 44, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; LIDO Study Group. Performance and Limitations of Steatosis Biomarkers in Patients with Nonalcoholic Fatty Liver Disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Johansson, L.; Ahlström, H.; Eriksson, J.W.; Larsson, A.; Risérus, U.; Kullberg, J.; Oscarsson, J. Comparison of Four Non-Alcoholic Fatty Liver Disease Detection Scores in a Caucasian Population. World J. Hepatol. 2020, 12, 149–159. [Google Scholar] [CrossRef]
- Sviklāne, L.; Olmane, E.; Dzērve, Z.; Kupčs, K.; Pīrāgs, V.; Sokolovska, J. Fatty Liver Index and Hepatic Steatosis Index for Prediction of Non-Alcoholic Fatty Liver Disease in Type 1 Diabetes: Hepatic Steatosis Indices in Diabetes. J. Gastroenterol. Hepatol. 2018, 33, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Koehler, E.M.; Schouten, J.N.L.; Hansen, B.E.; Hofman, A.; Stricker, B.H.; Janssen, H.L.A. External Validation of the Fatty Liver Index for Identifying Nonalcoholic Fatty Liver Disease in a Population-based Study. Clin. Gastroenterol. Hepatol. 2013, 11, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Piazzolla, V.A.; Mangia, A. Noninvasive Diagnosis of NAFLD and NASH. Cells 2020, 9, 1005. [Google Scholar] [CrossRef]
- Motamed, N.; Sohrabi, M.; Ajdarkosh, H.; Hemmasi, G.; Maadi, M.; Sayeedian, F.S.; Pirzad, R.; Abedi, K.; Aghapour, S.; Fallahnezhad, M.; et al. Fatty Liver Index Vs Waist Circumference for Predicting Non-Alcoholic Fatty Liver Disease. World J. Gastroenterol. 2016, 22, 3023–3030. [Google Scholar] [CrossRef]
- Zheng, S.; Tong, M.; Dong, L.; Du, C.; Zheng, X.; Wang, L.; Huang, P.; Liu, W.; Lin, M.; Liu, C. Lipid Accumulation Product Independently Correlate with Hepatic Steatosis Quantified by Controlled Attenuation Parameter in Women with Polycystic Ovary Syndrome. Endocr. Connect. 2020, 9, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Kuwashiro, T.; Takahashi, H.; Hyogo, H.; Ogawa, Y.; Imajo, K.; Yoneda, M.; Nakahara, T.; Oeda, S.; Tanaka, K.; Amano, Y.; et al. Discordant Pathological Diagnosis of Non-Alcoholic Fatty Liver Disease: A Prospective Multicenter Study. J.G.H. Open. 2020, 4, 497–502. [Google Scholar] [CrossRef] [Green Version]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caussy, C.; Brissot, J.; Singh, S.; Bassirian, S.; Hernandez, C.; Bettencourt, R.; Rizo, E.; Richards, L.; Sirlin, C.B.; Loomba, R. Prospective, Same-Day, Direct Comparison of Controlled Attenuation Parameter With the M vs the XL Probe in Patients With Nonalcoholic Fatty Liver Disease, Using Magnetic Resonance Imaging–Proton Density Fat Fraction as the Standard. Clin. Gastroenterol. Hepatol. 2020, 18, 1842–1850.e6. [Google Scholar] [CrossRef] [PubMed]
- Caussy, C.; Alquiraish, M.H.; Nguyen, P.; Hernandez, C.; Cepin, S.; Fortney, L.E.; Ajmera, V.; Bettencourt, R.; Collier, S.; Hooker, J.; et al. Optimal Threshold of Controlled Attenuation Parameter with MRI-PDFF as the Gold Standard for the Detection of Hepatic Steatosis. Hepatology 2018, 67, 1348–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozłowska-Petriczko, K.; Wunsch, E.; Milkiewicz, P. Controlled Attenuation Parameter in Nonalcoholic Fatty Liver Disease: The Thresholds Do Matter. Clin. Gastroenterol. Hepatol. 2020. [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 167) | NAFLD (n = 109) | Non-NAFLD (n = 58) | p Value | |
|---|---|---|---|---|
| Demographic Data | ||||
| Age, years | 52.6 (12.4) | 53 (12.3) | 51.9 (12.6) | 0.58 |
| Female | 103 (62%) | 66 (61%) | 37 (64%) | 0.68 |
| Clinical Data | ||||
| Type 2 diabetes | 16 (10%) | 16 (15%) | 0 | <0.005 |
| Hypertension | 58 (35%) | 46 (42%) | 12 (21%) | <0.01 |
| BMI, kg/m2 | 28.6 (5.1) | 30.9 (4.4) | 24.2 (2.9) | <0.0001 |
| Waist circumference, cm | 95.0 (15) | 103.1 (10.6) | 80.3 (9.2) | <0.0001 |
| Hip circumference, cm | 105.4 (9.5) | 109.1 (9.4) | 98.9 (5.4) | <0.0001 |
| Statins | 21 (13%) | 20 (18%) | 1 (2%) | <0.01 |
| Obesity † | 116 (70%) | 99 (90%) | 17 (29%) | <0.0001 |
| Laboratory measures | ||||
| AST, U/L | 24 (12) | 27 (14) | 21 (7) | <0.001 |
| ALT, U/L | 23 (20) | 26 (24) | 17 (7) | <0.001 |
| GGT, U/L | 39 (32) | 49 (35) | 20 (14) | <0.0001 |
| ALP, U/L | 72 (25) | 77 (26) | 62 (19) | <0.001 |
| Total bilirubin, mg/dL | 0.5 (0.3) | 0.5 (0.3) | 0.5 (0.3) | 0.37 |
| Albumin, g/L | 49 (4) | 48 (3) | 49 (6) | 0.64 |
| Glucose, mg/dL | 100 (21) | 103 (25) | 95 (12) | 0.21 |
| Triglycerides, mg/dL | 141 (75) | 161 (82) | 105 (40) | <0.0001 |
| Total cholesterol, mg/dL | 202 (42) | 198 (43) | 208 (40) | 0.12 |
| LDL-cholesterol, mg/dL | 130 (37) | 130 (38) | 129 (36) | 0.78 |
| Ferritin, ng/mL | 166 (164) | 207 (186) | 91 (69) | <0.0001 |
| Fasting insulin, U/mL | 17 (22) | 20 (26) | 11 (11) | 0.01 |
| HOMA-IR | 3.8 (3.6) | 4.5 (3.8) | 2.7 (2.9) | <0.0001 |
| Creatinine, mg/dL | 0.9 (0.2) | 0.9 (0.2) | 0.9 (0.2) | 0.43 |
| Steatosis prediction algorithms | ||||
| FLI | 59.2 (28.1) | 73.7 (20.8) | 34.6 (20.8) | <0.0001 |
| HSI | 36.9 (6.5) | 39.9 (5.4) | 31.6 (4.5) | <0.0001 |
| LAP | 57.4 (47.3) | 76.3 (49.2) | 24.6 (15.2) | <0.0001 |
| Imaging Data | ||||
| Hamaguchi’s score | 1.97 (2) | 3 (1.7) | 0 (0) | <0.0001 |
| HRI | 1.7 (0.5) | 2 (0.4) | 1.27 (0.2) | <0.0001 |
| CAP | 274 (60) | 309.1 (42.8) | 208.6 (19.3) | <0.0001 |
| CAP in classes | S0: 58 (34.7%) | S1: 23 (13.8%) S2: 26 (15.6%) S3: 60 (35.9%) | <0.0001 | |
| IQR of CAP | 26.6 | 26.9 | 26.3 | 0.60 |
| TE | 5.1 (2.1) | 5.5 (2.4) | 4.4 (1) | <0.001 |
| IQR of TE | 13.7 | 13.4 | 14.1 | 0.55 |
| Probe size, n | ||||
| Use of M Probe | 143 (85%) | 84 (77%) | 58 (100%) | <0.0001 |
| Use of XL probe | 25 (15%) | 25 (23%) | 0 (0%) | |
| AUC (95% Confidence Interval) | Cut-Off Value | Sensitivity (%) | Specificity (%) | Kendall’s Tau-B | p Value | |
|---|---|---|---|---|---|---|
| Detection of CAP ≥234 Hamaguchi’s score | 0.94 (0.9–0.97) | 2 | 82.2 | 100 | 0.79 | <0.0001 |
| Detection of CAP ≥234 HRI | 0.94 (0.91–0.98) | 1.49 | 86.9 | 94.8 | 0.79 | <0.0001 |
| Detection of CAP ≥234 FLI | 0.90 (0.85–0.94) | 60 | 77.8 | 86.2 | 0.62 | <0.0001 |
| Detection of CAP ≥234 HSI | 0.90 (0.86–0.95) | 36 | 76.7 | 86.2 | 0.61 | <0.0001 |
| Detection of CAP ≥234 LAP | 0.92 (0.88–0.96) | 23 a 30.5 b | 93.1 | 62.1 | 0.6 | <0.0001 |
| Test Result Variable(s) | Cut-off Value | Sensitivity (%) | Specificity (%) | Kendall’s Tau-B | p Value | |
|---|---|---|---|---|---|---|
| CAP ≥ S1 | Hamaguchi ≥ S1 | 1 | 86.9 | 100 | 0.84 | <0.0001 |
| CAP ≥ S2 | Hamaguchi ≥ S2 | 3 | 79.8 | 97.5 | 0.78 | <0.0001 |
| CAP ≥ S3 | Hamaguchi ≥ S3 | 4 | 72.9 | 97.2 | 0.75 | <0.0001 |
| CAP ≥ S1 | HRI ≥ S1 | 1.41 | 91.6 | 86.2 | 0.78 | <0.0001 |
| CAP ≥ S2 | HRI ≥ S2 | 1.56 | 94 | 80.2 | 0.75 | <0.0001 |
| CAP ≥ S3 | HRI ≥ S3 | 2.015 | 57.6 | 90.6 | 0.52 | <0.0001 |
| Partial Correlation | p Value | R | |
|---|---|---|---|
| Hamaguchi’s score | 0.74 | <0.0001 | 0.87 |
| HSI | 0.46 | <0.0001 | |
| Hamaguchi’s score | 0.73 | <0.0001 | |
| BMI | 0.29 | <0.001 | 0.89 |
| Ferritin | 0.22 | <0.01 | |
| GGT | 0.20 | 0.0149 | |
| Hamaguchi’s score | 0.74 | <0.0001 | 0.91 |
| LAP | 0.17 | 0.06 | |
| HSI | 0.21 | 0.0192 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozłowska-Petriczko, K.; Wunsch, E.; Petriczko, J.; Syn, W.-K.; Milkiewicz, P. Diagnostic Accuracy of Non-Imaging and Ultrasound-Based Assessment of Hepatic Steatosis Using Controlled Attenuation Parameter (CAP) as Reference. J. Clin. Med. 2021, 10, 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10071507
Kozłowska-Petriczko K, Wunsch E, Petriczko J, Syn W-K, Milkiewicz P. Diagnostic Accuracy of Non-Imaging and Ultrasound-Based Assessment of Hepatic Steatosis Using Controlled Attenuation Parameter (CAP) as Reference. Journal of Clinical Medicine. 2021; 10(7):1507. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10071507
Chicago/Turabian StyleKozłowska-Petriczko, Katarzyna, Ewa Wunsch, Jan Petriczko, Wing-Kin Syn, and Piotr Milkiewicz. 2021. "Diagnostic Accuracy of Non-Imaging and Ultrasound-Based Assessment of Hepatic Steatosis Using Controlled Attenuation Parameter (CAP) as Reference" Journal of Clinical Medicine 10, no. 7: 1507. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10071507