
Coronary Microvascular Dysfunction: PET, CMR and CT Assessment

 , , and
, , and
Abstract
:1. Introduction
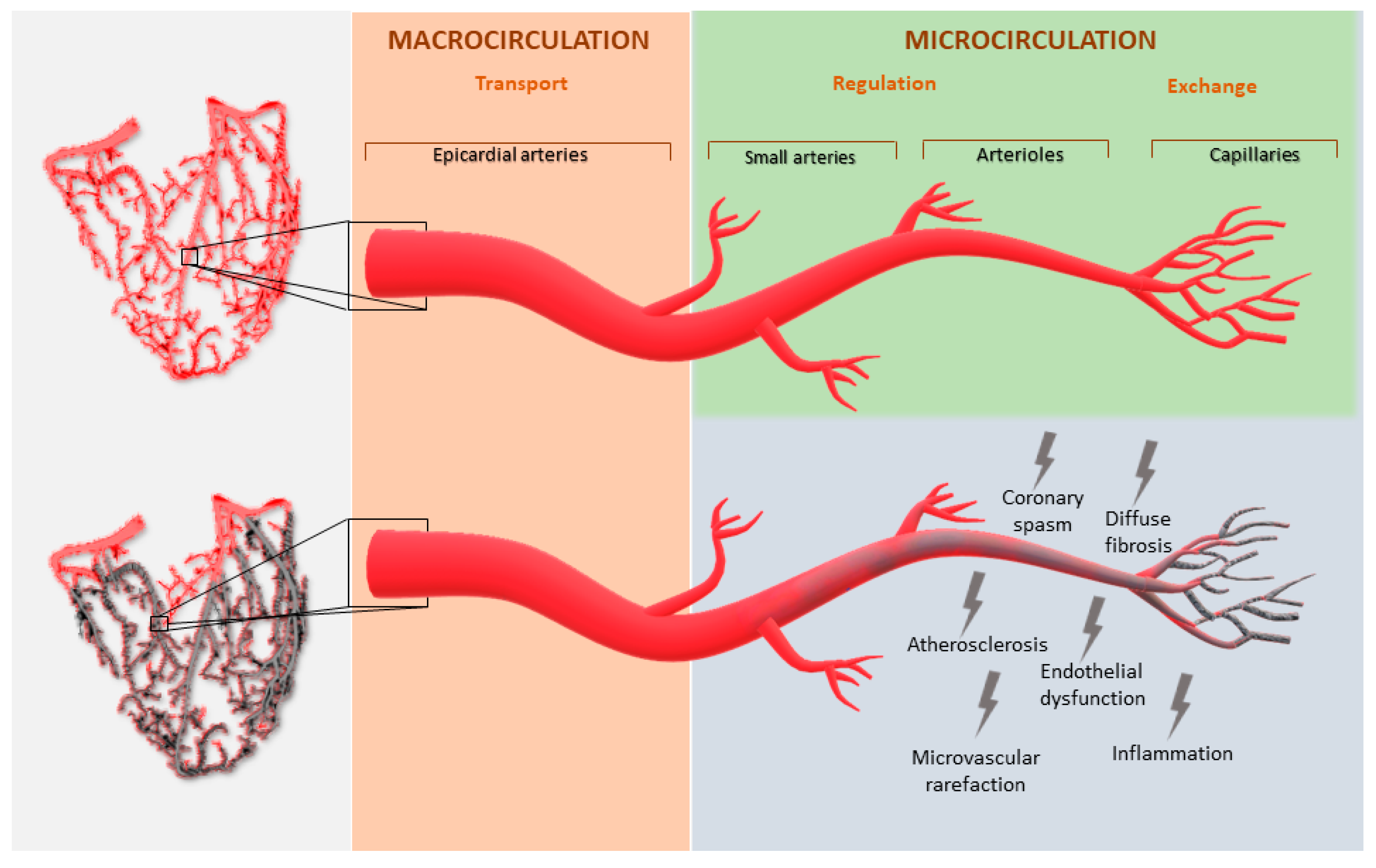
2. Microvascular Physiology and Dysfunction
3. Cardiac PET
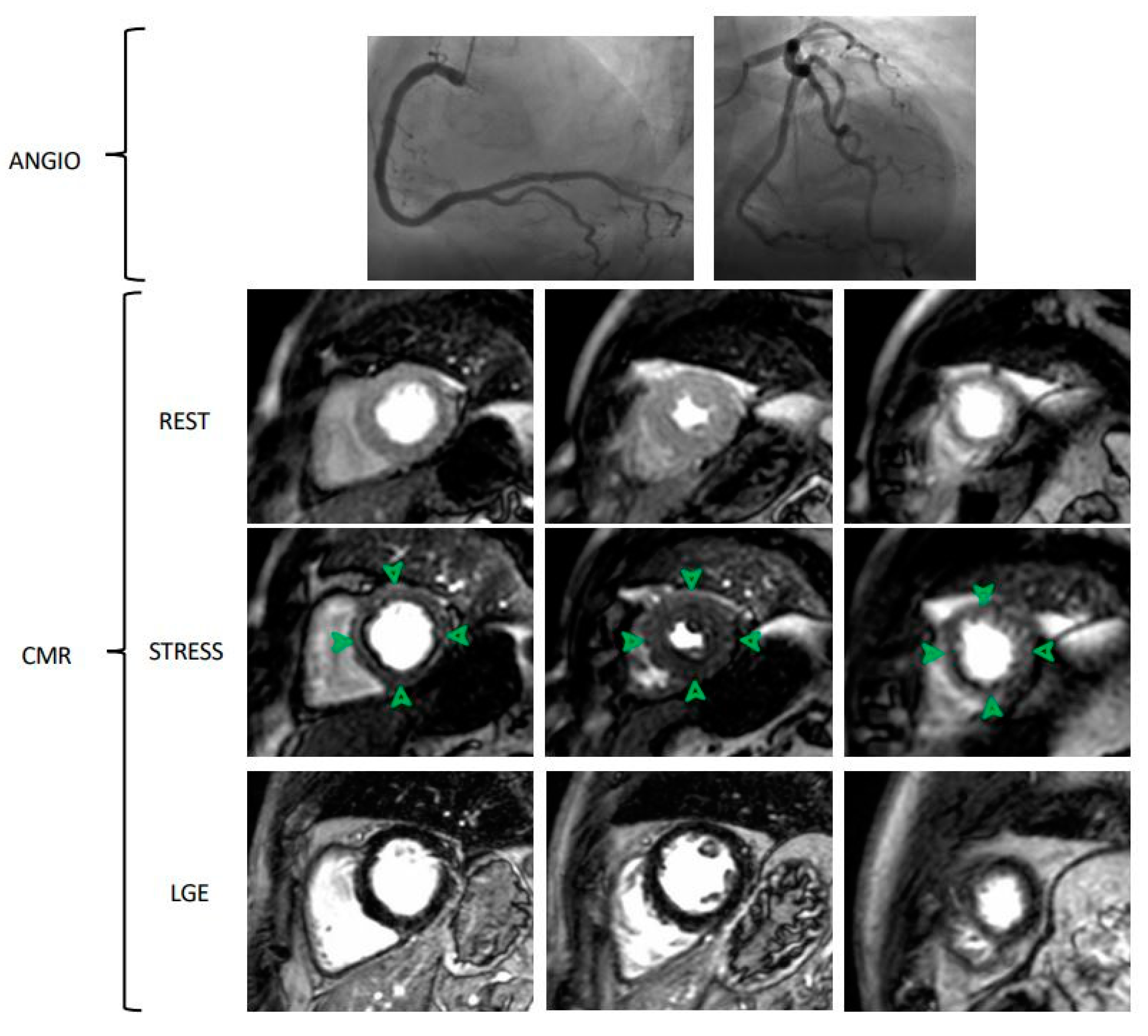
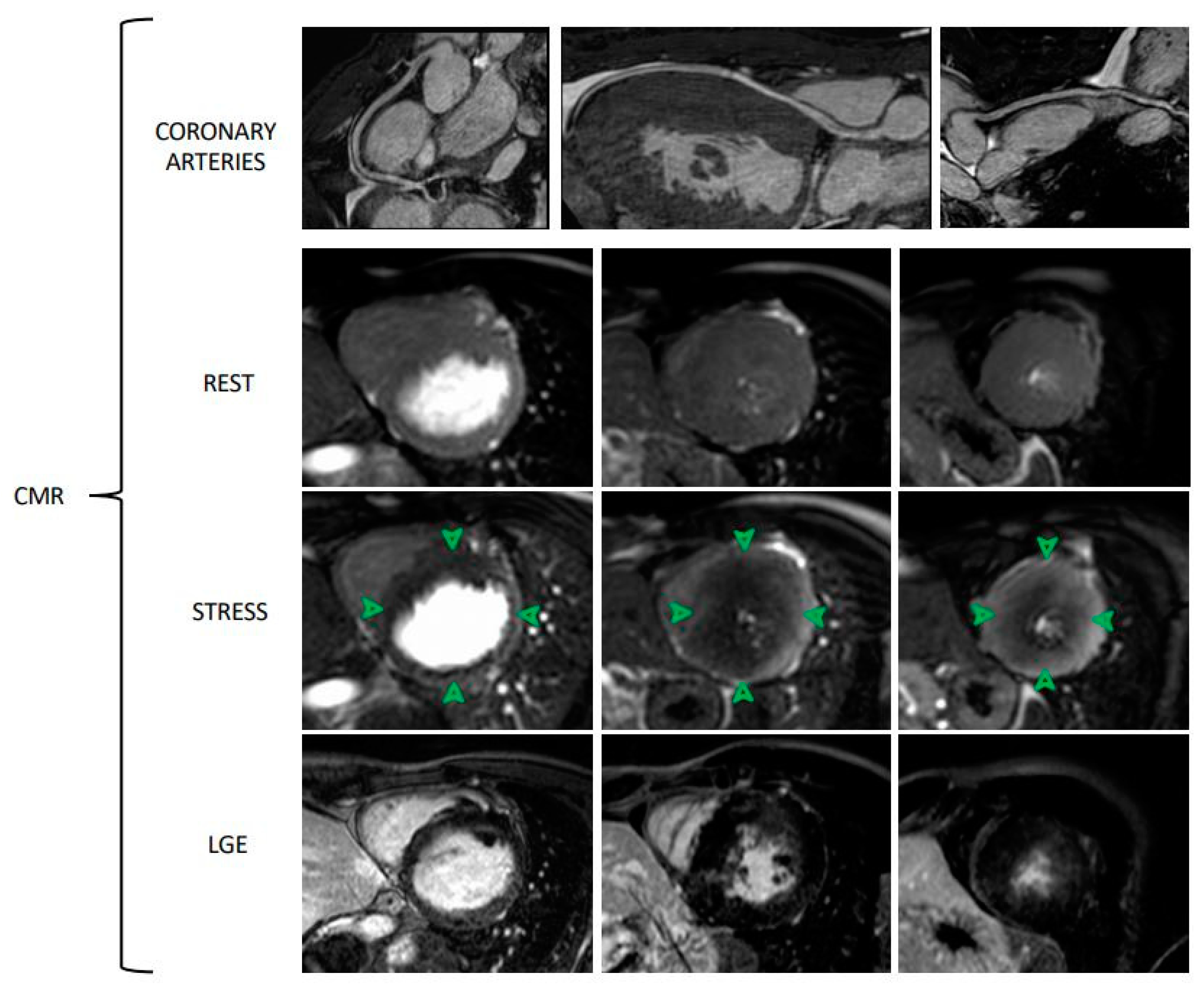
4. Cardiovascular MRI
5. Cardiac CT
- -
- Static CTP requires only a single image at peak myocardial contrast opacification, which is then compared with a single rest image. This technique requires prospective ECG triggering and is associated with a lower amount of radiation, but it allows only semiquantitative or qualitative perfusion evaluation;
- -
- Dynamic CTP obtains several sequential images over time from the first pass to the wash-out of contrast medium, allowing the calculation of the kinetics of iodinated contrast in the arterial blood pool and myocardium over time. As a consequence, a quantitative perfusion estimation is obtained. This method is related to quantifying MBF, but it requires a 3-fold higher radiation exposure than static CTP [43].
6. Limitations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, M.R.; Peterson, E.D.; Dai, D.; Brennan, J.M.; Redberg, R.F.; Anderson, H.V.; Brindis, R.G.; Douglas, P.S. Low diagnostic yelds of elective coronary angiography. N. Engl. J. Med. 2010, 362, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; López-Sendón, J.; Alexander, K.P.; et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef]
- Lu, D.Y.; Yalcin, H.; Yalcin, F.; Zhao, M.; Sivalokanathan, S.; Valenta, I.; Tahari, A.; Pomper, M.G.; Abraham, T.P.; Schindler, T.H.; et al. Stress Myocardial Blood Flow Heterogeneity is a Positron Emission Tomography Biomarjer of Ventricular Arrythmias in Patients with Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2018, 121, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Neglia, D.; Michelassi, C.; Trivieri, M.G.; Sambuceti, G.; Giorgetti, A.; Pratali, L.; Gallopin, M.; Salvadori, P.; Sorace, O.; Carpeggiani, C.; et al. Prognostic role of myocardial blood flow impairment in idiopathic left ventricular dysfunction. Circulation 2002, 105, 186–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
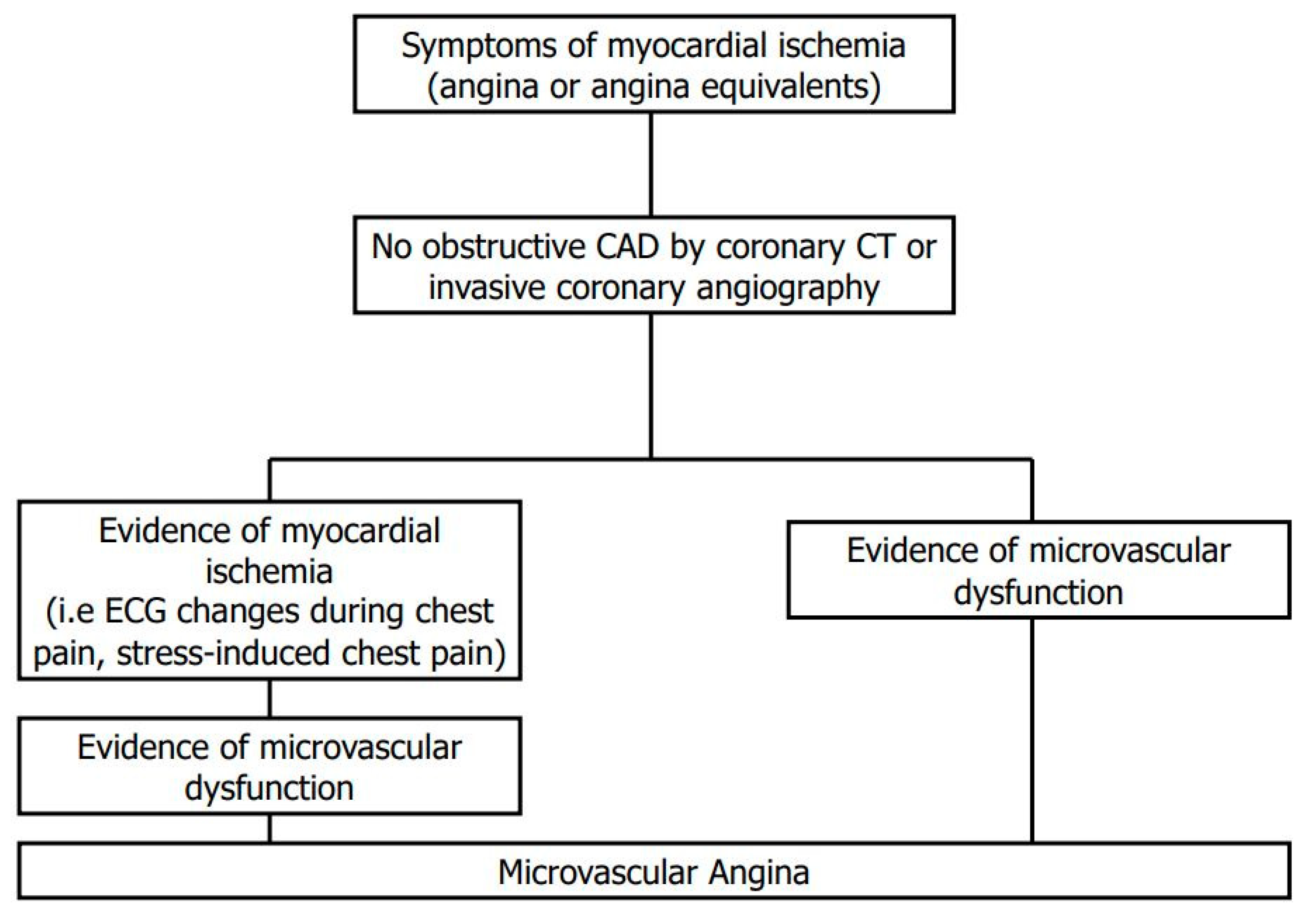
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Merz, C.N.B. International standardization of diagnostic criteria for microvascular angina. Int. J. Cardiol. 2018, 250, 16–20. [Google Scholar] [CrossRef]
- Camici, P.G.; Crea, F. Coronary Microvascular Dysfunction. N. Engl. J. Med. 2007, 356, 830–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recio-Mayoral, A.; Rimoldi, O.E.; Camici, P.G.; Kaski, J.C. Inflammation and Microvascular Dysfunction in Cardiac Syndrome X Patients Without Conventional Risk Factors for Coronary Artery Disease. JACC Cardiovasc. Imaging 2013, 6, 660–667. [Google Scholar] [CrossRef] [Green Version]
- Ford, T.J.; Stanley, B.; Good, R.; Ricchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson KHood, S.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J. Am. Coll. Cardiol. 2018, 72, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Schindler, T.H.; Zhang, X.L.; Vincenti, G.; Mhiri, L.; Nkoulou, R.; Just, H.; Ratib, O.; Mach, F.; Dahlbom, M.; Schelbert, H.R. Diagnostic value of PET-measured heterogeneity in myocardial blood flow during cold pressor testing for the identification of coronary vasomotor dysfunction. J. Nucl. Cardiol. 2007, 17, 688–697. [Google Scholar] [CrossRef] [Green Version]
- Di Carli, M.F.; Asgarzadie, F.; Schelbert, H.R.; Brunken, R.C.; Laks, H.; Phelps, M.E.; Maddahi, J. Quantitative relation Between Myocardial Viability and Improvement in Heart failure Symptoms After Revascularization in Patients with Ischemic cardiomyopathy. Circulation 1995, 92, 3436–3444. [Google Scholar] [CrossRef]
- Montecucco, F.; Carbone, F.; Schindler, T.H. Pathophysiology of ST-segment elevation myocardial infarction: Novel mechanisms and treatmens. Eur. Heart J. 2016, 37, 1268–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tebaldi, M.; Leone, A.M.; Biscaglia, S.; Di Cesare, A.; Erriquez, A.; Campo, G. Index of microcirculatory resistance assessment in patients with new diagnosis of left ventricular dilatation without significant coronary artery lesions: IMPAIRED pilot trial. Eur. J. Heart Fail. 2020, 22, 561–563. [Google Scholar] [CrossRef]
- Anagnostopoulos, C.; Georgakopoulos, A.; Pianou, N.; Nekolla, S.G. Assessment of myocardial perfusion and viability by Positron Emission Tomography. Int. J. Cardiol. 2013, 167, 1737–1749. [Google Scholar] [CrossRef]
- Bateman, T.M.; Dilsizian, V.; Beanlands, R.S.; Gordon DePuys, G.; Heller, G.V.; Wolinsky, D.A. American Society if Nuclear Cardiology and Society of Nuclear Medicine and Molecular Imaging Joint Position Statement on the Clinical Indications for Myocardial Perfusion PET. J. Nucl. Med. 2016, 57, 1654–1656. [Google Scholar] [CrossRef] [Green Version]
- Dilsizian, V.; Bacharach, S.L.; Beanlands, R.S.; Bergmann, S.R.; Delbeke, D.; Dorbala, S.; Gropler, R.J.; Knuuti, J.; Schelbert, H.R.; Travin, M.I. ASNC imaging guidelines/SNMMI procedure standard for positron emission tomography (PET) nuclear cardiology procedures. J. Nucl. Cardiol. 2016, 23, 1187–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinones, M.J.; Hernandez-Pampaloni, M.; Schelbert, H.; Bulnes-Enriquez, I.; Jimenez, K.; Hernandez, G.; De La Rosa, R.; Chon, Y.; Yang, H.; Nicholas, S.B.; et al. Coronary vasomotor abnormalities in insulin-resistant individuals. Ann. Intern. Med. 2004, 140, 700–708. [Google Scholar]
- Di Carli, M.F.; Charytan, D.; McMahon, G.T.; Ganz, P.; Dorbala, S.; Schelbert, H.R. Coronary circulatory function in patients with the metabolic syndrome. J. Nucl. Med. 2011, 52, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, I.; Momomura, S.I.; Ohtake, T.; Yonekura, K.; Nishikawa, J.; Sasaki, Y.; Omata, M. Reduced Myocardial Flow Reserve in Non-Insulin-Dependent Diabetes Mellitus. J. Am. Coll. Cardiol. 1997, 30, 1472–1477. [Google Scholar] [CrossRef] [Green Version]
- Taqueti, V.R.; Shaw, L.J.; Cook, N.R.; Murthy, V.L.; Shah, N.R.; Foster, C.R.; Hainer, J.; Blankstein, R.; Dorbala, S.; Di Carli, M.F. Excess Cardiovascular Risk in Women Relative to Men Referred for Coronary Angiography is Associated with Severely Impaired Coronary Flow Reserve, not Obstructive Disease. Circulation 2017, 135, 566–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taqueti, V.R.; Solomon, S.D.; Shah, A.M.; Desai, A.S.; Groarke, J.D.; Osborne, M.T.; Hainer, J.; Bibbo, C.F.; Dorbala, S.; Blankestein, R.; et al. Coronary microvascular dysfunction, and future risk of heart failure with preserved ejection fraction. Eur. Heart J. 2018, 39, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Bravo, P.E.; Pinheiro, A.; Higuchi, T.; Rischpler, C.; Merrill, J.; Santaularia-Tomas, M.; Abraham, R.; Wahl, R.L.; Abraham, T.P.; Bengel, F.M. PET/CT Assessment of Symptomatic Individuals with Obstructive and Nonobstructive Hypertrophic Cardiomyopathy. J. Nucl. Med. 2012, 53, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chih, S.; Chong, A.Y.; Erthal, F.; deKemp, R.A.; Davies, R.A.; Stadnick, E.; So, D.Y.; Overgaard, C.; Wells, G.; Mielniczuk, L.M.; et al. PET Assessment of Epicardial Intimal Disease and Microvascular Dysfunction in Cardiac Allograft Vasculopathy. J. Am. Coll. Cardiol. 2018, 71, 1444–1456. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.H.; Tahk, S.L.; Yang, H.M.; Woo, S.I.; Lim, H.S.; Kang, S.J.; Choi, B.J.; Choi, S.Y.; Hwang, G.S.; Shin, J.H. Comparison of accuracy in the prediction of left ventricular wall motion changes between invasively assessed microvascular integrity indexes and fluorine-18 fluorodeoxyglucose positron emission tomography in patients with ST-elevation myocardial infarction. Am. J. Cardiol. 2008, 102, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Hwang, D.; Park, J.; Tong, Y.; Koo, B.K. Physiologic mechanism of discordance between instantaneous wave-free ratio and fractional flow reserve: Insight from 13N-ammonium positron emission tomography. Int. J. Cardiol. 2017, 243, 91–94. [Google Scholar] [CrossRef]
- Schepis, T.; Gaemperli, O.; Treyer, V.; Valenta, I.; Burger, C.; Koepfli, P.; Namdar, M.; Adachi, I.; Alkadhi, H.; Kaufmann, P.A. Absolute quantification of myocardial blood flow with 12N-ammonia and 3-dimensional PET. J. Nucl. Med. 2007, 48, 1783–1789. [Google Scholar] [CrossRef] [Green Version]
- Des Prez, R.D.; Shaw, L.L.; Gillespie, R.L.; Jaber, W.A.; Noble, W.A.; Soman, P.; Wolinsky, D.G.; Williams, K.A. Cost-effectiveness of myocardial perfusion imaging: A summary of currently available literature. J. Nucl. Cardiol. 2005, 12, 750–759. [Google Scholar] [CrossRef]
- Al-Saadi, N.; Nagel, E.; Gross, M.; Bornstedt, A.; Schnackenburg, B.; Klein, C.; Klimek, W.; Oswald, H.; Fleck, E. Noninvasive Detection of Myocardial Ischemia from Perfusion Reserve Based on Cardiovascular Magnetic Resonance. Circulation 2000, 101, 1379–1383. [Google Scholar] [CrossRef] [Green Version]
- Larghat, A.M.; Maredia, N.; Biglands, J.; Greenwood, J.P.; Ball, S.G.; Jerosch-Herold, M.; Radjenovic, A.; Plein, S. Reproducibility of first-pass cardiovascular magnetic resonance myocardial perfusion. J. Magn. Reson. Imaging 2013, 37, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Utz, W.; Niendorf, T.; Wassmuth, R.; Messroghli, D.; Dietz, R.; Schulz-Menger, J. Contrast-dose relation in first-pass myocardial MR perfusion imaging. J. Magn. Reson. Imaging 2007, 25, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Christian, T.F.; Rettmann, D.W.; Aletras, A.H.; Liao, S.L.; Taylor, J.L.; Balaban, R.S.; Arai, A.E. Absolute myocardial perfusion in canines measured by using dual-bolus first-pass MR imaging. Radiology 2004, 232, 677–684. [Google Scholar] [CrossRef]
- Schuster, A.; Zarinabad, N.; Ishida, M.; Sinclair, M.; van den Wijngaard, J.P.H.M.; Morton, G.; Hautvast, G.L.T.F.; Bigalke, B.; van Horssen, P.; Smith, N.; et al. Quantitative assessment of magnetic resonance derived myocardial perfusion measurements using advanced techniques: Microsphere validation in an explanted pig heart system. J. Cardiovasc. Magn. Reson. 2014, 16, 82. [Google Scholar] [CrossRef] [Green Version]
- Engblom, H.; Xue, H.; Akil, S.; Carlsson, M.; Hindorf, C.; Oddstig, J.; Hedeer, F.; Hansen, M.S.; Aletras, A.H.; Kellman, P.; et al. Fully quantitative cardiovascular magnetic resonance myocardial perfusion ready for clinical use: A comparison between cardiovascular magnetic resonance imaging and positron emission tomography. J. Cardiovasc. Magn. Reson. 2017, 19, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mygind, N.D.; Pena, A.; Michelsen, M.M.; Qayyum, A.A.; Frestad, D.; Christensen, T.E.; Ghotbi, A.A.; Hasbak, P.; Kjaer, A.; Vejlstrup, N.; et al. Myocardial first pass perfusion assessed by cardiac magnetic resonance and coronary microvascular dysfunction in women with angina and no obstructive coronary artery disease. J. Clin. Lab. Investig. 2019, 79, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Wohrle, J.; Nusser, T.; Merkle, N.; Kestler, H.A.; Grebe, O.C.; Marx, N.; Hoher, M.; Kochs, M.; Hombach, V. Myocardial perfusion reserve in cardiovascular magnetic resonance: Correlation to coronary microvascular dysfunction. J. Cardiovasc. Magn. Reson. 2006, 8, 781–787. [Google Scholar] [CrossRef]
- Kotecha, T.; Martinez-Naharro, A.; Boldrini, M.; Knight, D.; Hawkins, P.; Kalra, S.; Patel, D.; Coghlan, G.; Moon, J.; Plein, S.; et al. Automated Pixel-Wise Quantitative Myocardial Perfusion Mapping by CMR to Detect Obstructive Coronary Artery Disease and Coronary Microvascular Dysfunction: Validation Against Invasive Coronary Physiology. JACC Cardiovasc. Imaging 2019, 12, 1958–1969. [Google Scholar] [CrossRef]
- Tonet, E.; Baggiano, A.; Pavasini, R.; Guglielmo, M.; Censi, S.; Cossu, A.; Rapezzi, C.; Muscogiuri, G.; Squeri, A.; Campo, G.; et al. Current evidence on the diagnostic and prognostic role of native T1 mapping in heart diseases. Trends Cardiovasc. Med. 2020. [Google Scholar] [CrossRef]
- Levelt, E.; Piechnik, S.K.; Liu, A.; Wijesurendra, R.S.; Mahmod, M.; Ariga, R.; Francis, J.M.; Greiser, A.; Clarke, K.; Neubauer, S.; et al. Adenosine stress CMR T1-mapping detects early microvascular dysfunction in patients with type 2 diabetes mellitus without obstructive coronary artery disease. J. Cardiovasc. Magn. Reson. Imaging 2017, 19, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmod, M.; Piechnik, S.K.; Levelt, E.; Ferreira, V.M.; Francis, J.M.; Lewis, A.; Pal, N.; Dass, S.; Ashrafian, H.; Neubauer, S.; et al. Adenosine stress native T1 mapping in severe aortic stenosis: Evidence for a role of the intravascular compartment on myocardial T1 values. Cardiovasc. Magn. Res. 2014, 16, 92. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Lee, J.C.Y.; Leung, S.T.; Lai, A.; Lee, T.F.; Chiang, J.B.; Cheng, Y.W.; Chan, H.L.; Yiu, K.H.; Goh, V.K.M.; et al. Long-Term Prognosis of Patients with Coronary Microvascular Disease Using Stress Perfusion Cardiac Magnetic Resonance. JACC Cardiovasc. Imaging 2021, 14, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Chiribiri, A.; Botnar, R.M.; Nagel, E. Magnetic resonance Coronary Angiography: Where Are We Today? Curr. Cardiol. Rep. 2013, 15, 328. [Google Scholar] [CrossRef] [Green Version]
- Baessato, F.; Guglielmo, M.; Muscogiuri, G.; Baggiano, A.; Fusini, L.; Scafuri, S.; Babbaro, M.; Mollace, R.; Collevecchio, A.; Guaricci, A.I.; et al. The Incremental Role of Coronary Computed Tomography in Chronic Coronary Syndromes. J. Clin. Med. 2020, 9, 3925. [Google Scholar] [CrossRef]
- Baggiano, A.; Fusini, L.; Del Torto, A.; Vivona, P.; Guglielmo, M.; Muscogiuri, G.; Soldi, M.; Martini, C.; Fraschini, E.; Rabbat, M.G.; et al. Sequential Strategy Including FFR CT Plus Stress-CTP Impacts on Management of Patients with Stable Chest Pain: The Stress-CTP RIPCORD Study. J. Clin. Med. 2020, 9, 2147. [Google Scholar] [CrossRef]
- Branch, K.R.; Haley, R.D.; Bittencourt, M.S.; Patel, A.R.; Hulten, E.; Blankestein, R. Myocardial computed tomography perfusion. Cardiovasc. Diagn. Ther. 2017, 7, 452–462. [Google Scholar] [CrossRef] [Green Version]
- Kuhl, J.T.; George, R.T.; Mehra, V.C.; Linde, J.J.; Chen, M.; Arai, A.E.; Di Carli, M.; Kitagawa, K.; Dewey, M.; Lima, J.A.C.; et al. Endocardial-epicardial distribution of myocardial perfusion reserve assessed by multidetector compjted tomograpy in symptomatic patients without significant coronary artery disease: Insight from the CORE320 multicentre study. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 779–787. [Google Scholar] [CrossRef] [Green Version]
- George, R.T.; Jerosh-Herold, M.; Silva, C.; Kitagawa, K.; Bluemke, D.A.; Lima, J.A.C.; Lardo, A.C. Quantification of myocardial perfusion using dynamic 64-detector computed tomography. Investig. Radiol. 2007, 42, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Bamberg, F.; Hinkel, R.; Marcus, R.P.; Baloch, E.; Hildebrandt, K.; Schwarz, F.; Hetterich, H.; Sadner, T.A.; Schlett, C.L.; Ebersberger, U.; et al. Feasibility of dynamic CT-based adenosine stress myocardial perfusion imaging to detect and differentiate ischemic and infarcted myocardium in a large experimental porcine animal model. Int. J. Cardiovasc. Imaging 2014, 30, 803–812. [Google Scholar] [CrossRef]
- Alessio, A.M.; Bindschadler, M.; Busey, J.M.; Shuman, W.P.; Caldwell, J.H.; Branch, K.R. Accuracy of Myocardial Blood Flow Estimation from Dynamic Contrast-Enhanced Cardiac CT Compared with PET. Circ. Cardiovasc. Imaging 2019, 12, e008323. [Google Scholar] [CrossRef] [PubMed]
- Bairey, M.C.N.; Pepine, C.J.; Shimokawa, H.; Berry, C. Treatment of coronary microvascular dysfunction. Eur. Heart J. Cardiovasc. Res. 2020, 116, 856–870. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Scenario | Patophysiology | PET | CMR | CT |
|---|---|---|---|---|
| MVD without obstructive CAD or myocardial diseases | Cardiovascular risk factors, such as hypertension and diabetes, determine endothelial dysfunction and abnormal function of vascular smooth muscle cells. | The most tested in this setting with a prognostic role | Tested in this setting | Contemporary assessment of epicardial vessels and MVD |
| MVD in the presence of obstructive CAD | Stable CAD: atherosclerotic involvement of microcirculation and endothelial dysfunction. Acute coronary syndrome: microvascular obstruction due to edema, hemorrhage and inflammation. | Tested in this setting | Tested in this setting and useful for tissue characterization | Contemporary assessment of epicardial vessels and MVD |
| MVD in the presence of myocardial or severe valvular diseases | Structural alterations (i.e., hypertrophy or interstitial fibrosis) determine capillary rarefaction and increase arterial stiffness. | The most tested in this setting | Tested in this setting and useful for tissue characterization and valvular diseases estimation | Not tested and limited usefulness in this setting |
| Radiotracer | Half-Life | Advantages | Disadvantages |
|---|---|---|---|
| 15O-water | 120 s | -High myocardial extraction fraction | -Limited application to facilities with an on-site cyclotron |
| 82Rubidium | 76 s | -Not requiring a cyclotron on site | -Significant roll-off at high flows -Low myocardial extraction fraction |
| 13N-ammonia | 10 min | -High myocardial extraction fraction | -Requiring a cyclotron on site |
| 18F-labeled agents | variable | -Flow-independent high extraction fraction (>90%) | -Alterations in the metabolic state of the myocardium may affect its retention -Current use only in investigational trials |
| Modality | Protocol | Pros | Cons |
|---|---|---|---|
| PET | Vasodilator stress and rest perfusion images | -Most validated technique -Prognostic values -Good reproducibility -Not limited by renal function | -High costs -Radiation exposure -Limited availability -Time consuming procedure |
| CMR | Vasodilator stress and rest perfusion images | -High spatial resolution -Tissue characterization -No radiation -Validated and compared with PET and invasive methods -Anatomic evaluation of epicardial coronary vessels (limited data) | -High costs -Limited by renal function -Limited availability -Poor prognostic data -Time consuming |
| CT | Vasodilator stress and rest perfusion images | Anatomic and functional data in the same study | -Limited availability -Limited by renal function -Radiation exposure -Risk of MBF overestimation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tonet, E.; Pompei, G.; Faragasso, E.; Cossu, A.; Pavasini, R.; Passarini, G.; Tebaldi, M.; Campo, G. Coronary Microvascular Dysfunction: PET, CMR and CT Assessment. J. Clin. Med. 2021, 10, 1848. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10091848
Tonet E, Pompei G, Faragasso E, Cossu A, Pavasini R, Passarini G, Tebaldi M, Campo G. Coronary Microvascular Dysfunction: PET, CMR and CT Assessment. Journal of Clinical Medicine. 2021; 10(9):1848. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10091848
Chicago/Turabian StyleTonet, Elisabetta, Graziella Pompei, Evelina Faragasso, Alberto Cossu, Rita Pavasini, Giulia Passarini, Matteo Tebaldi, and Gianluca Campo. 2021. "Coronary Microvascular Dysfunction: PET, CMR and CT Assessment" Journal of Clinical Medicine 10, no. 9: 1848. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10091848