
Validation of Noninvasive Remote Dielectric Sensing System to Quantify Lung Fluid Levels

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Participant Selection
2.2. ReDS System
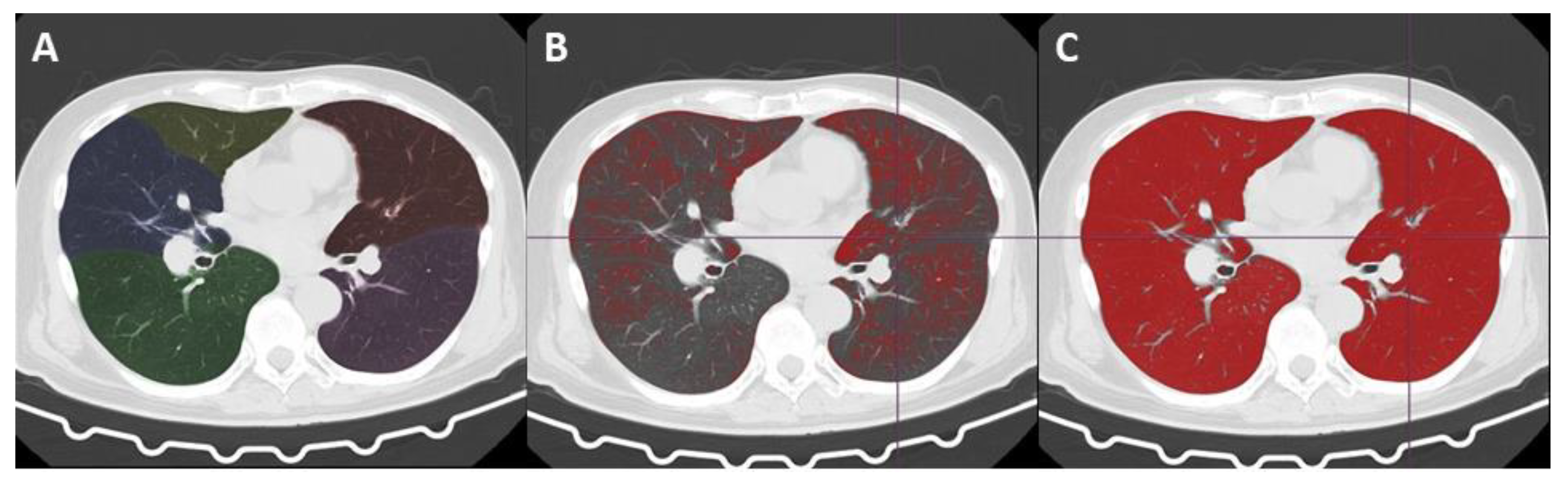
2.3. CT Image Acquisition
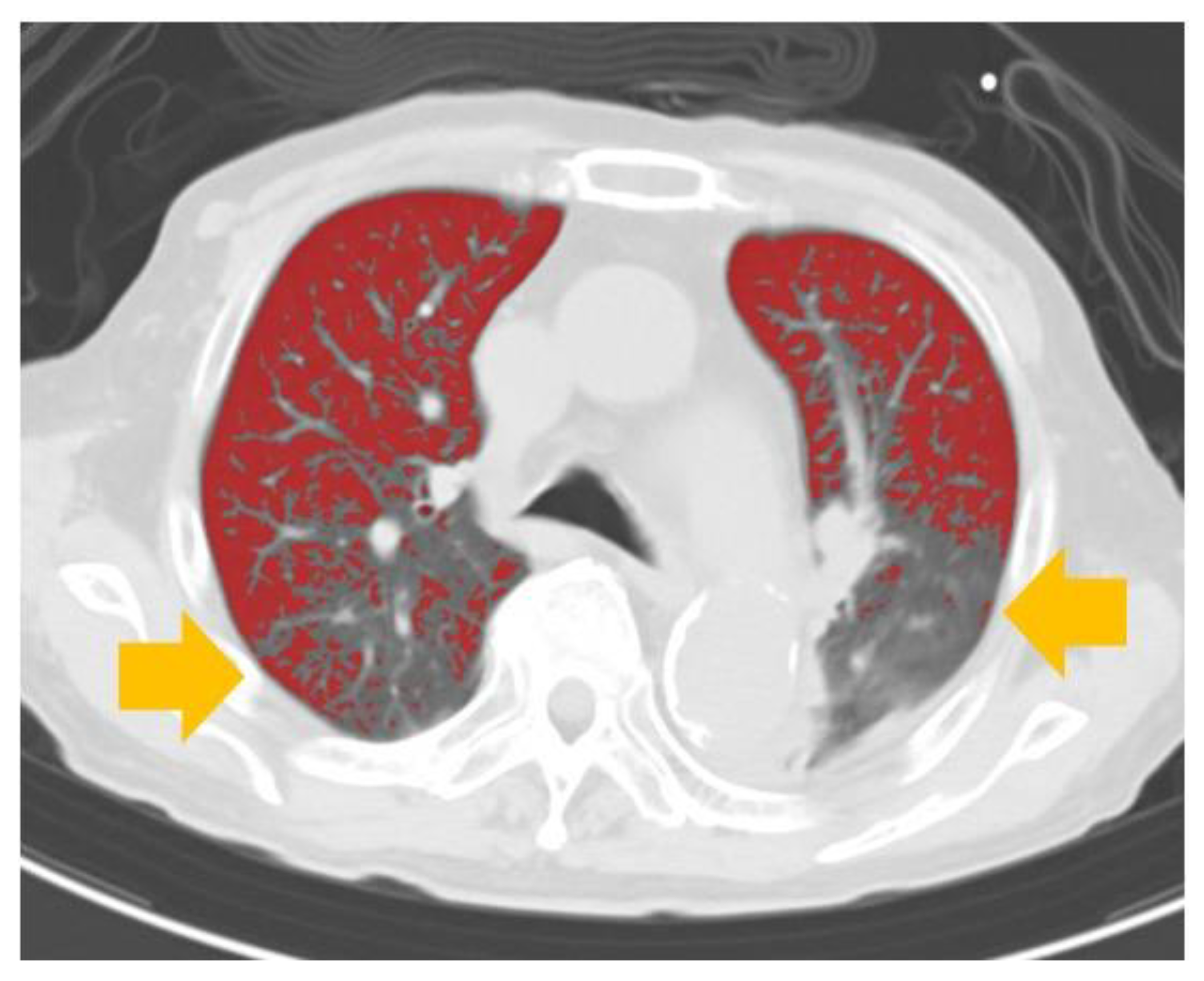
Automated Volume Analysis of the CT Images
2.4. Statistical Methods
3. Results
3.1. Baseline Characteristics
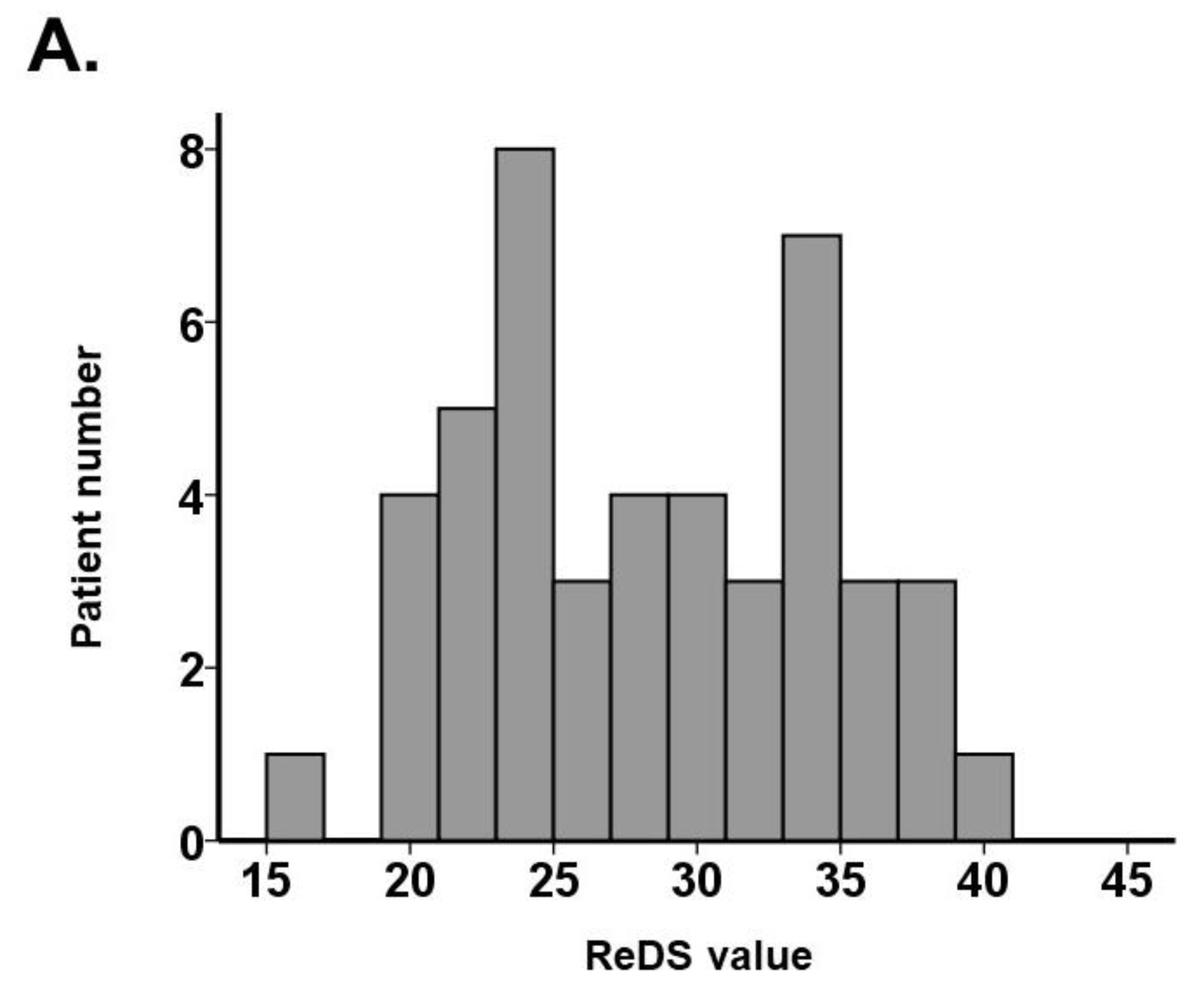
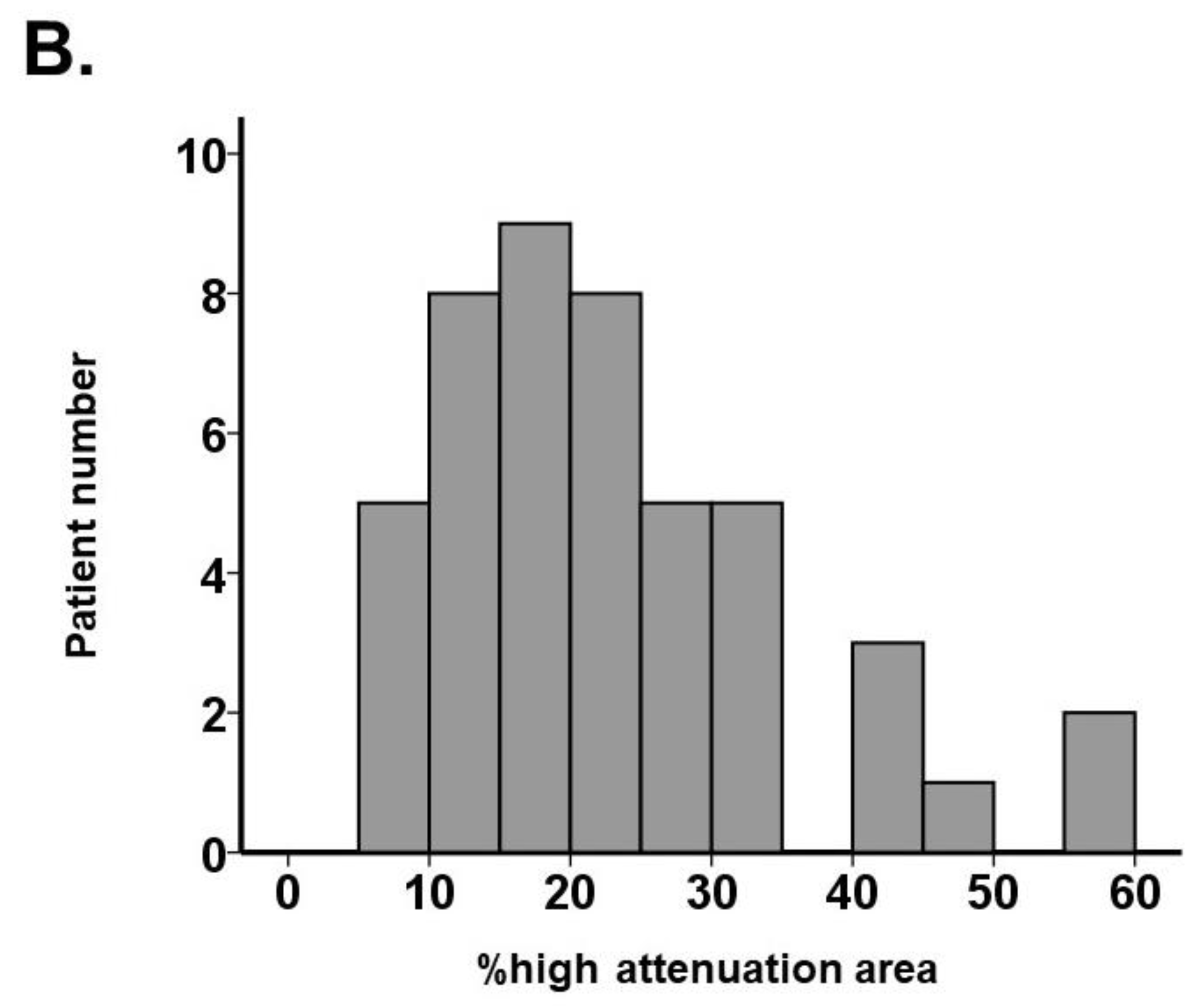
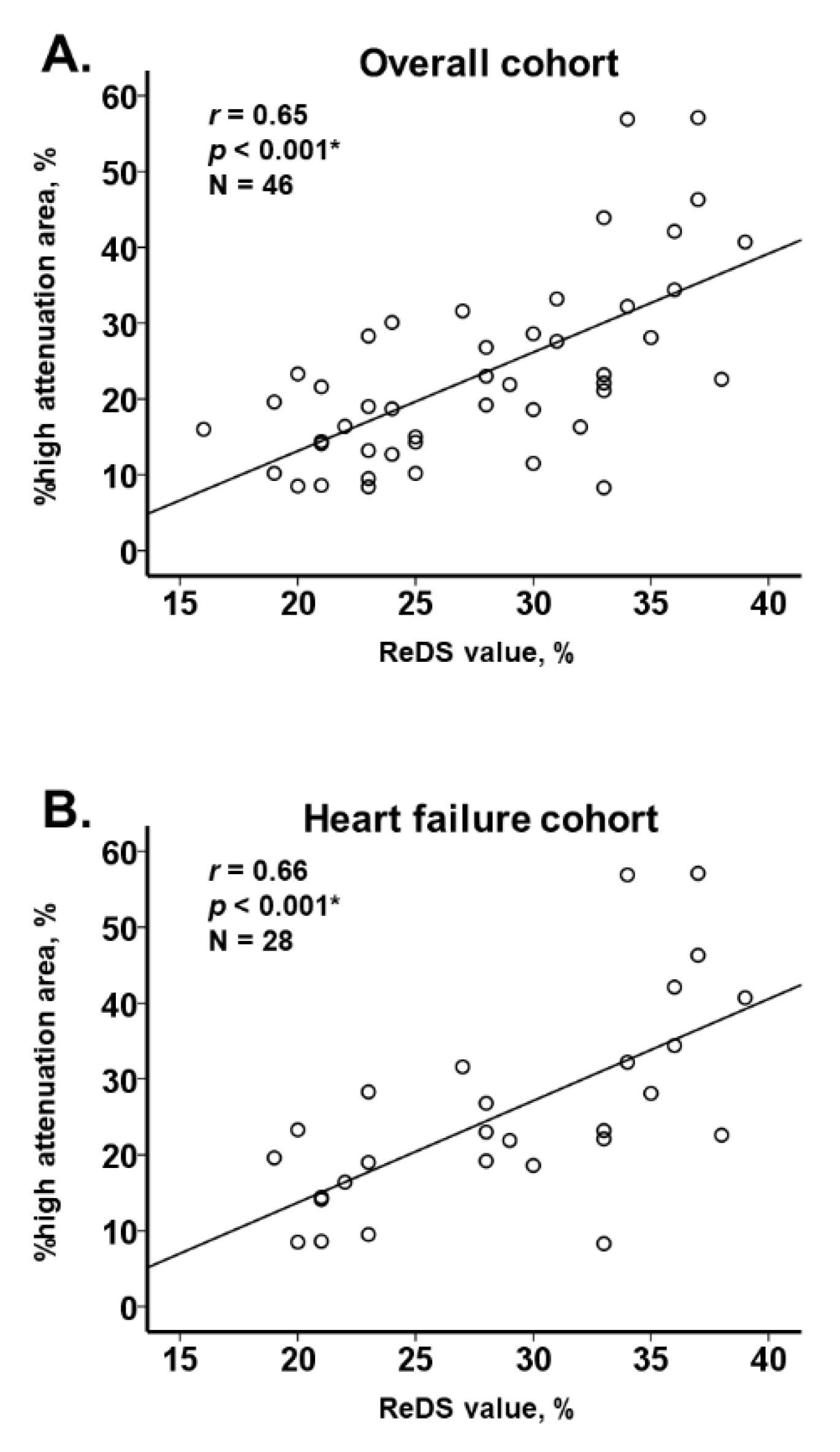
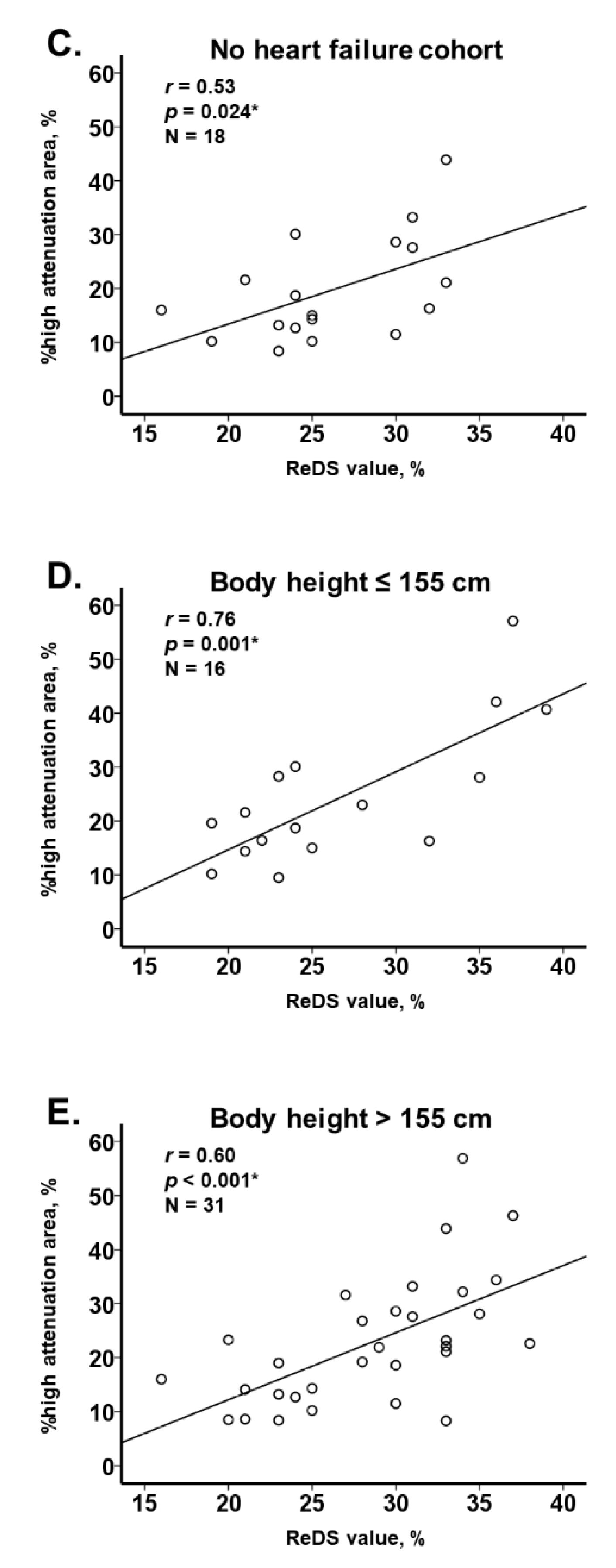
3.2. ReDS Value and %High Attenuation Area
4. Discussion
4.1. Conventional Methodologies to Assess Pulmonary Congestion
4.2. ReDS versus Invasive Hemodynamic Measurement
4.3. ReDS System and Chest CT
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vaduganathan, M.; Claggett, B.L.; Jhund, P.S.; Cunningham, J.W.; Pedro Ferreira, J.; Zannad, F.; Packer, M.; Fonarow, G.C.; McMurray, J.J.V.; Solomon, S.D. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: A comparative analysis of three randomised controlled trials. Lancet 2020, 396, 121–128. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Shah, A.M.; Borlaug, B.A. Heart Failure With Preserved Ejection Fraction In Perspective. Cir. Res. 2019, 124, 1598–1617. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Bohm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Girerd, N.; Seronde, M.F.; Coiro, S.; Chouihed, T.; Bilbault, P.; Braun, F.; Kenizou, D.; Maillier, B.; Nazeyrollas, P.; Roul, G.; et al. Integrative Assessment of Congestion in Heart Failure Throughout the Patient Journey. JACC Heart Fail. 2018, 6, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Amir, O.; Rappaport, D.; Zafrir, B.; Abraham, W.T. A novel approach to monitoring pulmonary congestion in heart failure: Initial animal and clinical experiences using remote dielectric sensing technology. Congest. Heart Fail. 2013, 19, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Amir, O.; Azzam, Z.S.; Gaspar, T.; Faranesh-Abboud, S.; Andria, N.; Burkhoff, D.; Abbo, A.; Abraham, W.T. Validation of remote dielectric sensing (ReDS) technology for quantification of lung fluid status: Comparison to high resolution chest computed tomography in patients with and without acute heart failure. Int. J. Cardiol. 2016, 221, 841–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amir, O.; Ben-Gal, T.; Weinstein, J.M.; Schliamser, J.; Burkhoff, D.; Abbo, A.; Abraham, W.T. Evaluation of remote dielectric sensing (ReDS) technology-guided therapy for decreasing heart failure re-hospitalizations. Int. J. Cardiol. 2017, 240, 279–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lala, A.; Barghash, M.H.; Giustino, G.; Alvarez-Garcia, J.; Konje, S.; Parikh, A.; Ullman, J.; Keith, B.; Donehey, J.; Mitter, S.S.; et al. Early use of remote dielectric sensing after hospitalization to reduce heart failure readmissions. ESC Heart Fail. 2021, 8, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Iwano, S.; Hashimoto, N.; Matsuo, K.; Hasegawa, Y.; Naganawa, S. Lobar analysis of collapsibility indices to assess functional lung volumes in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 1347–1356. [Google Scholar] [CrossRef] [Green Version]
- Iwano, S.; Kitano, M.; Matsuo, K.; Kawakami, K.; Koike, W.; Kishimoto, M.; Inoue, T.; Li, Y.; Naganawa, S. Pulmonary lobar volumetry using novel volumetric computer-aided diagnosis and computed tomography. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crossley, D.; Renton, M.; Khan, M.; Low, E.V.; Turner, A.M. CT densitometry in emphysema: A systematic review of its clinical utility. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 547–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabuuchi, H.; Matsuo, Y.; Tsukamoto, H.; Horiuchi, T.; Sunami, S.; Kamitani, T.; Jinnouchi, M.; Nagao, M.; Akashi, K.; Honda, H. Evaluation of the extent of ground-glass opacity on high-resolution CT in patients with interstitial pneumonia associated with systemic sclerosis: Comparison between quantitative and qualitative analysis. Clin. Radiol. 2014, 69, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Li, Y.; Pang, S.; Wan, H.; Shi, G.; Cheng, Q.; Li, Q.; Pan, Z.; Huang, S. Normal lung attenuation distribution and lung volume on computed tomography in a Chinese population. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1657–1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattinoni, L.; Caironi, P.; Pelosi, P.; Goodman, L.R. What has computed tomography taught us about the acute respiratory distress syndrome? Am. J. Respir. Crit. Care Med. 2001, 164, 1701–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barile, M.; Hida, T.; Hammer, M.; Hatabu, H. Simple quantitative chest CT for pulmonary edema. Eur. J. Radiol. Open 2020, 7, 100273. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Nakamoto, T.; Iizuka, M. Early diagnosis and estimation of pulmonary congestion and edema in patients with left-sided heart diseases from histogram of pulmonary CT number. Chest 1996, 109, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Narang, N.; Chung, B.; Nguyen, A.; Kalathiya, R.J.; Laffin, L.J.; Holzhauser, L.; Ebong, I.A.; Besser, S.A.; Imamura, T.; Smith, B.A.; et al. Discordance Between Clinical Assessment and Invasive Hemodynamics in Patients With Advanced Heart Failure. J. Card. Fail. 2020, 26, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Goetze, J.P.; Bruneau, B.G.; Ramos, H.R.; Ogawa, T.; de Bold, M.K.; de Bold, A.J. Cardiac natriuretic peptides. Nat. Rev. Cardiol. 2020, 17, 698–717. [Google Scholar] [CrossRef] [PubMed]
- Callan, P.; Clark, A.L. Right heart catheterisation: Indications and interpretation. Heart 2016, 102, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Sayer, G.; Imamura, T.; Rodgers, D.; Kim, G.; Raikhelkar, J.; Sarswat, N.; Kalantari, S.; Chung, B.; Nguyen, A.; et al. Relationship Between Noninvasive Assessment of Lung Fluid Volume and Invasively Measured Cardiac Hemodynamics. J. Am. Heart Assoc. 2018, 7, e009175. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 46) | Heart Failure (N = 28) | Nonheart Failure (N = 18) | p Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 76 (73, 84) | 75 (72, 81) | 79 (74, 86) | 0.86 |
| Men | 28 (61%) | 16 (57%) | 12 (67%) | 0.37 |
| Body height, cm | 159 (150, 167) | 161 (151, 168) | 157 (149, 166) | 0.45 |
| Body mass index, kg/m2 | 21.6 (19.7, 26.0) | 20.8 (19.4, 23.9) | 23.8 (21.5, 26.7) | 0.087 |
| Comorbidity | ||||
| Hypertension | 33 (72%) | 23 (82%) | 10 (56%) | 0.054 |
| Dyslipidemia | 26 (57%) | 17 (61%) | 9 (50%) | 0.34 |
| Diabetes mellitus | 19 (41%) | 12 (43%) | 7 (39%) | 0.52 |
| Chronic kidney disease | 24 (52%) | 14 (50%) | 10 (56%) | 0.47 |
| History of stroke | 8 (17%) | 5 (18%) | 3 (17%) | 0.92 |
| Coronary heart disease | 7 (15%) | 2 (7%) | 5 (28%) | 0.057 |
| Atrial fibrillation | 9 (20%) | 7 (25%) | 2 (11%) | 0.25 |
| Echocardiography | ||||
| Left atrial diameter, mm | 41 (36, 46) | 40 (33, 46) | 43 (41, 46) | 0.29 |
| Left ventricular end-diastolic diameter, mm | 48 (45, 55) | 51 (46, 56) | 46 (43, 49) | 0.010 * |
| Left ventricular ejection fraction, % | 55 (47, 67) | 51 (38, 59) | 67 (58, 75) | <0.001 * |
| Mild or greater aortic regurgitation | 14 (30%) | 11 (39%) | 3 (17%) | 0.095 |
| Mild or greater mitral regurgitation | 23 (50%) | 17 (61%) | 6 (33%) | 0.065 |
| Mild or greater tricuspid regurgitation | 20 (43%) | 13 (46%) | 7 (39%) | 0.42 |
| Laboratory data | ||||
| Hemoglobin, g/dL | 11.9 (10.3, 13.4) | 11.9 (10.8, 13.1) | 11.9 (10.0, 14.4) | 0.41 |
| Serum albumin, g/dL | 3.6 (3.1, 3.9) | 3.6 (3.3, 4.0) | 3.6 (2.8, 3.9) | 0.63 |
| Serum sodium, mEq/L | 139 (137, 142) | 140 (138, 142) | 139 (137, 141) | 0.42 |
| eGFR, mL/min/1.73 m2 | 47.1 (31.1, 63.2) | 47.5 (29.3, 63.2) | 45.1 (31.1, 63.0) | 0.61 |
| Plasma B-type natriuretic peptide, pg/mL | 207 (53, 501) | 398 (179, 834) | 42 (16, 152) | <0.001 * |
| Medication | ||||
| Beta-blocker | 19 (41%) | 14 (50%) | 5 (28%) | 0.12 |
| Renin-angiotensin system inhibitor | 24 (52%) | 18 (64%) | 6 (33%) | 0.040 * |
| Mineralocorticoid receptor antagonist | 10 (22%) | 6 (21%) | 4 (22%) | 0.61 |
| Loop diuretics | 14 (32%) | 8 (29%) | 6 (33%) | 0.49 |
| ReDS value, % | 28 (23, 33) | 28 (23, 34) | 25 (24, 31) | 0.21 |
| %high attenuation area, % | 21.6 (14.4, 28.5) | 22.6 (17.5, 30.0) | 17.5 (12.1, 28.1) | 0.10 |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Beta Value | p Value | Beta Value | p Value | VIF | |
| Age, years | 0.168 | 0.24 | |||
| Body mass index, kg/m2 | −0.557 | 0.23 | −0.461 | 0.19 | 1.050 |
| Left ventricular ejection fraction, % | −0.127 | 0.22 | |||
| Mild or greater mitral regurgitation | 4.191 | 0.25 | |||
| Serum albumin, g/dL | −3.855 | 0.15 | |||
| eGFR, mL/min/1.73 m2 | −0.055 | 0.48 | |||
| Plasma B-type natriuretic peptide, pg/mL | 0.007 | 0.007 * | 0.004 | 0.12 | 1.147 |
| ReDS value, % | 1.301 | <0.001 * | 1.196 | <0.001 * | 1.098 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, T.; Gonoi, W.; Hori, M.; Ueno, Y.; Narang, N.; Onoda, H.; Tanaka, S.; Nakamura, M.; Kataoka, N.; Ushijima, R.; et al. Validation of Noninvasive Remote Dielectric Sensing System to Quantify Lung Fluid Levels. J. Clin. Med. 2022, 11, 164. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010164
Imamura T, Gonoi W, Hori M, Ueno Y, Narang N, Onoda H, Tanaka S, Nakamura M, Kataoka N, Ushijima R, et al. Validation of Noninvasive Remote Dielectric Sensing System to Quantify Lung Fluid Levels. Journal of Clinical Medicine. 2022; 11(1):164. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010164
Chicago/Turabian StyleImamura, Teruhiko, Wataru Gonoi, Masakazu Hori, Yohei Ueno, Nikhil Narang, Hiroshi Onoda, Shuhei Tanaka, Makiko Nakamura, Naoya Kataoka, Ryuichi Ushijima, and et al. 2022. "Validation of Noninvasive Remote Dielectric Sensing System to Quantify Lung Fluid Levels" Journal of Clinical Medicine 11, no. 1: 164. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010164