
Relationship between Depressive Symptoms, Personality, and Binge Drinking among University Students in Spain

 ,
,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
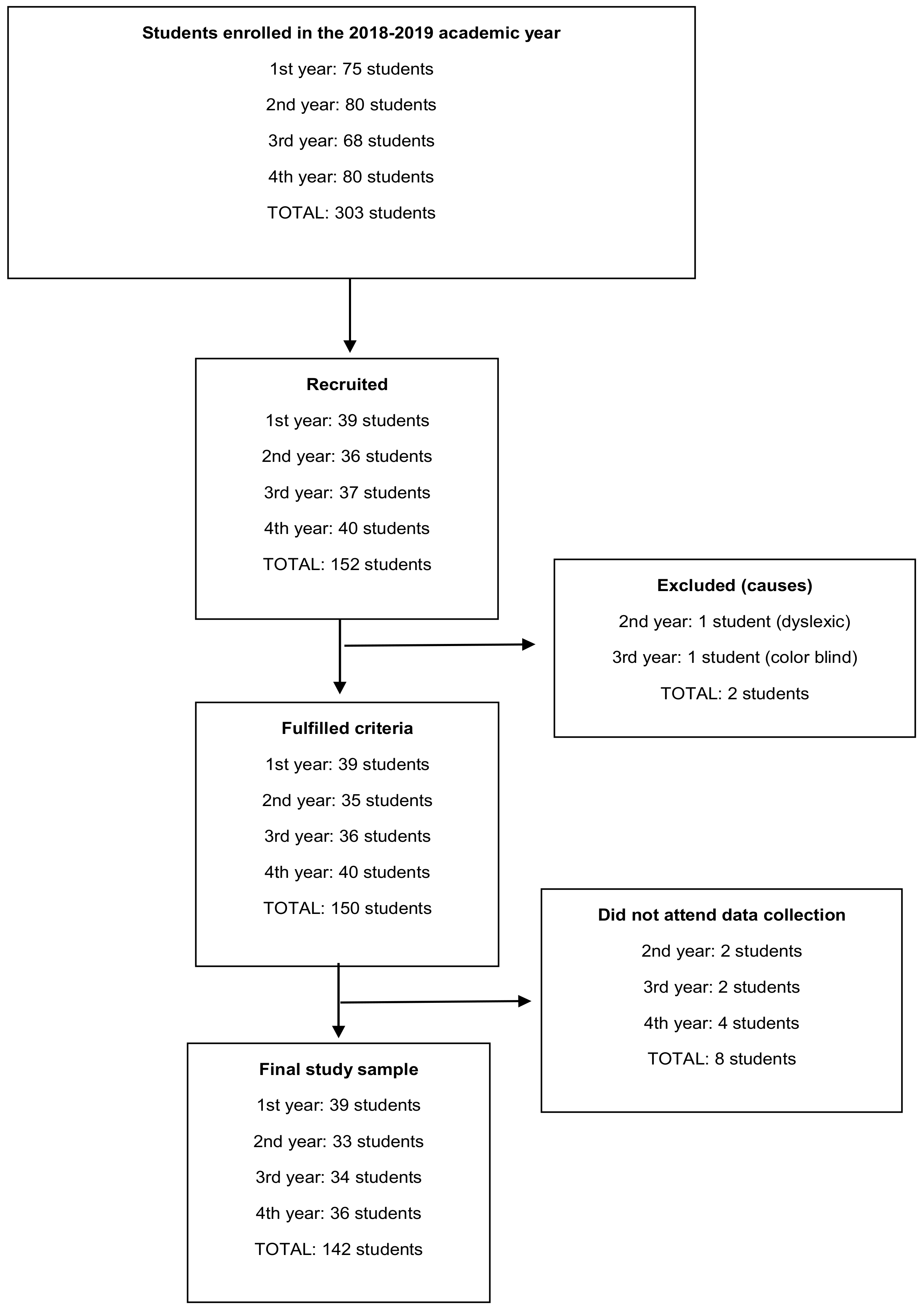
2.2. Participants
2.3. Variables and Measurement Tools
2.3.1. Sociodemographic, Academic, and Alcohol and Other Drug Consumption Variables
2.3.2. Depressive Symptoms
2.3.3. Personality
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic, Academic, Alcohol, and Other Drug Use Variables
3.2. Depressive Symptoms
3.3. Personality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-156563-9.
- Observatorio Español de las Drogas y las Adicciones. Informe 2019 Alcohol, Tabaco y Drogas Ilegales en España; Ministerio de Sanidad, Consumo y Bienestar Social: Madrid, Spain, 2019.
- Crews, F.; He, J.; Hodge, C. Adolescent Cortical Development: A Critical Period of Vulnerability for Addiction. Pharmacol. Biochem. Behav. 2007, 86, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Lange, J.E.; Clapp, J.D.; Turrisi, R.; Reavy, R.; Jaccard, J.; Johnson, M.B.; Voas, R.B.; Larimer, M. College Binge Drinking: What Is It? Who Does It? Alcohol. Exp. Res. 2002, 26, 723–730. [Google Scholar] [CrossRef]
- Courtney, K.E.; Polich, J. Binge Drinking in Young Adults: Data, Definitions, and Determinants. Psychol. Bull. 2009, 135, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Montes, M.; Alonso-Blanco, C.; Paz-Zulueta, M.; Sarabia-Cobo, C.; Ruiz-Azcona, L.; Parás-Bravo, P. Binge Drinking in Spanish University Students: Associated Factors and Repercussions: A Preliminary Study. Int. J. Environ. Res. Public Health 2019, 16, 4822. [Google Scholar] [CrossRef] [Green Version]
- Salas-Gomez, D.; Fernandez-Gorgojo, M.; Pozueta, A.; Diaz-Ceballos, I.; Lamarain, M.; Perez, C.; Sanchez-Juan, P. Binge Drinking in Young University Students Is Associated with Alterations in Executive Functions Related to Their Starting Age. PLoS ONE 2016, 11, e0166834. [Google Scholar] [CrossRef]
- Dantzer, C.; Wardle, J.; Fuller, R.; Pampalone, S.Z.; Steptoe, A. International Study of Heavy Drinking: Attitudes and Sociodemographic Factors in University Students. J. Am. Coll. Health 2006, 55, 83–89. [Google Scholar] [CrossRef]
- Carbia, C.; Cadaveira, F.; Caamaño-Isorna, F.; Rodríguez-Holguín, S.; Corral, M. Binge drinking during adolescence and young adulthood is associated with deficits in verbal episodic memory. PLoS ONE 2017, 12, e0171393. [Google Scholar] [CrossRef]
- Schulenberg, J.E.; Johnston, L.D.; O’Malley, P.M.; Bachman, J.G.; Miech, R.A.; Patrick, M.E. Monitoring the Future National Survey Results on Drug Use, 1975–2018: Volume II, College Students and Adults Ages 19–60. Available online: http://monitoringthefuture.org/pubs.html#monographs (accessed on 8 September 2020).
- National Collaborating Centre for Mental Health. Depression: The Nice Guideline on the Treatment and Management of Depression in Adults; The British Psychological Society; The Royal College of Psychiatrists: London, UK, 2010; ISBN 978-1-904671-85-5. [Google Scholar]
- Boden, J.M.; Fergusson, D.M. Alcohol and depression. Addiction 2011, 106, 906–914. [Google Scholar] [CrossRef]
- Wilkinson, A.L.; Halpern, C.T.; Herring, A.H.; Shanahan, M.; Ennett, S.T.; Hussey, J.M.; Harris, K.M. Testing Longitudinal Relationships Between Binge Drinking, Marijuana Use, and Depressive Symptoms and Moderation by Sex. J. Adolesc. Health 2016, 59, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Carver, C.S.; Sheier, M.F. Perspectives on Personality, 7th ed.; Pearson Education, Inc.: London, UK, 2012; ISBN 9780205151363. [Google Scholar]
- Digman, J.M. Personality structure: Emergence of the five-factor model. Annu. Rev. Psychol. 1990, 41, 417–440. [Google Scholar] [CrossRef]
- Costa, P.T.; McCrae, R.R. Revised NEO Personality Inventory (NEO PI-R) and Neo Five-Factor Inventory (NEO-FFI) Professional Manual, 2nd ed.; Psychological Assesssment Resources: Odessa, FL, USA, 1992; ISBN 84-7174-728-6. [Google Scholar]
- Malouff, J.M.; Thorsteinsson, E.B.; Rooke, S.E.; Schutte, N.S. Alcohol involvement and the five-factor model of personality: A meta-analysis. J. Drug Educ. 2007, 37, 277–294. [Google Scholar] [CrossRef]
- Adan, A.; Forero, D.A.; Navarro, J.F. Personality traits related to binge drinking: A systematic review. Front. Psychiatry 2017, 8, 134. [Google Scholar] [CrossRef]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Spanish Government Bulletin. Spanish Government Bulletin Organic Law 3/2018. Personal Data Protection; Spain’s Data Protection Agency: Madrid, Spain, 2018; Volume 294, pp. 5–68.
- Babor, T.F.; Higgins-biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care, 2nd ed.; World Health Organization: Geneva, Switzerland, 2001.
- Rubio Valladolid, G.; Bermejo Vicedo, J.; Caballero Sánchez-Serrano, M.C.; Santo-Domingo Carrasco, J. Validación de la prueba para la identificación de trastornos por uso de alcohol (AUDIT) en Atención Primaria. Rev. Clin. Esp. 1998, 198, 11–14. [Google Scholar]
- García Carretero, M.Á.; Novalbos Ruiz, J.P.; Martínez Delgado, J.M.; O’Ferrall González, C. Validation of the Alcohol Use Disorders Identification Test in university students: AUDIT and AUDIT-C. Adicciones 2016, 28, 194. [Google Scholar] [CrossRef] [Green Version]
- Cortés Tomás, M.T.; Giménez Costa, J.A.; Motos-Sellés, P.; Sancerni Beitia, M.D.; Cadaveira Mahía, F. The utility of the Alcohol Use Disorders Identification Test (AUDIT)for the analysis of binge drinking in university students. Psicothema 2017, 29, 229–235. [Google Scholar] [CrossRef]
- Parada, M.; Corral, M.; Caamaño-Isorna, F.; Mota, N.; Crego, A.; Rodríguez Holguín, S.; Cadaveira, F. Definición del concepto de consumo intensivo de alcohol adolescente (binge drinking). Adicciones 2011, 23, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Sanz, J.; Navarro, M.E.; Vázquez, C.; Eugenia Navarro, M.; Vazquez, C. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. Propiedades psicométricas en población general. Clínica Salud 2003, 14, 249–280. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996; ISBN 978-01-5-801838-6. [Google Scholar]
- Sanz Fernández, J.; Navarro, M.; Vázquez Valverde, C. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): Propiedades psicométricas en estudiantes universitarios. Análisis Modif. Conduct. 2003, 29, 239–288. [Google Scholar]
- Manga, D.; Ramos, F.; Morán, C. The Spanish norms of the NEO five-factor inventory: New data and analyses for its improvement. Int. J. Psychol. Psychol. Ther. 2004, 4, 639–648. [Google Scholar]
- Pedersen, D.E. Gender differences in college binge drinking: Examining the role of depression and school stress. Soc. Sci. J. 2013, 50, 521–529. [Google Scholar] [CrossRef]
- Tavolacci, M.-P.; Boerg, E.; Richard, L.; Meyrignac, G.; Dechelotte, P.; Ladner, J. Prevalence of binge drinking and associated behaviours among 3286 college students in France. BMC Public Health 2016, 16, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haardörfer, R.; Windle, M.; Fairman, R.T.; Berg, C.J. Longitudinal changes in alcohol use and binge-drinking among young-adult college students: Analyses of predictors across system levels. Addict. Behav. 2021, 112, 106619. [Google Scholar] [CrossRef] [PubMed]
- Paljärvi, T.; Koskenvuo, M.; Poikolainen, K.; Kauhanen, J.; Sillanmäki, L.; Mäkelä, P. Binge drinking and depressive symptoms: A 5-year population-based cohort study. Addiction 2009, 104, 1168–1178. [Google Scholar] [CrossRef] [PubMed]
- Nourse, R.; Adamshick, P.; Stoltzfus, J. College Binge Drinking and Its Association with Depression and Anxiety: A Prospective Observational Study. East Asian Arch. Psychiatry 2017, 27, 18–25. [Google Scholar]
- Couture, M.E.; Pearson, R.; Halloran, J.; Stewart, S.H. A qualitative study of the perceived effects of alcohol on depressive symptoms among undergraduates who drink to cope with depression. Drug Alcohol Rev. 2020, 39, 180–188. [Google Scholar] [CrossRef]
- Kenney, S.R.; Anderson, B.J.; Stein, M.D. Drinking to cope mediates the relationship between depression and alcohol risk: Different pathways for college and non-college young adults. Addict. Behav. 2018, 80, 116–123. [Google Scholar] [CrossRef]
- Dahlin, M.; Joneborg, N.; Runeson, B. Stress and depression among medical students: A cross-sectional study. Med. Educ. 2005, 39, 594–604. [Google Scholar] [CrossRef]
- Adan, A.; Navarro, J.F.; Forero, D.A. Personality profile of binge drinking in university students is modulated by sex. A study using the Alternative Five Factor Model. Drug Alcohol Depend. 2016, 165, 120–125. [Google Scholar] [CrossRef]
- Ibáñez, M.I.; Camacho, L.; Mezquita, L.; Villa, H.; Moya-Higueras, J.; Ortet, G. Alcohol expectancies mediate and moderate the associations between big five personality traits and adolescent alcohol consumption and alcohol-related problems. Front. Psychol. 2015, 6, 1838. [Google Scholar] [CrossRef] [Green Version]
- Kuntsche, E.; Kuntsche, S.; Thrul, J.; Gmel, G. Binge drinking: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 976–1017. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total (n = 142) | Binge Drinkers | |||||
|---|---|---|---|---|---|---|
| No (n = 88) | Yes (n = 54) | |||||
| Mean | SD | Mean | SD | Mean | SD | |
| Age | 20.73 | 2.67 | 20.77 | 2.77 | 20.67 | 2.53 |
| p = 0.9830 a | ||||||
| Mean grade | 7.18 | 0.9 | 7.24 | 0.96 | 7.07 | 0.79 |
| p = 0.1753 a | ||||||
| n | % | n | % | n | % | |
| Gender | ||||||
| Female | 125 | 88.03% | 81 | 92.05% | 44 | 81.48% |
| Male | 17 | 11.97% | 7 | 7.95% | 10 | 18.52% |
| p = 0.0598 b | ||||||
| Place of residence | ||||||
| Family home | 113 | 79.58% | 68 | 77.27% | 45 | 83.33% |
| Not in the family home | 29 | 20.42% | 20 | 22.73% | 9 | 16.67% |
| p = 0.3845 b | ||||||
| Maternal level of studies | ||||||
| University | 43 | 30.28% | 33 | 37.5% | 10 | 18.52% |
| Secondary/vocational training | 57 | 40.14% | 32 | 36.36% | 25 | 46.3% |
| Primary | 36 | 25.35% | 21 | 23.86% | 15 | 27.78% |
| No studies | 6 | 4.23% | 2 | 2.27% | 4 | 7.41% |
| p = 0.0631 b | ||||||
| Paternal level of studies | ||||||
| University | 45 | 31.69% | 27 | 30.68% | 18 | 33.33% |
| Secondary/vocational training | 55 | 38.78% | 36 | 40.91% | 19 | 35.19% |
| Primary | 36 | 25.35% | 22 | 25.00% | 14 | 25.93% |
| No studies | 6 | 4.23% | 3 | 3.41% | 3 | 5.56% |
| p = 0.8671 a | ||||||
| Total (n = 142) | Binge Drinkers | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No (n = 88) | Yes (n = 54) | |||||||||||
| Mean | SD | Range | Median | Mean | SD | Range | Median | Mean | SD | Range | Median | |
| Age of onset of alcohol use (n = 136) | 15.24 | 1.65 | 8–19 | 15 | 15.67 | 1.66 | 8–19 | 16 | 14.59 | 1.43 | 12–18 | 15 |
| p < 0.0001 a | ||||||||||||
| AUDIT total | 4.96 | 4.55 | 0–20 | 3 | 2.94 | 2.92 | 0–14 | 2 | 8.26 | 4.83 | 1–20 | 7 |
| p < 0.0001 a | ||||||||||||
| SUBSTANCE USE IN THE LAST 12 MONTHS | ||||||||||||
| n | % | n | % | n | % | |||||||
| Alcohol | ||||||||||||
| Less than monthly | 41 | 28.87% | 39 | 44.32% | 2 | 3.7% | ||||||
| 1 to 3 times a month | 57 | 40.14% | 38 | 43.18% | 19 | 35.19% | ||||||
| Once a week | 17 | 11.97% | 5 | 5.68% | 12 | 22.22% | ||||||
| 2 or more times per week | 27 | 19.01% | 6 | 6.82% | 21 | 38.89% | ||||||
| p < 0.0001 b | ||||||||||||
| Tobacco | ||||||||||||
| Never | 99 | 69.72% | 71 | 80.68% | 28 | 51.85% | ||||||
| Some days | 32 | 22.54% | 15 | 17.05% | 17 | 31.48% | ||||||
| Every day | 11 | 7.75% | 2 | 2.27% | 9 | 16.67% | ||||||
| p = 0.0003 b | ||||||||||||
| Cannabis | ||||||||||||
| Never | 110 | 77.46% | 79 | 89.77% | 31 | 57.41% | ||||||
| Some days | 32 | 22.54% | 9 | 10.23% | 23 | 42.59% | ||||||
| p < 0.0001 b | ||||||||||||
| Cocaine | ||||||||||||
| Never | 142 | 100.00% | 88 | 100.00% | 54 | 100.00% | ||||||
| Total (n = 142) | Binge Drinkers | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No (n = 88) | Yes (n = 54) | |||||||||||
| Mean | SD | Range | Median | Mean | SD | Range | Median | Mean | SD | Range | Median | |
| BDI-II Total score | 7.46 | 6.86 | 0–37 | 6.00 | 6.83 | 6.34 | 0–37 | 5.00 | 8.48 | 7.57 | 0–37 | 7.5 |
| p = 0.2476 b | ||||||||||||
| n | % | n | % | n | % | |||||||
| BDI-II tercile | ||||||||||||
| BDI-II ≤3 | 46 | 32.39% | 29 | 32.95% | 17 | 31.48% | ||||||
| 3 < BDI-II ≤11 | 64 | 45.07% | 43 | 48.86% | 21 | 38.89% | ||||||
| BDI-II >11 | 32 | 22.54% | 16 | 18.18% | 16 | 29.63% | ||||||
| p = 0.2583 a | ||||||||||||
| Level of depressive symptomatology | ||||||||||||
| Minimum (0–13) | 121 | 85.21% | 77 | 87.50% | 44 | 81.48% | ||||||
| Mild (14–19) | 14 | 9.86% | 8 | 9.09% | 6 | 11.11% | ||||||
| Moderate (20–18) | 5 | 3.52% | 2 | 2.27% | 3 | 5.56% | ||||||
| Severe (29–63) | 2 | 1.41% | 1 | 1.14% | 1 | 1.85% | ||||||
| p = 0.7096 a | ||||||||||||
| Total (n = 142) | Binge Drinkers | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No (n = 88) | Yes (n = 54) | |||||||||||
| TOTAL SCORES | ||||||||||||
| Mean | SD | Range | Median | Mean | SD | Range | Median | Mean | SD | Range | Median | |
| Neuroticism | 20.37 | 8.24 | 3–44 | 20.00 | 20.39 | 8.52 | 3–44 | 20.00 | 20.33 | 7.85 | 7–39 | 20.50 |
| Difference: 0.05 CI (−2.77−2.88) p = 0.9705 a | ||||||||||||
| Extraversion | 32.58 | 7.30 | 10–47 | 33.00 | 31.32 | 7.09 | 10–44 | 32.00 | 34.63 | 7.24 | 14–47 | 35.00 |
| p = 0.0062 b | ||||||||||||
| Openness | 30.25 | 6.98 | 10–47 | 30.00 | 29.86 | 6.21 | 15–44 | 29.50 | 30.89 | 8.10 | 10–47 | 32.00 |
| p = 0.4273 b | ||||||||||||
| Agreeableness | 31.31 | 5.88 | 16–45 | 31.00 | 31.56 | 5.99 | 16–45 | 31.00 | 30.91 | 5.72 | 19–43 | 31.50 |
| Difference: 0.65 CI (−1.36−2.66) p = 0.4601 a | ||||||||||||
| Conscientiousness | 33.05 | 6.73 | 10–55 | 33.00 | 34.19 | 6.41 | 10–55 | 34.00 | 31.19 | 6.87 | 16–44 | 31.50 |
| p = 0.0224 b | ||||||||||||
| TERCILE | ||||||||||||
| n | % | n | % | n | % | |||||||
| Neuroticism (NEU) | ||||||||||||
| NEU ≤ 13 | 37 | 26.06% | 24 | 27.27% | 13 | 24.07% | ||||||
| 13 < NEU ≤ 26 | 70 | 49.30% | 41 | 46.59% | 29 | 53.70% | ||||||
| NEU > 26 | 35 | 24.65% | 23 | 26.14% | 12 | 22.22% | ||||||
| p = 0.7108 c | ||||||||||||
| Extraversion (EXT) | ||||||||||||
| EXT ≤ 28 | 42 | 29.58% | 32 | 36.36% | 10 | 18.52% | ||||||
| 28 < EXT ≤ 37 | 67 | 47.18% | 40 | 45.45% | 27 | 50.00% | ||||||
| EXT > 37 | 33 | 23.24% | 16 | 18.18% | 17 | 31.48% | ||||||
| p = 0.0429 c | ||||||||||||
| Openness (OPE) | ||||||||||||
| OPE ≤ 25 | 37 | 26.06% | 21 | 23.86% | 16 | 29.63% | ||||||
| 25 < OPE ≤ 35 | 73 | 51.41% | 51 | 57.95% | 22 | 40.74% | ||||||
| OPE > 35 | 32 | 22.54% | 16 | 18.18% | 16 | 29.63% | ||||||
| p = 0.1164 c | ||||||||||||
| Agreeableness (AGR) | ||||||||||||
| AGR ≤ 28 | 45 | 31.69% | 24 | 27.27% | 21 | 38.89% | ||||||
| 28 < AGR ≤ 36 | 69 | 48.59% | 47 | 53.41% | 22 | 40.74% | ||||||
| AGR > 36 | 28 | 19.72% | 17 | 19.32% | 11 | 20.37% | ||||||
| p = 0.2796 c | ||||||||||||
| Conscientiousness (CON) | ||||||||||||
| CON ≤ 29 | 41 | 28.87% | 21 | 23.86% | 20 | 37.04% | ||||||
| 29 < CON ≤ 37 | 69 | 48.59% | 44 | 50.00% | 25 | 46.30% | ||||||
| CON > 37 | 32 | 22.54% | 23 | 26.14% | 9 | 16.67% | ||||||
| p = 0.1793 c | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrero-Montes, M.; Alonso-Blanco, C.; Paz-Zulueta, M.; Pellico-López, A.; Ruiz-Azcona, L.; Sarabia-Cobo, C.; Fradejas-Sastre, V.; Boixadera-Planas, E.; Parás-Bravo, P. Relationship between Depressive Symptoms, Personality, and Binge Drinking among University Students in Spain. J. Clin. Med. 2022, 11, 53. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010053
Herrero-Montes M, Alonso-Blanco C, Paz-Zulueta M, Pellico-López A, Ruiz-Azcona L, Sarabia-Cobo C, Fradejas-Sastre V, Boixadera-Planas E, Parás-Bravo P. Relationship between Depressive Symptoms, Personality, and Binge Drinking among University Students in Spain. Journal of Clinical Medicine. 2022; 11(1):53. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010053
Chicago/Turabian StyleHerrero-Montes, Manuel, Cristina Alonso-Blanco, María Paz-Zulueta, Amada Pellico-López, Laura Ruiz-Azcona, Carmen Sarabia-Cobo, Víctor Fradejas-Sastre, Ester Boixadera-Planas, and Paula Parás-Bravo. 2022. "Relationship between Depressive Symptoms, Personality, and Binge Drinking among University Students in Spain" Journal of Clinical Medicine 11, no. 1: 53. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010053